
Abstract
Background:
Active surveillance has been introduced as a management option for low-risk papillary thyroid microcarcinoma (PTMC) due to its mostly indolent course.
Methods:
This was a multicenter study of 370 PTMC patients who underwent active surveillance more than one year. The changes in volume and maximum diameter between initial and last ultrasonography were evaluated to identify the natural course of PTMC during active surveillance.
Results:
Patients' age at diagnosis was 51 ± 12 years, and 110 (30%) patients were <45 years of age. The initial maximum diameter and volume of PTMCs were 5.9 ± 1.7 mm and 81.0 ± 77.7 mm3, respectively. During the median 32.5 months of follow-up, 86 (23.2%) patients were found to have an increase in tumor volume, and 13 (3.5%) patients showed an increase in the maximal diameter of the tumor. The cumulative incidence of volume increase gradually rose with time (6.9%, 17.3%, 28.2%, and 36.2% after two, three, four, and five years, respectively). The risk of volume increase in patients <45 years of age was twice as high as in older patients (p = 0.002). There was no significant difference in tumor size change according to sex, levothyroxine treatment, or presence of Hashimoto's thyroiditis. During the period, 58 (15.7%) patients underwent delayed thyroid surgery due to anxiety (37.9%), tumor size increase (32.8%), or appearance of cervical lymph node metastasis (8.6%). Lymph node metastasis was found in 29.3% of patients on pathological examination.
Conclusions:
A significant number of PTMCs grow during active surveillance, and tumor volume change is a more sensitive means of evaluating tumor growth. Active surveillance can be carefully applied for selected patients. Although it is not contraindicated, it should be applied more cautiously for younger patients.
Introduction
A
Previous Japanese studies have evaluated tumor size increase using the maximal increase in diameter ia mm as the criterion, which is now regarded as a surgical indication during active surveillance (4 –6). However, recent studies suggest that determination of the three-dimensional volume is a more sensitive marker of PTMC growth (7,8). Although its clinical significance has not yet been evaluated, the measurement of tumor volume should allow early detection of PTMC growth during active surveillance.
Knowledge of the clinically relevant factors for the prediction of tumor growth is important. Recently, Brito et al. proposed useful recommendations for the selection of candidates for active surveillance based on the characteristics of the tumor, patient, and medical team (9). Little research has been conducted regarding the ideal candidate or how to manage the patient during the active surveillance period. However, a few studies suggest that young age and ultrasonographic features could be associated with tumor growth during active surveillance (10,11).
This study evaluated the natural course of low-risk PTMCs during active surveillance by evaluating three-dimensional changes in structure by neck ultrasonography (US) in a multicenter cohort in Korea. It also evaluated the clinically relevant factors associated with tumor growth during active surveillance.
Methods
Study population
This multicenter, retrospective cohort study included 370 patients who were cytopathologically diagnosed with PTMC and then underwent active surveillance, rather than immediate thyroid surgery, for more than a year between 2002 and 2017 in three tertiary referral centers in Korea: Asan Medical Center (AMC), Samsung Medical Center (SMC), and Seoul St. Mary's Hospital (SMH). Initially, 383 patients were screened, but 13 patients were excluded from the study because they were followed for less than a year or because of a lack of clinical data. Patients underwent active surveillance for the following reasons: (i) the patient's own decision after detailed discussion with the attending physician between surgical intervention and active surveillance, (ii) the presence of other underlying malignancies, (iii) a high risk of general anesthesia due to a cardiopulmonary problem, (iv) the presence of other uncontrolled systemic comorbidities, or (v) pregnancy. Patients with clinical evidence of cervical lymph node (LN) metastasis or any evidence of macroscopic invasion into the perithyroidal soft tissue, trachea, or recurrent laryngeal nerve on initial US, or those with distant metastasis or a diagnosis of an aggressive variant of PTMC by fine-needle aspiration cytology (FNAC) or core-needle biopsy (CNB) were initially excluded. The study protocol was approved by the Institutional Review Board of each institution (AMC: 2018-0354; SMC: 2018-02-079; and SMH: KC16OISI0414).
Study design and definitions
The study aimed to evaluate the natural course of PTMC and the clinically relevant factors associated with tumor growth during active surveillance. Tumor growth was evaluated by assessing changes in both volume and maximum diameter between the initial and final US. Volume change was calculated using the following equation: [final volume (mL) − initial volume (mL)] × 100/initial volume (mL) (1). Volume increase was defined as an increase of ≥50%, and maximum diameter increase was defined as an increase of ≥3 mm (1,12). Patients with tumor volume increase were placed in an “increasing” group, and others were placed in a “stable” group.
Hashimoto's thyroiditis was defined by a serum antithyroid peroxidase antibody level over each institutional cutoff, or by the presence of diffuse parenchymal heterogeneity on US.
Neck US and diagnosis of PTMC
All PTMC nodules were ≤10 mm in size on initial US and were cytopathologically diagnosed as suspicious for malignancy or malignant (13,14). Images of the thyroid gland and neck area were evaluated with the following US equipment: an iU22 unit (Philips Healthcare, Bothell, WA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) with a 5–14 MHz transducer at AMC, an HDI 5000 (Advanced Technology Laboratories, Bothell, WA) or a LOGIQ700 ultrasound scanner (GE Medical Systems, Milwaukee, WI) with a 12–50 MHz transducer at SMC, and a LOGIQ S6 (GE Medical Systems, Chicago, IL) with a 3.5–11 MHz transducer at SMH. The scanning protocol in all cases included both transverse and longitudinal real-time imaging of thyroid nodules. Neck US examinations were performed and were retrospectively reviewed by experienced radiologists or endocrinologists in each center. Radiologists or endocrinologists in the groups are trained as previously reported to minimize inter-observer variation (15). In the measurements of PTMC with coarse calcifications, the depth on the initial US was measured as a reference, and subsequently the diameter along the same contour was measured as similar as possible as in the initial US. PTMC was diagnosed with US-guided FNAC or CNB, according to published criteria (16,17).
Cytopathologic diagnoses were made by a pathologist experienced in thyroid cytopathology at each hospital. FNAC diagnoses were classified into six categories according to the Bethesda System (13), and CNB specimens were evaluated on the basis of the criteria proposed by the Korean Endocrine Pathology Thyroid CNB Study Group (14).
Follow-up protocol for active surveillance
The PTMC nodules were examined physically and by neck US every 6–12 months. When newly developed, highly suspicious LN changes were found during active surveillance, FNAC of LNs and washout thyroglobulin measurements were performed. Thyroid surgery was recommended by the attending physician when the primary tumor diameter had increased by ≥3 mm from the baseline US, when a new LN metastasis or distant metastasis was confirmed, or when the tumor threatened to impinge on the posterior capsule, recurrent laryngeal nerve, trachea, or esophagus. Prophylactic central neck dissection was performed in all patients who underwent delayed thyroid surgery. After initial thyroid surgery, patients were regularly followed up, as previously described (18 –20).
Statistical analysis
All statistical analyses were performed using R v3.4.0 (R Foundation for Statistical Computing, Vienna, Austria), and graphs were produced using GraphPad Prism v5.0 (GraphPad Software, Inc., San Diego, CA). Continuous variables are described using the mean and standard deviation or the median and interquartile range (IQR), and categorical variables are presented as frequency with percentage. In the evaluation of clinical features according to tumor size change, the chi-square test was used for the analysis of categorical variables, and Student's t-test was used for the analysis of continuous variables. Linear mixed models were used to evaluate the trends in tumor volume with time in each patient. Receiver operating characteristic curves were used to determine the optimal cutoff points for patient age. Survival curves were plotted using the Kaplan–Meier method, and the log-rank test was used to determine their significance. p-Values of <0.05 were considered to represent statistical significance.
Results
Baseline characteristics of patients with PTMC who underwent active surveillance
Table 1 shows the baseline characteristics of the 370 patients with PTMC who underwent active surveillance. The mean age of the patients was 51.1 ± 11.7 years, 110 (29.7%) patients were <45 years, and 76.8% were female. The initial maximum diameter and volume of PTMC on baseline US were 5.9 ± 1.7 mm and 81.0 ± 77.7 mm3, respectively. During active surveillance, 28 (7.6%) patients were taking levothyroxine, and 14 (3.8%) were on thyrotropin suppression therapy. The most common reason for pursuing active surveillance was the patient's own decision (70.0%). In addition, 20.3% of patients had concomitant distinct malignant disease, 4.6% were high risk for general anesthesia due to cardiopulmonary disease, 3.8% had concomitant distinct uncontrolled systemic disease, and 1.4% were pregnant at the time of diagnosis.
Baseline Characteristics of PTMC Patients Under Active Surveillance
Continuous variables are presented as means (standard deviation). Categorical variables are presented as numbers (percentages).
PTMC, papillary thyroid microcarcinoma.
Clinical features of patients with PTMC classified according to change in tumor size
The clinical features of patients with PTMC under active surveillance, classified according to the measured change in tumor size, are shown in Table 2. During a median 32.5 (IQR 21.5–47.6) months of active surveillance, 86 (23.2%) patients experienced a volume increase, and 13 (3.5%) patients experienced an increase in maximum diameter of >3 mm. The median duration of surveillance was 34.1 (23.6–47.0) months in the increasing group and 31.4 (IQR 19.9–47.2) months in the stable group. Patients in the increasing group were younger than those in the stable group (p = 0.016): more patients were <45 years old in the increasing group (40.7%) than in the stable group (26.4%; p = 0.016). There were no significant differences in sex, number of patients being treated with thyroxine, or number of patients with Hashimoto's thyroiditis between the two groups.
Clinical Features of PTMC Patients Under Active Surveillance According to Tumor Size Change
Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as numbers (percentages).
Changes in PTMC volume during active surveillance overtime
Figure 1A and B shows the time-dependent logarithmic-transformed actual tumor volume in each patient. Tumors in the stable group tended not to increase in size. However, in the increasing group, the tumor volume did increase linearly with time (β = 0.987; p < 0.001). The mean percentage change in tumor volume from the initial value is presented in Figure 1C. The difference in the percentage change in volume between the stable and increasing groups significantly increased with time (p = 0.003).
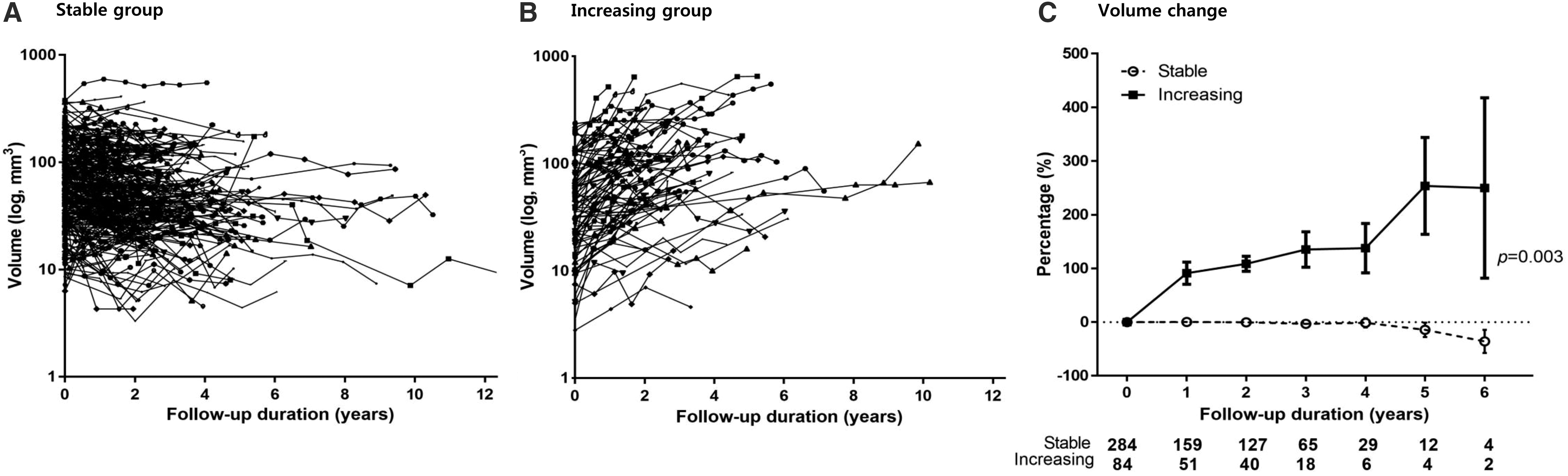
Changes in tumor volume with time. Time-dependent logarithmically transformed tumor volume in each patient (
Time-dependent growth of PTMCs during active surveillance
The time-dependent change in tumor size during active surveillance is presented in Figure 2. The cumulative incidence of tumor volume increase gradually rose with time (6.9% at two years, 17.3% at three years, 28.2% at four years, 36.2% at five years, and 47.5% at six years; Fig. 2A). By contrast, the cumulative incidence of maximum diameter increase rose more slowly with time in stepwise manner (0.6% at two years, 3.2% at three years, 5.3% at four years, 6.4% at five years, and 12.0% at six years; Fig. 2B).
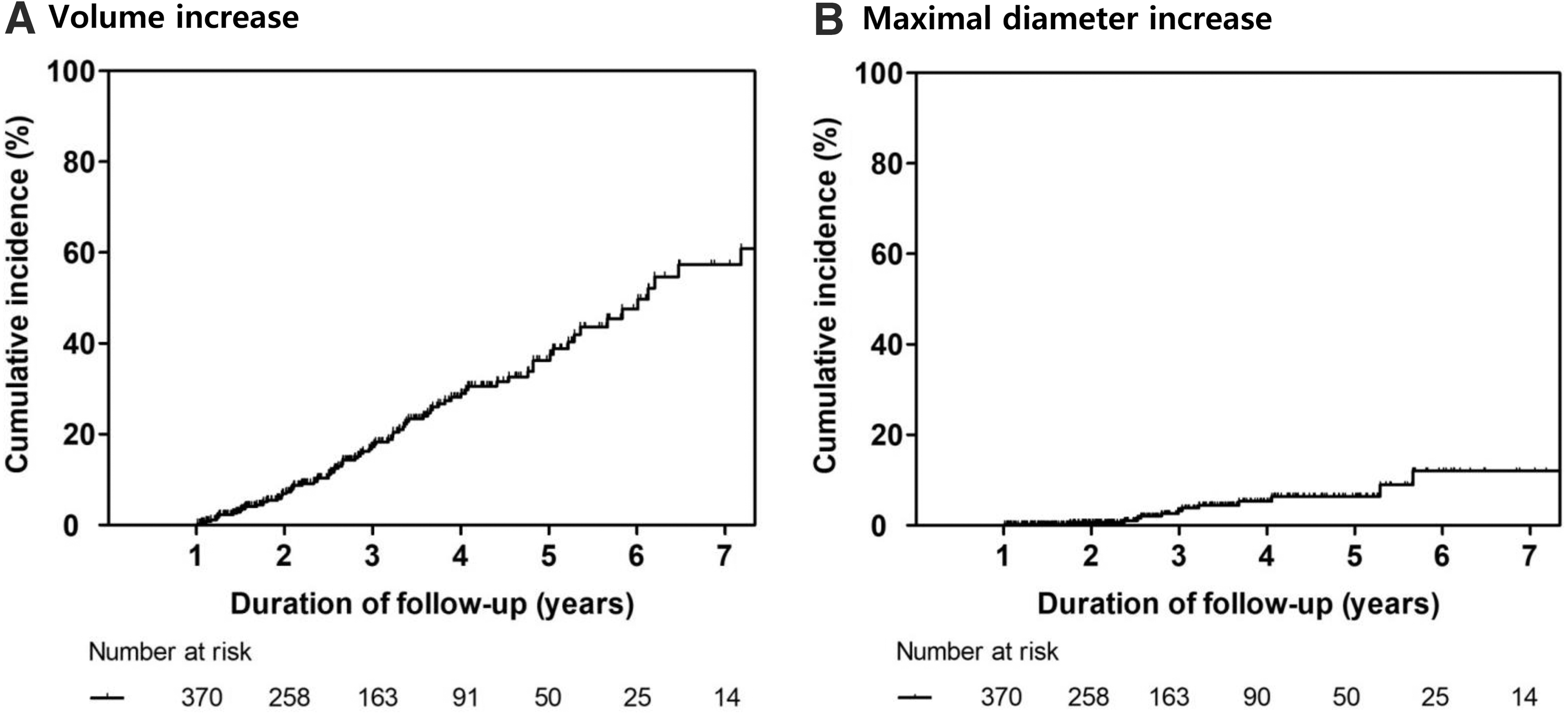
Time-dependent cumulative incidence of papillary thyroid microcarcinoma (PTMC) growth during active surveillance. Proportion of patients who showed a volume increase of ≥50% (
Figure 3 shows the time-dependent change in PTMC size in patients of <45 years and ≥45 years. There was a significant difference in tumor size increase according to the age of the patient, such that the relative risk of tumor size increase in younger patients was almost double that in older patients (hazard ratio = 2.2 [confidence interval 1.3–3.6], p = 0.002). However, there was no difference with respect to the maximum diameter increase (p = 0.315).
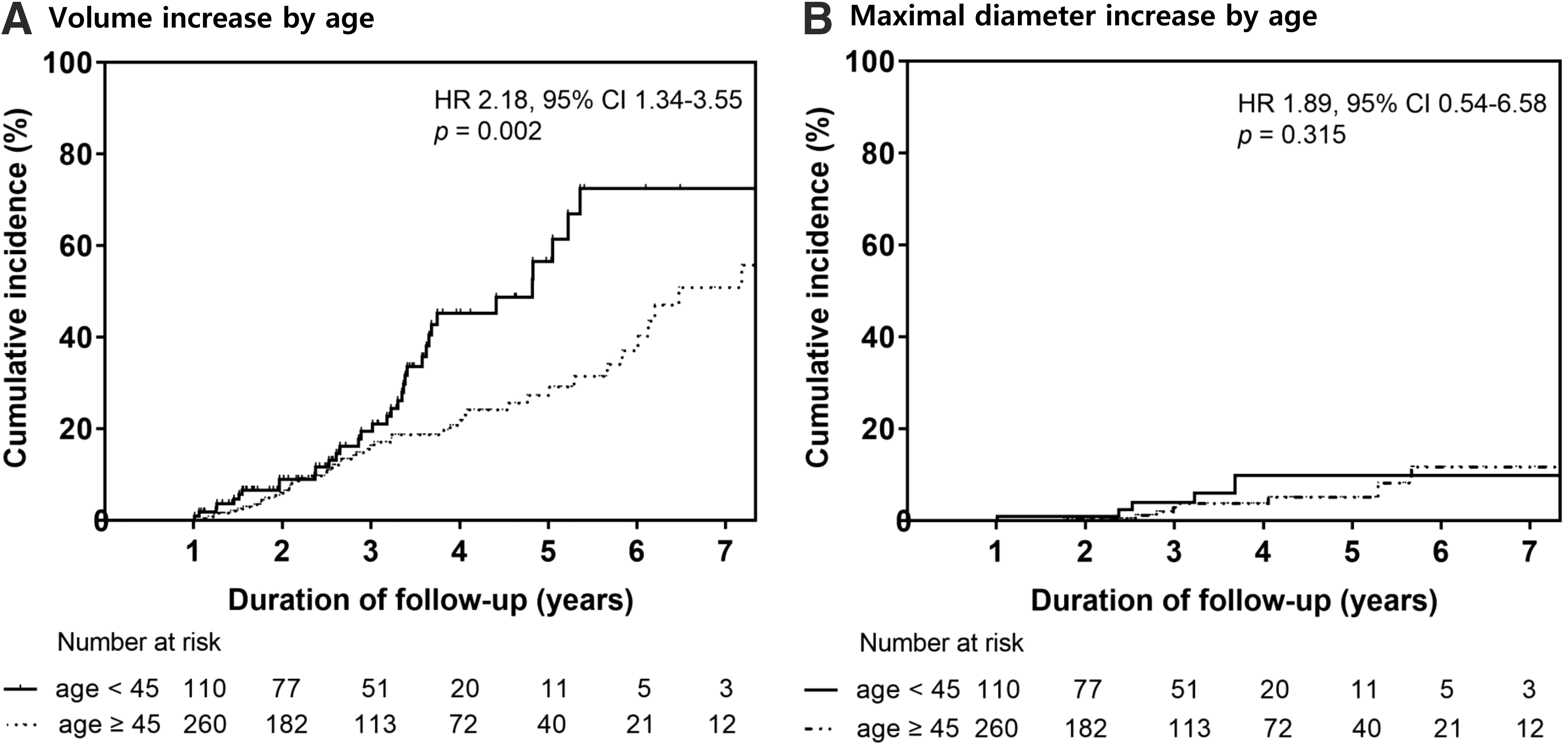
Relationship between age and the proportion of patients demonstrating papillary thyroid microcarcinoma (PTMC) growth during active surveillance. Time to a tumor volume increase ≥50%, classified according to age <45 years or ≥45 years (
Clinicopathologic features of patients who underwent delayed thyroid surgery
During active surveillance, 58 (15.7%) PTMC patients underwent delayed thyroid surgery (Table 3). The median time between diagnosis and surgery was 24.8 (IQR 16.5–35.4) months. The mean age of the study subjects was 48.5 ± 9.1 years, and 79.3% were female. The most common reason for delayed thyroid surgery was anxiety of the patients (48.3%), and the second most common reason was tumor size increase (22.4%). Five (8.6%) patients underwent surgery due to the newly developed LN metastasis, visible on US.
Clinicopathologic Features of Patients who Underwent Delayed Thyroid Surgery for PTMC
Continuous variables are presented as mean (standard deviation). Categorical variables are presented as numbers (percentages).
LN, lymph node.
The maximum diameters of the tumors on initial US, final US, and surgical pathology were 6.3 ± 1.7 mm, 7.2 ± 1.9 mm, and 8.3 ± 1.1 mm, respectively. Among the 58 patients who underwent delayed thyroid surgery, 41 (70.7%) underwent lobectomy and 17 (29.3%) underwent total thyroidectomy. Five patients with appearance of LN metastasis during active surveillance underwent therapeutic central neck dissection, and others underwent prophylactic central neck dissection. On final surgical pathology, 51 (87.9%) patients had classical PTMCs, four (6.9%) had a follicular variant PTC, and three (5.2%) had tall-cell type PTMCs. LN metastases were found in 17 (29.3%) patients, all of which were confined to the central neck area. No patient showed recurrence after the initial thyroid surgery during a median 18.7 (IQR 7.7–32.2) months of follow-up. No patients developed distant metastasis, and there was no case of cancer-specific death.
Discussion
Active surveillance is considered to be a new option for the management of patients with low-risk PTMCs instead of immediate thyroid surgery (1,2,21). The natural course of PTMC during active surveillance was evaluated in a multicenter cohort study. Over a median 32.5-month active surveillance period, 86 (23.2%) patients experienced tumor volume increase, and 17 (4.6%) patients had LN metastasis on final surgical pathology. Almost half of the patients with PTMC showed a volume increase over a six-year period. The age of the patient was associated with the risk of tumor size increase, with patients <45 years of age being more common in the increasing group.
Active surveillance of thyroid cancer was first introduced by a Japanese group, who reported that 5% and 10% of patients had a maximum diameter increase of ≥3 mm after 5 and 10 years, respectively (4,5). A recent study from the United States reported similar results, in that around 10–15% of PTMCs showed increases in tumor diameter of ≥3 mm during the first five years of active surveillance (8). The present study had similar findings, but it also showed that the cumulative incidence of tumor growth slowly increases in a linear fashion with time. Although the growth rate of these tumors is not rapid, they may eventually progress when observed over a long period. Prospective observational longer studies are required to evaluate the clinical outcome of active surveillance.
In this study, age-related differences in tumor growth were detected by measurement of volume but not by measurement of maximum diameter. Recent studies report that the assessment of tumor growth by volume change is a more sensitive method than the use of changes in maximal diameter (7,8). Because volume is calculated by multiplying three diameters, an increase in volume is more likely to be detected than a small increase in diameter, but the clinical significance of the former could be lower, despite the greater sensitivity of the measurement. Further studies regarding the clinical significance and application of volume assessment for the evaluation of tumor growth during active surveillance are needed. However, considering linear increase of tumor volume in each patient, this approach may be utilized as an early indicator for surgical intervention during active surveillance. If confirmed through a prospective observational trial, this volume increase ultimately will result in a significant increase in the maximal diameter, which leads to surgical intervention.
Age is an important consideration in the management of differentiated thyroid cancer, and indeed thyroid cancer is the only malignancy for which age is considered to be a prognostic factor (22 –25). According to studies from Japan, younger age was associated with tumor growth during active surveillance (5,10). The findings of the present study were similar in that the risk of PTMC growth in younger patients was almost doubled compared to older patients during active surveillance, suggesting that immediate thyroid surgery may be preferable for younger patients, although active surveillance is not necessarily contraindicated.
According to some previous studies and the results of the current study, sex does not represent a risk factor for tumor growth in low-risk PTMC patients during active surveillance (5,7). However, other previous studies showed that men were more likely to show LN metastasis associated with low-risk PTMCs (24,25). Previous studies of active surveillance of low-risk PTMC have focused on the measurement of tumor size (4,5,7,8,10). In the present study, only 5/17 patients with LN metastasis on postoperative pathology had LN metastasis that was visible on US. Considering the low sensitivity of preoperative US for the detection of central LN metastasis (26,27), men who are at high risk for LN metastasis should be more concerned about the adequacy of active surveillance.
During active surveillance, 15.7% of PTMC patients eventually underwent delayed thyroid surgery. A previous study suggested that surgery for PTMC can be safely delayed >18 months without any adverse patient outcomes (28). The most common reason for the decision to perform surgery was anxiety of the patients (48.3%). In prostate cancer, quality of life (QoL) during active surveillance has been shown not to differ between active surveillance groups and immediate surgery groups (29,30). However, the two types of cancer are not directly comparable. The complication rate after immediate surgery is much lower in thyroid cancer: the incidence of major complications after prostate cancer surgery (impotence and urinary incontinence) can exceed 50%, while the incidence of major complications in thyroid cancer (voice alterations and hypoparathyroidism) tend to be <10% (31,32). The mean patient age at diagnosis of thyroid cancer is much younger than that for prostate cancer, and the majority of thyroid cancer patients are female (33,34). Considering that women tend to develop more anxiety disorders than men (35), anxiety levels regarding the presence of an untreated malignancy might therefore be different between thyroid and prostate cancer patients. QoL is an important consideration when considering treatment options. Therefore, further studies evaluating QoL during active surveillance of PTMC patients are needed.
Previous studies reported that some tumors decrease during active surveillance (7,8). In this study, 27 (7.3%) patients were found to have a significant volume decrease >50%. This decrease has been explained by the FNAC-related changes, including hemorrhage, infarction, fibrosis, and formation of granulation tissue (7,36).
In this study, five patients underwent active surveillance due to pregnancy. With a median of 18.3 (IQR 13.3–26.4) months of follow-up, two (40%) patients had significant maximal diameter and volume increases. Four patients underwent surgery after delivery due to anxiety (two patients) or increase in tumor size (two patients). Only a limited number of studies exist evaluating the changes in thyroid cancer during pregnancy (37 –39). The impact of pregnancy on thyroid cancer remains controversial, and additional research is needed (37 –39).
This study had several limitations. First, there is a possibility of selection bias due to the study's retrospective design. Second, due to the relative short period of active surveillance, the long-term outcomes of active surveillance should be explored in future studies. Third, samples from only a few patients (n = 117) were available for mutational analysis. There was no difference in BRAF mutation status between the increasing group and the stable group when analyzed in a subset of patients (p = 0.380). Finally, there can be inter-observer variation of tumor size and volume measurements due to the innate limitation of serial neck US (15). However, this is the first multicenter cohort study to evaluate the results of active surveillance of low-risk PTMC, and the findings suggest that there is a possibility of tumor progression in some low-risk PTMC patients. Identifying low-risk PTMCs that may demonstrate more aggressive behavior is important.
In conclusion, a significant number of PTMCs might grow during active surveillance, and tumor volume change is a sensitive index in the evaluation of tumor growth. Tumor volume increase may be utilized as an early indicator for surgical intervention, but this concept needs to be confirmed with long-period follow-up studies. Active surveillance should be carefully applied to selected patients and may be used cautiously for younger patients.
Footnotes
Acknowledgments
Part of this study was presented at the 6th Seoul International Congress of Endocrinology and Metabolism meeting and the 48th European Thyroid Association meeting.