
Abstract
Background:
Maternal hypothyroidism has been associated with adverse pregnancy outcomes. A large nationwide register-based cohort with data on medication purchases was established to study the associations between maternal hypothyroidism, levothyroxine (LT4) use, and pregnancy and perinatal complications.
Methods:
The data included all singleton births between 2004 and 2013 (N = 571,785) in Finland. Hypothyroid mothers (n = 16,364) were identified in the Finnish Medical Birth Register. Of these women, 95.8% used LT4 medication, and 37.5% had consistent LT4 use during pregnancy. Hypothyroid mothers were compared to mothers without thyroid disease (N = 550,860) using logistic regression. The main outcome measures were pregnancy and perinatal complications.
Results:
Maternal hypothyroidism was associated with several pregnancy and perinatal complications, including gestational diabetes mellitus (odds ratio [OR] = 1.19 [confidence interval (CI) 1.13–1.25]), gestational hypertension (OR = 1.20 [CI 1.10–1.30]), severe preeclampsia (OR = 1.38 [CI 1.15–1.65]), cesarean section (OR = 1.22 [CI 1.17–1.27]), preterm births (OR = 1.25 [CI 1.16–1.34]), large-for-gestational age newborns (OR = 1.30 [CI 1.19–1.42]), major congenital anomalies (OR = 1.14 [CI 1.06–1.22]), and neonatal intensive care unit admission (OR = 1.23 [CI 1.17–1.29]). However, among mothers with consistent LT4 purchases, only the associations between gestational diabetes mellitus (OR = 1.12 [CI 1.03–1.22]), cesarean section (OR = 1.13 [CI 1.06–1.21]), neonatal intensive care unit admission (OR = 1.09 [CI 1.01–1.29]), and large-for-gestational age newborns (OR = 1.26 [CI 1.10–1.45]) and maternal hypothyroidism remained.
Conclusions:
Maternal hypothyroidism is associated with several pregnancy and perinatal complications, but consistent LT4 use may reduce many of the risks.
Introduction
O
Subclinical or inadequately treated maternal hypothyroidism has been associated with adverse pregnancy outcomes, including spontaneous abortions (3,8,9), gestational hypertension or preeclampsia (3,10 –13), gestational diabetes mellitus (GDM) (3,10,11,14 –16), preterm delivery (2,3,11), low birth weight (15), placental abruption (2), and fetal death (14). Positive maternal thyroid autoantibodies in euthyroid women have been associated with miscarriage (8), preterm birth (8,17), and perinatal mortality (18). Moreover, cesarean section (CS) (9 –11,16), induction of labor (10), and neonatal intensive care unit (NICU) admission (11) have all been associated with maternal hypothyroidism. However, not all studies have found an increased risk of adverse outcomes associated with maternal subclinical hypothyroidism (1,19,20).
A large register- and population-based cohort with data on medication purchases during pregnancy was established to study if maternal hypothyroidism is associated with pregnancy or perinatal complications and how consistent LT4 use impacts these associations.
Methods
The data are based on the Finnish Medical Birth Register (MBR; established in 1987 and maintained by the National Institute for Health and Welfare) and included all births in Finland between 2004 and 2013 (N = 589,459). After excluding multiple pregnancies (n = 17,674), the data consisted of 357,293 women with 571,785 singleton pregnancies.
For each delivery in Finland, personnel at the delivery hospital complete a structured form of the MBR at hospital discharge or at seven days after delivery, whichever occurs first. In Finland, practically all women give birth in delivery hospitals led by obstetricians; planned home births are very rare, with 13 per year during the study period. The MBR includes data on all live births and stillbirths with birth weight ≥500 g or gestational age at birth ≥22 weeks, with key perinatal and newborn data up to the age of seven days. Maternal data from the MBR include age, occupation, place of residence, marital status, pregnancy history, smoking status, diseases, hospitalization during pregnancy, and mode of delivery. Data on the newborn include sex, gestational age at birth, birth weight, height, head circumference, umbilical artery and vein pH, diagnosis, treatment, and hospitalization during the perinatal period. The data quality of the MBR is good or satisfactory when compared to hospital record data (21), and the usefulness of MBR increases when data from other registers are used (22).
Information on major congenital anomalies was obtained from the Finnish Malformation Register, which includes information on all newborns in Finland with at least one detected major congenital anomaly classified and coded according to the extended International Classification of Diseases version 9 (ICD-9). Minor anomalies are excluded from the register according to the practices of the European Surveillance of Congenital Anomalies (23).
The data on LT4 purchases three months prior and during the current pregnancy were obtained from the Statistics on Reimbursements for Medical Expenses (Prescription Register and Special Refund Entitlement Register) maintained by the Social Insurance Institution. The register collects information from all pharmacies in Finland on all reimbursed prescription-only medication purchases such as LT4. Medications given in hospitals or over-the-counter drugs are not included in the register. The register data include information related to the medicine: the International Anatomic Therapeutic Chemical classification code (codes H03A01–05 for LT4) and the time and number of purchases. Any LT4 purchases indicated LT4 use in this study. LT4 use was deemed consistent if a mother had purchased LT4 during each trimester of pregnancy with or without pre-pregnancy purchases. For pregnant women, LT4 is the treatment of choice for hypothyroidism in Finland.
Information on maternal chronic diseases was collected from the MBR, the Special Refund Entitlement Register maintained by Social Insurance Institution, and the Hospital Discharge Register. The Special Refund Entitlement Register comprises information on diagnosed chronic diseases with medication and reimbursement of medical expenses. The Hospital Discharge Register includes information on diagnoses at discharge from all hospital wards using the ICD-codes. The register has an accuracy of 83–95% (24). Data linkage between the MBR and the other registers was possible using the unique personal identification numbers assigned to all Finnish citizens and permanent residents. Personnel not involved with this study performed the data linkage and data encryption before statistical analyses.
Identification of women with hypothyroidism and exposure to LT4 during pregnancy in 2004–2013
In this study, women had hypothyroidism if they were listed as having the ICD-10 code E03 (with all digits), ICD-9 or ICD-8 code 244 for hypothyroidism in any of the registers, or if they purchased LT4 three months prior or during the current pregnancy (n = 16,364). Women diagnosed with ICD-10 code O99.2 (endocrine, nutritional, and metabolic diseases complicating pregnancy, childbirth, and puerperium) who had documented LT4 purchases were also deemed hypothyroid. Women with other thyroid diseases (hyperthyroidism, thyroiditis, goiter, iodine deficiency–related disorders, benign and malignant neoplasms of thyroid gland; n = 4544) were identified through the registers and were excluded from the current study.
Pregnancy and perinatal and infant health outcomes
The main pregnancy-related outcome measures obtained from the MBR were: gestational hypertension; mild/moderate or severe preeclampsia (including HELLP [hemolysis, elevated liver enzymes, low platelet count] syndrome) eclampsia; GDM; delivery mode (vaginal, breech, instrumental, or elective CS and acute CS); placenta previa; and placental abruption. The main perinatal outcomes were early (<34 completed gestational weeks) and late (34 + 0–36 + 6 gestational weeks) preterm births, number of small-for-gestational age (birth weight less than two standard deviations from the gestational age adjusted mean), and large-for-gestational age (LGA; birth weight more than two standard deviations from the gestational age adjusted mean) infants, low Apgar score (<7 points at five minutes), major congenital anomalies, admission to NICU, need for respiratory treatment, stillbirth, and early neonatal death.
Ethical issues
The study was approved by the ethical board of Northern Ostrobothnia Hospital District. The National Institute of Health and Welfare gave permission to use data obtained from the national health registers. Data collection was conducted with permission from the register administrators. The study was funded in part by the Northern Ostrobothnia Hospital District.
Statistical analyses
Pregnancy was the unit of analysis for all statistical testing. Demographic data on mothers with hypothyroidism and mothers with hypothyroidism with consistent LT4 purchases were compared to mothers without thyroid disease using the chi-square test or Fisher's exact test. Logistic regression with generalized estimating equations (GEE) and a first-order autoregressive correlation matrix were used to estimate the odds ratios (ORs) with confidence intervals (CIs) of adverse outcomes among women with hypothyroidism compared to mothers without thyroid disease. The GEE accounted for the correlations among the repeated pregnancies of the same mother. All analyses were adjusted for maternal age at delivery, body mass index, parity, smoking status, socioeconomic status (i.e., upper white-collar worker, lower white-collar worker, blue-collar worker, other, and unknown), year of delivery, and maternal residence within the five university hospital districts. As the unadjusted and adjusted odds were similar; only the adjusted odds are presented. Missing data on outcomes were rare and excluded on a case basis. Statistical analyses were performed using SAS v9.3 (SAS Institute, Cary, NC).
Results
Demographic data
Overall, 16,364 (3%) of all pregnancies were complicated by maternal hypothyroidism between 2004 and 2013. Of these women, 95.8% had documented LT4 purchases at some stage of pregnancy, and 37.5% had consistent LT4 purchases during pregnancy. Altogether, 65.9% of mothers with consistent LT4 purchases had also pre-pregnancy purchases. The mothers with hypothyroidism were older, more often multiparous, more likely to be overweight or obese, smoked less, and had had more miscarriages than women without thyroid disorders (Table 1).
Demographic Characteristics of Mothers With Singleton Pregnancies (2004–2013) With and Without Hypothyroidism
The data are reported as number of mothers (%) unless stated otherwise.
Data on mothers with hypothyroidism and mothers with hypothyroidism with consistent levothyroxine purchases were compared to mothers without thyroid disease using the chi-square test or Fisher's exact test. All comparisons were statistically significant, with a p-value of <0.0001.
Pregnancy complications
The odds of gestational hypertension (OR = 1.20 [CI 1.10–1.30]) and severe preeclampsia (OR = 1.38 [CI 1.15–1.65]) were associated with maternal hypothyroidism, but these odds were no longer statistically significant when restricting the data to hypothyroid mothers with consistent LT4 purchases (Fig. 1). Moreover, an association between GDM (OR = 1.19 [CI 1.13–1.25]), placenta previa (OR = 1.44 [CI 1.21–1.72]), elective CS (OR = 1.24 [CI 1.17–1.32]), and acute CS (OR = 1.15 [CI 1.09–1.21]) with maternal hypothyroidism was observed. These associations persisted among mothers with consistent LT4 purchases (Fig. 1). No association was observed between breech presentation, instrumental delivery, or placental abruption and maternal hypothyroidism.
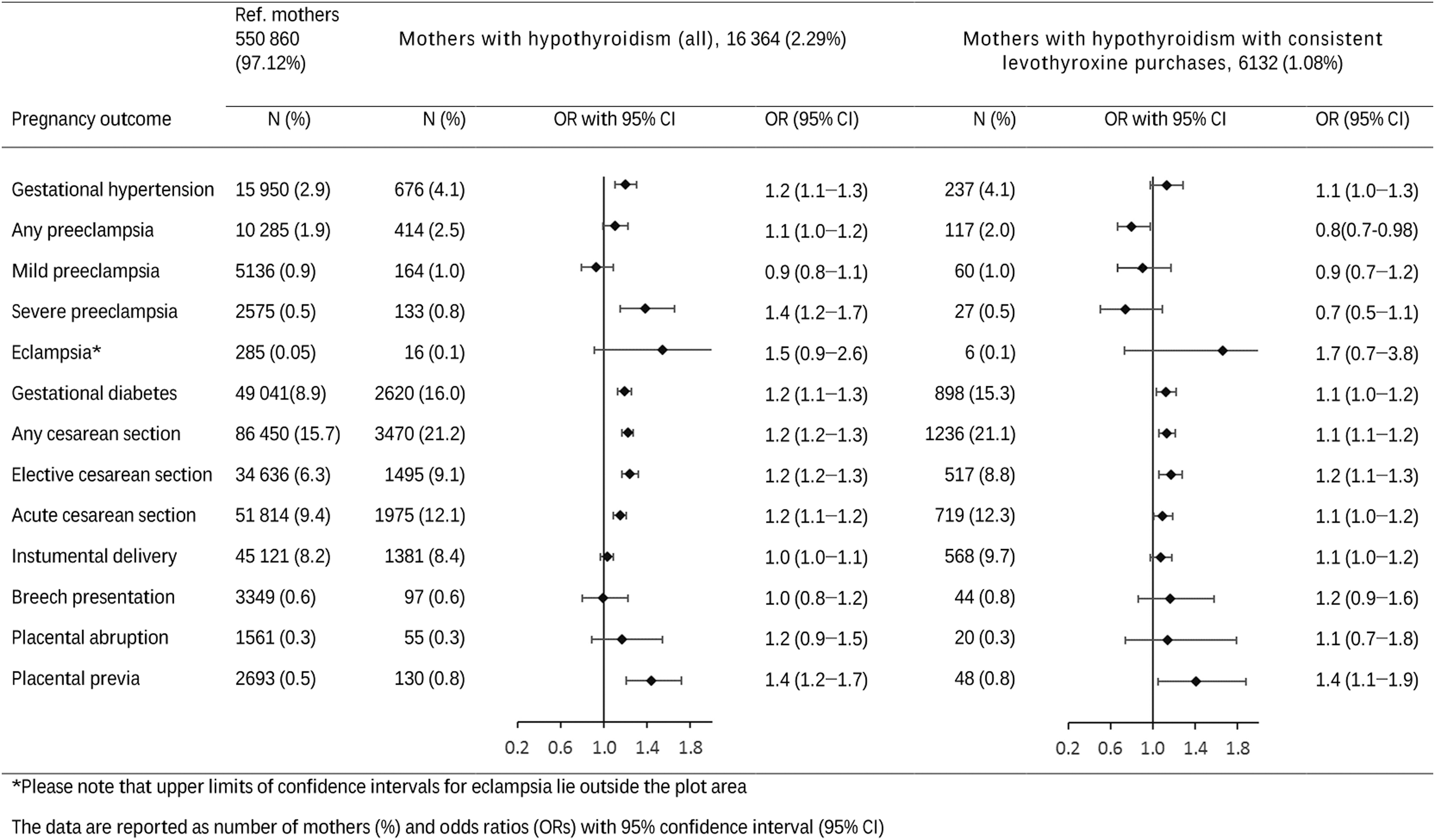
Prevalence and odds of pregnancy complications among singleton pregnancies of mothers with and without hypothyroidism in 2004–2013 in Finland.
Perinatal outcome
Maternal hypothyroidism was associated with both early and late preterm births (OR = 1.35 [CI 1.19–1.53] and OR = 1.20 [CI 1.10–1.31], respectively). Again, these odds were no longer statistically significant when restricting the data to mothers with consistent LT4 purchases (Fig. 2). Moreover, an association was found between NICU admission (OR = 1.23 [CI 1.17–1.29]), need for respiratory treatment (OR = 1.41 [CI 1.24–1.60]), and lower Apgar scores at five minutes (OR = 1.20 [CI 1.09–1.33]) and maternal hypothyroidism, but none with umbilical artery pH. The newborns of hypothyroid mothers were more often LGA than those of mothers without thyroid disease (OR = 1.30 [CI 1.19–1.42]). Slightly increased odds of major congenital anomalies were found among children born to mothers with hypothyroidism (OR = 1.14 [CI 1.06–1.22]). Only the association between NICU admission (OR = 1.09 [CI 1.01–1.18]) and LGA newborns (OR = 1.26 [CI 1.10–1.45]) with maternal hypothyroidism remained among those with consistent LT4 purchases (Fig. 2). The incidence of stillbirths and early neonatal deaths was low and did not differ between groups.
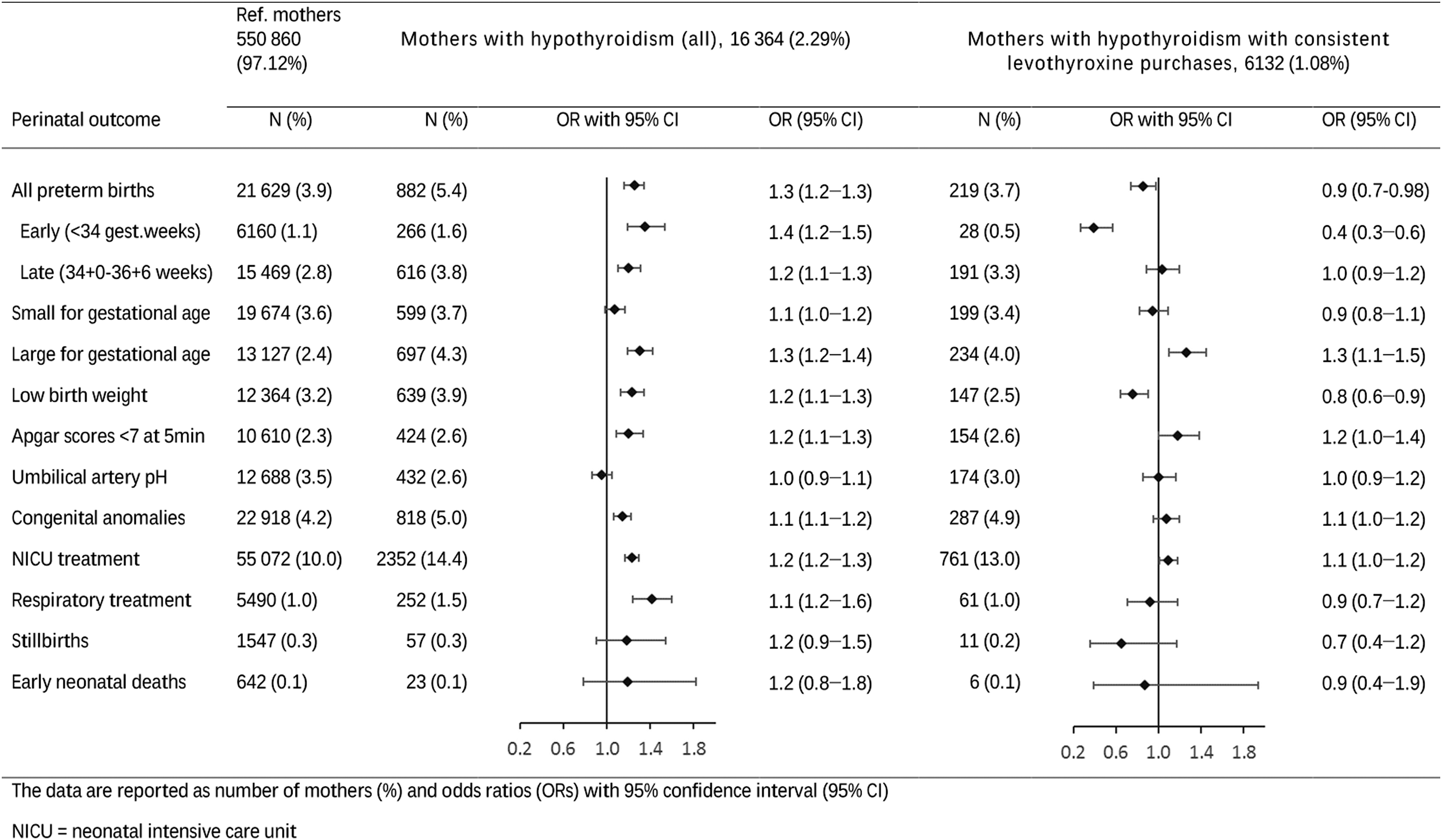
Prevalence and odds of perinatal complications among singleton pregnancies of mothers with and without hypothyroidism in 2004–2013 in Finland. NICU, neonatal intensive care unit.
Additional analysis
The demographic data of mothers with consistent LT4 use was similar to those of mothers who had LT4 treatment started during the second and the third trimester. Including women with type I diabetes into analyses had no major effect on any of the results.
Discussion
This study is the only one to evaluate extensively pregnancy and perinatal complications with LT4 use established through medication purchases. The study shows that up to 3% of women giving birth were on LT4 medication during pregnancy. Maternal hypothyroidism increased the odds of GDM, CS, and LGA, as well as the risk for NICU admission, even if LT4 use was consistent during pregnancy. The odds of gestational hypertension, severe preeclampsia, preterm births, and congenital anomalies seemed to be driven by inconsistent LT4 use, as these increased odds were not observed for mothers with consistent LT4 use.
The observed association between GDM and hypothyroidism was found in some (10,14,15,17) but not all previous studies (25). Adequate thyroid function maintains normal energy and lipid metabolism (26). Therefore, underlying changes in energy metabolism, insulin resistance, and autoimmune diseases or shared risk factors (i.e., obesity, age, and parity) may explain the association between hypothyroidism and GDM. Moreover, women with hypothyroidism are at increased risk of subsequent diabetes, suggesting common risk factors (18). As with some previous studies, an association was also observed between hypothyroidism and LGA (27). The observed association between maternal hypothyroidism and GDM may at least partly explain this finding.
Mothers with hypothyroidism had increased odds of CS, a finding previously found in some (9 –11,17) but not all studies (20). In one previous work, hypothyroidism was an independent risk factor for CS (9), but the reason for increased risk could be due to the associated pregnancy complications, such as hypertension and diabetes. In previous studies, associations between maternal hypothyroidism and gestational hypertension, preeclampsia, and preterm birth have been controversial (2,8,10 –12,15,16,20,28). This study also found these aforementioned associations, but the odds were not statistically significant among mothers with consistent LT4 use, suggesting that adequate treatment throughout pregnancy may diminish the risk for these complications. Differences in the adequacy of treating hypothyroidism in different studies or the lack of controlling for confounders may partly explain these controversial findings.
Newborns of hypothyroid mothers were more likely to need NICU admission or respiratory treatment, which is consistent with previous studies (11,27). The odds of NICU admission and respiratory treatment persisted after restricting data to term births, thus suggesting that prematurity did not fully explain this association. A small but statistically significant association between congenital anomalies and maternal hypothyroidism was found. This finding was previously observed at least in two studies (10,29). The finding persisted after adjusting for covariates and the exclusion of women with type 1 diabetes who are known to have a higher risk of congenital anomalies (30).
Strengths and limitations
The strength of this study is its large sample size with comprehensive nationwide data based on compulsory administrative health registers of high quality. The MBR covers practically all births in Finland. Combining medication data with the MBR data gave a valuable database for research purposes. Data were derived from the population with minimal loss to follow-up of study subjects, and therefore selection bias was not a concern. However, since the data are based on births, they contain only pregnancies that resulted in delivery. Therefore, women with sub- or infertility, possibly associated with thyroid dysfunction, may not have been included. The risk of recall bias was avoided, as the information was based on administrative register data and collected prospectively during routine visits to maternity welfare clinics. Practically all pregnant Finnish women attend this free-of-charge public maternity care with regular visits to a nurse/midwife and a physician near their local residence, and they give birth at public hospitals led by obstetricians. The large data set provided the opportunity to assess rare outcomes with the ability to evaluate and adjust for confounding factors. However, very rare outcomes such as neonatal deaths might require even bigger cohort studies.
The compact study period (10 years) with comprehensive data collection and uniform national recommendations to treat hypothyroidism gave an outstanding database for the study. National evidence-based guidelines, which include information on common pregnancy-related problems and their management, are available for maternity care personnel. Hypothyroid mothers without other pregnancy-related problems are mainly treated at the local maternity care during their pregnancies. Cases of pregnancy complications are sent to specialized maternity policlinics in the delivery hospital.
Laboratory data to confirm the thyroid hormone and thyroid antibody status would have been useful but were not feasible, given the study size. Therefore, it is unknown whether women who were taking LT4 during pregnancy were adequately treated or if they had overt or subclinical hypothyroidism. In fact, in a recent study, many LT4-treated women had early gestational thyrotropin levels above the recommended targets and even overt hypothyroidism (31). In this study, only 39% of hypothyroid women made LT4 purchases in each trimester. These hypothyroid women were most likely adequately treated during pregnancy and therefore had the lowest risk of adverse pregnancy and perinatal outcomes. The study suggests that inconsistent LT4 use is associated with adverse pregnancy and perinatal outcomes, regardless of whether the inconsistent use is due to inadequate treatment of a known thyroid disease or due to treating newly diagnosed hypothyroidism during pregnancy.
Conclusion
Hypothyroidism is common among women of childbearing age, and it is associated with some adverse pregnancy and perinatal outcomes. In this large register- and population-based cohort study, maternal hypothyroidism was associated with several pregnancy and perinatal complications, but among mothers with consistent LT4 use, the odds of some important complications (gestational hypertension, severe preeclampsia, and preterm birth) were no longer statistically significant. However, maternal hypothyroidism was associated with increased odds for GDM, CS, and LGA, as well as the risk for NICU admission, even if LT4 use was consistent during pregnancy.
Footnotes
Acknowledgments
We thank Aini Bloigu (University of Oulu, Finland) for her technical support with the figures, and Elisa Huovinen (National Institute of Health and Welfare) for statistical assistance. This work was supported in part by the Northern Ostrobothnia Hospital District (S.T.) and the Drugs and Pregnancy project by the THL (National Institute for Health and Welfare), FIMEA (Finnish Medicines Agency), and KELA (Social Insurance Institution of Finland; M.G. and A.-M.L.-K.).
Author Disclosure Statement
No competing financial interests exist.