
Abstract
Background:
Agranulocytosis occurs in 0.2–0.5% of patients treated with the antithyroid drugs (ATDs) methimazole and propylthiouracil. The objectives of this study were to evaluate the risk of ATD-related agranulocytosis in patients with amiodarone-induced thyrotoxicosis (AIT), and to compare it with the agranulocytosis risk in patients with thyrotoxicosis due to other etiologies treated with ATDs.
Methods:
This was a retrospective cohort study. Participants were 14,781 adult patients with thyrotoxicosis, newly treated with an ATD between January 1, 2002, and December 31, 2015. Among them were 593 patients treated by ATDs due to AIT. The main outcome measures were incidence rates and crude and adjusted hazard ratios using univariate and multivariable Cox regression models for ATD-related agranulocytosis within one year of treatment initiation, in association with AIT.
Results:
Agranulocytosis occurred in 28 (0.19%) of patients newly treated with methimazole or propylthiouracil during the first year of follow-up. Of these 28 patients, 8/593 (1.35%) were AIT patients and 20/14,188 (0.14%) were thyrotoxic patients that was not AIT related (p < 0.001). Incidence rates were 22 (9.47–43.36) cases/1000 person-years of follow-up in AIT, and 1.79 (1.09–2.76)/1000 person-years of follow-up in non-AIT thyrotoxicosis (p < 0.0001). In univariate Cox regression analysis, risk for ATD agranulocytosis associated with AIT was 9.71 (4.28–22.05) compared to the risk in non-AIT thyrotoxicosis. In a multivariable model, adjusting for age, sex, body mass index, smoking history, year of cohort entry, diabetes mellitus, hypertension, renal failure, beta blockers, calcium channel blockers, anti-aggregants, and dose of ATDs, the risk associated with AIT was 5.70 (2.14–15.21). In a model adjusted for a propensity score to receive amiodarone, risk for ATD agranulocytosis associated with AIT was 6.32 (1.22–32.70).
Conclusions:
ATD use is associated with a higher risk for agranulocytosis in patients with AIT.
Introduction
The antithyroid drugs (ATDs) methimazole (MMI) and propylthiouracil (PTU) are used for the treatment of hyperthyroidism. Carbimazole, a MMI precursor, is a third option available in some European and Asian countries. ATDs are highly effective. However, serious adverse effects are not uncommon. Agranulocytosis, defined as a granulocyte count of <0.5 × 109/L, is the most severe adverse effect, occurring in 0.2–0.5% of treated patients, usually in the early treatment period (1,2). It is foremost important to identify risk factors for this life-threatening adverse event. Higher ATD dose, older age, and retreatment have been associated with increased susceptibility (3 –8). Common predisposing genetic variants in human leukocyte antigen genes have been identified in Japan and Taiwan (9,10), as well as in Caucasians (11), and two predisposing rare NOX3 variants have been identified in the Netherlands (12).
Amiodarone, an antiarrhythmic medication widely used in treatment of atrial and ventricular tachyarrhythmias, is an extremely iodine-rich compound with a structural resemblance to thyroxine (T4). Thyroid dysfunction (hypo- or hyperthyroidism) develops in 15–20% of amiodarone-treated patients (13). Amiodarone-induced thyrotoxicosis (AIT), occurring in 6–10% of patients managed with amiodarone (2), is the result of either accelerated thyroid hormone synthesis secondary to iodine overload in a gland harboring autonomous nodules (type 1 AIT), or of destructive thyroiditis, resulting in excess release of preformed T4 and triiodothyronine (T3) into the circulation (type 2 AIT) (13,14). ATDs are the primary modality of therapy in patients with type 1 AIT, while type 2 AIT is responsive to glucocorticoids treatment (13 –15). Glucocorticoids are useful as an adjunctive therapy in type 1 AIT as well due to their inhibition of 5′-deiodinase activity and the reduction of free T3 (fT3) levels (13). Imaging methods, including radioiodine uptake scan, color flow Doppler sonography, and 2-methoxyisobutyl isonitrile scan, for the purpose of distinguishing between the two pathophysiology mechanisms (13 –16) are inaccurate and sometimes lead to misdiagnosis and delayed treatment. In addition, both mechanisms can concur in the same patient (mixed type AIT) (15,17). Thus, in clinical practice, a clear distinction between AIT types is often impossible, and a pragmatic approach combining ATDs with glucocorticoids and beta blockers is applied (15,17,18).
We have noticed a relatively high rate of ATD-associated agranulocytosis in AIT patients. This study sought to evaluate the agranulocytosis risk in a large clinical database, and to compare the risk in AIT patients to the risk of ATD-associated agranulocytosis in thyrotoxicosis that is not amiodarone related.
Methods
Data source
A cohort study was conducted using the Clalit Health Services database. Clalit is the largest health services provider in Israel, providing medical care to 4.2 million people, which is more than half of the Israeli population. All clinical and administrative data of Clalit have been centrally computerized since 1998 to produce electronic medical records that include all patients' diagnoses from primary-care physicians and community specialty clinics (coded using the International Statistical Classification of Diseases, Ninth Revision [ICD-9]), anthropometric and life-style variables such as body mass index (BMI) and smoking, full hospitalization records, and radiology, laboratory, and pharmacy data of filled prescriptions. This database has been formerly described and is valid and reliable (19,20). A chronic disease registry is compiled from these data sources. Diagnoses are captured in the registry by diagnosis-specific algorithms using both code reading (e.g., ICD-9 and International Classification of Primary Care) and text reading. A record is kept of the sources and dates used to establish the diagnosis, with the earliest recorded date being considered the starting date.
Study population
All patients aged ≥18 years with a diagnosis of thyrotoxicosis, hyperthyroidism, thyroid nodule, thyroid goiter, or benign neoplasm of the thyroid from the Clalit database (ICD-9 codes 226 and 240–242) and who were also newly treated with the ATDs available in Israel (MMI or PTU) between January 1, 2002, and December 31, 2015, were included. Date of entry into the cohort was the date of the first prescription of an ATD. Patients were also required to have at least six months of medical history in Clalit before entering the cohort in order for a reliable clinical background to be obtained for each patient.
All patients with previous diagnoses of malignancy, myelodysplastic syndrome, myeloproliferative diseases, or organ/blood marrow transplantation (ICD-9 codes 140–172, 174–209,199.2, 238.4, 238.71–7, 284, 285.0, 289.83, 996.8, and V42) before the cohort entry date were excluded. Patients with a diagnosis of systemic lupus erythematosus (SLE) before cohort entry and patients treated with immune-modulating drugs (including all immunosuppressive drugs, interferon, and gold) before cohort entry were also excluded by obtaining drug dispensing data from Clalit pharmacies for each patient in the cohort. Patients with agranulocytosis (granulocyte count <0.5 × 109/L), anemia (hemoglobin level <10 g/dL), or thrombocytopenia (platelet count <100,000/μL) in the last blood count before cohort entry were also excluded.
Exposure and outcome assessment, follow-up, and potential confounders
The nearest fT3 and free T4 (fT4) laboratory results before the cohort entry date (up to one year before cohort entry) were obtained from the laboratory database. Variables that were retrieved from the Clalit computerized database for the main analysis included date of birth, sex, BMI, history of smoking, and a history of hypertension, diabetes mellitus, or chronic renal failure at cohort entry. Multiple imputations were conducted to impute missing data for smoking history and BMI.
Drug dispensing data from Clalit pharmacies were used to identify treatment with amiodarone at cohort entry (up to three months before cohort entry) and to identify treatment with platelet aggregation inhibitors, beta-blocking agents, and calcium channel blockers at cohort entry (±3 months). The drug dispensing database was also used to establish the starting doses of MMI and of PTU. The ATD dose was classed as high if either the MMI or PTU administered dose was above the median starting dose for that drug (the median dose being the middle value of the initial ATD dose in this study population). All glucocorticoid prescriptions were also retrieved at the cohort entry date (±1 month) to control for the effect of addition of glucocorticoid treatment to patients with thyrotoxicosis.
All blood counts performed during follow-up were searched for an outcome event, which was defined as agranulocytosis (without anemia and without thrombocytopenia at the time of agranulocytosis ±7 days).
For the main analysis of ATD-associated agranulocytosis, usually occurring in the first few months of therapy, patients were followed for one year, or until an outcome event, March 31, 2016, death, or the end of registration in Clalit, whichever came first.
To assess the robustness of the findings, a secondary analysis was performed in which follow-up was continued until three months after the last ATD prescription was dispensed, an event of agranulocytosis (without anemia and without thrombocytopenia at the time of agranulocytosis event ±7 days), March 31, 2016, death, or end of registration in Clalit, whichever came first.
For sensitivity analysis, a propensity score to receive amiodarone was calculated that included the following baseline covariates at cohort entry: age, sex, Jewish/Arab origin, smoking, BMI, renal failure, liver disease, atrial fibrillation, ischemic heart disease, cerebrovascular accident, transient ischemic attack, cardiac valvular disease, congestive heart failure, diabetes mellitus, hyperlipidemia, and hypertension.
To assess the outcome of agranulocytosis cases, their blood counts were followed until recovery from agranulocytosis, and data on the use of colony-stimulation factor and of death occurring up to one month from the agranulocytosis event and therefore classed as associated with the event were retrieved.
Statistical analysis
Continuous variables are presented as the mean and standard deviation (SD). Categorical variables are presented as proportions. The incidence rate was estimated by dividing the total number of agranulocytosis cases by the total number of person-years of follow-up in the cohort, with 95% confidence intervals (CIs) based on Poisson distribution.
For agranulocytosis-risk estimation, univariate and multivariable Cox regression models were used. Hazard ratios (HR) and CIs for an agranulocytosis event were estimated. In the first model, the association between AIT and ATD-related agranulocytosis was studied, adjusting for the baseline variables age, sex, BMI, and smoking. In the second model, the association between AIT and ATD-related agranulocytosis was studied, adjusting for baseline, clinical, and treatment variables, including age, sex, BMI, smoking, hypertension, diabetes mellitus, renal failure, year of cohort entry, platelet aggregation inhibitors, beta blockers, calcium channel blockers, and ATD starting dose.
Kaplan–Meier estimates were used to compute proportion free of agranulocytosis curves in order to examine the unadjusted association between AIT and ATD agranulocytosis and between non-AIT thyrotoxicosis and ATD agranulocytosis, and the log-rank test was used to compare groups.
Sensitivity analysis
As a sensitivity analysis, a multivariable Cox regression model was performed for the association between AIT and ATD agranulocytosis, adjusting for a propensity score to receive amiodarone. The distribution of propensity scores for both groups was examined, and the top and bottom 5% of each distribution was removed from the outcome model. These adjustments were made because people treated contrary to extreme scores may have important unmeasured characteristics that could bias effect estimates. Another sensitivity analysis was performed without trimming the 5% tails of each distribution to investigate the effect of this analytic decision.
Secondary analysis
As a robustness analysis, multivariable Cox regression analysis was performed for the association between AIT and ATD agranulocytosis, continuing follow-up until three months after the last ATD prescription was dispensed, and adjusting for age, sex, BMI, smoking, year of cohort entry, history of hypertension, diabetes mellitus, hyperlipidemia, chronic renal failure, platelet aggregation inhibitors, beta blocking agents, calcium channel blockers, and mean daily ATD dose.
All tests were two-sided, and a p-value of ≤0.05 was considered significant. Analyses were conducted with IBM SPSS for Windows v24 (IBM Corp., Armonk, NY). The Clalit Health Services Institutional Review Board gave ethical approval for the study (no. 0134-16-COM1).
Results
A total of 14,781 Clalit patients with thyrotoxicosis were newly treated with an ATD between 2002 and 2015. A detailed description of the cohort selection can be found in Figure 1. In 28 (0.19%) patients, agranulocytosis developed during 11,566 years of follow-up (mean follow-up time = 9.36 months, SD = 3.55, minimum = 0.16, maximum = 11.97 months). There was no difference in agranulocytosis occurrence between male and female patients. The incidence rate of agranulocytosis was 2.42 [CI 1.61–3.50] cases/1000 person-years of follow-up.
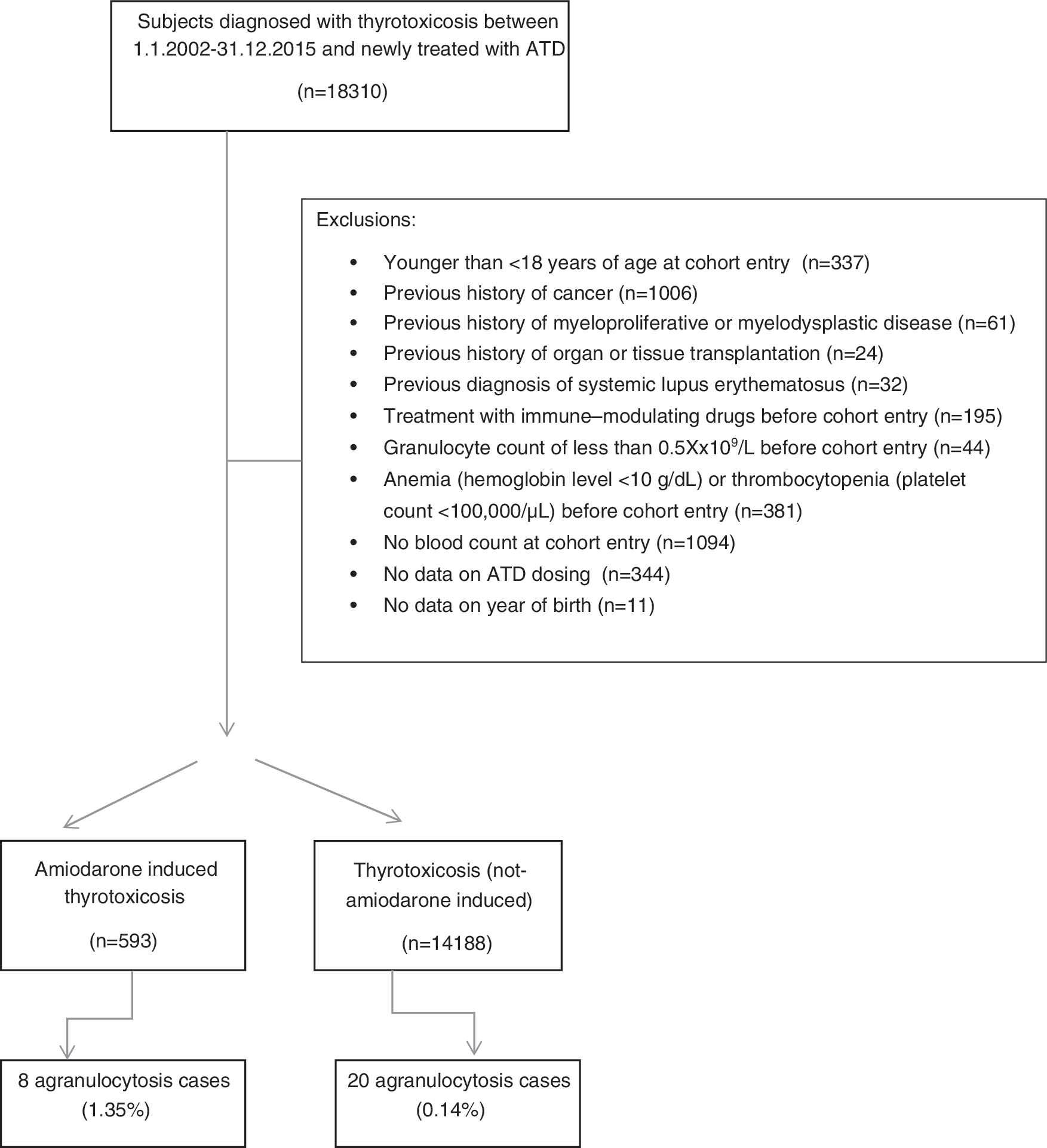
Flowchart of the study cohort formation.
Patients in whom agranulocytosis developed were older at the beginning of ATD treatment than patients in whom agranulocytosis did not develop: (M age = 64.04, SD = 19.31 and M age = 51.88, SD = 18.45, respectively; p < 0.001). There was no significant difference between the rate of occurrence of agranulocytosis in MMI- and PTU-treated patients (0.17% and 0.18%, respectively). The mean starting dose of MMI was 25.0 mg/day in patients who developed agranulocytosis later, and 21.49 mg/day in patients who did not develop agranulocytosis (HR = 1.96 [CI 0.77–4.97]). In patients treated with PTU who developed agranulocytosis, the mean starting dose was 193.75 mg/day compared to 172.74 mg/day in patients without the event (HR = 1.57 [CI 0.39–6.29]; dose differences for both medications were not significant in univariate Cox regression analyses). No association was found between fT3 and fT4 levels at cohort entry and agranulocytosis. Mean granulocyte count at the time of the agranulocytosis event was 179.6/mm3 (SD = 155; median = 100/mm3).
Of the 14,781 patients in the cohort, 593 were treated with ATDs due to thyrotoxicosis caused by amiodarone. The characteristics of AIT patients and patients with thyrotoxicosis due to other etiologies (non-AIT patients) treated by ATDs are shown in Table 1. In 8/593 (1.35%) AIT patients and 20/14,188 (0.14%) non-AIT thyrotoxicosis patients, agranulocytosis developed within one year of ATD treatment (p < 0.001). Incidence rates were 22 (9.47–43.36)/1000 person-years of follow-up in AIT, and 1.79 (1.09–2.76)/1000 person-years of follow-up in non-AIT thyrotoxicosis patients (p < 0.0001). Agranulocytosis occurred after a mean of 1.51 months in AIT patients (SD = 0.66, minimum = 0.3, maximum = 2.46), and after 1.66 months (SD = 0.69, minimum = 0.79, maximum = 3.38) in non-AIT thyrotoxicosis patients. AIT was associated with a HR of 9.71 [CI 4.28–22.05] for ATD-induced agranulocytosis compared to the risk in non-AIT thyrotoxicosis patients in univariate Cox regression analysis. Figure 2 shows Kaplan–Meier curves of the time until study participants developed agranulocytosis.
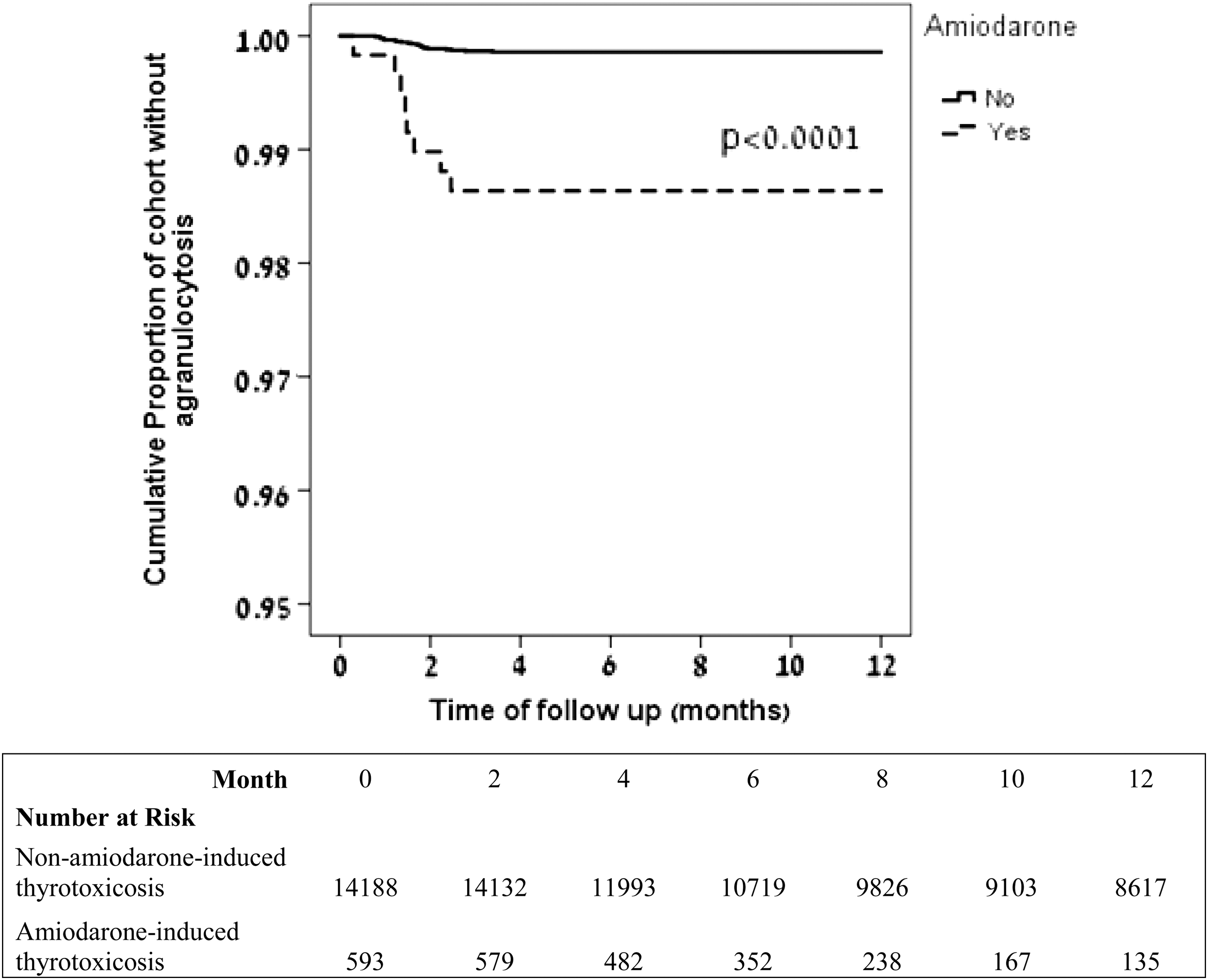
Kaplan–Meier curves displaying time to agranulocytosis in antithyroid drug (ATD)-treated thyrotoxicosis patients: amiodarone-induced thyrotoxicosis patients (n = 593) and non-amiodarone-induced thyrotoxicosis patients (n = 14,188). Incidence rate in amiodarone-induced thyrotoxicosis patients: 22 (9.47–43.36) cases/1000 person-years of follow up; incidence rate in non-amiodarone thyrotoxicosis patients: 1.79 (1.09–2.76)/1000 person-years of follow up (p < 0.0001).
Characteristics of a Cohort of 14,781 Thyrotoxicosis Patients Treated with Antithyroid Drugs
Serum fT3 normal values: 3.5–6.5 pmol/L; serum fT4 normal values: 10–20 pmol/L.
Including imputation for smoking data for 3% of participants and for BMI data for 3.5% of participants.
2032 patients were prescribed both drugs during follow-up.
BMI, body mass index; SD, standard deviation; fT3, free triiodothyronine; fT4, free thyroxine.
AIT patients were older and more often carried diagnoses of chronic diseases, including hypertension, diabetes mellitus, and chronic renal failure, and were more often treated with platelet aggregation inhibitors, beta-blocking agents, and calcium channel blockers (Tables 1 and 2). Multivariable Cox regression analyses were performed to evaluate the risk for agranulocytosis associated with AIT, adjusting for these baseline clinical differences (Fig. 3). In the first model, AIT was associated with an increased risk for ATD agranulocytosis, with a HR of 7.61 [CI 3.08–18.77]. Age was associated with an independent risk in the model, with a HR of 1.03 [CI 1.01–1.05] for one year increase in age, meaning that being older by one year was associated with a 1.03-fold increase in hazard. In the second model, adjusted for age, sex, BMI, smoking history, year of cohort entry, diabetes mellitus, hypertension, renal failure, beta blockers, calcium channel blockers, platelet aggregation inhibitors, and ATD starting dose, the risk associated with AIT was 5.70 [CI 2.14–15.21]. AIT was associated with a HR of 6.32 [CI 1.22–32.70] after adjusting for propensity score, when the top and bottom 5% of each distribution was removed from the outcome model (Fig. 3). In a sensitivity analysis, adjusted for the propensity score in the full cohort without trimming the upper and lower 5%, and for ATD starting dose, AIT was associated with a HR of 4.54 ([CI 1.45–14.22]; p = 0.009) for ATD agranulocytosis. In all multivariable analyses, the ATD starting dose was not associated with an independent risk for agranulocytosis.
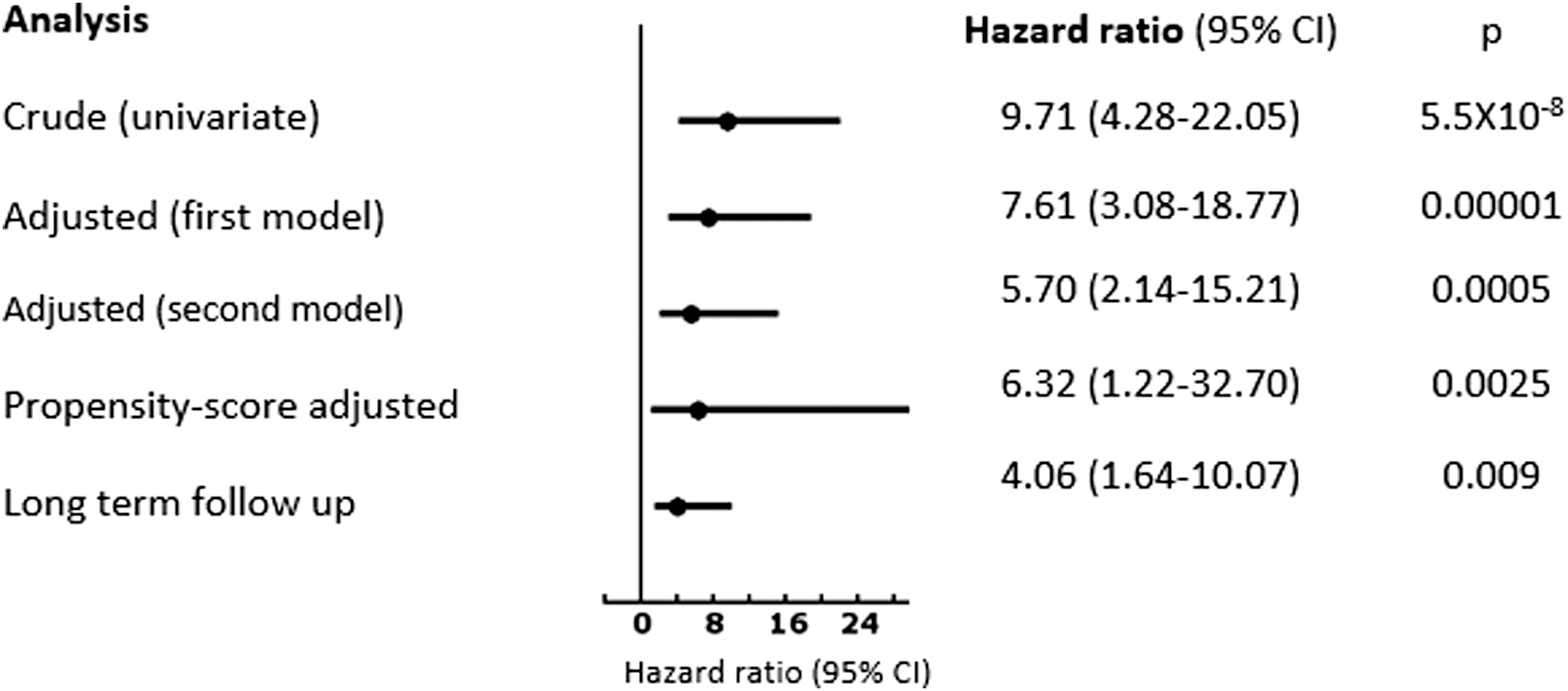
Forest plot summarizing results of univariate and multivariate analyses showing hazard ratios and confidence intervals for association between amiodarone-induced thyrotoxicosis and ATD agranulocytosis.
Comorbidities and Major Cardiovascular Drug Use in Amiodarone-Induced Thyrotoxicosis Patients and in Patients with Thyrotoxicosis due to Other Etiologies, n (%)
Of 593 AIT patients, 76 were treated with glucocorticoids in addition to the ATD treatment at cohort entry. When the cohort was stratified by treatment with ATD only and treatment with ATD plus glucocorticoids, the risk for agranulocytosis associated with ATD together with glucocorticoids increased in AIT patients but not in non-AIT patients. This might reflect the association of agranulocytosis with the background clinical variables or clinical severity. In the multivariable model in which the glucocorticoid treatment was introduced as a variable in the model, it was not associated with an independent risk. As the study was designed to include a cohort of ATD-treated thyrotoxicosis patients, patients who might have been treated with glucocorticoids only, without an ATD, were not included.
In the secondary analysis, in which follow-up of the same cohort of 14,781 thyrotoxicosis patients treated with ATDs was continued until three months after the last ATD prescription was dispensed, 11 more patients developed agranulocytosis during follow-up, making a total of 39 (0.3%) patients who developed agranulocytosis during 40,551 years of follow-up (incidence rate = 0.96 [0.68–1.32]/1000 years of follow-up. The mean follow-up time was 2.7 years (SD = 3.1 years; range = 0.01–14.2 years). Agranulocytosis occurred after a median of 55 days. In this analysis of long-term follow-up, adjusted for all variables from the second model, AIT was associated with a HR of 4.06 [CI 1.64–10.07] for ATD agranulocytosis (Fig. 3).
Granulocyte counts recovered in 24/28 patients with agranulocytosis, within a median of two days. Fifteen patients were treated with colony-stimulating factor. Of the 28 patients with agranulocytosis, five (17.9%) died within one month from the agranulocytosis event: one (0.168%) patient with AIT and four (0.028%) non-AIT thyrotoxicosis patients (p = 0.185). Of the five patients from the cohort who died, only one was treated with colony stimulating factor. Causes of death were fasciitis and Escherichia coli bacteremia in an 84-year-old patient; Pseudomonas aeruginosa bacteremia in a 78-year-old patient; cellulitis in a 76-year-old patient; and no additional information on two patients who died at the ages of 88 and 92 years with ATD agranulocytosis. The four patients in whom the granulocytes count had not recovered died. Patients who died within a month from the agranulocytosis event were older (M age = 84 years) compared to patients who survived the agranulocytosis event (M age = 60 years; p = 0.001). Patients who died with an agranulocytosis event also had a higher BMI (44 vs. 28 in patients who survived; p = 0.04). There was no difference in other clinical characteristics or in the ATD starting doses between patients who survived and patients who died with an ATD agranulocytosis event.
Discussion
Agranulocytosis is the most dreaded side effect of ATD therapy, with fatality rates reported in the literature of 5–10% (21). The earlier that ATDs are withheld and supportive therapy is administered, the higher the likelihood of an improved prognosis (22 –24). Granulocyte count monitoring in patients receiving ATDs has not been considered a cost-effective approach (21), and screening for predisposing genetic variants is not clinically available yet. Recognizing other risk factors for this adverse effect might enable closer follow-up in high-risk groups in order to try to identify early a dangerous granulocyte count decline.
This large population-based cohort of patients with thyrotoxicosis shows for the first time that AIT is associated with an increased risk for ATD-related agranulocytosis. A HR of 9.71 [CI 4.28–22.05] was found for agranulocytosis associated with AIT compared to the risk in patients with thyrotoxicosis due to other etiologies in univariate analysis, and a HR of 5.70 [CI 2.14–15.21] was found for agranulocytosis associated with AIT in a multivariable model, adjusting for ATD dose, age, sex, BMI, smoking history, year of cohort entry, and major baseline clinical characteristics, including diabetes mellitus, hypertension, renal failure, beta blockers, calcium channel blockers, and platelet aggregation inhibitors. The rate of agranulocytosis in the first year of ATD therapy in this cohort was 0.19%, which is in agreement with rates reported in the literature (1,21,25). However, in AIT patients, the rate of agranulocytosis was 1.35%.
The cohort was defined by the ATD treatment in order to evaluate the risk of agranulocytosis related to ATD. Thus, patients with AIT were included in the cohort once they had begun treatment with ATDs (or ATDs combined with glucocorticoids). A clinical distinction between AIT type 1 and 2 might have been made by the patients' endocrinologist but could not be evaluated as part of the database diagnoses. Of note, patients who might have been diagnosed with definite type 2 AIT and treated by glucocorticoids alone were not included in the study.
Amiodarone is a very lipophilic molecule that accumulates in adipose tissue, cardiac and skeletal muscle, and in the thyroid gland, among others (26,27). Although there is a general decline in the use of amiodarone, consistent with growing safety concerns (28,29), this effective antiarrhythmic medication is still prescribed to many patients by cardiologists and internal medicine specialists. The pathophysiological mechanism underlying the increased risk for ATD-related agranulocytosis in patients with AIT remains elusive. Agranulocytosis is caused by an autoimmune-mediated reaction and a direct toxic effect of ATDs on bone-marrow hematopoietic stem cells (21,30,31). Amiodarone is not known to be associated with neutropenia by itself (32). Nevertheless, it has been demonstrated that amiodarone is concentrated in the bone marrow (33) and is associated with bone-marrow granulomas (34 –36) and even pancytopenia (37), which is sometimes reversible upon amiodarone cessation (38). It is possible that amiodarone, if present in bone marrow, creates a “favorable” environment for the ATD-induced damage. In this cohort, all patients with anemia, thrombocytopenia, or neutropenia were excluded at cohort entry while already on amiodarone, excluding patients with possible pre-existing amiodarone-related pancytopenia. Thus, it is assumed that the association observed is most probably the well established ATD-associated agranulocytosis, worsened by the concomitant presence of amiodarone.
Patients with AIT are usually treated with higher ATD doses, since iodine enrichment in the thyroid gland secondary to amiodarone therapy appears to be less responsive to treatment (13). AIT patients in the present cohort were exposed to higher starting doses of ATDs and were older than patients with thyrotoxicosis due to other etiologies (Tables 1 and 2). However, a high ATD dose was not found to be an independent risk factor for ATD agranulocytosis in the multivariable model, and the risk for ATD agranulocytosis associated with AIT was 5.70 times higher after adjusting for ATD dose, age, and other clinical variable. In several previous studies, higher MMI starting doses were associated with agranulocytosis (1,4–5); no dose-related association was found for PTU (1). Others have not shown a higher risk associated with increased doses (7,25). In the present cohort, there was a tendency toward higher MMI and PTU starting doses in patients who later developed agranulocytosis, but as the range of starting doses in the cohort was not wide (in the full cohort, the mean MMI starting dose was 21.49 with a SD of 11.1, median 20), differences were not statistically significant. Older age was associated with a higher risk for agranulocytosis in the current cohort, as well as for mortality associated with agranulocytosis, in agreement with former reports (21).
The mean time to granulocytes count recovery is reported to be around 7 (0–22) days, with a median of 5.5 days (6,8). In the present cohort, recovery occurred within a median of 2 days. In a cohort of ATD agranulocytosis patients hospitalized in tertiary hospitals in Korea (6), 44/54 agranulocytosis patients were treated with colony-stimulating factor. In the present cohort, which was comprised of population-derived agranulocytosis patients, the rate of colony-stimulating factor use was lower, probably due to faster spontaneous recovery of neutrophil counts. Most of the patients who were not treated with colony-stimulating factor were also not hospitalized. The case-fatality rate was 7% in a cohort of hospitalized Graves' patients with ATD-induced agranulocytosis (M age = 38.2 years, SD 14.9, range 9–72 years) (6), and a case-fatality rate of 4% was reported in a collection of spontaneous reports of ATD-related agranulocytosis Graves' disease cases in Japan (M age = 43.4 years, SD 15.2) (3). In the present cohort of much older patients with ATD agranulocytosis (M age = 64.04 years, SD 9.31), the case-fatality rate was 12.8%.
Strengths and weakness of this study
The major strength of this study is its population-based design, which also allowed a cohort of AIT within thyrotoxic patients to be identified that was large enough to assess rates of ATD-related agranulocytosis in AIT and non-AIT thyrotoxic patients. There is paucity of clinical data in the literature on AIT patients. This study was able to show that the higher agranulocytosis risk in AIT patients was not merely an association with older age characterizing AIT patients and the higher ATD dose used in AIT patients. The ability to control for potential important confounders is another strength of this analysis. Laboratory results were used to exclude patients in whom anemia or thrombocytopenia or neutropenia were present before ATD therapy, and to define the outcome measure. A new-users design was followed in order to avoid ATD prevalent users' bias and to allow assessment of the ATD starting dose. To reduce potential time-related biases, time-dependent analyses were used, and year of cohort entry was included in the analysis to reduce bias associated with time-related trends in treatment.
Yet, this study has some limitations. It relied on an administrative computerized database that was not specifically designed for the present study. This cohort study is observational in nature and, as such, cannot prove cause-and-effect relationship, and residual confounding is possible. Although patients with neutropenia, anemia, or thrombocytopenia before beginning ATD treatment, as well as patients with diseases that might have been related to a reduction in white blood cell count, such as SLE and cancer, were excluded, misclassification of some patients to ATD-associated agranulocytosis might have occurred. However, this misclassification is non-differential and is expected to bias the results toward the null. It is possible that there is a genetic predisposition for ATD-related agranulocytosis, as had been found in Japan and Taiwan and in Caucasians. It was beyond the scope of this study to investigate genetic predisposition. However, the rate of ATD agranulocytosis found was in the same range as in the literature, which adds external validity to the results. Still, a residual risk associated with a genetic predisposition for agranulocytosis in AIT, non-AIT thyrotoxicosis, or in both cannot be excluded.
Controversy exists as to the value of monitoring white blood cell counts in ATD-treated patients. Its usefulness is doubtful because agranulocytosis sometimes develops abruptly. Most clinicians in the United States do not perform periodic monitoring, and in the American Thyroid Association guidelines, there was insufficient evidence to recommend for or against routine monitoring of white blood cell counts in patients treated with ATDs (39). However, it has been shown that routine white blood cell counts performed as part of follow-up visits in Japan detected a large portion of asymptomatic patients with agranulocytosis (40,41). Tighter granulocyte count measurement in selected patient groups might be a reasonable approach. Taking into account the higher risk for agranulocytosis associated with AIT, particularly within the first three months of ATD therapy, one could consider a closer follow-up of white blood cell counts during the first three months of ATD therapy in AIT patients. Finally, development of reliable means to differentiate between type 1 and type 2 AIT would help reduce the unnecessary risk to which type 2 AIT patients are exposed while their thyrotoxicosis can be managed without ATD.
Conclusions and Implications
This study shows that AIT is associated with a high risk for ATD-related agranulocytosis. These findings have important implications for the management of AIT patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.