
Abstract
Background:
It is unclear whether a history of thyroid cancer is associated with an increased risk of adverse pregnancy outcomes in subsequent pregnancies. This study aimed to evaluate the risk of adverse obstetric outcomes and the abnormal growth of offspring in women with a history of thyroid cancer.
Methods:
This retrospective observational study used nationwide data from between 2006 and 2014 to compare pregnancy outcomes of women with a history of thyroid cancer and those with no such history. Cases of thyroid cancer were identified using ICD-10 codes.
Results:
During the study period, 7232 women with a history of thyroid cancer and 2,269,051 women without a history of thyroid cancer gave birth. The risks of cesarean section, preterm birth, low birth weight, large for gestational age, preeclampsia, placental abruption, placenta previa, and stillbirth were not different between the groups. Women with a history of thyroid cancer had a statistically higher risk of postpartum hemorrhage (odds ratio [OR] = 1.23 [confidence interval (CI) 1.15–1.32], p < 0.05, corrected with the false discovery rate). Additionally, generalized estimating equations analysis showed that there was no difference in the risk of underweight (OR = 1.05 [CI 0.93–1.19]) and obese (OR = 0.94 [CI 0.84–1.05]) offspring assessed over a period of 80 months after adjusting for confounding factors.
Conclusions:
Women with a history of thyroid cancer have similar pregnancy outcomes and offspring growth to those with no such history.
Introduction
Thyroid cancer is the most common malignant endocrine tumor, and its incidence is increasing globally (1 –4). A retrospective analysis in the United States observed on average 3.6% per year (from 4.56% per 100,000 person-years in the period 1974–1977 to 14.42 per 100,000 person-years in the period 2010–2013) (3). It is also the most common cancer in American adults between 16 and 33 years of age (5). Despite the increased incidence, the overall mortality from thyroid cancer has remained stable at 0.46 per 100,000 person-years (3).
In general, there is a higher risk of adverse pregnancy outcomes among survivors of cancer, including preterm birth (risk ratio = 2.8 [confidence interval (CI) = 2.1–3.7), cesarean delivery (odds ratio [OR] = 1.75 [CI 1.43–2.15]), postpartum hemorrhage (PPH; OR = 1.56 [CI 1.09–2.23]), and low birth weight (LBW; OR = 2.02 [CI 1.15–3.55]) (6 –10). However, this association varies depending on the type of cancer and the specific pregnancy outcome assessed.
Thyroid hormones play a critical role in the maintenance of maternal health and the development of the fetus during pregnancy (11). Both hypo- and hyperthyroidism in pregnancy may lead to adverse outcomes such as miscarriage, preterm delivery, preeclampsia, and small for gestational age (SGA) births (12 –16). Women who undergo thyroid cancer treatment such as hemi- or total thyroidectomy have an increased risk for developing hypothyroidism during pregnancy (11), and women with thyroid cancer who are on thyrotropin (TSH) suppression therapy may be hyperthyroid (11). Moreover, considering the critical role of thyroid hormones in the maintenance of maternal and offspring health, women with a history of thyroid cancer will face fears and anxiety about possible pregnancy risks and health effects in their offspring, just like survivors of other cancers (17), which are known to be associated with adverse pregnancy outcomes (18,19). Thus, women with a history of thyroid cancer may be at risk for adverse pregnancy outcomes. However, few studies have reported on outcomes for women with a history of thyroid cancer. Although some studies have suggested that such women are not at an increased risk of preterm birth (6 –9), the results were based on small sample sizes, and only a limited number of outcomes were reported. Therefore, this study aimed to evaluate the risk of adverse obstetric outcomes in women previously diagnosed with thyroid cancer.
Methods
In Korea, 97% of the population is enrolled in the Korea National Health Insurance (KNHI) program. All claims information for these individuals is contained within the KNHI claims database. Nearly all information about the prevalence of different diseases can be obtained from this centralized database, with the exception of procedures not covered by insurance. As part of the KNHI system, children aged 4–80 months are eligible for a National Health Screening Program for Infants and Children (NHSP-IC). An NHSP-IC is composed of seven consecutive health examinations based on age groupings. The first to the seventh health examinations are performed at 4–9, 9–18, 18–30, 30–42, 42–54, 54–66, and 66–80 months, respectively. An NHSP-IC consists of history taking, physical examination, anthropometric examination, developmental screening, and visual acuity testing based on the child's age. Women's data in the KNHI claims database were linked to the data of their offspring contained within the NHSP-IC database.
Data on women's health conditions including obstetric diagnosis were obtained from the KNHI claims database using ICD-10 codes (Supplementary Table S1). Data on preterm birth and birthweight were corrected from the NHSP-IC database.
Data set and outcomes
Using the KNHI claims database, this study identified all women who had given birth between January 1, 2007, and December 31, 2014. It also identified whether these women had thyroid cancer based on ICD-10 codes and whether this form of cancer had occurred prior to giving birth.
Figure 1 shows the flow chart of study participants' enrollment. To identify the stillbirth rate as an adverse pregnancy outcome among women who had given birth between January 1, 2007 and December 31, 2014, women who had thyroid diseases or other cancers prior to the study period (data set 1) were excluded. Using data set 1, stillbirth was identified based on ICD-10 codes.
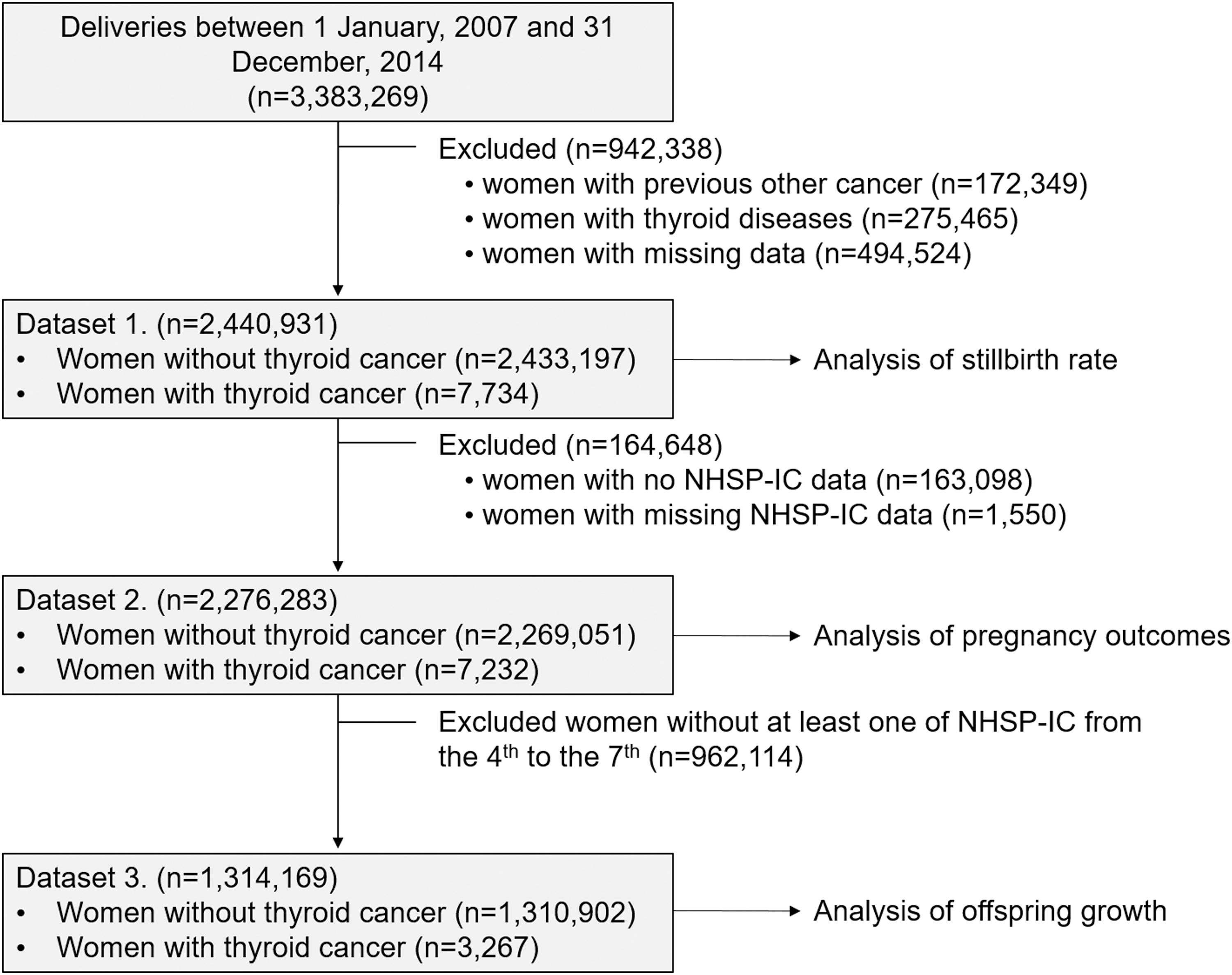
Flow chart of the enrollment of study participants. NHSP-IC, National Health-Screening Program for Infants and Children.
For the other outcomes, the KNHI claims database and the NHSP-IC database were merged. Women were excluded from analysis if their offspring did not undergo at least one of the seven consecutive NHSP-IC examinations or had missing data (data set 2). Data regarding maternal and offspring outcomes were extracted from data set 2. This information included pregnancy outcomes such as delivery mode, preeclampsia, PPH, placental abruption, and placenta previa from the KNHI claims database, and preterm birth, LBW, and large for gestational age (LGA) from the NHSP-IC database. Preterm birth was defined as gestational age <37 weeks. LBW was defined as birth weight <2.5 kg. LGA was defined as birth weight >4.0 kg.
Offspring growth was assessed using body mass index (BMI) measurements, which were taken between 30 and 80 months of age (from the fourth to the seventh NHSP-IC examinations). For this analysis, women were excluded from analysis if their offspring did not undergo at least one NHSP-IC examination from the fourth to the seventh or had missing data (data set 3). Current BMI was categorized according to age- and sex-specific BMI, which was derived from a NHSP-IC (20). Underweight was defined as a BMI ≤10th percentile, and obesity was defined as a BMI ≥90th percentile.
Covariate
Covariate data included maternal age, primiparity, incomes, pre-pregnancy hypertension (HTN), and pre-pregnancy diabetes mellitus (DM). As employee health insurance premiums reflect a worker's salary, the study used premiums as a substitute variable for income level. Pre-pregnancy insurance premiums were classified into five quintiles of performance, with the highest income level in Q5. Pre-pregnancy HTN and pre-pregnancy DM were identified using ICD-10 codes.
Statistical analysis
Continuous and categorical variables are expressed as the mean ± standard deviation and percentages, respectively. Clinical characteristics were compared using the t-test for continuous variables and the chi-square test for categorical variables. Multivariable logistic regression analysis was used to estimate the adjusted OR and the CIs for the association of a history of thyroid cancer with adverse pregnancy outcomes. For multivariable analyses, a fixed set of known risk factors for adverse pregnancy outcomes was adjusted for potential confounding: maternal age (continuous variable), primiparity (categorical variable), income (categorical variable), pre-pregnancy HTN (categorical variable), and pre-pregnancy DM (categorical variable). Results were considered significant if they reached p < 0.05, corrected with the false discovery rate (FDR).
The risk of underweight and obese offspring, in relation to the presence or absence of a maternal history of thyroid cancer, was also evaluated using multivariable logistic regression analysis at each follow-up period of NHSP-IC, using data from the fourth, fifth, sixth, and seventh screening examination results.
Generalized estimating equations (GEE) were used to evaluate the association between a maternal history of thyroid cancer and offspring growth longitudinally, considering the correlation between repeated measurements in the same individual. Statistical analyses were performed using SAS for Windows v9.4 (SAS, Inc., Cary, NC). The study protocol was approved by the Institutional Review Board of the Korea University Medical Center.
Results
Among 2,276,283 women who gave birth during the study period, 7232 (0.32%) women had a history of thyroid cancer. The median interval (95% range) from the diagnosis of thyroid cancer to delivery was 3.1 years (0.7–8.3 years).
Table 1 shows the basic characteristics of the two groups. Women with a history of thyroid cancer tended to be older, with a higher prevalence of pre-pregnancy HTN and DM. The distribution of income was different between the two groups.
Basic Participant Characteristics Stratified by a Maternal History of Thyroid Cancer
Values are expressed as the mean (SD) or n (%). Advanced age was defined as age ≥35 years.
HTN, hypertension; DM, diabetes mellitus.
Table 2 shows the pregnancy outcomes between the two groups. Women with a history of thyroid cancer had a higher prevalence of multiple gestations, cesarean section, preterm birth, LGA, preeclampsia, PPH, and placenta previa. However, birth weight and the prevalence of LBW, placental abruption, and stillbirth were not different between the two groups.
Pregnancy Outcomes of Participants Stratified by a Maternal History of Thyroid Cancer
Values are expressed as the mean (SD) or n (%).
LBW, low birth weight; LGA, large for gestational age; PPH, postpartum hemorrhage.
Table 3 shows the risk of developing adverse pregnancy outcomes according to the presence or absence of a history of thyroid cancer. On unadjusted analysis, women with a history of thyroid cancer had a higher risk of multiple gestations (OR = 1.43 [CI 1.21–1.69]), cesarean section (OR = 1.13 [CI 1.08–1.19]), preterm birth (OR = 1.18 [CI 1.04–1.34]), LGA (OR = 1.16 [CI 1.03–1.30]), preeclampsia (OR = 1.33 [CI 1.15–1.54]), PPH (OR = 1.24 [CI 1.16–1.33]), and placenta previa (OR = 1.46 [CI 1.21–1.76]). However, there were no differences in the risk of LBW (OR = 1.11 [CI 0.99–1.24]), placental abruption (OR = 1.22 [CI 0.86–1.73]), and stillbirth (OR = 1.06 [CI 0.84–1.34]) between the groups. When adjusted for age, primiparity, incomes, pre-pregnancy HTN, and pre-pregnancy DM, women with a history of thyroid cancer continued to have a higher risk of multiple gestations (OR = 1.19 [CI 1.00–1.40], p < 0.01 FDR corrected) and PPH (OR = 1.12 [CI 1.01–1.25], p < 0.01 FDR corrected).
Multiple Logistic Regression Analysis with Adverse Pregnancy Outcomes as a Dependent Variable and the History Of Thyroid Cancer as an Independent Variable
Adjusted for maternal age, primiparity, incomes, pre-pregnancy HTN, and pre-pregnancy DM.
OR, odds ratio; CI, confidence interval; FDR, false discovery rate.
Table 4 shows the offspring BMI, prevalence and associations between maternal history of thyroid cancer, and underweight and obesity in offspring until 80 months of age. Until 80 months of age, the BMI of the offspring of women with a history of thyroid cancer did not differ from that of the offspring of women without a history of thyroid cancer. The prevalence of underweight or obese offspring of women with a history of thyroid cancer did not differ from those of women without a history of thyroid cancer group. On multivariable regression analysis, the risk of underweight or obese offspring was not different between the two groups at each follow-up period of NHSP-IC, from 30 to 80 months.
BMI, Prevalence, and Associations Between a Maternal History of Thyroid Cancer and Underweight and Obese Offspring Until 80 Months of Age
p-Value for difference in BMI between the groups.
p-Value for difference in prevalence between the groups.
Adjusted for maternal age, maternal income, maternal pre-pregnancy HTN, maternal pre-pregnancy DM, preterm birth, maternal preeclampsia, cesarean section, LBW, and LGA.
BMI, body mass index.
When repeated underweight and obesity status measurements at each follow-up period were considered using GEE, the risk of being underweight (OR = 1.05 [CI 0.93–1.19]) or obese (OR = 0.94 [CI 0.84–1.05]) was not different in the offspring of women with a history of thyroid cancer after adjustment for maternal age, primiparity, maternal income, maternal pre-pregnancy HTN, maternal pre-pregnancy DM, preterm birth, maternal preeclampsia, cesarean section, LBW, and LGA compared to that of women without a history of thyroid cancer group.
Discussion
In this study, women with a history of thyroid cancer had a higher risk of PPH compared to women without a history of thyroid cancer, after adjustment for other factors related to PPH, in line with the results from a study that reported cancer survivors having higher rates of PPH (10). The mechanism through which a history of thyroid cancer affects the development of PPH is unclear. However, there are several possible explanations. First, as with other cancers, a history of thyroid cancer makes these women more likely to encounter increased surveillance and more accurate measurement of blood loss, as they are perceived to be high risk (10). As blood loss at delivery is often subjectively measured (21), women with a history of thyroid cancer are more likely to be diagnosed with PPH. Second, several animal studies undertaken to investigate the effect of thyroid dysfunction on pregnant uterine tissue found an effect of low levels of T4 on uterine contractile activity, indicating that thyroid dysfunction may affect uterine responsiveness to agonists (22,23). Thus, as physiological biochemical hypothyroidism may occur in early pregnancy in women who undergo thyroid cancer treatment such as hemi- or total thyroidectomy before pregnancy (11) or use the thyroxine (24), the risk of PPH in women with a history of thyroid cancer may be attributed to abnormal uterine contraction due to abnormal thyroid function. However, patients with thyroid cancer, who are on TSH suppression therapy may be hyperthyroid (11), and moreover it is recommended that thyroid function is evaluated in patients with thyroid cancer as soon as pregnancy is confirmed and that thyroid function is monitored carefully in order to avoid hypothyroidism (11). Therefore, it is unlikely that these patients have abnormal thyroid function throughout pregnancy. Of note, it has been reported that thyroid cancer treatments, such as radioactive iodine (RAI) therapy, are associated with a significant decline in hemoglobin (Hb) levels one year after the last RAI therapy (25). Given that a low Hb concentration is one of the major risk factors for PPH (26), the higher risk of PPH in women with a history of thyroid cancer may simply be due to low Hb levels before pregnancy. However, in this study, the median interval from the diagnosis of thyroid cancer to delivery was 3.1 years (range 8 months–8.3 years), which falls outside the window of waiting for six months post radioactive iodine for those women who were treated and then wished to conceive (11). Thus, this makes it unlikely that this was a RAI effect. It has been reported that in Korea approximately 85% of the patients with thyroid cancer undergo total thyroidectomy as the initial surgery (27), and nearly half of patients receive RAI therapy (28). However, specific data on these variables were not available for this study population. Further studies characterizing other variables such as extent of surgery, RAI therapy, post-treatment thyroid hormone replacement, and Hb levels are warranted to confirm the present findings further.
In this study, women with a history of thyroid cancer were more likely to have multiple gestations. Another study also showed similar trends in women using thyroxine, although these trends were not statistically significant (OR = 1.13 [CI 0.96–1.32]) (29). This may be due to the higher frequency of treatment for subfertility with assisted reproductive technology in these women rather than a phenomenon associated with the thyroid cancer itself (30).
It has been reported that cancer survivors have a higher risk of preterm birth in subsequent pregnancies (6 –10) and that this risk may be attributed to the long-term effects of cancer treatments such as chemotherapy (7,31). In this study, a history of thyroid cancer was associated with preterm delivery in unadjusted analysis, but statistical significance disappeared after further adjustment for confounding factors. These results are consistent with the results of sub-analyses from other studies (6 –9). Also, RAI therapy for thyroid cancer has not been found to be associated with a risk of preterm birth (32,33).
It has been reported that women with abnormal thyroid function have a higher risk of preeclampsia compared to controls (12,13) due to endothelial dysfunction (34), which is known to play a pivotal role in the pathophysiology of preeclampsia (35). However, the risk of preeclampsia and other placental conditions such as placental abruption and placenta previa was not found to be increased in this study. Several studies have previously reported an association between all-cancer survival and preeclampsia (9,10). The study presented here evaluated for the first time the effects of maternal thyroid cancer on the development of preeclampsia.
In this study, a maternal history of thyroid cancer was not associated with the birth weight of offspring, in agreement with the results of previous studies (6,7,9). To the best of the authors' knowledge, this study is the first to evaluate the effect of a maternal history of thyroid cancer on the growth of offspring until 80 months of age, and it was found that a maternal history of thyroid cancer was not associated with the growth of offspring or the risk of underweight and obese offspring. These results are likely to reassure women with thyroid cancer concerned about the growth of their offspring.
The information on preterm birth and birthweight were corrected based on data from the NHSP-IC database. Thus, to estimate the risk of preterm birth, LBW, and LGA, women were excluded from analysis if their offspring did not undergo at least one of the seven consecutive health examinations offered by NHSP-IC or had missing data in data set 2, which might increase the influence of the inherent selection bias factor. However, when reanalyzed using the data before excluding them, the same association of a history of thyroid cancer with other adverse pregnancy outcomes was found (Supplementary Table S2). Thus, it is unlikely to have influenced the association between a history of thyroid cancer and adverse pregnancy outcomes. In addition, offspring growth was assessed using BMI measurements from the NHSP-IC database. As BMI was measured between 30 and 80 months of age (from the fourth to the seventh NHSP-IC health examination), women were excluded from analysis if their offspring did not undergo at least one of the NHSP-IC examinations from the fourth to the seventh in data set 3. However, many of the excluded offspring have not yet reached the age of 30 months. Therefore, a study based on a longer follow-up period is required.
Several limitations need to be considered when interpreting the findings. First, the diagnosis of thyroid cancer in this study was based on insurance claims data from the KNHI claims database, which is designed for cost claim analysis and not for research purposes. Therefore, the main limitation is the validity of the diagnoses in this database. However, the accuracy of diagnostic codes tends to be higher for claims with more severe conditions (36). This would include the diagnoses of cancers including thyroid cancer. Second, detailed information such as pathological type, disease severity, and laboratory data (such as post-treatment thyroid hormone levels) was not included. Some adverse reproductive outcomes (e.g., stillbirths and cytogenetic abnormalities) in female cancer survivors are hypothesized to result from germ cell toxicity caused by mutagenic exposures, and others (e.g., preterm birth and LBW) have been known to be linked to direct abdominal/pelvic radiation-induced damage to the vasculature and elastic properties of the uterus (31,37). Similarly, thyroid cancer treatment such as hemi- or total thyroidectomy may be also associated with adverse pregnancy outcomes through hypothyroidism (11), although data on thyroid cancer treatment such as extent of surgery, RAI therapy, and post-treatment thyroid hormone replacement were lacking. In addition, even though maternal age, primiparity, maternal income, maternal pre-pregnancy HTN, and pre-pregnancy DM were adjusted for, a large number of variables that could act as confounders were not included in the analyses—for example, maternal smoking during pregnancy, use of assisted reproductive methods to achieve pregnancy, and medication use such as anticoagulation (38 –40). Therefore, further studies are necessary to evaluate whether thyroid cancer itself, the effect of cancer treatment, post-treatment thyroid hormone status, or other factors may influence pregnancy outcomes.
Nevertheless, the strength of the present study is that it represents a large population-based study with mother-offspring pairs.
In conclusion, in this study, the risk of PPH was slightly higher in women with a history of thyroid cancer, but other risk factors, including preterm birth and preeclampsia, were not different, and there was no effect of maternal history of thyroid cancer on offspring growth until 80 months of age. These results are likely to reassure women with a history of thyroid cancer intending to have a child.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2