
Abstract
Background:
It is currently uncertain whether primary hypothyroidism is associated with nonalcoholic fatty liver disease (NAFLD). We performed a meta-analysis of relevant studies to quantify the magnitude of association between primary hypothyroidism and risk of NAFLD.
Methods:
We searched PubMed, Web of Science and Scopus databases from January 2000 to March 2018 using predefined keywords to identify observational cross-sectional, case-control, and longitudinal studies in which NAFLD was diagnosed by imaging or biopsy. Data from selected studies were extracted and meta-analysis was performed using random-effects modeling.
Results:
A total of 12 cross-sectional and 3 longitudinal studies enrolling 44,140 individuals were included in the final analysis. Hypothyroidism (defined either by self-reported history of hypothyroidism with use of levothyroxine replacement therapy or by presence of abnormal thyroid function tests) was associated with an increased risk of prevalent NAFLD (n = 12 studies; random-effects odds ratio 1.42 [95% confidence interval (CI) 1.15–1.77]; I 2 = 51.2%), independently of age, sex, body mass index and other common metabolic risk factors. The magnitude of risk paralleled the underlying severity of NAFLD histology (n = 3 studies; random-effects odds ratio 2.73 [CI 1.90–3.93]; I2 = 0%), and tended to increase across the different definitions used for diagnosing hypothyroidism. Meta-analysis of data from the three longitudinal studies showed that subclinical hypothyroidism was not independently associated with risk of incident ultrasound-defined NAFLD over a median of 5 years (random-effects hazard ratio 1.29 [CI 0.89–1.86]; I2 = 83.9%). Sensitivity analyses did not alter these findings. Funnel plot did not reveal significant publication bias.
Conclusions:
This large and updated meta-analysis shows that the presence of variably defined hypothyroidism is significantly associated with the presence and severity of NAFLD. However, the observational design of the eligible studies does not allow for proving causality.
Introduction
N
It is known that the development and progression of NAFLD usually occur in the presence of profound derangements of glucose and lipid metabolism and dysregulation of energy homeostasis (1,3,5). Thyroid hormones are critical regulators of energy homeostasis and have prominent direct effects on glucose and lipid metabolism (9). To date, several observational studies have explored the association between primary subclinical/overt hypothyroidism and imaging-defined or biopsy-proven NAFLD (10 –24). However, the findings from such studies have been conflicting so far, with some studies reporting that the prevalence of primary hypothyroidism, especially subclinical hypothyroidism, was extremely common among patients with NAFLD (occurring in up to 20–25% of these patients) (10,12), while other studies failing to find any significant association between hypothyroidism and risk of NAFLD (14 -18). This finding raised concern as to whether subclinical hypothyroidism could be associated with an increased risk of NAFLD. Although two previous small meta-analyses have further explored this question, they had important methodological limitations (e.g., pooling of cross-sectional and longitudinal studies; very high heterogeneity and significant publication bias of results) and did not consider much of the currently available evidence (i.e., studies published in 2017 and 2018), thus providing controversial and inconclusive findings (25,26). On this background of evidence, it still remains uncertain whether subclinical hypothyroidism is a risk factor for NAFLD.
We therefore carried out a systematic review and meta-analysis of observational cross-sectional and longitudinal studies examining the association between primary hypothyroidism and NAFLD. The major aim of this meta-analysis was to determine whether and to what extent variably defined primary hypothyroidism was associated with the risk of NAFLD. We also examined whether there was a significant association between primary hypothyroidism and the severity of NAFLD histology.
Methods
Registration of review protocol
The protocol for this systematic review and meta-analysis was registered in advance with PROSPERO (International Prospective Register of Systematic Reviews, No. CRD42018091285).
Data sources and searches
We conducted a systematic literature search from January 1, 2000, to March 1, 2018, of PubMed, Scopus, and Web of Science for all observational studies examining the association between primary hypothyroidism and NAFLD. Search free text terms were “hypothyroidism” OR “subclinical hypothyroidism” OR “thyroid dysfunction” AND “nonalcoholic fatty liver disease” (OR “fatty liver” OR “NAFLD”). Searches were restricted to human studies. No language restrictions were imposed. Additionally, we reviewed references from relevant original papers and review articles to identify further eligible studies not covered by the original database searches. We performed a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Because the included studies were observational in design, we followed the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines for the meta-analysis of these studies (27).
Study selection
The inclusion criteria of the meta-analysis were as follows: (1) observational cross-sectional, case-control, or longitudinal (prospective or retrospective) studies that explored the association between primary hypothyroidism and NAFLD; (2) all studies should report odds ratios (ORs) or hazard ratios (HRs) with 95% confidence interval [CI] values for the outcome of interest; (3) the diagnosis of NAFLD was based on either liver biopsy or imaging techniques (mostly ultrasonography), in the absence of excessive alcohol consumption and other competing causes of chronic liver disease; and (4) the diagnosis of primary hypothyroidism was either based on a self-reported history of hypothyroidism with use of levothyroxine replacement therapy or based on measurement of serum thyrotropin (TSH) and free thyroxine (fT4) levels for identifying those individuals with newly diagnosed subclinical or overt hypothyroidism. Subclinical primary hypothyroidism was defined as presence of elevated TSH with fT4 levels within the reference range, whereas overt hypothyroidism was defined as elevated TSH with low circulating fT4 levels. Study participants included in the meta-analysis were of either sex without any restriction in terms of age, race or ethnicity.
Criteria for exclusion of the selected studies from this meta-analysis were as follows: (1) congress abstracts, case reports, theses, reviews, practice guidelines, commentaries, and editorials; (2) studies where NAFLD diagnosis was based exclusively on serum liver enzyme levels or other surrogate markers of NAFLD (e.g., fatty liver index); (3) studies that did not exclude individuals with excessive alcohol consumption and other known causes of chronic liver disease; and (4) studies that did not specifically report any OR or HR and 95% CIs for the outcome measure of interest.
Two investigators (A.M. and G.T.) independently examined all titles and abstracts and obtained full texts of potentially relevant papers. Working independently and in duplicate, we read the papers and determined whether they met inclusion criteria. Discrepancies were resolved by consensus, referring back to the original article in consultation with a third author.
Data extraction and quality assessment
For all studies, we extracted information on study design, study size, publication year, study country, participants characteristics, definition of primary hypothyroidism, methods used for NAFLD diagnosis, histological severity of NAFLD, follow-up duration, outcome of interest, and covariates adjusted in multivariate regression analyses. In the case of multiple publications, we included the most up-to-date or comprehensive information.
Two investigators (A.M. and G.T.) assessed the risk of bias independently. Any discrepancies were addressed by a reevaluation of original articles by a third author. Quality assessment was performed according to the Newcastle-Ottawa Quality Assessment Scale (NOS), which is a validated scale for non-randomized studies in meta-analyses (28). We used a NOS scale adapted for the cross-sectional studies (28). The NOS scale uses a star system to assess the quality of a study in three domains: selection, comparability, and outcome/exposure. The NOS assigns a maximum of four stars for selection (or five stars in the case of cross-sectional studies), two stars for comparability, and three stars for outcome/exposure. We judged studies that received a score of at least eight stars to be at low risk of bias (i.e., thus reflecting the highest quality).
Data synthesis and analysis
The outcome measure was the presence (or the occurrence over the follow-up for longitudinal studies) of either imaging-defined or biopsy-proven NAFLD. The ORs (for cross-sectional studies) or HRs (for longitudinal studies) and 95% CIs were considered as the effect size for all the eligible studies. When studies had several adjustment models, we extracted those that reflected the maximum extent of adjustment for potentially confounding variables.
The adjusted OR/HRs of all eligible studies were pooled, and an overall estimate of effect size was calculated using a random-effects model, as this methodology considers any differences between studies even if there is no statistically significant heterogeneity.
Visual inspection of the forest plots was used to investigate the possibility of statistical heterogeneity. The statistical heterogeneity among studies was assessed by the I 2 statistic, which provides an estimate of the percentage of variability across studies that is due to heterogeneity rather than chance alone. According to Higgins and Thompson (29), a rough guide to interpretation is as follows: I 2 values of approximately 25% represent low heterogeneity; approximately 50% represent medium heterogeneity; and approximately 75% represent high heterogeneity.
The possibility of publication bias was evaluated using the funnel plot and the Egger's regression asymmetry test (30).
To explore the possible sources of the (expected) heterogeneity among the eligible studies and to test the robustness of the associations, we conducted stratification-sensitivity analyses by the study design, the age population, the study country, the definition used for establishing the presence of hypothyroidism, the methods used for NAFLD diagnosis, the severity of NAFLD histology (NASH ± advanced fibrosis vs. no-NASH), whether the studies had eight or nine stars on the NOS scale (i.e., the “high-quality” studies), or whether they had full adjustment for known risk factors (i.e., those studies adjusting at least for age, sex, body mass index, diabetes, or metabolic syndrome). We also tested for possibly excessive influence of individual studies using a meta-analysis influence test that eliminated each of the included studies at a time.
All statistical tests were two-sided and used a significance level of p < 0.05. We used STATA® 14.2 (StataCorp, College Station, Texas) for all statistical analyses.
Results
Literature search and study characteristics
Supplementary Figure S1 (Supplementary Data are available online at
In total, fifteen observational studies were eligible for inclusion in the meta-analysis and were assessed for quality (10 –24). The main characteristics of the included studies are shown in Table 1. These studies recruited both adults (n = 13 studies) and overweight/obese children or adolescents (n = 2 studies). The diagnosis of NAFLD was based on liver biopsy (n = 3 studies), ultrasonography (n = 11 studies) or computed tomography (n = 1 study), in the absence of excessive alcohol consumption and other competing causes of chronic liver disease. The diagnosis of primary hypothyroidism was either based on a self-reported history of hypothyroidism with use of levothyroxine replacement therapy (n = 2 studies where the large majority of patients were euthyroid) or based on serum TSH/fT4 measurements (n = 13 studies). Approximately half of the included studies were carried out in Asia (n = 7 studies from China, Iran, Philippines and South Korea); five studies were carried out in Europe (Germany, Italy, Netherlands and Sweden), and three studies were carried out in the Unites States (n = 2 studies) or Mexico. Most of these studies included adult individuals (median age, 45 years), predominantly of female sex. Twelve studies had a cross-sectional or case-control design, whereas three studies had a longitudinal design.
Data ordered by publication year and by age population.
Degree of adjustment: 0, unadjusted; +, adjusted for age, sex, and BMI; ++, further adjustment for diabetes, dyslipidemia, and hypertension; +++, further adjustment for other potential risk factors (including waist circumference).
aHR, adjusted hazard ratio; aOR, adjusted odds ratio; BMI, body mass index; CI, 95% confidence interval; fT3, free triiodothyronine; fT4, free thyroxine; HDL, high-density lipoprotein; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; TSH, thyrotropin; uOR, unadjusted odds ratio.
Overall, in the 15 studies included in the meta-analysis there were 44,140 individuals with a total of 6067 subjects with primary hypothyroidism and 7810 subjects with NAFLD. In particular, in the twelve cross-sectional studies, there were 15,523 individuals with a total of 3720 subjects with primary hypothyroidism and 4149 subjects with imaging-defined or biopsy-proven NAFLD. In the three longitudinal studies, there were 28,617 adult individuals (2347 with hypothyroidism) with a total of 3661 new cases with incident NAFLD (assessed by ultrasonography) occurring over a median follow-up period of 5 years.
Of the twelve included cross-sectional studies (Supplementary Table S2), two studies received at least eight stars on the NOS (indicating that those studies had a low risk of bias), five studies received seven stars, and the remaining five studies received six stars or less (i.e., being at high risk of bias). Conversely, among the three longitudinal studies two studies received eight stars, whereas one study received seven stars on the NOS.
Hypothyroidism and risk of prevalent NAFLD
The distribution of the twelve cross-sectional studies (involving a total of 15,523 individuals) by estimate of the association between hypothyroidism and risk of NAFLD is plotted in Figure 1.

Forest plot and pooled estimates of the effect of variably defined primary hypothyroidism (defined as either self-reported use of levothyroxine replacement therapy or abnormal levels of serum thyroid stimulating hormone and/or free thyroxine) on the risk of prevalent nonalcoholic fatty liver disease (NAFLD) in 12 eligible cross-sectional studies.
Presence of variably defined hypothyroidism was significantly associated with an increased risk of prevalent NAFLD (random-effects OR 1.42 [CI 1.15–1.77]; I 2 = 51.2%). As we have always used the fully adjusted OR estimates for each eligible study (as specified in Table 1), in most of the included studies this random-effects OR was independent of age, sex, BMI and common metabolic risk factors.
Hypothyroidism and risk of severe NAFLD
The distribution of studies by estimate of the association between hypothyroidism and the severity of NAFLD is plotted in Figure 2. Three cross-sectional or case-control studies (involving a total of 1717 U.S. or South Korean adults) provided data suitable for the pooled primary analysis (10,12,22). In these studies, the diagnosis of NAFLD was always confirmed by liver biopsy; in particular, the outcome measure was the presence of histological NASH in two studies, and histological advanced fibrosis in a single study. The diagnosis of primary hypothyroidism was based on a self-reported history of hypothyroidism with use of levothyroxine replacement therapy in two studies and based on the presence of subclinical hypothyroidism in a single study. No data were available about the effect of newly diagnosed overt hypothyroidism on the histological severity of NAFLD.
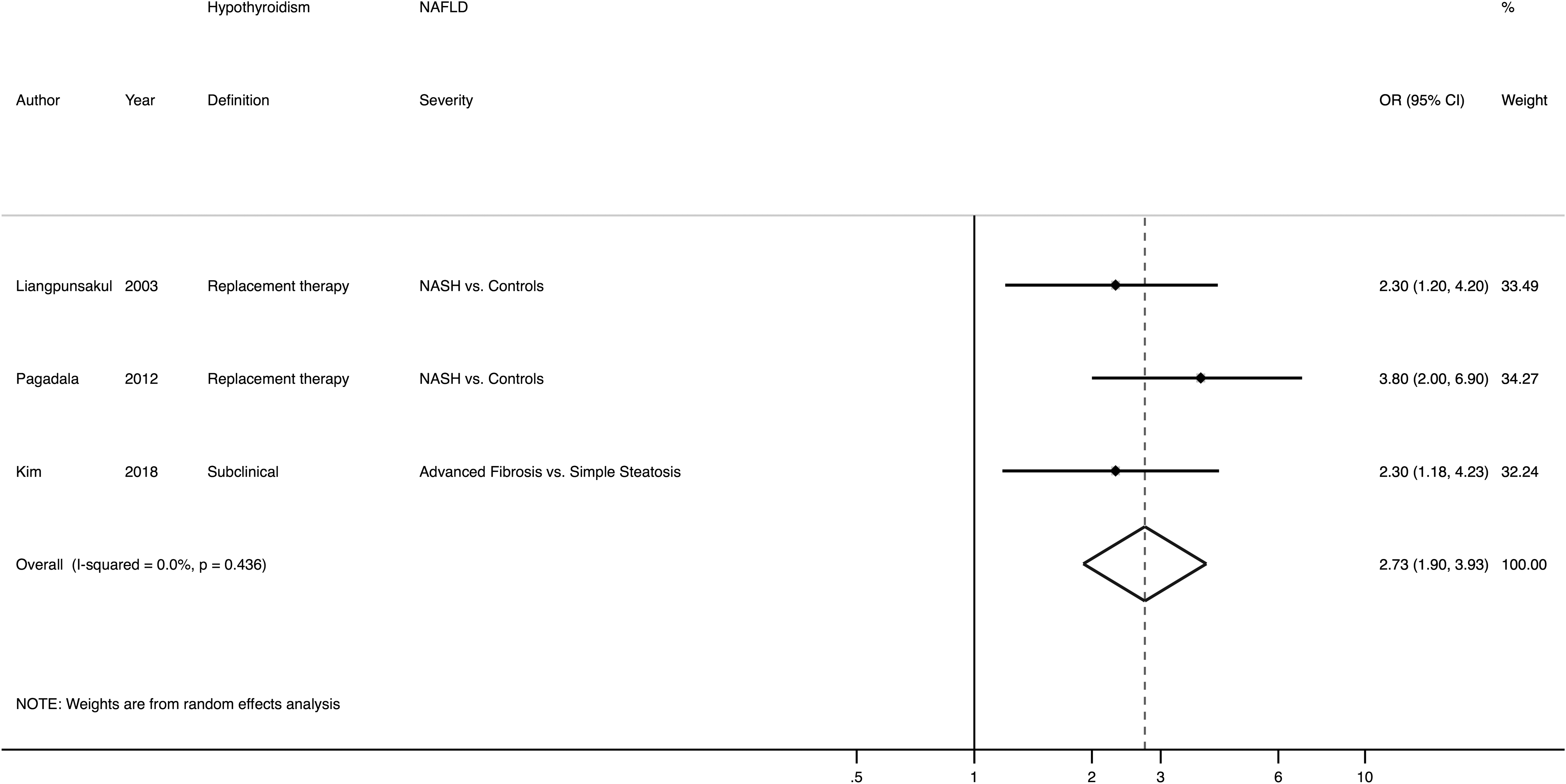
Forest plot and pooled estimates of the effect of variably defined primary hypothyroidism on the severity of NAFLD on liver histology in three eligible cross-sectional studies.
Overall, the presence of variably defined hypothyroidism was associated with a 2.7-fold higher risk of prevalent NASH or advanced fibrosis (random-effects OR 2.73 [CI 1.90–3.93]; I 2 = 0%). This association was independent of age, sex, BMI, diabetes, or other common metabolic risk factors.
Hypothyroidism and risk of incident NAFLD
The distribution of longitudinal studies by estimate of the association between hypothyroidism and risk of incident NAFLD is plotted in Figure 3. Three longitudinal studies (involving a total of 28,617 adult individuals from China, South Korea, or the Netherlands) provided data suitable for the pooled primary analysis (15,19,20). In these studies, the diagnosis of hypothyroidism was based exclusively on abnormal thyroid function tests (mainly identifying those individuals with subclinical hypothyroidism), whereas the development of incident NAFLD over a median period of 5 years was detected using ultrasonography in all participants (n = 3661 cases of incident NAFLD).
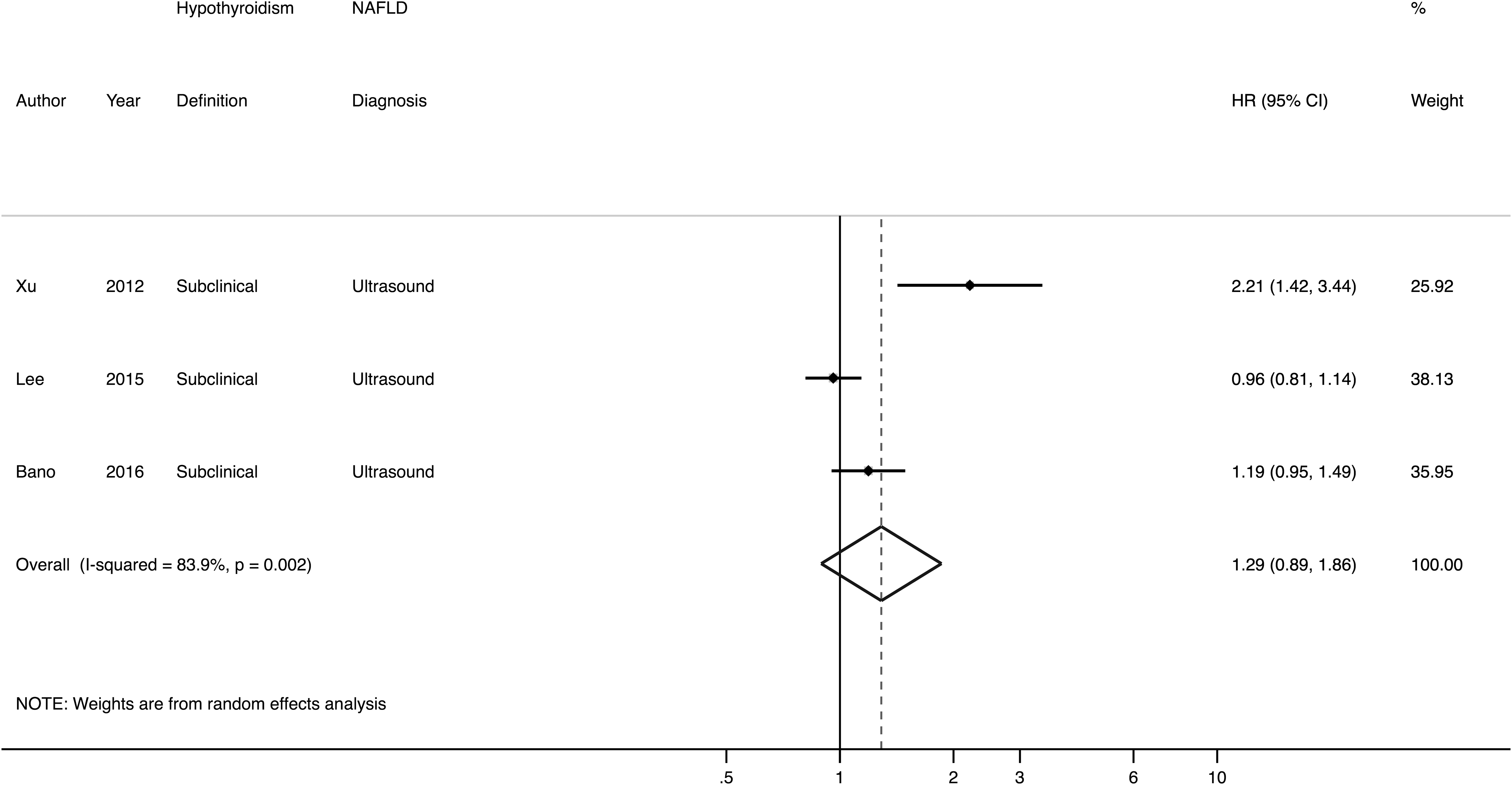
Forest plot and pooled estimates of the effect of subclinical primary hypothyroidism (defined as elevated serum thyroid stimulating hormone with normal free thyroxine levels) on the risk of developing incident NAFLD (detected by ultrasonography) over a median follow-up period of five years in three eligible longitudinal studies.
Overall, the presence of subclinical hypothyroidism was not significantly associated with an increased risk of incident ultrasound-diagnosed NAFLD (random-effects HR 1.29 [CI 0.89–1.86]; I 2 = 83.9%) even after controlling for age, sex, BMI, diabetes, or other known metabolic risk factors. No sufficient data were available in the eligible studies to test the effect of overt hypothyroidism on the development of incident NAFLD. However, it should be noted that in the cohort study of Bano et al. (20) both subclinical hypothyroidism (adjusted OR 2.14 [CI 1.04–4.07]) and overt hypothyroidism (adjusted OR 6.64 [CI 1.04–23.9]) were independently associated with an increased risk of developing NAFLD with varying levels of hepatic fibrosis (as assessed by vibration-controlled transient elastography).
Subgroup/sensitivity analyses and meta-regression
To explore possible sources of heterogeneity across the included studies, we carried out several sensitivity analyses (Table 2).
Data stratified by category of Newcastle-Ottawa quality assessment scale, degree of covariate adjustment, diagnostic methods for NAFLD, definition of primary hypothyroidism, study country, and age population.
Degree of covariate adjustment: 0, unadjusted; +, adjusted for age, sex, and BMI; ++, further adjustment for diabetes, dyslipidemia, and hypertension; +++, further adjustment for other potential risk factors.
NOS, Newcastle-Ottawa quality assessment scale.
Limiting the analysis to “high-quality” studies with NOS ≥8 stars or those with full adjustment for covariates provided overall estimates consistent with the pooled primary analysis for both cross-sectional and longitudinal studies.
When the comparison was stratified by methods used for diagnosing NAFLD, the significant association between variably defined hypothyroidism and NAFLD was consistent both for cross-sectional studies using biopsy (n = 3 studies) and for cross-sectional and longitudinal using liver ultrasonography or computed tomography (n = 12 studies).
When the comparison was stratified by the criteria used for identification of hypothyroidism, the significant association between primary hypothyroidism and NAFLD was consistent for both cross-sectional studies using the self-reported history of hypothyroidism with use of levothyroxine replacement therapy (n = 2 studies) and cross-sectional or longitudinal studies using serum TSH/fT4 measurements as diagnostic criterion for identifying newly diagnosed subclinical and overt hypothyroidism (singly or in combination) and also tended to increase across the different definitions of hypothyroidism (with the greatest random-effects ORs in patients taking levothyroxine replacement therapy, intermediate in patients with overt hypothyroidism, and lowest in those with subclinical hypothyroidism).
Finally, when the comparison was stratified either by study country or by age population, the significant association between variably defined hypothyroidism and risk of NAFLD was consistent both for both adults and overweight or obese children/adolescents, whereas it seemed to be (slightly) stronger in U.S./European populations compared with Asian populations. No longitudinal studies were available for this subgroup analysis in pediatric populations.
We also tested for the possibility of excessive influence of individual studies using an influence test that eliminated each of the included studies one at a time. Eliminating each of the eligible studies from the analysis had no significant effect on the overall risk of NAFLD (data not shown).
In Supplementary Figure S2 we reported the results of univariable meta-regression analyses showing the lack of any significant association of age, sex, or BMI with the risk of prevalent NAFLD in the eligible cross-sectional studies.
As shown in Supplementary Figure S3, the Egger's regression test did not show statistically significant asymmetry of the funnel plots, thus suggesting that publication bias was unlikely, although it should be noted that the number of included studies (n = 15) was relatively small.
Discussion
Our meta-analysis involves a total of 15 observational studies using either liver biopsy or imaging techniques (mostly ultrasonography) to diagnose NAFLD with aggregate data on 44,140 individuals, nearly 14% of whom who were either taking levothyroxine replacement therapy or had subclinical or overt hypothyroidism. Meta-analysis of data from the twelve cross-sectional studies has shown that the presence of variably defined hypothyroidism was associated with a 42% increased risk of imaging-defined or biopsy-proven NAFLD. This risk tended to increase across the different definitions used for diagnosing hypothyroidism (i.e., a self-reported history of hypothyroidism with use of levothyroxine replacement therapy > newly-diagnosed overt biochemical hypothyroidism > newly-diagnosed subclinical hypothyroidism), and appeared to further increase with greater severity of NAFLD (reaching a risk of almost three times greater in the presence of NASH or advanced fibrosis on liver histology) and, most importantly, remained significant in those studies where analysis was fully adjusted for age, sex, BMI, diabetes, or other common metabolic risk factors. Conversely, meta-analysis of data from the three longitudinal studies has shown that subclinical hypothyroidism was not independently associated with the risk of incident NAFLD (assessed by ultrasonography) over a median follow-up of 5 years. It should be noted that, as expected, no sufficient data were available in most of the eligible studies to examine the effect of newly diagnosed overt hypothyroidism on the risk of incident NAFLD.
Our meta-analysis exploring the association between variably defined primary hypothyroidism and the risk of NAFLD is the largest and most comprehensive assessment to date. Two previous smaller meta-analyses have yielded controversial findings (25,26]. One meta-analytic study of nine studies (involving a total of ∼32,000 subjects) showed that patients with NAFLD had no significant differences in serum thyroid hormone levels compared with control individuals and that there was no significant association between variably defined primary hypothyroidism and NAFLD (random-effects OR 1.21 [CI 0.91–1.61]; I 2 = 72%) (25). Compared with our meta-analysis, the authors have included six identical studies to those included in our meta-analysis (11,13,14,16,18,19), but also three cross-sectional studies (31 –33) that we have excluded for the reasons specifically reported in supplementary Table 1. In addition, they did not include studies performed in adolescents (23,24), and cross-sectional or longitudinal studies published in adults from 2016 to 2018 (20 –22). Conversely, in the other published meta-analysis of 13 cross-sectional and longitudinal studies (involving a total of ∼41,000 subjects), He et al. reported a significant association between variably defined primary hypothyroidism and the risk of NAFLD (random-effects OR 1.52 [CI 1.24–1.87]; I 2 = 75.1%) (26). Compared with our meta-analysis, these authors have included eleven studies identical to those included in our meta-analysis (10–13,15–17,19,20,23,24), but also an unpublished M.D. thesis and a case-control study conducted in India (31) that we have excluded from the pooled primary analysis (Supplementary Table S1), because it provided extraordinarily high ORs (adjusted OR 14.9 [CI 3.5–63] for the association between hypothyroidism and NAFLD. Moreover, the authors did not include in their meta-analysis the studies by Zhang et al. and Ludwig et al. (14,18) as well as some other cross-sectional studies published from 2017 to 2018 (21,22).
For the aforementioned reasons, we believe that the findings of these two previous meta-analyses should be interpreted cautiously, especially because they have important methodological limitations (combining, for example, the results of both cross-sectional and longitudinal studies within the same pooled primary analysis; including a number of studies of very low quality according to the NOS scale; not performing extensive sensitivity analyses to explore possible sources of heterogeneity) and did not consider much of the currently available evidence (mainly the studies published in 2017 and 2018, which we have included in our meta-analysis). As a result of these methodological limitations, it should also be noted that in both meta-analyses there was a very high degree of heterogeneity (I 2 ≥ 72%) for the pooled primary analysis, and the visual inspection of the funnel plots showed the presence of significant publication bias (25,26).
Compared with these two previous meta-analyses, we have included some new observational studies published in 2017 and 2018 (as specified above) and conducted more thorough statistical analyses. As a result of this methodological effort, our meta-analysis provides strong evidence that the presence of variably defined hypothyroidism is significantly associated with a 42% increased risk of prevalent NAFLD (random-effects OR 1.42 [CI 1.15–1.77]; I 2 = 51.2%); moreover, we also show that this risk is consistent both for studies using the self-reported history of hypothyroidism with use of levothyroxine replacement therapy and for those using serum TSH/fT4 measurements as diagnostic criteria for diagnosing hypothyroidism. No sufficient data were available in the eligible studies to examine the effect of overt hypothyroidism on risk of incident NAFLD.
Notably, our meta-analysis is first in suggesting that the presence of variably defined hypothyroidism is associated with a 2.7-fold higher risk of prevalent NASH or advanced fibrosis on liver histology (n = 3 studies included; random-effects OR 2.73, 95% CI 1.90-3.93; I 2 = 0%), independently of age, sex, BMI, or other common metabolic risk factors. In addition, performing separate meta-analytic analyses for longitudinal studies (n = 3 studies totaling nearly 29,000 individuals), we show for the first time that the presence of subclinical hypothyroidism is not independently associated with the risk of incident NAFLD (detected by ultrasonography) over a median follow-up of 5 years (random-effects HR 1.29, 95% CI 0.89-1.86; I 2 = 83.9%). However, on the basis of the available studies, it is likely that this finding could be due to the lack of adequate statistical power, and that larger (n > 10,000 individuals) prospective cohort studies with longer follow-up periods (≥10 years) will be needed to better elucidate this important topic.
That said, we believe that the findings of our meta-analysis strongly support the notion that variably defined primary hypothyroidism is significantly associated with NAFLD, and may also have clinical practice implications for the potential screening of hypothyroidism and NAFLD. Indeed, these findings suggest that individuals with NAFLD should probably be screened for primary hypothyroidism; and that NAFLD should be looked for in patients with hypothyroidism, given that these patients are at higher risk of NASH and advanced fibrosis.
A detailed description of the multifactorial pathogenesis involved in the hypothyroidism-induced NAFLD is beyond the scope of this meta-analysis. To date, there is convincing evidence of biological plausibility that overt hypothyroidism can promote NAFLD development through multiple extrahepatic (systemic) and intrahepatic mechanisms. Indeed, hypothyroidism can induce NAFLD through the systemic development of metabolic disorders, low-grade inflammation, and increased oxidative stress. Moreover, thyroid hormones also have direct effects on hepatic glucose and lipid metabolism (9,34,35).
In addition to the adverse effects of decreased serum thyroid hormones on hepatic glucose and lipid metabolism, it is also possible that elevated serum TSH per se could promote the development of NAFLD by stimulating hepatic de novo lipogenesis (36). Additionally, the intrahepatic thyroid hormone concentration and/or thyroid hormone signaling could be decreased in the livers of patients with NAFLD (37 –39). Recent advances in areas such as cell imaging, autophagy and metabolomics have also generated a more detailed picture of thyroid hormone–mediated regulation of hepatic lipid metabolism at the molecular level (9). Given these potentially beneficial effects on lipid metabolism, it is possible that thyroid hormone analogues or mimetics could be useful for the treatment of metabolic diseases involving the liver, such as dyslipidemia and NAFLD (9,35). In a recent phase 2b single arm trial, it has been reported that low dose levothyroxine significantly reduced hepatic fat content (assessed by magnetic resonance spectroscopy) in euthyroid patients with type 2 diabetes and NAFLD (40). A multicenter, double-blinded, randomized, placebo-controlled phase 2 trial is also ongoing to evaluate the efficacy and safety of MGL-3196 (i.e., a highly selective liver-directed, thyroid hormone receptor-β agonist) in patients with biopsy-proven NASH.
Our meta-analysis has some important limitations (strictly inherent to the design of the included studies) that should be mentioned. First, the observational design of the (cross-sectional and longitudinal) studies does not allow establishing temporal or causal relationships between hypothyroidism and NAFLD. Second, although the large majority of the included studies have adjusted the results at least for age, sex, BMI, and diabetes (or metabolic syndrome), the possibility of residual confounding by some unmeasured factors cannot be ruled out. Third, the studies included in the meta-analysis used various definitions of primary hypothyroidism (ranging from a self-reported history of hypothyroidism with the use of levothyroxine replacement therapy to abnormal levels of thyroid function tests with variably different TSH laboratory cutoffs for diagnosing subclinical hypothyroidism). In particular, in the meta-analysis there were two cross-sectional studies that defined the presence of “hypothyroidism” as a self-reported use of levothyroxine replacement therapy. It is likely that the large majority of these patients were euthyroid. Indeed, as also reported in Table 1, in the study by Pagadala et al. the mean TSH levels of these patients were within the reference range (12). Conversely, no data on serum TSH levels were available for the study by Liangpunsakul et al. (10).
Another limitation of the meta-analysis is that serum levels of TSH and fT4 were not serially monitored, and that levels of thyroid antibodies were not consistently measured in all studies [except for the study by Bano et al. (20), who measured serum TPO antibodies but did not find any significant association between levels of TPO antibodies and risk of incident NAFLD]; hence, the cause of hypothyroidism is not clear. A potential limitation of the meta-analysis is that most of the eligible studies used liver ultrasonography, which has a good sensitivity (∼85%) and specificity (∼95%) for detecting mild-to-moderate steatosis compared with liver histology (i.e., when at least 20–30% of hepatocytes are steatotic on biopsy), but it is not sensitive enough to detect milder degrees of steatosis (2,41 –43), whereas only a minority of the eligible studies used biopsy, which is the reference standard for diagnosing and staging NAFLD (2,3). In this regard, the available data supporting a significant, graded relationship between hypothyroidism and the histological severity of NAFLD are derived from three, though large, cross-sectional studies (10,12,22). However, it should be noted that longitudinal studies with adequate histological endpoints were not available for this analysis, thus limiting the generalizability of these findings. Nevertheless, it should also be pointed out that both subclinical and overt hypothyroidism were independently associated with an increased 10-year risk of developing incident NAFLD with clinically significant hepatic fibrosis (assessed by vibration-controlled transient elastography, Fibroscan®) in a large population-based cohort of elderly Dutch individuals (20).
We believe that future larger prospective studies, possibly using magnetic resonance-proton density fat fraction and magnetic resonance-based elastography (which are rapidly being recognized as being as good as liver biopsies) (2,44) will be needed to better elucidate whether subclinical hypothyroidism increases risk of developing incident NAFLD. Another important limitation of the meta-analysis is that although we found a medium level of heterogeneity (I 2 = 51.2%) for the pooled primary analysis of cross-sectional studies, the overall quality of these studies was relatively low, suggesting a medium-high risk of bias according to the NOS scale. In contrast, although the quality of the three longitudinal studies was relatively high on the NOS scale, the level of heterogeneity was high (I 2 = 83.9%) for the pooled primary analysis of these studies. We systematically explored and identified possible sources of statistical heterogeneity using stratified analyses, meta-regression, and sensitivity analyses. However, we believe that more detailed analyses of the causes of heterogeneity will require collaborative pooling of individual participant data from large prospective studies as these become available over time. Finally, although a selective reporting bias of eligible studies could be not definitely excluded, we also searched for grey literature in Scopus and Web of Science databases and made every effort to rule out very low-quality studies by using stringent inclusion criteria. We believe that our comprehensive search has made it unlikely that any published reports were missed, and visual inspection of funnel plots and formal tests demonstrated no statistical evidence of publication bias.
Notwithstanding these limitations, our meta-analysis has several important strengths. As previously discussed, the present meta-analysis provides the most comprehensive assessment to date on the association between variably defined primary hypothyroidism and risk of prevalent and incident NAFLD. Additionally, we employed standardized risk estimates from all eligible studies to allow a consistent combination of estimates across studies. The large number of individuals with NAFLD or hypothyroidism has provided high statistical power to quantitatively assess the magnitude of the association between hypothyroidism and risk of NAFLD. It should be noted that none of the included studies have examined the effect of levothyroxine replacement therapy when exploring the risk of NAFLD in patients with subclinical or overt hypothyroidism. A post hoc analysis of a randomized controlled trial recently showed that levothyroxine replacement therapy for 15 months had beneficial effects on both serum liver enzyme levels and ultrasound-diagnosed NAFLD among patients with subclinical hypothyroidism (45). More clinical trials with histological liver endpoints are needed to better examine the possible benefits of levothyroxine replacement therapy on NAFLD.
In conclusion, this comprehensive meta-analysis of observational studies provides evidence for a significant and independent association between variably defined primary hypothyroidism and the presence and severity of imaging-defined or biopsy-proven NAFLD. However, it remains also uncertain whether subclinical hypothyroidism independently predicts the development of incident NAFLD. It should be noted that the temporal relationship between liver and thyroid diseases is not clear, and that a causal relationship between NAFLD and primary hypothyroidism cannot be definitely established. Further large and well-designed prospective studies to confirm these findings should be undertaken, and mechanistic studies to better elucidate the mechanisms underlying the association between hypothyroidism and NAFLD are also warranted.
Footnotes
Acknowledgments
We would like to thank Dr. A. Bano and L. Chaker (Erasmus Medical Center, Rotterdam), who have kindly provided extra information to us on their study included in the meta-analysis.
G.T. is supported in part by grants from the University School of Medicine of Verona, Verona, Italy.
Author Disclosure Statement
No competing financial interests exist.