
Abstract
Background:
The potential risk of subsequent malignant neoplasms (SMNs) after radioactive iodine (RAI) treatment of thyroid cancer (TC) is an important concern.
Methods:
A systematic review was updated comparing the risk of SMNs in TC patients treated with RAI to TC patients without RAI. Six electronic databases were searched (up to March, 2018), supplemented with a hand search. Two reviewers independently screened citations, reviewed full-text papers, and critically appraised/abstracted data. Random-effects meta-analyses were conducted using crude data and data statistically adjusted for confounders. The outcomes were any SMN and specific SMNs for which sufficient data were available.
Results:
In total, 3506 unique electronic search citations and 93 full-text papers were examined, including 17 studies (3 systematic reviews and 14 original studies). Published knowledge syntheses were limited by inclusion of small numbers of studies, with two systematic reviews suggesting an increased risk of any SMN and one meta-analysis suggesting a reduced risk of breast SMN after RAI treatment. In a meta-analysis of crude data, the risk ratio of any SMN in RAI-treated TC patients was 0.98 ([confidence interval (CI) 0.76–1.27]; n = 10 studies of 65,539 individuals, heterogeneity Q = 64.26, degrees of freedom [df] = 9, p < 0.001, I 2 = 85.99). The pooled risk ratio for any SMN, adjusted for confounders, was 1.16 ([CI 0.97–1.39]; n = 6 studies, data from at least 11,241 TC patients, Q = 10.86, df = 5, p = 0.054, I 2 = 53.96). In secondary analyses examining specific SMNs, although relatively rare, the risk of subsequent leukemia was increased, but the risk of multiple myeloma was reduced in RAI-treated TC patients. There was no significant increased relative risk of breast cancer, salivary cancer, or combined hematologic malignancies according to RAI treatment status.
Conclusions:
The body of evidence on whether 131I treatment of thyroid cancer is associated with the primary outcome of any SMN is highly heterogeneous and complex. More research examining the long-term risk of specific SMNs after 131I treatment is needed.
Introduction
It is estimated that worldwide, over five years, more than a million individuals are diagnosed with thyroid cancer (TC) (1). Following surgery for differentiated TC, radioactive iodine (RAI) may be used for ablation of the thyroid remnant, as adjuvant treatment, or as treatment of persistent or recurrent disease (2). The potential risk of subsequent malignant neoplasms (SMNs) associated with RAI is an important concern.
The objective was to update a systematic review and meta-analysis (3), comparing and quantifying the SMN risk among TC patients treated with RAI (131I after thyroid cancer surgery) to that in TC patients who did not receive RAI. The original review was published in 2009, and at the time, there were very few data on the topic (two included studies). This updated systematic review was performed due to a recent increment in published data in this area.
Methods
Study question and eligibility criteria for study selection
A systematic review and meta-analysis was conducted of published English language studies examining whether the risk of SMN was different in TC survivors treated with RAI compared to those not treated with RAI. Thyroid cancer was required to be the first malignancy, and studies were required to report the rate of any SMN or specific SMN(s) in RAI-treated and non-RAI treated individuals, respectively (or describe the crude data in respective treatment groups in sufficient detail that a relative risk could be calculated). Eligible studies included published clinical trials, observational studies (>50 thyroid cancer patients), or systematic reviews/meta-analyses that were focused on the study question. Narrative reviews, editorials, or letters without original data were not eligible for inclusion. For overlapping study groups (such as multiple reports from the same clinical or registry data set), the largest (i.e., containing the largest number of thyroid cancer patients) or most recent report containing relevant data (for respective SMN outcomes) was included. Included studies were also restricted to the English language due to insufficient resources for translation.
Data sources and searches
An information specialist (R.F.) conducted a search of six electronic databases (MEDLINE Epub ahead of print and in-process and other non-indexed citations, Ovid MEDLINE, CINAHL [from EBSCOhost], Cochrane Clinical Trials, Cochrane Systematic Reviews, and EMBASE [from OVID platform]) from the period of the prior review (2008) until June 2017 (details listed in Supplementary Table S1; Supplementary Data are available online at
Critical appraisal of included studies and data abstraction
Data were abstracted, and individual study quality was appraised by two independent reviewers from a review team (A.M.S., C.Y., A.G., or O.S.), with final consensus on all of the results. In the case of any important discrepancies or questions, a third reviewer from the team independently performed a review, and a final consensus was reached. For included papers, the individuals critically appraising papers were not authors of the studies under review. A customized data abstraction form was utilized by the abstractors, and consensus results were tabulated. The following critical appraisal methods were used, as indicated by the design of the included study: (i) Cochrane Risk of Bias Assessment Tool: for non-randomized studies of interventions (ACROBAT-NRSI, v1.0.0, 2014) (4) (a complete description of this tool with instructions for its use and a template freely are available at
Statistical analyses
Random-effects meta-analyses were performed comparing the relative risk (risk ratio) of one or more SMNs between TC patients treated with RAI to those not treated with RAI (Comprehensive Meta-Analysis software v2.0; Biostat, Inc.). The random-effects meta-analysis, which was originally described by DerSimonian and Laird, accounts for variation in effects across studies by incorporating an estimate of the effect variation between studies (6). Random-effects meta-analyses were chosen, as studies from a variety of study settings were expected to be included, examining a variety of second primary malignancies with heterogeneous baseline risk rates. Respective meta-analyses were performed, pooling (i) crude event rates (cumulative incidence rates over the entire duration of follow-up or lifetime) and (ii) risk estimates that were statistically adjusted for confounders (i.e., in a multivariable explanatory model or propensity analysis, where two or more potential confounders were accounted for in the analysis) (7). It was assumed that alternative risk estimates were comparable to risk ratios (relative risks) for relatively uncommon events (i.e., <10% cumulative SMN incidence within the total study follow-up period) in the adjusted meta-analysis (8). In the adjusted model, the inverse variance calculation method was used, and the pooled effect was exponentiated, such that a risk ratio of >1 represented increased risk, as previously described (9). Secondary subgroup mixed-effects meta-analyses of the unadjusted risk of any SMN were also planned to explore the impact on heterogeneity, respectively stratifying according to cumulative 131I activity administered, examining the effect of 131I activity and study quality. It is important to note that for the 131I activity comparisons, specific cut points for activity comparisons were not defined, a priori, as this was intended as an exploratory secondary analysis of available included data. Thus, the cut points for 131I activity comparisons were dependent on the availability of sufficient data for meaningful subgroup analyses among the various studies. Heterogeneity (variability) of risk estimates among included studies was evaluated using Cochrane's Q-test (10) and the I 2 measure (11). Potential publication bias was evaluated graphically using a funnel plot (12) for the primary outcome of any SMN, assuming a minimum of 10 studies for meaningful analysis (9). Statistical significance was defined as an alpha level of 0.05, with the exception of Cochrane's Q-test, where an alpha level of 0.1 was used (11). All statistical analyses were performed using Comprehensive Meta-Analysis software version 2.0 (Biostat, Inc.).
Results
In the electronic search, 4651 citations were identified, which yielded 3506 unique citations after excluding duplicates (Fig. 1). Another 12 relevant full-text papers were identified through the hand search. A total of 93 full-text papers were reviewed (3,13 –28) (Supplementary References S1–S76 and Supplementary Table S2). Seventeen studies were included in the current systematic review, including three published knowledge syntheses (systematic reviews/meta-analyses) (3,13,14) and 14 original studies (15 –28) (Fig. 1).
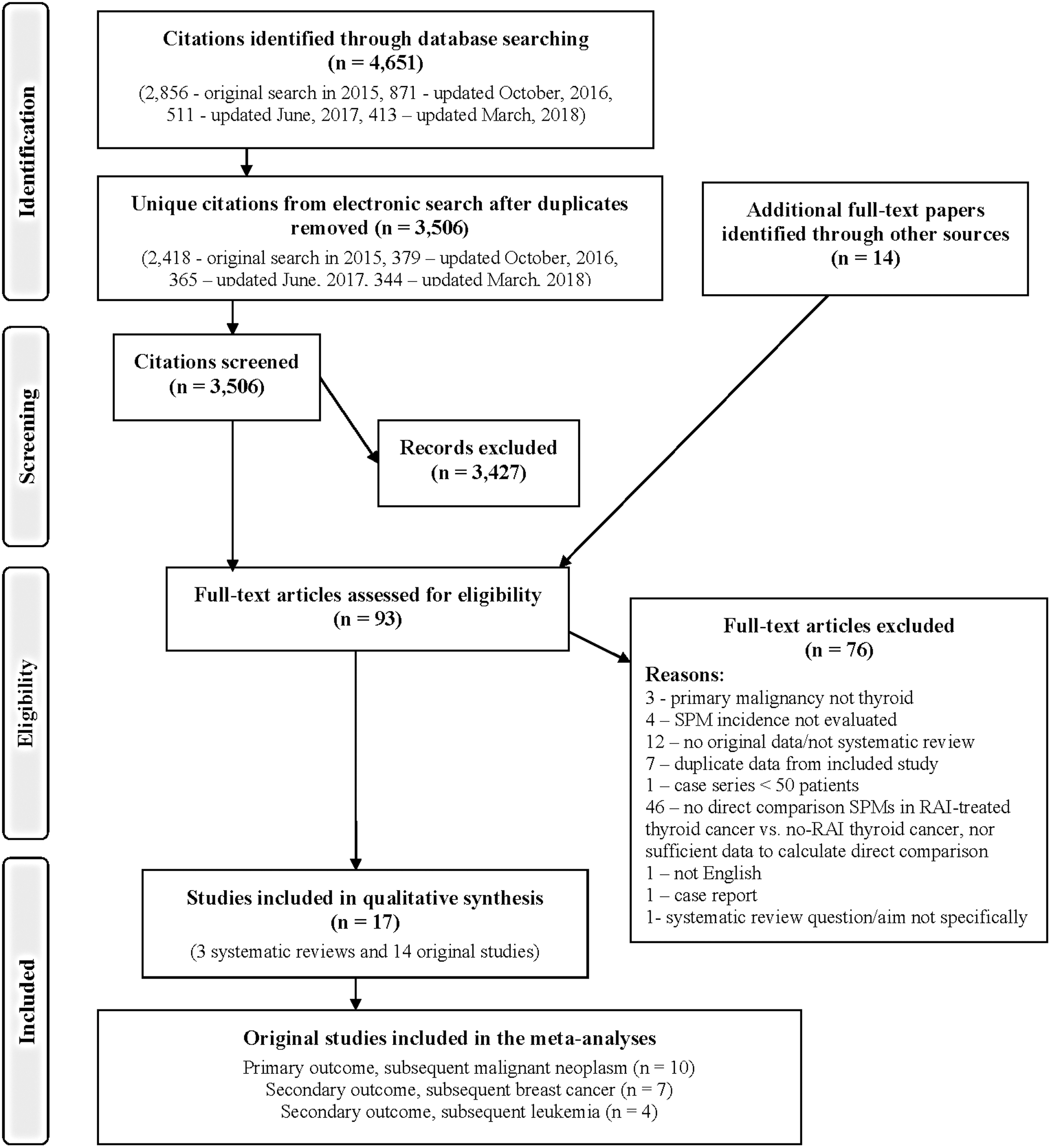
Study flow diagram (using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses format) (29).
Review of published knowledge syntheses
The results of published knowledge syntheses were reviewed to enable an understanding of prior knowledge on the topic. A summary of the characteristics and critical appraisal of the three included systematic reviews/meta-analyses (3,13,14) is shown in Table 1. In summary, two systematic reviews (3,13) suggested an increased risk of SMNs in individuals with TC who were treated with RAI compared to those who were not, but these reviews were limited by a small number of included papers (i.e., two to four studies for this comparison). Zhang et al. performed a systematic review and meta-analysis examining the risk of second primary breast cancer in female TC survivors, and reported a risk ratio of 0.61 [confidence interval (CI) 0.47–0.79] in the RAI group (data from six observational studies, including 17,914 women, with no significant heterogeneity) (14). A limitation of this review was a lack of critical appraisal of study quality (14). One systematic review reported on the relationship between 131I cumulative activity and SMN risk (13). Clement et al. reported that in four of five studies (n = 7831), which included a multivariable explanatory model, the SMN risk was significantly elevated, with increasing 131I activity (13).
Characteristics of the Included Systematic Reviews
AMSTAR, Assessment of Multiple Systematic Reviews critical appraisal tool.
Description of the included original studies
Fourteen original studies were included, which reported data on SMNs (in general) or one or more specific SMNs, and all of them were observational (15 –28). The study characteristics and results of critical appraisal are shown in Table 2.
Description of the Study Characteristics of the Included Original Studies
The prevalence of this characteristic was not compared between patients who received 131I and those who did not.
Reported as radiotherapy in the original paper.
Others include the Electricité De France, COGEMA, and FRAMATOME.
Timing of the external beam radiation treatment relative to the thyroid cancer diagnosis not clearly reported.
The two respective studies from Molenaar et al. reported on different SPM outcomes.
Outcome of any SMN
Ten studies reported data on the rate of any SMN in TC patients according to RAI treatment status (15,25,16 –21,23,26). The mean or median follow-up periods varied from 5 to 16 years, for studies reporting this characteristic (15 –18,20,21,23,25,26,28). The mean or median cumulative 131I activity varied from 3700 to 5550 MBq (100–150 mCi) for studies reporting on this characteristic (18,23 –25,26). Two studies commented on patient preparation methods for RAI treatment (i.e., thyroid hormone withdrawal or recombinant human thyrotropin [rhTSH]) but combined both preparation groups so a comparison was not possible (21,25). One of the studies included patients treated prior to regulatory approval of rhTSH use for RAI therapy in the regions of study (Europe). So, these patients most likely underwent thyroid hormone withdrawal (23). The percentage of all TC patients who developed any SMN in the respective included studies varied from 2.5% to 12.0% (15,25,16 –21,23,26). In the updated meta-analysis, the risk ratio of any SMN in RAI-treated TC patients was 0.98 ([CI 0.76–1.27], n = 10 studies using crude cumulative risk data from 65,539 thyroid cancer survivors, including 5053 SMN events, with a high degree of heterogeneity among studies, Q = 64.26, degrees of freedom [df] = 9, p < 0.001, I 2 = 85.99; Fig. 2). A funnel plot suggested some potential publication bias (Fig. 3), with fewer than expected small studies with reduced SMN risk with RAI treatment, although one must be cautious in the interpretation of this plot, given the relatively small number of studies included in the analysis (n = 10) and the observed heterogeneity of risk among studies.
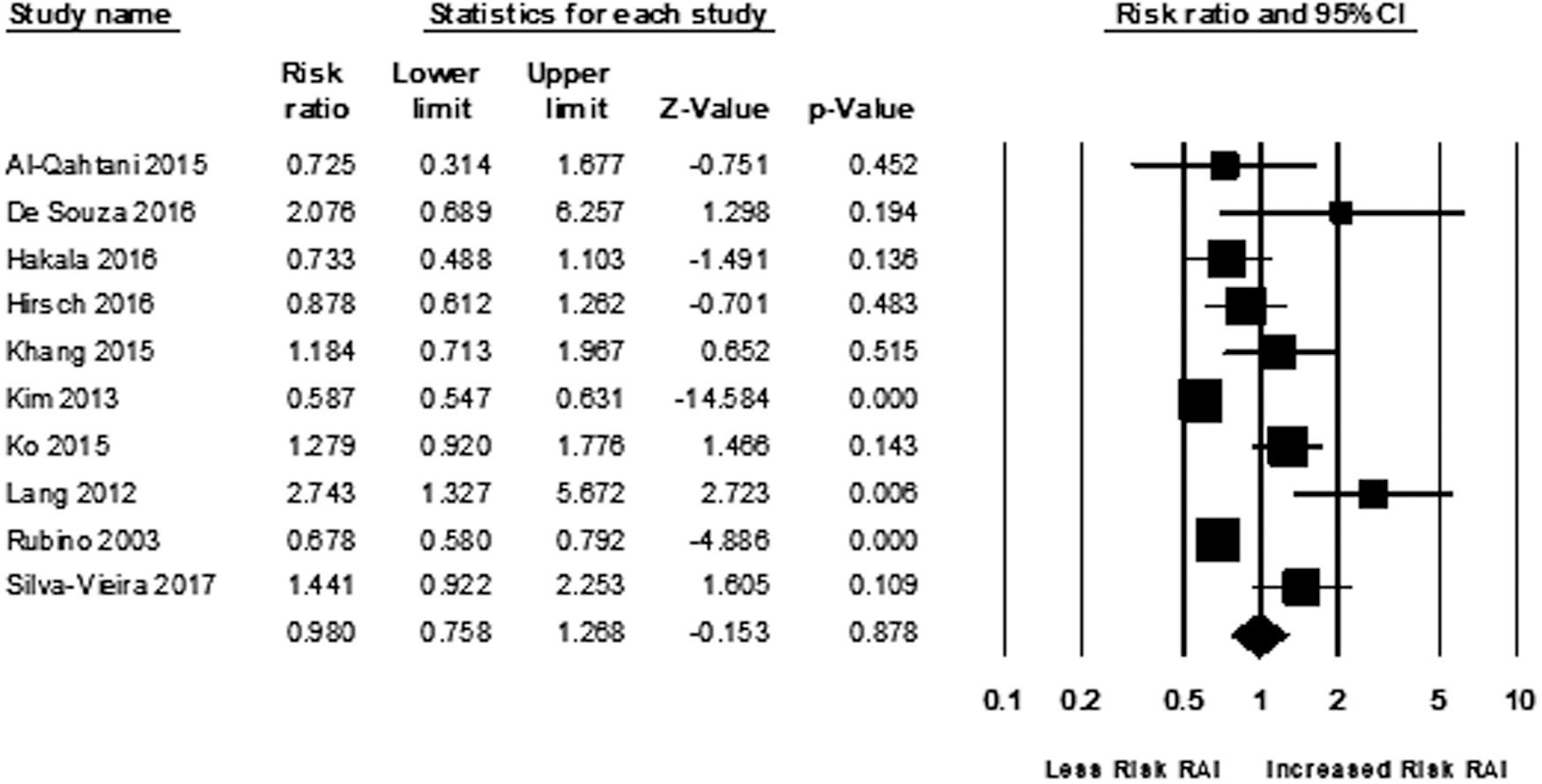
Forest plot showing a random-effects meta-analysis of unadjusted risk of subsequent malignant neoplasms in thyroid cancer patients treated with RAI compared to those who did not receive RAI. The diamond at the bottom of the figure represents the pooled relative risk. RAI, radioactive iodine.

Funnel plot demonstrating some publication bias in reported crude data for the outcome of risk ratio of any subsequent malignant neoplasm (SMN). The funnel plot depicts the relationship between study size (expressed as a standard error) on the vertical axis and effect size (risk estimate relative to RAI treatment) on the horizontal axis, where the clear circles represent studies included in the meta-analysis and the diamond represents the pooled risk estimate (generated using CMA Meta-Analysis v2.0; Biostat, Inc.). In the absence of publication bias, there should be a symmetrical distribution of studies on either side of the diamond.
Multivariable explanatory model or propensity analyses predicting any SMN risk relative to RAI treatment were reported in eight studies (16 –18,20,21,23,25,26). DeSouza et al. reported that in a multivariable explanatory model, adjusted for age at TC diagnosis, sex, and histology (papillary TC), there was no statistically increased risk relative to RAI use (regression coefficient = 0.56, standard error [SE] = 0.59, p = 0.35, n = 413) (25). Hakala et al. reported that the rate ratio for SMN in RAI-treated TC patients was 1.12 ([CI 0.91–1.38], p = 0.161, n = 914) after adjusting for age, sex, year of diagnosis, histologic subtype, and RAI dose (incorporating duration of follow-up) (16). Furthermore, Hirsch et al. reported that in a time-to-event analysis adjusted for age, sex, and cumulative 131I dose, the hazard ratio (HR) for SMN in RAI-treated TC patients was 1.00 ([CI 0.99–1.01], p = 0.933, n = 1877) (17). Khang et al. reported that the odds ratio (OR) for SMN in RAI-treated TC patients was 1.14 ([CI 0.67–1.91], n = 2468) in a multivariable explanatory model adjusted for age, sex, period of diagnosis, pathology (follicular or papillary thyroid cancer), and cumulative activity (n = 2468) (18). However, Khang et al. also reported that in a very high cumulative activity subgroup (≥37,000 MBq [≥1000 mCi]), an increased SMN risk was observed (OR = 5.85 [CI 2.61–13.07]) (18). Ko et al. matched 131I-treated TC patients with those who did not receive RAI according to a propensity score, calculated using a logistic regression model where 131I treatment status was regressed relative to baseline characteristics (incorporating age, sex, Charlson comorbidity index score, and treatment [chemotherapy, radiotherapy]) and observed that the hazard ratio (HR) for SMN in the RAI-treated group was 1.23 ([CI 0.88–1.72], n = 3668) (20). Lang et al. performed a Cox proportional hazards analysis predicting SMN that was adjusted for age, sex, period of TC diagnosis, disease stage, and cumulative RAI activity and reported that the adjusted risk of SMN was increased in individuals receiving 3000–8900 MBq of 131I (81–241 mCi; HR = 2.78 [CI 1.08–7.15], p = 0.034) but not in those receiving >9000 MBq of 131I (>243 mCi; HR = 3.15 [CI 0.65–12.82], p = 0.131; total study N = 895) (21). Rubino et al. reported that the relative risk of SMN in RAI-treated TC patients was 1.2 ([CI 1.0–1.4], n = 6841) after adjusting for study cohort (i.e., registry location), external beam radiotherapy, and incorporating years of patient follow-up (23). Silva-Vieira et al. reported that using a Fine and Gray regression model adjusted for age, sex, familial cancer history, personal cancer history, and competitive risk, the relative risk of SMN in RAI-treated TC patients was 1.84 ([CI 1.02–3.31], p = 0.043, n = 2031) (26). It was observed that in a random-effects meta-analysis of data adjusted for statistical confounders, the risk ratio for SMN in RAI-treated patients was 1.17 ([CI 0.98–1.39], p = 0.093), including data from six studies, including at least 11,241 TC patients (Cochrane's Q = 11.43, df = 5, p = 0.043, I2 = 56.26; Fig. 4).

Forest plot showing the meta-analysis of relative risk of subsequent malignant neoplasms after RAI treatment compared to no RAI treatment, adjusted for confounders. The diamond at the bottom of the figure represents the pooled relative risk. Data from the following studies could not be pooled using the inverse variance calculation method for the following reasons: Rubino et al. (23), log of confidence interval asymmetric; De Souza et al. (25), lower limit of log of confidence interval <0; Lang et al. (21), subgroup of RAI-treated TC patients who received >9000 MBq (243 mCi) lower limit of log of confidence interval <0. For the study by Lang et al., data from the subgroup of patients who received 3000–8900 MBq (81–241 mCi) is included in the meta-analysis. The total number of patients included in this meta-analysis is estimated to be at least 11,654 (excluding the n of RAI-treated patients in the study from Lang et al., as the n for the specific dose activity subgroup included was not specified in the original publication).
The impact of RAI activity on crude SMN risk compared to thyroid cancer controls not treated with RAI was explored. The cut point(s) for comparing 131I activities were based on the availability of sufficient data for meaningful analysis. The most commonly used 131I activity cut point in the included studies was 3700 MBq (100 mCi) (15 –18). In three studies (15 –17) reporting on detailed subgroup data for thyroid cancer patients treated with ≤3700 MBq (≤100 mCi) of 131I, the relative risk of any SMN was 0.84 ([CI 0.52–1.34], p = 0.458; data from 132 thyroid cancer survivors treated with 131I and 1457 thyroid cancer patients who did not receive 131I). Furthermore, in four studies (15 –18) reporting on detailed subgroup data for thyroid cancer patients treated with >3700 MBq (>100 mCi) compared to thyroid cancer patients who did not receive 131I, the relative risk was 1.06 ([CI 0.70–1.59], p = 0.793), including data from 132 thyroid cancer patients treated with 131I and 2420 thyroid cancer patients who did not receive 131I). In a secondary mixed-effects analysis of crude SMN rates, stratified by these subgroups of respective dose activities, the overall relative risk of SMN after 131I treatment was estimated to be 0.96 ([CI 0.70–1.30], p = 0.744), and there was no significant difference between the lower and higher dose subgroups (heterogeneity between activity strata, Cochrane's Q = 0.537, df = 1, p = 0.464, using the respective subgroup data from the seven studies). Furthermore, a secondary mixed-effects meta-analysis of crude SMN rates from 10 studies, stratified by study quality (low or moderate risk of bias compared to serious risk of bias), the overall relative risk was estimated to be 0.98 ([CI 0.76–1.28], p = 0.903), with some evidence of a significant difference between strata (Cochrane's Q = 4.04, df = 1, p = 0.044, with a possibility for lower risk estimates in lower quality studies).
Risk of subsequent breast cancer
Seven original studies reported on the risk of subsequent breast cancer in TC survivors treated with RAI and those not treated with RAI (17,19,21 –23,25,26). The mean or median follow-up period for studies reporting this variable varied from 7 to 13 years (17,21 –23,25,26). The risk of subsequent breast cancer varied from 1.2% to 2.5% in these seven studies (17,19,21 –23,25,26). Breast cancer was the most commonly reported type of SMN in six studies reporting on various SMN types (17,19,21,23,25,26). In a pooled analysis, it was found that the relative risk of breast cancer in RAI-treated TC patients compared to TC controls was 0.80 ([CI 0.53–1.21], p = 0.281, n = 7 studies, using crude data from 68,481 TC survivors, including 1276 subsequent breast cancer events). However, this finding was subject to a high degree of statistical heterogeneity (with Cochrane's Q = 28.83, df = 6, p < 0.001, I 2 = 79.19).
There was one study that reported on the risk of subsequent breast cancer relative to RAI treatment after adjustment for relevant confounders (22). Lin et al. reported that the adjusted hazard ratio for secondary breast cancer was 1.18 [CI 0.79–1.77] in TC patients treated with cumulative 131I dose activities of ≤4440 MBq, and 0.90 [CI 0.56–1.46] in TC patients treated with >4440 MBq compared to thyroid cancer patients who did not receive 131I (after adjustment for age, comorbidities, hormone therapy [i.e., estrogen/progesterone], mammography, ultrasound, radiotherapy, chemotherapy, and thyroxine treatment) (22).
Risk of subsequent leukemia and chronic myeloproliferative neoplasms/myelodysplastic syndrome
Four studies provided data on the risk of subsequent leukemia (any type) in TC patients treated with RAI compared to those not treated with RAI (23,24,26,28), and the largest of these was a Korean national insurance database study from Seo et al. (24). The cumulative incidence rate of subsequent leukemia varied from 0.03% to 0.26% (23,24,26,28) over a mean or median follow-up period varying from 2 (24) to 13 years (23) (for respective studies reporting on this variable). In a pooled analysis, it was found that the relative risk of subsequent leukemia in RAI-treated TC patients (compared to TC controls without RAI) was 1.60 ([CI 1.30–1.96], p < 0.001, including data from four studies, n = 367,369 TC patients, including 384 subsequent leukemia events, with little evidence to suggest heterogeneity of effect among studies, Cochrane's Q = 2.58, df = 3, p = 0.461, I 2 = 0). One study reported the results of adjusted analyses for subsequent leukemia risk (28). Specifically, Molenaar et al. reported an increased risk of acute myeloid leukemia (AML; HR = 1.79 [CI 1.13–2.82], p = 0.012) and chronic myeloid leukemia (HR = 3.44 [CI 1.87–6.36], p < 0.001), after adjustment for age at diagnosis, race, sex, disease stage, tumor size, and year of diagnosis (28).
There was one study that examined the risk of chronic myleoproliferative neoplasms and myelodysplastic syndrome, respectively, in well-differentiated thyroid cancer survivors (27). These outcomes are highly clinically relevant, as chronic myeloid neoplasms may transform to AML, and myelodysplastic syndrome is associated with a poor prognosis (27). Molenaar et al. reported that the rates of chronic myeloproliferative neoplasms and myelodysplastic syndrome with a median follow-up of 6.6 years were: 131I group, 32/68,374 (0.05%) and 35/68,374 (0.05%); no 131I group, 34/79,841 (0.04%) and 42/79,841 (0.05%) (27). The authors reported no significant difference in the median number of years to development of Philadelphia chromosome negative myeloproliferative neoplasms, according to RAI treatment status (no 131I, 8.3; RAI, 4.2; p = 0.18), or myelodysplastic syndrome (no RAI, 5.1; RAI, 4.1; p = 0.54) (27). However, after adjusting for age at diagnosis, sex, and year of diagnosis, and comparing to background population risks in the analyses, the relative risk of developing chronic myeloproliferative neoplasms was 3.1 ([CI 1.1–6.8], p = 0.012) and myelodysplastic syndrome 3.9 ([CI 1.7–7.6], p = 0.0005) in 131I-treated thyroid cancer patients in the second and third year after 131I exposure, respectively, but not significantly elevated in thyroid cancer patients who did not receive 131I (27).
Other SMN outcomes for which sufficient data were available for meta-analysis
Data on the composite outcome of any subsequent hematologic malignancy were reported in four studies (17,21,23,28). In a random-effects meta-analysis examining the risk of any subsequent hematologic malignancy, the risk ratio in RAI-treated TC patients was 1.01 ([CI 0.88–1.16]), and there was no significant heterogeneity of the treatment effect (Q = 0.80, df = 3, p = 0.850, I2 = 0; n = 4 studies, data from 157,055 TC patients, including a total of 823 subsequent hematologic malignancy events). Three studies reported on the outcome of subsequent multiple myeloma (23,26,28), and the pooled relative risk in the RAI-treated group was 0.60 ([CI 0.42–0.86], p = 0.005, with no significant heterogeneity, Q = 0.96, df = 2, p = 0.618, I2 = 0, n = 156). There were 279 thyroid cancer survivors, including a total of 138 subsequent multiple myeloma events, with a mean or median follow-up period varying from 9 (26) to 13 years (23). Data on the outcome of subsequent salivary malignancy was reported in three studies (19,23,26). In a random-effects meta-analysis examining the risk of subsequent salivary gland malignancy, the risk ratio in RAI-treated TC patients was 1.17 [CI 0.59–2.30], also with no significant heterogeneity of the treatment effect (Q = 1.50, df = 2, p = 0.471, I2 = 0; n = 3 studies), with data from 54,850 TC survivors, including a total of 39 subsequent salivary malignancy events.
Discussion
The current systematic review included 17 studies, with three published knowledge syntheses (3,13,14) and 14 original studies (15 –28). Previously published systematic reviews suggested an association between RAI use in TC and increased SMN risk (3,13), although significant heterogeneity was noted in the one meta-analysis, which was limited by having two studies eligible for inclusion at the time (3). One of the published systematic reviews qualitatively suggested a general positive relationship between RAI cumulative activity and SMN risk (13). Yet, one published systematic review/meta-analysis suggested that breast cancer risk was reduced in RAI-treated women (14). The current study found heterogeneous results of overall SMN risks according to RAI treatment status, with a high degree of heterogeneity observed on pooling crude SMN rates. Furthermore, significant heterogeneity was also observed in pooling SMN data that were statistically adjusted for confounders. An important limitation of the included studies examining SMN risk is relatively limited follow-up periods (mean or median 5–16 years), which could limit detection of SMNs with potentially long latency periods. The most commonly reported SMN was breast cancer, and RAI treatment was not associated with this malignancy. Furthermore, the risk of subsequent salivary cancer or the composite outcome of any subsequent hematologic malignancy was not increased. The risk of subsequent leukemia was increased in RAI-treated TC patients compared to TC patients who did not receive RAI in a meta-analysis that included >300,000 patients, although this finding must also be tempered by an understanding of the relative rarity of this event (cumulative incidence rate of 0.08% in the TC patients who did not receive RAI, with a relative risk of 1.6 in the RAI-treated TC patients, yielding an estimated absolute excess risk of 0.05% in RAI-treated patients during subsequent follow-up). In contrast, a reduced risk of subsequent multiple myeloma was observed in RAI-treated TC patients, although this meta-analysis was dominated (94.1% weight) by a large Surveillance, Epidemiology, and End Results study from Molenaar et al. (28). In estimating the absolute risk of subsequent multiple myeloma, the baseline risk in TC patients not treated with RAI was 0.11%, and the relative risk in RAI-treated TC patients was 0.60. So, the percentage of expected fewer subsequent multiple myeloma cases in the RAI-treated TC group was 0.04% compared to TC patients who did not receive RAI during subsequent follow-up. Thus, both subsequent leukemia and multiple myeloma were relatively rare events.
Explanations for these findings are not clear, although some credence is lent to the finding of increased leukemia risk after RAI, with the concurrent observation of increased risk of chronic myeloproliferative neoplasms (which may transform to AML). The observation of a reduced relative risk of multiple myeloma in RAI-treated TC patients certainly requires confirmation, as it is largely based on the findings of one large study (28), and it is possible it could be spurious. Radiation hormesis, which is a theory that purports radiation in “low doses” may stimulate positive biologic effects in some tissues (30), could be considered as an alternative explanation for this finding. One challenge in surmising a protective effect of low-dose radiation in this context is that there were insufficient data available on relative dose to the therapeutic targets and the bone marrow. It may also be speculated that some thyroid cancer patients with subclinical, undiagnosed subsequent multiple myeloma experienced some unintentional therapeutic benefit from 131I treatment. Further research is clearly needed to understand the relationship between RAI treatment and 131I activities with specific SMNs better, including multiple myeloma. Such studies must consider the full spectrum of potential of targeted and off-target outcomes.
Some strengths of this study include the execution of a comprehensive electronic database search (with multiple updates), at least two independent reviews of citations and papers, at least two data abstractions, the inclusion of a meta-analysis adjusted for confounders, and several secondary analyses exploring heterogeneity. Another strength of this study was that the control comparison group consisted of TC patients who did not receive RAI, rather than general population controls. Some limitations of this review include methodological limitations in the primary studies (which may be subject to bias, given their observational nature), relatively limited follow-up periods of included studies (some of which may be unequal between groups), potential publication bias (particularly relating to fewer than expected studies showing a potential positive effect of RAI treatment on SMN outcomes), and limited searching of unpublished literature, lack of measurement of completeness of the electronic searches, lack of more detailed 131I activity data (due to limited data in the primary studies), and lack of data on specifics of preparation for 131I treatment (i.e., thyroid hormone withdrawal or use of rhTSH). A potential limitation is that prediction intervals were not presented (31,32). However, the decision was made not to do so, given that the study sample size was highly variable among included studies (e.g., varying from 413 to 45,978 in crude data analysis for the outcome of any SMN), and recent statistical literature has suggested that performance of prediction intervals may be suboptimal under such conditions (33). Furthermore, the results may not be directly generalizable to pediatric TC populations, as the primary data were largely from adults, and there may be important biologic differences in growing children. The results may also not apply to the use of relatively high 131I dose activities, treatment of genetically predisposed populations, or patients who have undergone prior radiation treatment for other conditions.
In conclusion, this updated systematic review found heterogeneous data on whether RAI use in TC survivors is associated with the outcome of any SMN (compared to no RAI in TC survivors), reflected by a high degree of statistical heterogeneity in both unadjusted and adjusted analyses for the primary outcome. Heterogeneity in the pooled analysis of crude SMN data was partly accounted for by study quality, so it remains largely unexplained. For the most common SMN of breast cancer, the body of evidence did not support an increased risk associated with 131I treatment of TC, although this meta-analysis was also subject to significant heterogeneity. RAI use was associated with an increased risk of subsequent leukemia but reduced risk of subsequent multiple myeloma. Yet, each of these outcomes is relatively rare. The heterogeneity of results within the outcome of any SMN and variability in effects observed among various specific SMNs suggest that it may be preferable for future studies to examine the risks of respective second primary cancers, rather than the composite outcome of any SMN. The findings also suggest that there may be variable biologic effects associated with RAI treatment in different tissues, although confirmatory research is needed. However, particularly for uncommon SMNs, some of which may be subject to long latency periods, very large prospective studies with long term follow-up (i.e., >10 years) are needed. Furthermore, data on RAI cumulative activity (as well as first activity and number of administrations, if applicable), method of preparation for RAI treatment (i.e., rhTSH or thyroid hormone withdrawal), and relevant confounders such as risk factors for specific malignancies should be explicitly reported in order to facilitate understanding of any observed relationships. It is important to note that appropriate RAI treatment of individuals at high risk of thyroid cancer mortality or structural recurrence should not be compromised due to fear of SMNs. The decision as to what 131I activity and which method of stimulation should be used in intermediate- or high-risk patients should take many other factors into consideration.
Footnotes
Acknowledgments
A.M.S. was supported in part by a University of Toronto Department of Medicine Clinician Scientist Merit Award. Library service expenses were funded in part from a University Health Network Thyroid Cancer Research Fund (private charitable donations to the UHN Foundation). The authors would like to thank Mrs. Coreen Marino for assistance in retrieving the full-text papers for reviewThis work was presented in part at the 87th Annual Meeting of the American Thyroid Association in Victoria, Canada, on October 19, 2017 (Poster #97).
Author Disclosure Statement
None declared.