
Abstract
Background:
The recently published eighth edition of the American Joint Committee on Cancer (AJCC) staging system has emphasized the importance of gross extrathyroidal extension (gETE) while classifying the tumor (T) stage in differentiated thyroid carcinoma (DTC). However, the clinical impact of gETE invading only the strap muscles or the recurrent laryngeal nerve (RLN) remains unclear due to scarce and conflicting data.
Methods:
A retrospective cohort study was carried out in patients with DTC who underwent thyroid surgery from 1996 to 2005. In total, 3104 patients were included, and disease-specific survival (DSS) was compared according to the degree of gETE, with a median follow-up duration of 10 years.
Results:
Patients with gETE invading only the strap muscles and with a tumor size ≤4 cm (T3b [≤4 cm]) showed no difference in DSS compared to patients with T2 stage disease (hazard ratio [HR] = 0.81 [confidence interval (CI) 0.24–2.77]; p = 0.737) but rather showed a better DSS than patients with T3a disease (HR = 0.19 [CI 0.05–0.72]; p = 0.014). Conversely, patients with gETE invading to the posterior direction showed significantly poorer DSS than patients with T3 stage disease, even when only the RLN was invaded (HR = 7.78 [CI 3.41–17.75]; p < 0.001). However, there was no difference in DSS between gETE invading only the RLN and that invading other posterior organs beyond the RLN (p = 0.563). A modified T classification was suggested to downgrade patients with T3b (≤4 cm) disease to the T2 stage, which revealed higher predictability of survival than the T classification according to the eighth edition of the American Joint Committee on Cancer tumor-node-metastasis staging system (proportion of variation explained: 3.6% vs. 2.65%).
Conclusions:
gETE invading only the strap muscles did not significantly affect DSS, while that invading the posterior organs significantly affected DSS, even when only the RLN was invaded. The data support the applicability of downgrading patients with T3b (≤4 cm) disease to the T2 stage for a better predictability of survival.
Introduction
Extrathyroidal extension (ETE) is defined as the involvement of perithyroidal structures by direct extension from the primary thyroid cancer (1). ETE ranges from minimal ETE, ETE detected by histological examination, to gross ETE (gETE), ETE detected by radiological and/or intraoperative evidence. The incidence of ETE in differentiated thyroid carcinoma (DTC) ranges from 5% to 34% (2 –5), and it has been established as an important prognostic factor along with other factors, such as age, tumor size, and cervical lymph node (LN) metastasis (3,4,6).
The recently published eighth edition of the American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) staging system (TNM-8) has placed a high importance on gETE and eliminated minimal ETE in T staging (1). Previous studies have revealed that minimal ETE is not an independent factor for poor prognosis (7 –9). Thus, it is now no longer a variable while determining the T classification. However, gETE remains a significant prognostic factor. According to the TNM-8, gETE is classified into three stages, depending on its extent: T3b disease (gETE involving only the strap muscles); T4a disease (gETE invading subcutaneous soft tissues, larynx, trachea, esophagus, or the recurrent laryngeal nerve [RLN]); and T4b disease (gETE invading prevertebral fascia or encasing the carotid artery or mediastinal vessels).
The strap muscles (53%) and RLN (47%) are two of the most commonly invaded structures in locally invasive thyroid cancer, followed by the trachea (37%) (10). They represent the structures most closely adjacent to the thyroid gland in the anterior or posterior direction, respectively. However, whether gETE invading the strap muscles or RLN independently leads to adverse outcomes remains unclear because of scarce and discordant published data (10 –12). To verify this issue, the clinical impact of gETE on disease-specific survival (DSS) of patients with DTC was compared according to the extent of gETE, with the focus on gETE invading only the strap muscles or the RLN. The predictability of survival was analyzed by calculating the proportion of variation explained (PVE) on the basis of modified T classification.
Methods
Study design and patients
This retrospective cohort study was carried out with 3104 patients with DTC who underwent initial thyroid surgery from 1996 to 2005 at the Asan Medical Center (Seoul, Korea). All the included patients were >18 years of age and were pathologically proven as having papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma (FTC), including Hürthle cell carcinoma. Data collection and subsequent analysis were approved by the Institutional Review Board of the Asan Medical Center.
Definitions of T stages
Patients were initially classified into five groups according to the T classification of the TNM-8 (1): T1 disease (tumor ≤2 cm in the greatest dimension but limited to the thyroid), T2 disease (tumor >2 cm but ≤4 cm in the greatest dimension but limited to the thyroid), T3a disease (tumor >4 cm but limited to the thyroid), T3b disease (gETE invading only the strap muscles from tumor of any size), and T4a disease (gETE invading the subcutaneous soft tissues, larynx, trachea, esophagus, or RLN from tumor of any size). There were no patients who presented with T4b stage disease.
For a more detailed evaluation of the clinical impact of gETE, patients with T3b disease were divided into two groups according to tumor size: (i) those with gETE invading only the strap muscles with tumor size ≤4 cm (T3b [≤4 cm]) or (ii) those with tumor size >4 cm (T3b [>4 cm]). Additionally, pathology reports, operation records, and preoperative thyroid ultrasound were reviewed in all patients with T4a disease to assess the extent of gETE. Patients were classified into those with gETE (i) invading only the RLN, (ii) invading only subcutaneous tissue, and (iii) invading other major structures, such as the esophagus, trachea, or larynx. Patients with lesions with gETE who fell into more than one category were classified in the higher group. Because there were no patients with T4a disease with gETE invading only subcutaneous tissue, they were divided into two groups: (i) those with gETE only in the RLN (T4a [RLN]) and those with gETE invading beyond the RLN to other major organs (T4a [others]).
Primary outcome
The primary outcome of this study was death from DTC. DSS, defined as the time from the date of surgery until death from DTC or last censoring, was compared according to the T stage.
Statistical analysis
R v3.4.0 and R libraries car, Cairo, survival, and survminer were used for data analysis and drawing graphs (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline characteristics
Table 1 summarizes the baseline clinicopathologic characteristics of the 3104 patients with DTC. The median age was 45.9 years (IQR 37.8–54.2 years), with a female predominance of 87.4%. Most patients were diagnosed with PTC (n = 2987; 96.2%), while the remaining 3.8% presented with FTC. Cervical LN metastasis was identified in 1520 (48.9%) patients, and 53 (1.7%) patients showed initial distant metastasis. The median follow-up duration was 10 years (IQR = 8.1–12 years).
Baseline Clinicopathologic Characteristics of Patients with DTC
Continuous variables are presented as the median (IQR). Categorical variables are presented as n (%).
DTC, differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; LN, lymph node; RAI, radioactive iodine; RLN, recurrent laryngeal nerve; AJCC, American Joint Committee on Cancer; TNM, tumor-node-metastasis; IQR, interquartile range.
The distribution of patients according to each T stage was as follows: T1 in 1997 (64.3%) patients, T2 in 496 (16.0%) patients, T3a in 96 (3.1%) patients, T3b (≤4 cm) in 376 (12.1%) patients, T3b (>4 cm) in 38 (1.2%) patients, T4a (RLN) in 61 (2.0%) patients, and T4a (others) in 40 (1.3%) patients.
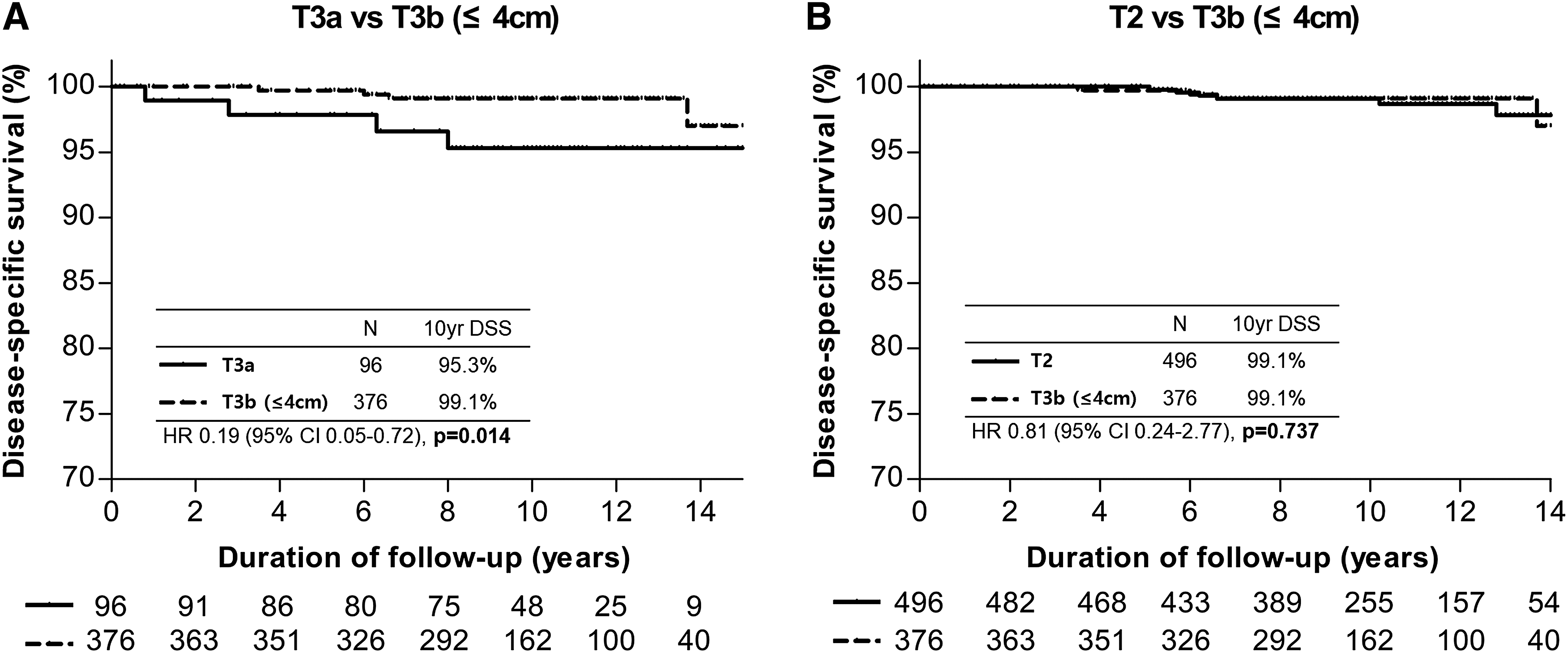
Prognostic impact of gETE invading only the strap muscles on DSS
While patients with gETE invading only the strap muscles are classified as T3b disease regardless of tumor size, this study compared the DSS of patients with T3b (≤4 cm) with T3a and T2 disease in order to evaluate the clinical impact on survival of patients with gETE invading only the strap muscles (Fig. 1). Figure 1A indicates that patients with T3b (≤4 cm) disease showed a significantly better DSS than patients with T3a disease (hazard ratio [HR] = 0.19 [confidence interval (CI) 0.05–0.72]; p = 0.014). Moreover, as shown in Figure 1B, there was no significant difference between the DSS of patients with T3b (≤4 cm) and those with T2 disease (HR = 0.81 [CI 0.24–2.77]; p = 0.737). Taken together, it was assumed that gETE invading only the strap muscles had minimal impact on survival, and the emphasis should be placed on tumor size. Therefore, patients with T3b (≤4 cm) disease were merged into the T2 category, and patients with T3a and T3b (>4 cm) disease were combined as T3. Based on this modification, 376 (12%) patients were downgraded.
Disease-specific survival (DSS) according to T stage. (
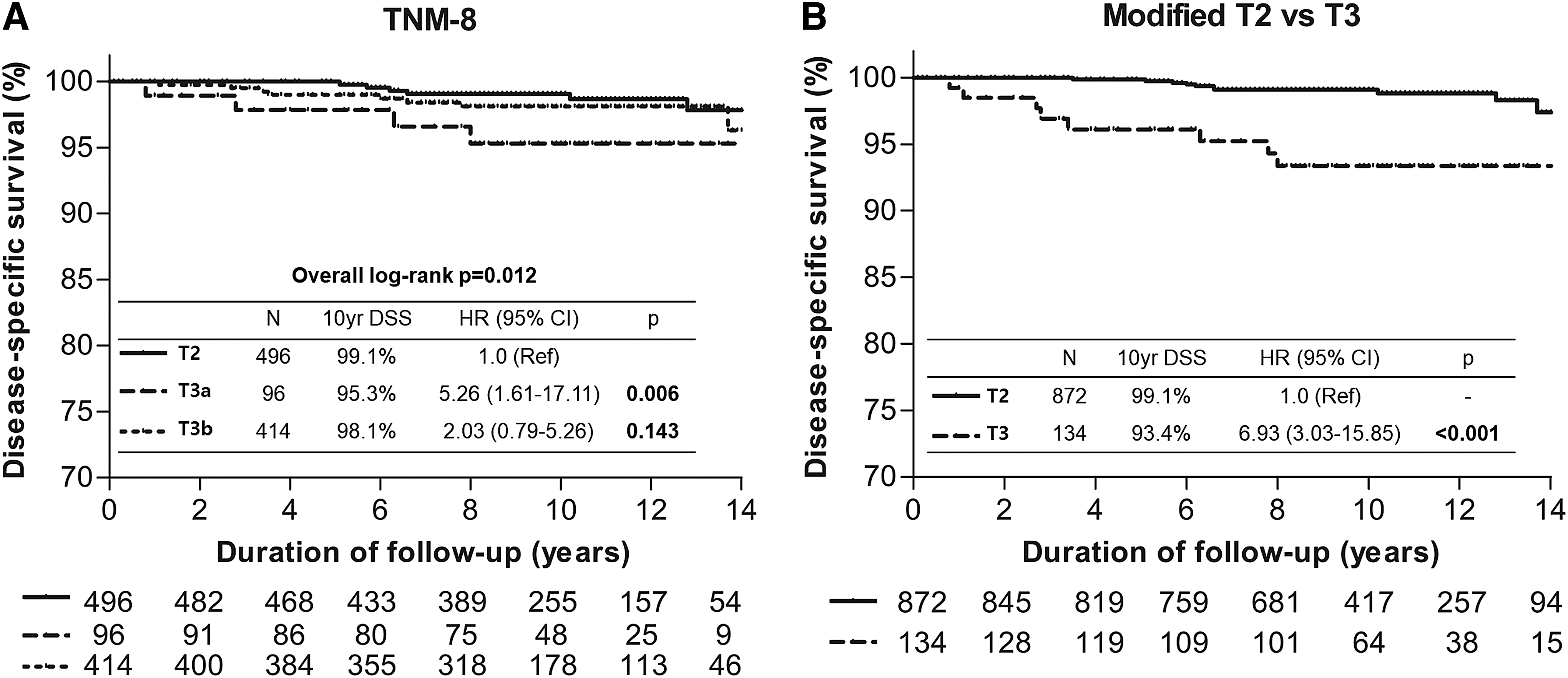
The DSS rates of patients with T2 and T3 stage disease were analyzed according to the TNM-8 (Fig. 2A) and modified T category, as described above (Fig. 2B). Unlike the inverse association of DSS between patients with T3a and T3b disease and no difference between patients with T2 and T3b tumors, the DSS of patients with T2 and T3 tumors after modification presented a more simplified and significant difference between the two groups (HR = 6.93 [CI 3.03–15.85], p < 0.001).
Comparison of DSS between T stages 2 and 3 according to (
Prognostic impact of gETE invading only the RLN on DSS
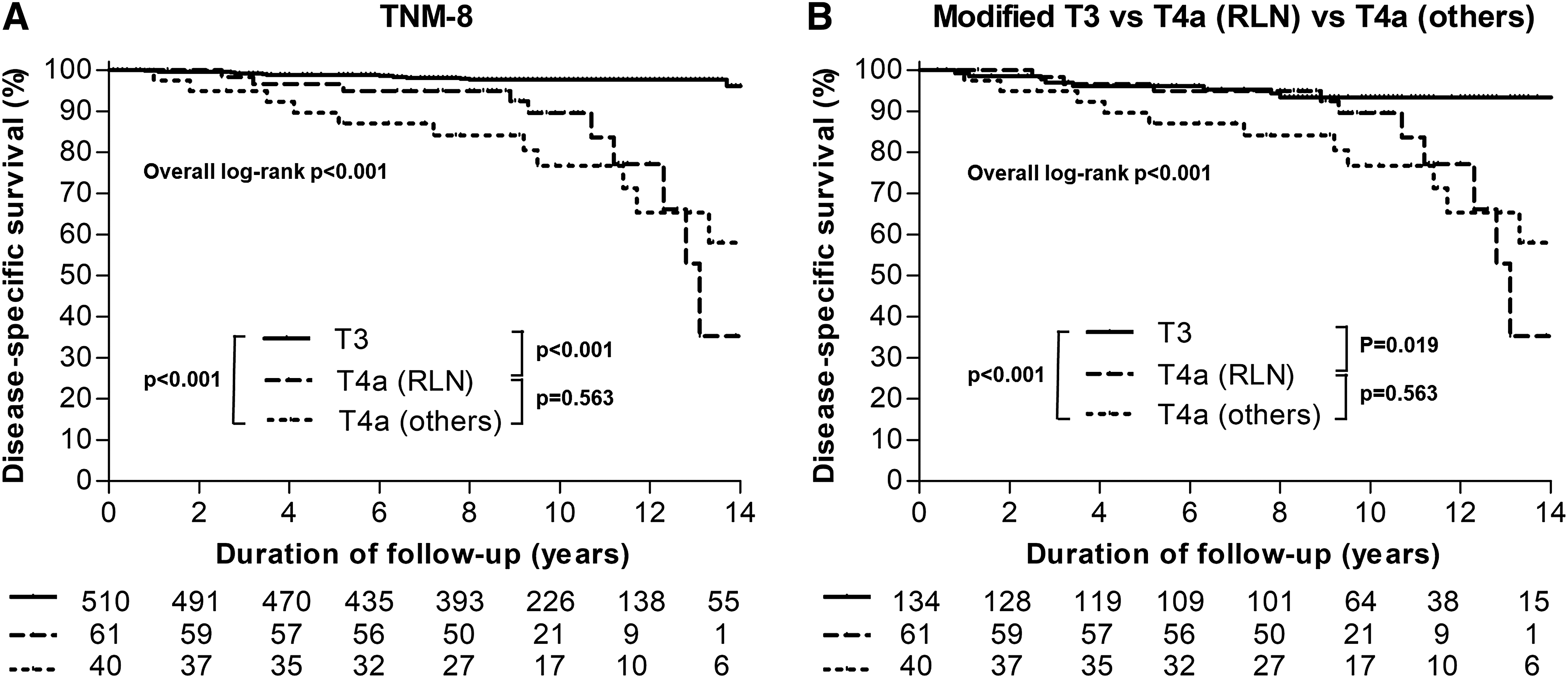
To determine the clinical impact of gETE invading only to the RLN and no organ beyond the RLN, DSS rates of patients with T3 (including T3a and T3b), T4a (RLN), and T4a (others) stages were compared. As indicated in Figure 3A, patients with T4a (RLN) disease showed a significantly poorer DSS than patients with T3 disease (HR = 7.78 [CI 3.41–17.75]; p < 0.001). Patients with T4a (others) disease showed an evidently poorer DSS than patients with T3 disease (HR = 11.88 [CI 5.65–24.98]; p < 0.001). However, there was no significant difference in DSS between patients with T4a (RLN) and T4a (others) disease (HR = 1.29 [CI 0.54–3.05]; p = 0.563).
Comparison of DSS between T3 and T4a after dividing T4a patients into T4a (recurrent laryngeal nerve) and T4a (others) according to (
Figure 3B illustrates the DSS of patients with modified T3 disease (removal of T3b (≤4 cm) as defined earlier), those with T4a (RLN) disease, and those with T4a (others) disease. Patients with T4a (RLN) disease continued to show significantly poorer DSS than patients with modified T3 disease (HR = 2.90 [CI 1.19–7.08]; p = 0.019).
Univariate/multivariate analysis for DSS
Cox proportional hazard regression analysis for variables associated with DSS was performed, including age, sex, tumor size, cervical LN metastasis, distant metastasis, along with the extent of gETE (Table 2). In univariate analysis, all of these factors increased the disease-specific mortality. However, in multivariate analysis, gETE invading only the strap muscles was not associated with DSS while gETE invading other major organs (corresponding to T4 stage) significantly increased disease-specific mortality (HR = 4.83 [CI 2.41–9.70], p < 0.001).
Univariate and Multivariate Analysis for DSS
Statistically significant values are shown in bold.
DSS, disease-specific survival; HR, hazard ratio; CI, confidence interval; Y, yes; gETE, gross extrathyroidal extension.
Comparison of T stage of the TNM-8 and the modified T stage
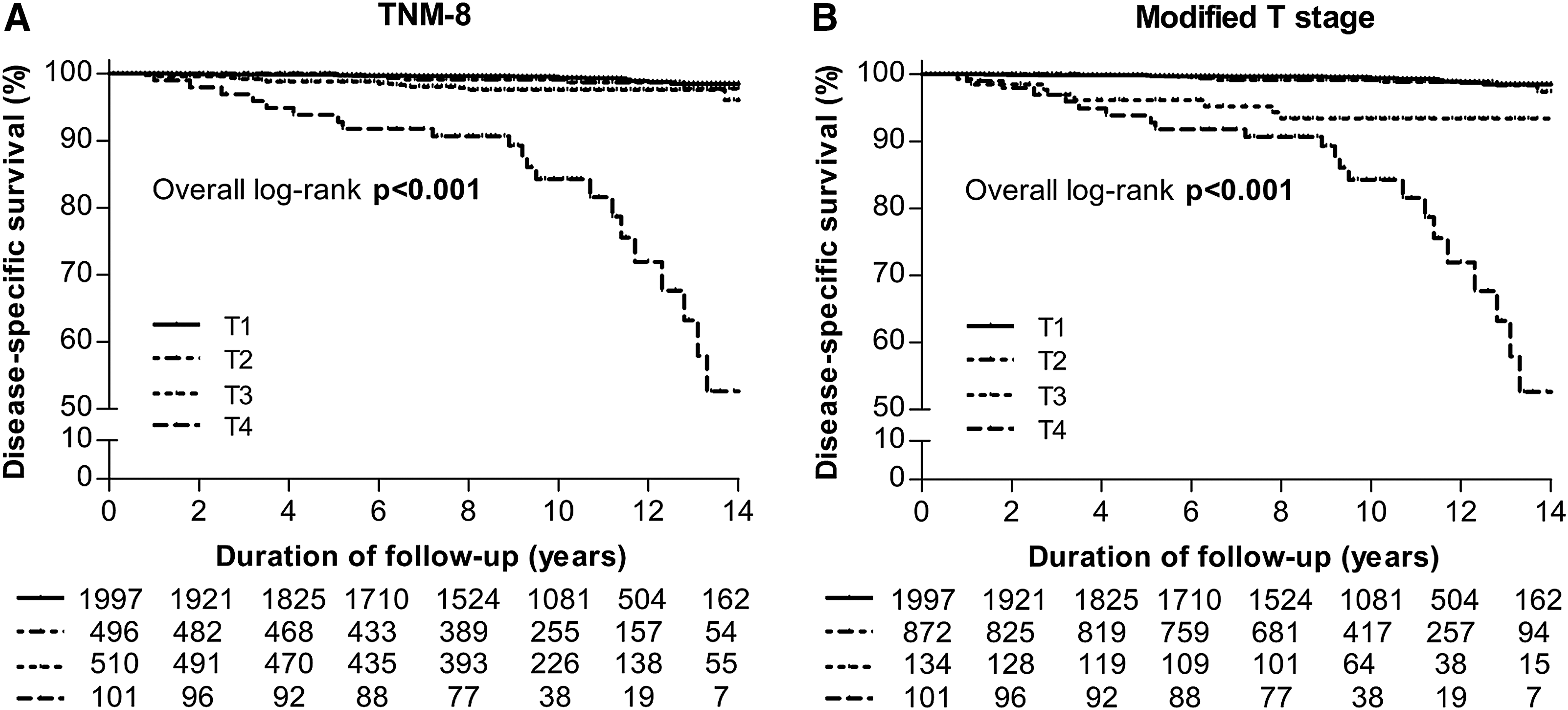
Figure 4 illustrates the comparison of DSS according to the T category of the TNM-8 (Fig. 4A) and the modified T stage (Fig. 4B), in which original patients with T3b (≤4 cm) disease were downgraded to T2 tumors. Both classifications predicted DSS with statistical significance (p < 0.001 and 0.001, respectively, by log-rank). However, the modified T category yielded a better survival prediction with a PVE of 3.6% compared to the T stage of the TNM-8 with a PVE of 2.65% (Table 3).
DSS according to (
Cox Regression Model and the PVE of the T Staging System According to TNM-8 and Modified T Stage
PVE, proportion of variation explained; TNM, tumor-node-metastasis.
Discussion
The clinical impact of gETE invading only the strap muscles or RLN—the two most closely adjacent structures to the thyroid gland in the anterior and posterior direction, respectively—is not well understood. To fill this research gap, this study investigated DSS according to the severity of gETE. In this study, patients with T3b (≤4 cm) disease showed no difference in DSS compared to those with T2 disease but rather showed better DSS compared to those with T3a stage disease. This allowed the patients with T3b (≤4 cm) disease to be downgraded to the T2 stage, which accounted for 12% of the patients in the study. In addition, patients with T4a (RLN) disease showed significantly poorer DSS than patients with T3 stage disease, while they showed no significant difference in DSS compared to the patients with T4a (others) disease. These findings indicate that gETE invading to the posterior direction has a significant impact on DSS, even when gETE invades the RLN only. Furthermore, the modified T classification based on these results showed a better predictability of survival than the T classification of the TNM-8.
One of the major findings of this study was that gETE invading only the strap muscles did not affect DSS. This is in agreement with the findings of a previous study, which was undertaken to determine the long-term outcomes of patients with gETE only in the strap muscles compared to patients without ETE or with minimal ETE (11). In that study, no significant differences were observed in 10-year cancer-specific survival rates of three groups. The present results additionally revealed that patients without gETE but with a tumor size >4 cm (T3a) showed worse DSS than patients with gETE only in the strap muscles. This may be attributed to the fact that patients with T3a disease showed higher rates of distant metastasis than patients with T3b (≤4 cm) disease (T3a, 5.0% vs T3b [≤4 cm], 2.4%). When patients with distant metastasis at initial presentation were excluded, there was no significant difference in DSS (HR = 0.92 [CI 0.12–9.22], p = 0.939) between the two groups. Thus, patients with a large tumor size have a higher possibility of developing distant metastases, consequently associated with poorer survival.
While gETE to the anterior direction showed little impact on the long-term outcomes, gETE to the posterior direction significantly affected DSS, even when only the RLN was invaded. Previous studies, although few, have reported conflicting results of the clinical significance of gETE invading only the RLN. McCaffrey et al. reported that RLN invasion had no independent influence on survival (10). In contrast, Ito et al. reported that RLN invasion was associated with worse recurrence-free survival compared to no or minimal ETE (12). The present results support the latter, since patients with T4a (RLN) disease showed an approximately eight times higher probability of mortality than patients with T3 stage disease. The reason gETE to the posterior direction has worse clinical outcomes than gETE to the anterior side may be attributed to the greater feasibility of achieving complete resection of cancer invading to the anterior. Another important finding is that patients with gETE invading only the RLN did not show a significant difference in DSS compared to patients with gETE invading other posterior organs beyond the RLN, such as the trachea or esophagus. This result is discordant with the results of the aforementioned study (12). There are some explainable reasons for this discrepancy, such as differences in the extent of the invasion, depth of organs, and the extent of surgical resection (complete or conservative). Specifically, tracheal invasion is commonly classified into four stages on the basis of the depth of invasion (15). While stage I disease, characterized by tumor abutting but not invading the external perichondrium of the trachea, shows no difference in recurrence or survival rate compared to disease without airway involvement, stage II or higher disease is associated with higher recurrence and shorter overall survival (16). Moreover, performing conservative surgery, such as a shave procedure for tracheal invasion, may result in worse survival than performing radical resection (17,18). Further studies considering these factors are necessary to determine the impact of gETE invading to the posterior more precisely.
A strength of the present study is that detailed survival analysis according to the extent of gETE was performed in a relatively large study population with a long duration of follow-up. Further, the modified T classification, which downgraded 12% of the patients, showed a better predictability of survival than the T classification of the TNM-8. However, when this modification was applied to the overall TNM stage, only 44 (1.4%) patients were downgraded from stage II to stage I after removing patients aged <55 years or with LN metastasis (Supplementary Table S1). Further studies with more patients aged ≥55 years are necessary to evaluate this modification more accurately. Also, since this study was a retrospective single-center study at a tertiary medical center, selection bias cannot be eliminated, which may limit the generalization of the findings on a broader scale.
In conclusion, gETE invading only the strap muscles does not show significant influence on survival and highlights the relevance of downgrading patients with T3b (≤4 cm) disease to the T2 stage. In addition, unlike gETE invading only the strap muscles, gETE invading to the posterior significantly affects DSS, even when only the RLN is invaded. This confirms the importance of the direction of invasion beyond the thyroid capsule and the involved sites.
Footnotes
Acknowledgments
This study was supported by the National Research Foundation of Korea Research Grant (NRF-2015R1C1A1A02036597) and a grant (no. 2018-582) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Author Disclosure Statement
The authors declare no potential conflict of interest.