
Abstract
Background:
Thyroid autoimmunity, especially Graves' disease or hypothyroidism with positive autoantibodies (TRAb) to the thyrotropin receptor (TSHR), occurs in 30–40% of patients with relapsing multiple sclerosis following treatment with alemtuzumab (ALTZ). ALTZ therapy therefore provides a unique opportunity to study the evolution of TRAb prior to clinical presentation. TRAb can stimulate (TSAb), block (TBAb), or not affect (“neutral”) the TSHR function, causing hyperthyroidism, hypothyroidism, or euthyroidism, respectively.
Methods:
A longitudinal retrospective analysis was conducted of TRAb bioactivity over a period of nine years in 45 multiple sclerosis patients receiving ALTZ using available stored serum. Of these 45 patients, 31 developed thyroid dysfunction (TD) and 14 remained euthyroid despite being followed for a minimum of five years (NO-TD). The presence of TRAb was evaluated at standardized time points: (i) before ALTZ, (ii) latest time available following ALTZ and before TD onset, and (iii) following ALTZ during/after TD onset. Serum TRAb were detected by published in-house assays (ihTRAb): flow cytometry detecting any TSHR-binding TRAb, and luciferase bioassays detecting TSAb/TBAb bioactivity. Purified immunoglobulin G was used to verify TSAb/TBAb in selected hypothyroid cases. Standard clinical automated measurements of TRAb, antithyroid peroxidase autoantibodies (TPOAb), thyrotropin, free thyroxine, and free triiodothyronine were also collected.
Results:
Before ALTZ, combined ihTRAb (positive with flow cytometry and/or luciferase bioassay) but not automated TRAb were present in 5/16 (31.2%) TD versus 0/14 (0%) NO-TD (p = 0.017). Detectable ihTRAb preceded TD development in 9/28 (32.1%) and by a median of 1.2 years (range 28 days–7.3 years). Combination testing of ihTRAb and TPOAb at baseline predicted 20% of subsequent cases of hyperthyroidism and 83% of hypothyroidism.
Conclusions:
Evidence is presented that TRAb measured with custom-made assays can be detected prior to any change in thyroid function in up to a third of cases of ALTZ-related TD. Furthermore, the presence of ihTRAb prior to ALTZ treatment was strongly predictive of subsequent TD. The findings suggest that a period of affinity maturation of TRAb may precede clinical disease onset in some cases. Combined testing of TPOAb and ihTRAb may increase the ability to predict those who will develop TD following ALTZ.
Introduction
A
Among TA, ALTZ predominantly induces Graves' disease (GD; 63%), followed by hypothyroidism (34%), and rarely transient thyroiditis (11). GD is caused by antithyrotropin receptor (TSHR) autoantibodies (TRAb) persistently activating the TSHR (TSHR-stimulating antibodies [TSAb]), leading to hyperthyroidism (15). TRAb can also block the TSHR (TSHR-blocking antibodies [TBAb]), causing hypothyroidism (16,17), and “neutral” TRAb (which bind the TSHR without affecting thyroid function; TNAb) have been reported in around 12% of subjects with normal thyroid function, 59–84% of GD patients (depending on the assay type used), and patients with autoimmune thyroiditis at lower rates (18 –20). TNAb seem to bind to the TSHR but do not activate the cAMP signaling cascade, which is the principal pathway leading to thyroid hormones synthesis. However, they may be able to trigger alternative and multiple signaling cascades having complex downstream effects, including oxidative stress (20).
In spontaneous TA, TBAb account for a minority of cases of hypothyroidism (around 9–10%) (16,21), the remainder being due to lymphocyte-mediated damaging of the thyroid, as in classical Hashimoto's thyroiditis (22). Autoantibodies to thyroid peroxidase (TPOAb) are the hallmark of such autoimmune thyroiditis. However, they are very often positive in GD also, indicating that in TA the self-tolerance breakdown involves multiple thyroid antigens (23). Surprisingly, TRAb are positive in 50.0–76.7% of patients with post-ALTZ hypothyroidism (9,10), with TBAb representing a common mechanism of post-ALTZ hypothyroidism in a recent analysis (10).
TPOAb are very common in the general population (up to 20%) (24,25), and have been identified as a predictive marker of TD subsequent to ALTZ (9). In particular, 69% of MS subjects who were TPOAb+ before ALTZ developed subsequent TD compared to 31% of TPOAb– subjects. However, 85% patients who later developed TD were TPOAb– at baseline, indicating that TPOAb status alone has limited value in risk stratification in the majority of patients (9).
The longitudinal study of ALTZ-treated patients provides a rare opportunity to study TRAb prevalence and biological function prior to disease “triggering” in patients who develop GD. The automated TRAb assays (autTRAb) used in clinical diagnostics are unable to distinguish TSAb/TBAb (26). As a result, several groups have developed in-house bioassays able to detect TSAb (27,28) and TBAb (21,29), as well as TNAb (19). It was postulated that TRAb, in particular TNAb, pre-existing before ALTZ may be the precursors of the TSAb and TBAb that subsequently develop by somatic hypermutation and affinity maturation in B cells (30,31). Detection of low-titer or low-affinity TSAb/TBAb or the presence of TNAb prior to ALTZ therapy in combination with TPOAb testing may also increase the ability to predict thyroid dysfunction (TD) after ALTZ.
In addition, in-house TRAb bioassays (ihTRAb) were used to analyze TRAb bioactivity arising after ALTZ therapy, which has so far only been described in spontaneous TA (21,28,32). In a recent British study conducted in collaboration between Cambridge and Cardiff, TSAb/TBAb analysis was introduced in post-ALTZ TA. However, this was limited to only a few patients affected with hypothyroidism or “fluctuating” GD, defined as multiple alternate phases of hyperthyroidism and hypothyroidism (10). In the present study, this analysis was extended to all available cases, including a third different in-house assay to detect TSHR-binding TRAb independently from their bioactivity (19).
Methods
Patients and sera
Blood samples from Welsh MS patients consenting to research have been consecutively collected for research purposes from 2006 (REC# 05/WSE03/111) and stored within the Welsh Neuroscience Research Tissue Bank (REC# 14/WA/0073; Cardiff, United Kingdom). Blood samples were processed within three hours of collection following a standardized protocol, including spin at 4423 g for 10 minutes at 4°C. Serum and plasma were subsequently aliquoted and stored at −80°C.
Sera of 45 patients affected with relapsing MS treated with ALTZ with longitudinal samples between August 2006 and October 2015 were identified, including samples from 31 consecutive subjects with post-ALTZ TD. Samples from 14 patients who had not developed TD (NO-TD) were also selected based on the availability of serum before ALTZ and clinical follow-up of five years or more in order to exclude cases of late-onset TD (11). Sera from pre-specified time points were requested for TD and NO-TD groups (Fig. 1): (i) first available pre-ALTZ time; (ii) the latest time available following ALTZ and before the onset of TD; (iii) following ALTZ at the onset of TD or alternatively the earliest subsequent time available (TD only).
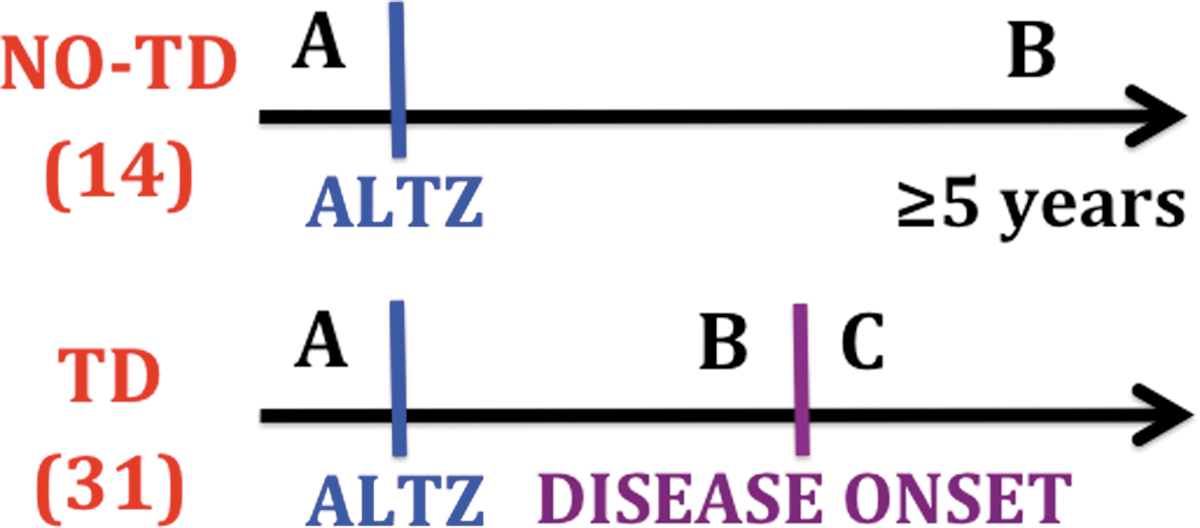
Serum time points. ALTZ, first alemtuzumab treatment; TD, patients developing thyroid dysfunction; NO-TD, patients not developing thyroid dysfunction; A, first available time before ALTZ (both TD and NO-TD); B, post ALTZ, first available time before the onset of thyroid dysfunction (TD) or the latest available time post ALTZ (NO-TD); C, post ALTZ during the onset of thyroid function abnormalities, or in alternative the earliest available time after it (TD only). Color images available online at
All patients were treated with ALTZ at the University Hospital of Wales (UHW; Cardiff, United Kingdom), and followed both at UHW and local Welsh hospitals. ALTZ was administered intravenously five consecutive days for the first cycle, with the majority of subjects receiving a second cycle (three consecutive days) 12 months later. In some patients, further doses were given at least one year apart, depending on clinical and radiological outcomes. The date of the first ALTZ administration within the patient cohort ranged from April 2002 to November 2012. The initiation dose was 24–30 mg/day prior to 2006 and then reduced to 12 mg/day. Since blood collection for research purposes commenced only in 2006, this explains why time point A is missing in several patients.
Information about patients' age, thyrotropin (TSH), free thyroxine (fT4), free triiodothyronine (fT3), TPOAb, TRAb determined by automated assays, thyroid treatment, and number of ALTZ treatments were collected when available. Demographic information and detailed longitudinal clinical information was available for all patients, with the last update in February 2018.
Luciferase bioassays (TSAb/TBAb)
In-house luciferase bioassays (LB) to detect TSAb and TBAb were performed using a Chinese Hamster Ovary (CHO) cell line stably transfected with the human TSHR and a cAMP responsive luciferase reporter (pA3Luc), as previously described (Lulu*) (27,29). Briefly, cells were seeded at 2 × 104 cells/well in 96-well plates in Ham's F12 containing 10% fetal calf serum, and switched to Ham's F12 containing 10% charcoal-stripped calf serum the day before the assay. When performing the assays, cells were incubated for four hours at 37°C in 5% CO2 in air with whole human serum (1:10 dilution) in serum-free medium (SFM; Ham's F-12 supplemented with 2.5% sodium bicarbonate) for the TSAb assay, and SFM containing 1 mIU/mL bovine TSH (bTSH; Sigma–Aldrich, Poole, United Kingdom) in the TBAb assay. Cells were also incubated with SFM alone as negative control, and 5 mIU/mL bTSH and 0.2 ng/μL M22 human monoclonal antibody to TSHR (RSR, Cardiff, United Kingdom) as positive controls. Cells were finally lysed, and the luciferase activity measured using commercially available kits (Promega, Madison, WI) and a luminometer machine (Glomax®-Multi Detection System; Promega).
Randomly selected sera from nine euthyroid participants from the Controlled Antenatal Thyroid Screening II (CATS II) study (33,34) were used as euthyroid pool in both TSAb/TBAb assays. They were all adult women (M age ± standard deviation [SD] = 40.8 ± 5.3 years) with normal thyroid function and negative for TPOAb.
In the TSAb assay, CHO cells transfected with pA3Luc only (Zulu) were used in parallel to Lulu*. The considered positivity cutoff was a stimulation index (SI) >1.5 calculated with the following formula:
The TBAb assay positivity cutoff was an inhibition index (InI) >20%, as previously determined (formula A) (29) using Lulu* cultured with 1 mIU/mL bTSH:
In order to exclude interference of high serum TSH levels with the in-house TSAb/TBAb serum assay, especially among hypothyroid patients, experiments were repeated using immunoglobulin G (IgG; amount equivalent to 1:10 serum dilution) in place of serum. If results were discordant, those using IgG were counted. IgG was purified from selected serum samples with the Melon Gel IgG Purification Kit (Pierce, Rockford, IL) according to the manufacturer's protocol. Briefly, serum samples were diluted 1:10, and the diluted serum was added to a spin column containing the Melon Gel resin. After 30 minutes of incubation, the purified IgGs were collected in the flow through by centrifugation of the spin column, and the IgG concentration was measured by ultraviolet optical absorption at 280 nm with a NanoDrop™ Lite spectrophotometer (Thermo Fisher Scientific, Waltham, MA). All IgG-purified samples were promptly used for downstream analysis or aliquoted and stored at −20°C.
Flow cytometry (TSHR-binding TRAb)
In order to reduce the high nonspecific background staining due to human antibodies recognizing and/or cross-binding to surface CHO proteins, a serum pre-adsorption step using Zulu cells was performed, as previously described (35).
Flow cytometry (FC) detection of TSHR-binding TRAb (FC-TRAb) in pre-adsorbed sera was then performed using CHO cells expressing the glycosylphosphatidylinositol (GPI)-anchored TSHR extracellular domain (CHO-TSHR), as previously described (19). As minor protocol modifications, 1:100 goat polyclonal anti-human IgG (H + L) Alexa Fluor 488 (Life Technologies, Carlsbad, CA) and 1:1000 LIVE/DEAD® Fixable Near-IR Dead Cell Stain Kit (Invitrogen, Carlsbad, CA) were used as second conjugated antibody and viability dye, respectively (35). Zulu cells were used as CHO control cell line not expressing TSHR. The fluorescence of 10,000 cells/tube was assayed by BD FACSCanto II flow cytofluorometer, FACSDiva Software (BD Biosciences, San Jose, CA); no fluorescein isothiocyanate (FITC; TRAb) or Apc-Cy7 (LIVE/DEAD®) channels compensation was needed (500–520 nm and 633–750 nm excitation emission peaks wavelengths, respectively) (35).
FC data were analyzed using FlowJo v8.8.6 (TreeStar, Inc., Ashland, OR), and damaged or dead cells (Apc-Cy7+) were gated and excluded from analysis (35). The geometric mean FITC fluorescence intensity values of CHO-TSHR and Zulu cells were compared for all sera, and the Kolmogorov–Smirnov univariate two-sample test was used to obtain the greatest difference between the two histograms, quoted as D-value (36). Cutoff values were defined based on the mean D + 2 SD of individual pre-adsorbed sera from nine healthy women from the CATS II study (33,34) used as controls. All values higher than this were considered positive (FC-TRAb+) (35).
Automated laboratory measurements
AutTRAb were measured with the Brahms Diagnostika Lumitest TRAK assay (Berlin, Germany; reference ranges: negative <1 IU/L, borderline 1–1.5 IU/L, positive >1.5 IU/L) until January 2014 and then the Roche Cobas® e411 assay (Basel, Switzerland; reference ranges: negative <0.9 IU/L, borderline 0.9–1.6 IU/L, positive >1.6 IU/L). According to Thermo Fisher Scientific, human TSH does not interfere with TRAb measurement in the Lumitest TRAK assay, up to TSH values of at least 500 mIU/L. UHW Biochemistry Department also runs specific cross-reactivity tests using patient serum with a TSH concentration of 179 mIU/L, confirming no interference with either Brahms or Roche TRAb assays.
TPOAb, TSH, fT4, and fT3 analyses were performed using an ADVIA Centaur automated immunoassay analyzer (Bayer plc, Reading, United Kingdom) until May 31, 2010, followed by chemiluminescent microparticle immunoassay methods with the ARCHITECT® System (Abbott Laboratories, Chicago, IL) until the end of the observation period. Supplementary Table S1 (Supplementary Data are available online at
Definitions of thyroid function
All 45 patients included in the study were euthyroid when receiving the first ALTZ treatment and had no clinical history of thyroid disease. The time of TD onset was defined as the first alteration of the thyroid function defined as persistent (i.e., detectable in consecutive blood tests at least three months apart) and/or significant (i.e., requiring immediate thyroid treatment). Hyperthyroidism was defined as low TSH with or without raised fT4/fT3 levels; hypothyroidism was defined as raised TSH with or without low fT4/fT3 levels.
Thyroid diagnosis was defined as: (i) GD: TRAb+ hyperthyroidism; (ii) fluctuating GD: TRAb+ cases with multiple alternate phases of hyperthyroidism and hypothyroidism, not explained by overtreatment or poor treatment compliance; (iii) TRAb+ hypothyroidism; (iv) chronic autoimmune thyroiditis (37): persistent hypothyroidism (≥6 months) with positive TPOAb and negative TRAb; (v) subacute thyroiditis: transient hyperthyroidism, hypothyroidism, or both, with TD lasting less than six months in total, TRAb–, with or without TPOAb; (vi) TPOAb–/TRAb– hypothyroidism: persistent hypothyroidism (≥6 months) with negative TPOAb and TRAb.
Statistical analysis
According to the TRAb prevalence in the general population of 12% (19), an a priori power calculation indicated 12 versus 12 subjects were required to provide 80% power to detect a fivefold TRAb prevalence (60%) in patients who will later develop ALTZ-induced TD, with a 0.05 significance level (two-tailed).
Presence of TRAb at different time points was compared between TD and NO-TD groups using Fisher's exact text, considering a p-value of <0.05 as significant. As explorative analysis, positivity of TPOAb and TRAb measured with automated assays was also considered.
Fisher's exact test and a t-test were used also to compare the characteristics of TD and NO-TD groups, considering a p-value of <0.05 as significant.
Results
Patients
The date of first ALTZ treatment ranged from 2002 to 2012 (median 2008), and the M ± SD follow-up was 9.0 ± 2.5 years post ALTZ (range 4.3–14.0 years). The TD group comprised patients showing post-ALTZ hyperthyroidism (n = 19) or hypothyroidism (n = 12) as first clinical manifestation (TD onset).
Table 1 summarizes the characteristics of TD and NO-TD groups. No significant differences were detected between the different groups. Before TD onset (time points A and B), all patients were euthyroid and free of persistent thyroid function abnormalities. Note that at time point C (TD group), many patients who developed TD were already on thyroid medication. A detailed description of their treatment and outcome has been reported elsewhere (10).
Patient Characteristics
Fisher exact test (sex distribution) and t-test (other variables) excluded significant differences between the groups, when comparable (p = n.s).
Until TD onset.
Until the end of the observational period (time point B).
Time point A serum was available in 10 hyperthyroid, 6 hypothyroid (16 overall TD), and 14 NO-TD patients.
Time point B serum was available in 17 hyperthyroid, 8 hypothyroid (25 overall TD), and 14 NO-TD patients.
Time point C serum was available in 17 hyperthyroid and 12 hypothyroid (29 overall TD) patients.
ALTZ, alemtuzumab treatment; NA, not applicable; SD, standard deviation; TD, thyroid dysfunction (abnormal thyroid hormones); TD onset, time of the first TD defined as persistent (i.e., detectable in consecutive blood tests at least three months apart) and/or significant (i.e., requiring a thyroid treatment to be started immediately).
Combined ihTRAb results at all time points
The overall results obtained with the three different ihTRAb assays (FC-TRAb, LB-TSAb, and LB-TBAb) were compared at all time points in TD and NO-TD groups. Due to the retrospective nature of this study, sera from some time points were unavailable for the TD group (Table 1). As shown in Figure 2, at time point A (before ALTZ), 5/16 (31.2%) TD patients were found to be ihTRAb+ compared to 0/14 (0%) NO-TD patients (p = 0.017). Following ALTZ, 6/25 (24.0%) TD patients were ihTRAb+ at time point B (before TD onset). As expected, at time point C (during or after TD onset), ihTRAb+ cases markedly increased to 18/29 (62.1%). This prevalence is likely to be underestimated, considering the late average collection time of time point C compared with disease onset (Table 1). Among NO-TD patients, 4/14 (28.6%) were ihTRAb+ at time point B. When splitting the overall ihTRAb+ results according to the TD subtype at onset (hyperthyroidism or hypothyroidism), time point A ihTRAb were predominantly positive in those who subsequently developed hypothyroidism (4/6; 66.7%) rather than hyperthyroidism (1/10; 10%; p = 0.036). It is worth noting that two initially hypothyroid ihTRAb+ patients subsequently showed a fluctuating thyroid function and were classified as fluctuating GD.

Positive in-house antithyrotropin receptor autoantibody (ihTRAb+) results at all time points. Cross-sectional results of all available sera at pre-specified time points (see Fig. 1) analyzed with ihTRAb obtained in TD and NO-TD patients. Below the dashed line, TD patients were further subgrouped into hyperthyroidism (HYPER) or hypothyroidism (HYPO) as first clinical manifestation. Numbers in parentheses indicate the total number of available sera for each time point and patient subgroup. A, time point A = before the first treatment with alemtuzumab (ALTZ); B, time point B = latest available time post ALTZ and before TD onset, when applicable; C, time point C (TD only) = post ALTZ during the onset of thyroid function abnormalities, or in alternative the earliest available time after it. FC-TRAb (blue), TRAb detected by flow cytometry; LB-TSAb (green), stimulating TRAb detected by luciferase bioassays; LB-TBAb (purple), blocking TRAb detected by luciferase bioassays; Tot ihTRAb (orange), positive FC-TRAb and/or LB-TSAb and/or LB-TBAb (percentages refer to this column); Neg TRAb (white), ihTRAb– results with all the three techniques: flow cytometry and luciferase bioassays to detect TSAb and TBAb. Color images available online at
Time point A: predictors of post-ALTZ TD
To validate TRAb as an independent predictor of ALTZ-induced TD, ihTRAb results were compared to autTRAb and TPOAb data at time point A (Table 2). Pre-ALTZ ihTRAb and TPOAb had a very similar predictive value for future TD development. When ihTRAb and TPOAb testing were combined together, 7/16 (43.8%) TD patients were positive versus 0/14 in the NO-TD group (p = 0.007). In particular, 83.3% hypothyroid and 20% hyperthyroid cases were predicted versus 50% and 20%, respectively, when considering TPOAb alone (Table 2, last two columns). Detailed TRAb and/or TPOAb predictive values, sensitivity, and specificity are reported in Supplementary Table S2.
Time Point A: Predictive Value of Baseline TRAb versus TPOAb
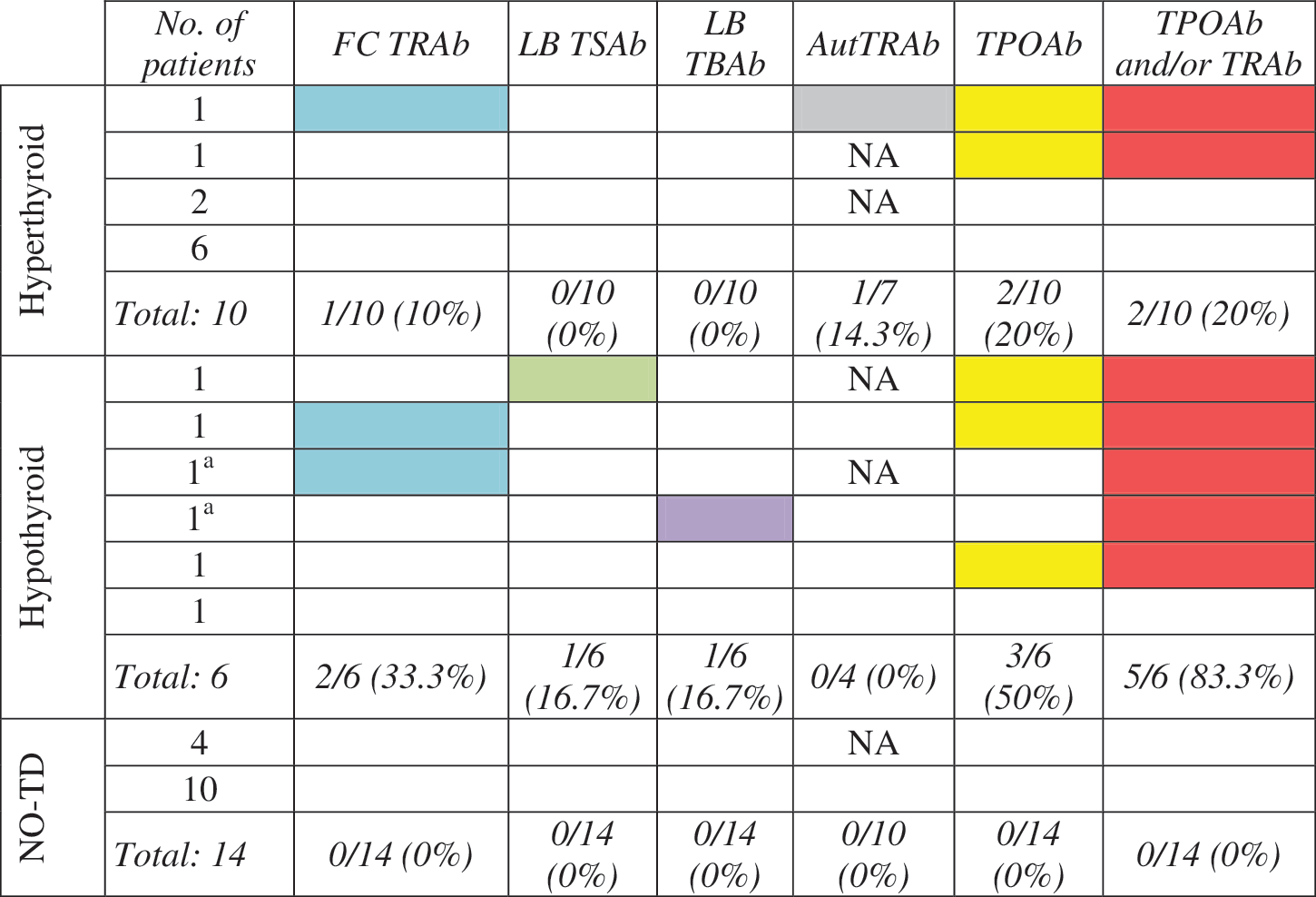
Cross-sectional results of all available sera at time point A (before alemtuzumab treatment; see Fig. 1) for autoantibodies to the thyrotropin receptor (TRAb) and autoantibodies to thyroid peroxidase (TPOAb), obtained in patients developing subsequent hyperthyroidism or hypothyroidism as first clinical manifestation, and patients not developing any thyroid dysfunction (NO-TD) following alemtuzumab treatment.
White cells represent negative TRAb/TPOAb results. Colored squares represent positive results: blue, TRAb detected by flow cytometry (FC-TRAb); green, stimulating TRAb detected by luciferase bioassays (LB-TSAb); purple, blocking TRAb detected by luciferase bioassays (LB-TBAb); gray, TRAb detected by automated systems (Aut-TRAb); yellow, TPOAb (automated assay); red, TRAb (any test) and/or TPOAb.
Fluctuating Graves' disease (GD) presenting hypothyroidism as first clinical manifestation.
Color table available online at
In-depth analysis of ihTRAb+ cases
Tables 3 –6 report in more detail the ihTRAb+ cases only, describing the different ihTRAb subtypes in comparison with autTRAb, TPOAb, and TSH results, when available. Here, the hyperthyroid group was further subdivided into classic hyperthyroid GD and fluctuating GD. At time point A, ihTRAb+ cases as expected were predominantly TNAb (3/5; 60%), defined as FC-TRAb+ but both LB-TSAb/TBAb– (3–6).
TRAb, TPOAb, and TSH Status in Patients with ihTRAb+: Hyperthyroid Patients (GD)
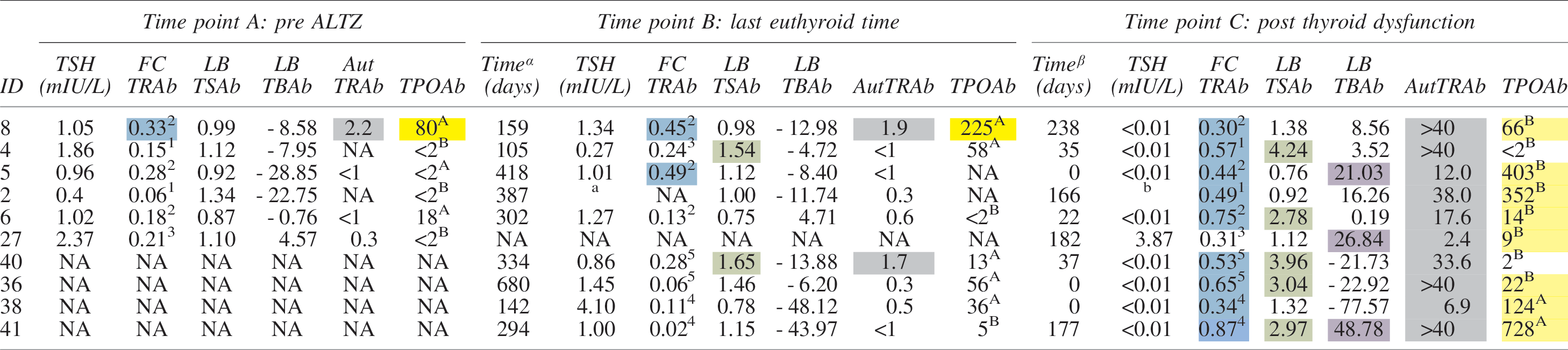
Summary of autoantibodies to the thyrotropin receptor (TRAb), autoantibodies to thyroid peroxidase (TPOAb), and thyrotropin (TSH) status among patients positive for in-house TRAb assays (ihTRAb+). Only patients who were ihTRAb+ in at least one time point are represented.
TSH normal reference range varies between 0.30–4.4 mIU/L and 0.35–5.5 mIU/L, depending on the assay used and the date of test (see Supplementary Table S1).
Time (days) before onset of thyroid dysfunction.
Time (days) after onset of thyroid dysfunction.
Reference ranges and positivity cutoffs:
AutTRAb (IU/L) reference ranges: negative <1, borderline 1–1.5, positive >1.5 (until January 2014); negative <0.9, borderline 0.9–1.6, positive (from February 2014 onwards).
TPOAb (IU/mL) reference ranges: Anegative <60, positive ≥60 (until May 2010); B negative <6, positive ≥6 (from June 2010 onwards).
FC-TRAb positivity cut-offs. Samples have been tested in five different sets of experiments, each producing slightly different mean of greatest differences in fluorescence intensity between the two histograms (D) and relative standard deviation (SD) among pooled controls. Samples were considered positive if Dsample > Dcontrols + 2 SD.
Set 1 Dcontrols + 2 SD = 0.26.
Set 2 Dcontrols + 2 SD = 0.30.
Set 3 Dcontrols + 2 SD = 0.42.
Set 4 Dcontrols + 2 SD = 0.21.
Set 5 Dcontrols + 2 SD = 0.32.
LB-TSAb positive if stimulation index (SI) >1.5.
LB-TBAb (%) positive if inhibition index (InI) >20%.
ID 2 is missing TSH values for both time points Ba and C,b so the closest TSH results are provided:
Previous TSH = 0.36 mIU/L (233 days before); next TSH <0.02 mIU/L (202 days after, during a transient subclinical hyperthyroidism phase lasted <3 months).
Previous TSH <0.02 mIU/L (166 days before, same day of thyroid dysfunction onset); next TSH = 17.81 mIU/L (55 days after, during carbimazole treatment).
White cells, negative TRAb/TPOAb results. Colored squares represent positive results: blue, TRAb detected by flow cytometry (FC-TRAb); green, stimulating TRAb detected by luciferase bioassays (LB-TSAb); purple, blocking TRAb detected by luciferase bioassays (LB-TBAb); gray, TRAb detected by automated systems (AutTRAb); yellow, TPOAb (automated assay).
Color table available online at
ALTZ, alemtuzumab; GD, Graves' disease; ID, patient's identification number; NA, not applicable or not available.
TRAb, TPOAb, and TSH Status in Patients with ihTRAb+: Fluctuating GD

TSH not available. Previous TSH = 1.96 mIU/L (182 days before); next TSH = 159.68 mIU/L (583 days after, corresponding to time point C, same day of thyroid dysfunction onset).
Refer to Table 3 for additional footnotes. Color table available online at
TRAb, TPOAb, and TSH Status in Patients with ihTRAb+: Hypothyroid Patients

TSH not available, but likely within the normal range, considering the evidence of stable euthyroidism under levothyroxine treatment for nearly 4 years post ALTZ.
Refer to Table 3 for additional footnotes. Color table available online at
TRAb, TPOAb, and TSH Status in Patients with ihTRAb+: NO-TD Patients

TSH not available, but likely within the normal range, considering the evidence of stable euthyroidism for 5.9 years post ALTZ.
Refer to Table 3 for additional footnotes. Color table available online at
Considering this from a different perspective, TD developed in 7/7 (100%) baseline ihTRAb+ and/or TPOAb+ patients versus 9/23 (39.1%) baseline ihTRAb− and/or TPOAb– patients (p = 0.007).
AutTRAb were positive before ALTZ in only one patient in the TD hyperthyroid subgroup (14.3%) and none in the hypothyroid group, suggesting that autTRAb do not appear to be a useful predictive marker of subsequent TD development.
At time point B, ihTRAb+ cases were represented by a similar proportion of TNAb, TSAb, and TBAb (Tables 3 –6). In combination, TNAb or TSAb/TBAb preceded TD onset in nine (32.1%) cases (considering a total of 28 TD patients with time point A and/or B available), with an interval before TD onset of a median of 1.2 years (range 28 days–7.3 years).
At time point C (Tables 3 –6), as expected, all ihTRAb+ hyperthyroid GD and fluctuating GD patients were also autTRAb+, confirming a GD diagnosis. Among ihTRAb+ hyperthyroid and fluctuating GD cases, FC-TRAb was the most sensitive assay, with 13/14 (92.9%) positive versus 9/14 (64.3%) of TSAb. TBAb were positive in 3/10 (30%) purely hyperthyroid ihTRAb+ GD patients. As expected, fluctuating GD cases had a documented TSAb/TBAb coexistence in 2/4 (50%) cases (IDs 35 and 42); the other two cases were positive for TSAb only (IDs 1 and 7). Among the whole hypothyroid group (n = 10), 4 (40%) were ihTRAb+ at time point C. In particular, 2/4 (50%) were FC-TRAb+, and 2/4 (50%) were both FC-TRAb+ and TBAb+. AutTRAb results were concordant (Tables 3 –6). Surprisingly, both ihTRAb+ hypothyroid patients at time point A (IDs 15 and 37) were ihTRAb– at time point C.
Final thyroid diagnosis
TPOAb titers measured any time after ALTZ were available in 17/19 (89.5%) of the hyperthyroid group, and were positive in 15/17 (88.2%) cases. In fact, two TPOAb– GD patients at time point C (Tables 3 –6) later became TPOAb+ (e.g., ID 27). Any time after ALTZ, TPOAb were positive in 11/12 (91.7%) of hypothyroid patients. None of the 14 NO-TD patients developed post-ALTZ TPOAb.
According to their clinical course, TD patients were classified as pure hyperthyroid GD (n = 17), fluctuating GD (n = 4), and hypothyroid patients (n = 10). AutTRAb were positive in 17/17 (100%) GD and 4/4 (100%) fluctuating GD. Taking also the ihTRAb results into account, the final thyroid diagnosis as per criteria given in the methods was 17 (54.8%) GD, four (12.9%) fluctuating GD (two started with hypothyroidism, two with hyperthyroidism), four (12.9%) TRAb+ hypothyroidism, three (9.7%) chronic autoimmune thyroiditis, two (6.5%) TPOAb+ subacute thyroiditis, and one (3.2%) TPOAb–/TRAb– hypothyroidism.
Discussion
For the first time, the biological function of TRAb is described in a longitudinal cohort of patients developing ALTZ-induced TD using three different ihTRAb assays. Importantly, as a result of a structured monitoring and sampling process for patients with MS in South Wales and suitable for ALTZ treatment, serum was available before the onset of TD, enabling how and when TRAb become positive to be described in patients with ALTZ-induced TD. This setting is unique, as serum is not generally available before disease onset in sporadic GD. Interestingly, serum ihTRAb but not TRAb detected with standard automated assays (autTRAb) were detected before ALTZ in one third of patients who later developed TD and in none of those who remained free of TD (NO-TD) over a minimum follow-up period of five years. The appearance of ihTRAb was detected a mean of 1.2 years (range 28 days–7.3 years) prior to the development of TD. It is believed that this is the first report of the detection of TRAb prior to the onset of ALTZ-induced TD. Similar findings have been previously described for spontaneous TD in a retrospective study showing progressively increasing TRAb positivity, as well as TPOAb and antithyroglobulin antibodies, in patients who will later develop GD. In particular, TRAb positivity increased from 2% at seven years before diagnosis to 55% at diagnosis, with intermediate percentages of 7% and 20% at −5 and −2 years, respectively (38).
Furthermore, this study provides details about TRAb biological function over time. The presence of TNAb detected using flow cytometry in healthy euthyroid subjects has been previously reported but without any follow-up clinical data to indicate whether they later did develop TD (19). Information similar to the data in ALTZ-induced disease is difficult to collect in the setting of spontaneous autoimmune TD, requiring very large and long-term cohort studies. The fact that the rates of TD post ALTZ are much higher than generally seen in MS suggests that the two settings are not necessarily comparable. However, the principle that autoimmunity to the TSHR may precede TD by many months or years applies to both ALTZ-induced (this study) and spontaneous forms of TD as reported by others (38). Note that the wide range of pre-TD intervals (28 days–7.3 years) is partly a consequence of the retrospective nature of this study, not providing systematic and identical time points for all patients. Future prospective studies are needed to define precisely how long ihTRAb may precede the onset of TD in some cases.
In cases of TRAb positivity predating TD, it is hypothesized that TSHR-reactive B-cell clones may undergo progressive antigen-driven affinity maturation by somatic hypermutation within germinal centers, and finally generate high-affinity stimulating (TSAb) or blocking (TBAb) TRAb. The phenomenon of multiple different pathogenic TRAb arising from single B-cell clones by somatic hypermutation has already been described in mouse models of GD (30,31). In this context, the finding that ihTRAb more commonly preceded hypo- than hyperthyroidism is interesting, but may reflect that once a stimulatory TSAb-secreting clone develops, TD follows rapidly, whereas it may take longer for TBAb to achieve clinically relevant inhibition of thyroid function such that TSH levels rise. The observations are in accordance with previous evidence that TSAb are potent at low concentrations, therefore inducing hyperthyroidism rapidly after their appearance (23), while TBAb levels needed to trigger hypothyroidism are usually much higher than TSAb levels inducing hyperthyroidism (26). Further prospective studies with large numbers of subjects should clarify this. It also has to be mentioned that TD patients were not subclassified into subclinical and overt disease, since the vast majority of patients diagnosed with subclinical disease went on to develop overt TD or were treated immediately after diagnosis, preventing the possible evolution to overt disease.
Although it is understandable that TNAb can exist without altering thyroid function, it is less clear how this is possible with TSAb and TBAb. Possible explanations for TSAb/TBAb+ cases in euthyroid patients are: (i) they are low affinity and therefore not able to exert a significant function on TSHR activity with clinical consequence; or (ii) the in vitro assays in some cases do not reflect the different and more complex human thyroid environment, providing slightly different results from the in vivo situation. For example, luciferase bioassays use bovine and not human TSH, CHO cells instead of human thyrocytes, and only the cAMP pathway is investigated. The same observations about TNAb or low-affinity TSAb/TBAb apply to 28.6% euthyroid NO-TD patients developing post-ALTZ TRAb. In the future, they might remain positive with no long-term clinical consequences, or they might develop late-onset TD.
TD post ALTZ is often delayed by several years, and the ability to reliably predict those at risk would allow targeted monitoring and possibly early intervention or prevention. TPOAb are already known to identify subjects at risk, with 69% of individuals who are TPOAb+ at baseline developing TD. However, TPOAb testing only detects around 15% of all future cases of TD post ALTZ (9). The current data suggest that custom-made TRAb testing in combination with TPOAb testing at baseline might increase this to predicting around 20% of hyperthyroid cases and 80% of hypothyroid cases. Interestingly, in two hypothyroid patients, pre-ALTZ ihTRAb positivity was no longer detectable at the time of disease onset, suggesting that TRAb titers fluctuate over time and are not always detectable. Furthermore, in these cases, they also might have become spontaneously negative, and destructive thyroiditis might represent the sole mechanism of hypothyroidism.
The analysis of ihTRAb proved less valuable than expected for predicting the disease course after the onset of TD. For example, not all subjects who developed hypothyroidism or GD with fluctuating course had detectable TBAb. Several explanations are possible: (i) non-optimal timing of time point C, often several months after the disease onset and the commencement of antithyroid treatment, usually associated with TRAb titer decrease and negativization; (ii) TSAb/TBAb levels might fluctuate over time, not always being positive at the same time; (iii) TBAb might interact with the TSHR with a lower affinity compared to TSAb, and therefore might be masked by TSAb coexistence in the biological assays. Similarly, TBAb false-positive cases have been described due to the concomitant presence of TSAb. If TSAb act as weak agonists, they interfere with the bTSH in the TBAb assay, resulting in a signal reduction. In general, TSAb/TBAb coexistence can be challenging to demonstrate due to their mutual interference, depending on relative concentrations, affinities, and potencies, varying over time. Sometimes serum serial dilutions are needed to distinguish properly between the two TRAb populations (26).
However, the findings show that around 40% of hypothyroidism post ALTZ is TBAb mediated, as suggested in previous studies (9,10). This is nonetheless substantially higher than reports in spontaneous disease (around 10%) (16,21). By contrast, 91.7% (11/12) of hypothyroid subjects were TPOAb+, consistent with TBAb– hypothyroidism post ALTZ still being autoimmune in the majority of cases but perhaps cell mediated. However, it was notable that autTRAb were detectable in many subjects who developed hypothyroidism or a switching course, as well as all those with hyperthyroidism. Currently, autTRAb measurement is recommended only in patients developing hyperthyroidism. If these observations are confirmed in larger prospective studies, autTRAb testing should probably be extended to all cases of post-ALTZ TD, including hypothyroidism, since they appear to predict a more complex clinical course (i.e., possibility of thyroid function switching) requiring close observation.
The strengths of this study are the long follow-up to define outcome (≥5 years where no TD is reported) and the wide range of thyroid autoantibody assays used. However, ALTZ has only recently been licensed for use in relapsing/remitting MS (since 2014), and hence ALTZ-induced TD is currently not very common, especially cases with the long follow-up required to define outcome. As a result, the cohort is relatively small (n = 45), and this is a limitation. Furthermore, due to the retrospective nature of the study, serum was not available at all time points in the whole cohort, and in particular, samples at the time of TD onset were not always available. However, the finding that TRAb can precede disease onset and are associated with subsequent TD is robust, as the numbers were consistent with a priori power calculations.
In conclusion, it has been observed that TRAb can precede TD by many years and, if present before ALTZ, can increase the risk of subsequent development of TD. Future prospective studies are needed to determine the exact value of baseline and follow-up TRAb testing in subjects treated with ALTZ and the most valuable assay to use. Such studies, as well as large cohort studies in spontaneous thyroid autoimmunity, may also be used to investigate and define the process of affinity maturation in TRAb further. Now that ALTZ is licensed for the treatment of relapsing/remitting MS in more than 60 countries, the available case load for prospective studies is likely to increase substantially and make at least the studies in ALTZ-induced disease feasible.
Footnotes
Acknowledgments
This study was supported by the Society for Endocrinology Early Career Grant to I.M. The authors are also grateful to the Welsh Neuroscience Research Tissue Bank (Cardiff, United Kingdom) for providing the human sera used in the present study, and to the patients providing their consent for research purposes.
Author Disclosure Statement
I.M. reports grants from the Society for Endocrinology during the conduct of the study. No other competing financial interests exist.