
Abstract
Background:
Thyroid function assessment in pregnancy requires specific reference intervals stratified by gestational age and according to each laboratory method. Thyroid nodules may influence thyroid function in pregnant women. The aims of this study were to define the reference values of thyrotropin (TSH) and free thyroxine (fT4) in the three pregnancy trimesters in iodine-sufficient pregnant women, and to analyze the influence of thyroid nodules on thyroid function during pregnancy.
Methods:
This was a prospective, longitudinal study comprising 400 pregnant women with no history of thyroid disease and no medication influencing thyroid function. TSH, fT4, antithyroglobulin, and antithyroid peroxidase antibodies were measured each trimester by chemiluminescent immunoassays. Urinary iodine concentration was measured in the first trimester when a thyroid echography was also performed. Women with multiple gestation pregnancies, positive thyroid autoimmunity, TSH values >5 or <0.1 mIU/L with a simultaneous fT4 level above the general population reference value in the first trimester, or clinically significant thyroid nodules (nodules ≥1 cm and/or multiple nodules) were excluded to establish TSH and fT4 reference values.
Results:
Reference intervals in the first, second, and third trimesters were 0.13–4.16, 0.31–3.73, and 0.58–4.36 mIU/L, respectively, for TSH, and 0.85–1.24, 0.82–1.20, and 0.67–1.06 ng/dL, respectively, for fT4. The total prevalence of thyroid nodules was 28.8% [95% confidence interval (CI) 24.4–33.5%], and 6.0% of the participants showed clinically significant nodules. Pregnant women with thyroid nodules (n = 115) showed consistently lower TSH values during all pregnancy stages (first trimester: median 1.14 mIU/L [interquartile range (IQR) 0.53–1.75 mIU/L] vs. 1.48 mIU/L [IQR 0.94–2.19 mIU/L], p < 0.001; second trimester: 1.22 mIU/L [IQR 0.66–1.77 mIU/L] vs. 1.45 mIU/L [1.04–2.05 mIU/L], p = 0.001; third trimester: 1.74 mIU/L [IQR 1.08–2.36 mIU/L] vs. 1.93 mIU/L [IQR 1.37–2.58 mIU/L], p = 0.041) and higher fT4 values in the first trimester (M ± SD = 1.08 ± 0.14 ng/dL vs. 1.03 ± 0.12, p < 0.001) compared to those without nodules (n = 285). Both pregnant women with clinically significant thyroid nodules and those with nonsignificant ones had lower TSH values than women without nodules.
Conclusions:
TSH/fT4 reference intervals in pregnant women from the authors' geographical area will thyroid dysfunction in pregnancy to be appropriately diagnosed. The prevalence of thyroid nodules is high in iodine-sufficient pregnant women, and is associated with low TSH values across pregnancy.
Introduction
During the first half of pregnancy, maternal thyroid hormones play a key role in the development of the placenta and the fetus. Thyroid dysfunction occurs frequently in pregnancy, and is associated with maternal or fetal complications, including miscarriage, preterm birth, preeclampsia, and reduction of the child's IQ (1).
The assessment of thyroid function requires specific reference intervals stratified by trimesters during pregnancy, since pregnancy is associated with physiological changes in thyroid hormone production and metabolism. Reference intervals vary among studies. Differences are due to gestational age, iodine status, ethnic issues, and the analytical methods used (2,3). Body mass index (BMI) and smoking status may also influence thyroid function (4,5). For this reason, international guidelines recommend establishing local ranges for thyrotropin (TSH) and free thyroxine (fT4) during pregnancy, which should be established by recruiting healthy pregnant women with no known thyroid disease with an adequate iodine status and absent thyroid autoimmunity (1,6,7). Antithyroid peroxidase antibodies (TPO) and antithyroglobulin antibodies have been associated with higher TSH values in pregnancy (2).
Few studies including thyroid echography to select a reference population (RP) of pregnant women to establish reference intervals for thyroid function are available. If echography is performed, usually included variables are the presence/absence of goiter and/or changes in echogenicity (8,9). The prevalence of thyroid nodules detected by echography in pregnant women may reach 30% (10). Despite this, the influence of nodules on thyroid function in pregnancy has received little attention, and most studies are restricted to the iodine-deficient population (10,11). The presence of thyroid nodules may modify the physiological changes in thyroid hormone production associated with pregnancy. On the other hand, the high human chorionic gonadotropin (hCG) levels present in early pregnancy activate non-affected normal thyroid tissue and increase thyroid secretion (1). The nutritional iodine status also plays a relevant role, since women with adequate iodine intake before and during pregnancy usually have no difficulty in adapting to the increased demand for thyroid hormones during gestation. Since iodine-sufficient pregnant women may also have thyroid nodules, assessing the influence of nodular alterations on thyroid function during pregnancy may be of interest. Against this background, the first aim of this study was to define the reference values of TSH and fT4 in healthy pregnant women from the authors' geographical area in the three trimesters of pregnancy. The second aim was to analyze the influence of thyroid nodules detected by echography on TSH and fT4 values throughout pregnancy in an iodine-sufficient population.
Methods
Population
This was a prospective, longitudinal study comprising 400 first-trimester pregnant women with no personal history of thyroid disease and not receiving treatment with drugs able to influence thyroid function (i.e., amiodarone, lithium, levothyroxine, or antithyroid treatment). Participants were recruited in two Women's Care Centers in the Pamplona area (Navarra, Spain) when they attended for their first prenatal care visit.
Pregnant women were evaluated in person by trained personnel of the Endocrinology Service of the Hospital Complex of Navarra (CHN) between May 2014 and May 2016. History, cervical examination, thyroid echography, and collection of a simple urine sample to assess urinary iodine concentration (UIC) were performed at the same visit.
The medical history included personal history, pharmacological treatments, smoking status (nonsmoker, ex-smoker, or smoker), intake of iodine supplements, and first-degree family history of thyroid disease. Participants who had given up smoking at least six months before were considered ex-smokers. The height (in meters) and body weight (in kilograms) used to calculate the BMI were recorded at the first prenatal care visit. Following the routine procedures at the authors' institution, all pregnant women were taking supplements containing potassium iodide.
Blood collection for the measurement of TSH, fT4, and anti-TPO and antithyroglobulin antibodies was performed at the routine prenatal care visits (weeks 9, 15, and 36 for the first-, second-, and third-trimester assessments, respectively).
Women with multiple gestation pregnancies, positive thyroid autoimmunity, or relevant abnormalities detected by echography were excluded to establish TSH and fT4 reference values (i.e., median, interquartile range, and ranges [p2.5–p97.5]) in each trimester. For clinical reasons, those women with TSH values >5 mIU/L or <0.1 mIU/L with a simultaneous fT4 level above the general population reference value in the first trimester were also excluded from the RP, since these women were considered to suffer from undiagnosed thyroid disease.
When thyroid dysfunction and/or thyroid nodules were detected, the appropriate treatment and follow-up procedures were initiated according to the usual clinical practice of the authors' institution.
The study was approved by the regional Ethical Review Board of Navarra (reference number 57/2013), and all participants signed an informed consent form.
Thyroid echography and analytical measurements
Thyroid echography was performed with the patient in the supine position, using a 13 MHz linear probe (Sonosite MicroMaxx®; SonoSite, Inc., Bothell, WA). The volume of each thyroid lobe was calculated according to the following formula: longitudinal axis (cm) × transverse axis (cm) × anteroposterior axis (cm) × 0.479. The resulting values were added together to obtain the thyroid volume (mL). Thyroid nodules were evaluated according to the criteria followed in the authors' clinical practice, which are based on the American Thyroid Association (ATA) management guidelines for patients with thyroid nodules and differentiated thyroid cancer (12,13). Women with relevant ultrasound abnormalities (i.e., clinically significant thyroid nodules and/or goiter) were excluded from the RP. Thyroid nodules ≥1 cm were considered clinically significant, since generally only these lesions should be evaluated (12,13). Multiple thyroid nodules (more than four nodules) irrespective of size were also a criterion for clinically significant nodules. Goiter was considered when thyroid volume was >18 mL.
Blood measurements of TSH, fT4, and anti-TPO and antithyroglobulin antibodies were consecutively performed in the Central Laboratory of the CHN (Pamplona) using chemiluminescence-based tests on an Architect i2000 automatic analyzer (Abbott Laboratories, Abbott Park, IL). TSH and fT4 reference intervals in the authors' laboratory are 0.35–4.94 μIU/mL [99% confidence interval (CI)] and 0.70–1.48 ng/dL (99% central interval), respectively. Reference values for anti-TPO and antithyroglobulin antibodies are <5.61 and <4.11 IU/mL, respectively, according to the manufacturer. Values above the upper limit of the reference range were considered positive.
The assessment of UIC in a simple urine sample was performed at the Public Health Normative Laboratory of the Basque Government (Derio, Bizkaia, Spain) using an ion-pair reversed-phase high-performance liquid chromatography–based method with electrochemical detection and silver electrode (Waters Chromatography, Milford, MA). Detailed information regarding validation of the procedure and intra- and inter-series precision has previously been made available (14). Until shipment to the reference laboratory, samples were properly labeled and stored frozen at −20°C. World Health Organization (WHO) 2007 criteria were followed to assess iodine status: median UIC values of <150, 150–249, 250–499, and ≥500 μg/L were considered indicators of iodine insufficiency, adequate iodine status, more than adequate iodine status, and iodine excess, respectively (15).
Statistical analysis
Categorical variables are summarized using frequencies and percentages for each category. Continuous variables are described as the median (interquartile range [IQR]) or the mean ± standard deviation (SD), according to nonparametric or parametric distribution, respectively. The reference ranges in the healthy population (i.e., participants who did not fulfil any of the exclusion criteria detailed above) were estimated by the 2.5th and 97.5th percentile of the empirical distribution. Correlations between categorical variables or continuous nonparametric variables were analyzed by Spearman's test, while Pearson's test was used for parametric data. Prevalence rates of positive thyroid autoimmunity and thyroid nodules are described by the sample proportions together with their corresponding CI. The Kolmogorov–Smirnov test was used to determine whether variables were normally distributed. TSH and fT4 values obtained throughout the pregnancy period were compared using the Friedman test followed by Wilcoxon's test for two-by-two comparisons, or the analysis of variance test for dependent variables followed by Student's t-test for paired samples, according to nonparametric or parametric distribution, respectively. TSH and fT4 values according to positivity versus negativity in the thyroid autoimmunity tests were compared using the Mann–Whitney test or Student's t-test for independent variables when data distribution was nonparametric or parametric, respectively. The same procedures were used to compare TSH and fT4 values according to presence versus absence of thyroid nodules detected by echography. Associations between categorical variables were evaluated by the chi-square test. Additionally, multivariate linear regression analyses were performed using log-transformed TSH values to gain insight into the association between TSH and the other variables. The variables explored were age (in years), parity (nulliparity/multiparity), UIC (μg/L), smoking status (yes/no), BMI (<30/≥30 kg/m2), thyroid volume (mL), and presence/absence of thyroid nodules. Those whose association with TSH values was significant at α = 0.05 level in the univariate analyses were maintained in the model (age, parity, BMI, thyroid volume, and presence/absence of thyroid nodules). Analyses were performed using IBM SPSS Statistics for Windows v20 (IBM Corp., Armonk, NY). p-Values <0.05 were considered to be statistically significant.
Results
Study population
A total of 400 pregnant women aged 33.4 ± 4.0 years, most of whom were Caucasian, were studied. The in-person visit took place at week 10.8 ± 2.2 (M ± SD) of the pregnancy period. Most (98.5%) participants were taking iodine supplements at this time (M ± SD iodine dose: 202.6 ± 30.1 μg per day), and 42.5% had started taking such supplements at least one month prior to pregnancy.
There were 14 women with multiple gestations. Positive thyroid autoimmunity was detected in 75/400 (18.8%) participants, and clinically significant thyroid nodules were observed by echography in 24 (6%) women. Two participants showed TSH values >5 mIU/L in the first trimester. No cases of clinical hyperthyroidism were seen in this period. Six women fulfilled at least two of the exclusion criteria. There were four women with goiter on echography (thyroid volume >18 mL), all of whom also had clinically significant thyroid nodules. All of these participants (n = 109) were excluded from the calculations of the reference values of thyroid function, which were finally performed on a population of 291 healthy pregnant women (Fig. 1).
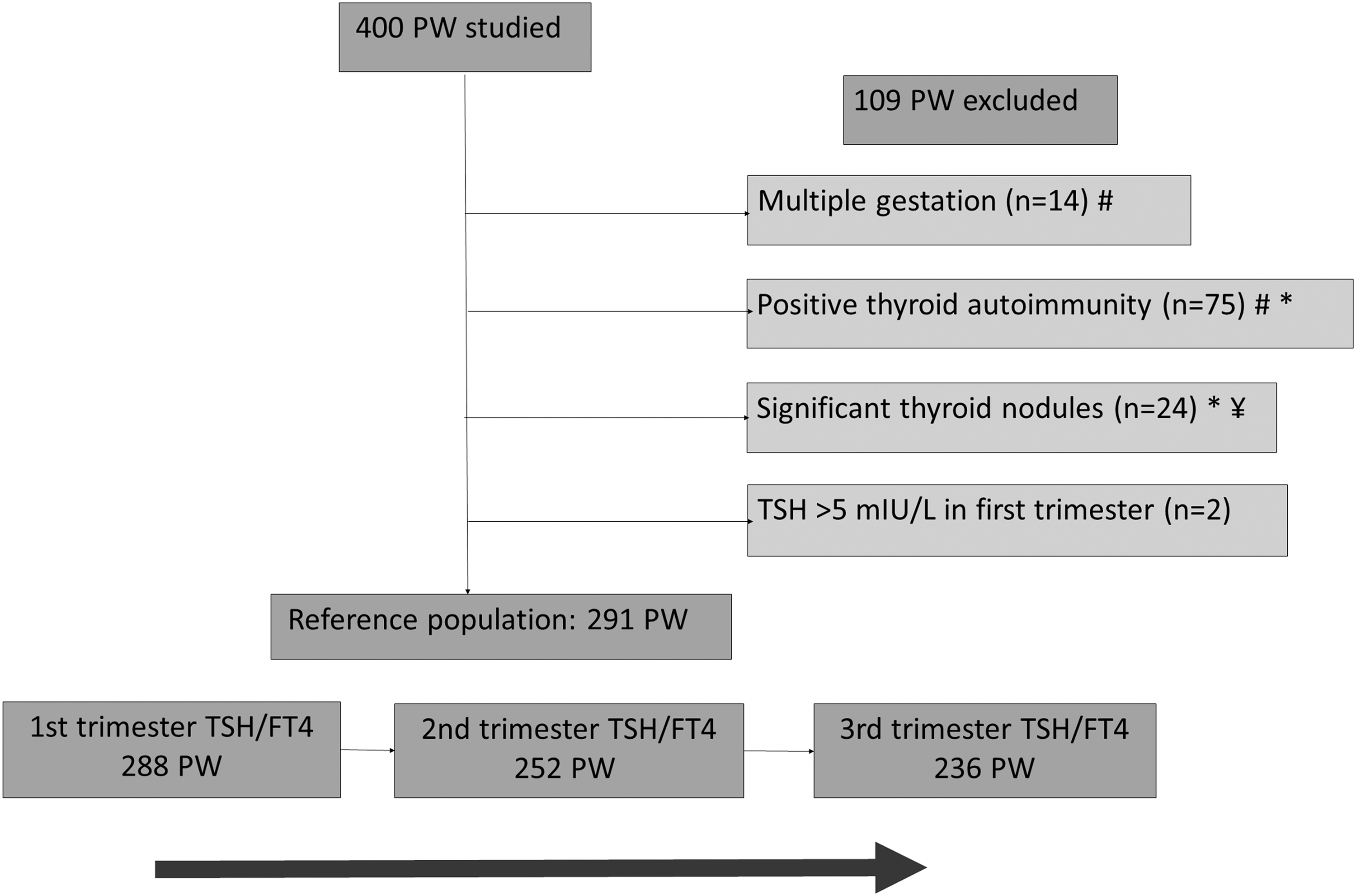
Flow chart of the study, showing the steps to select the reference population. A total of 400 pregnant women with no personal history of thyroid disease and without treatment with drugs influencing thyroid function were studied. Criteria to exclude participants from the population used to calculate TSH and fT4 reference values and the number of women fulfilling such criteria are specified. The number of participants in the reference population whose blood samples were available in the first, second, and third trimesters to establish TSH and fT4 reference ranges are also indicated. #Simultaneous multiple gestation and positive thyroid autoimmunity (n = 2). *Simultaneous clinically significant thyroid nodules as assessed by echography and positive thyroid autoimmunity (n = 4). ¥Women with goiter on echography (n = 4) and clinically significant nodules. TSH, thyrotropin; fT4, free thyroxine; PW, pregnant women.
The median UIC at week 10 of pregnancy was 242.0 μg/L (IQR 138.5–415.5 μg/L) in the entire population. These data fulfil the WHO criteria for an iodine-sufficient population. UIC values were <150 μg/L or ≥500 μg/L in 26.3% (n = 105) and 16.3% (n = 65) of participants, respectively. In the RP (i.e., women in the initial cohort whose TSH and fT4 values were used to establish the reference ranges; n = 291), the results were rather similar: the median UIC value was 232.0 μg/L (IQR 130.5–396.5 μg/L), and 28.5% (n = 83) showed levels <150 μg/L, and 15.1% (n = 44) showed levels ≥500 μg/L.
The overall prevalence rate of positive thyroid autoimmunity was 18.8% [CI 15.1–23.0%]. Among the 75 pregnant women with autoantibodies, 13 (17.3%) showed anti-TPO antibodies, 30 (40.0%) antithyroglobulin antibodies, and the remainder (n = 32; 42.7%) showed both types of autoantibodies.
Baseline characteristics of the overall population and RP are shown in Table 1.
Baseline Characteristics of the Overall and Reference Populations
The reference population consisted of all participants in the initial cohort with no multiple gestation pregnancies, negative thyroid autoimmunity, neither TSH >5 mIU/L nor TSH <0.1 mIU/L with simultaneous fT4 level above the general population reference value in the first trimester, and without clinically significant thyroid nodules detected by echography. Continuous variables are expressed as mean ± standard deviation or as median (interquartile range). UIC and thyroid volume correspond to week 10 (range 6–18) of the pregnancy.
BMI, body mass index; UIC, urinary iodine concentration; TSH, thyrotropin; fT4, free thyroxine.
Reference values of thyroid function
The trimester-specific TSH and fT4 values in the RP are displayed in Table 2. As Figure 2 shows, TSH levels increased across the pregnancy period and were significantly higher in the second and third trimesters compared to the first trimester. On the other hand, fT4 levels decreased significantly and continuously across the pregnancy period.
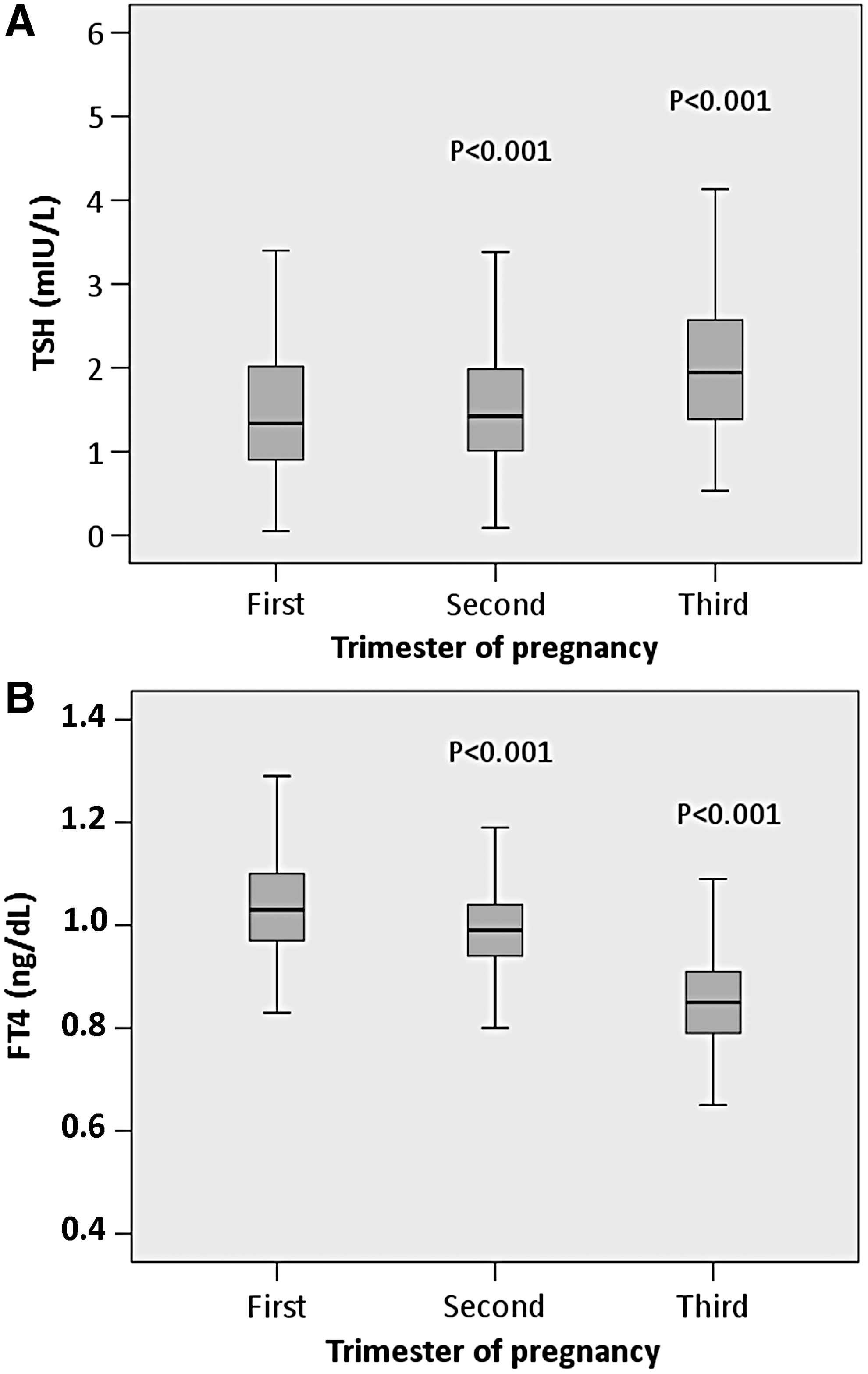
Circulating levels of thyroid hormones in the reference population across pregnancy. The evolution of TSH (
TSH and fT4 Values in the Reference Population
The reference estimators (median [IQR] or mean ± SD according to nonparametric or parametric distribution, respectively) and reference ranges (p2.5–p97.5) of circulating levels of TSH and fT4 in the reference population are shown. The median (IQR) gestational weeks at which samples were withdrawn were 9 (8–9), 15 (14–15), and 36 (36–37) for the first, second, and third trimesters, respectively. Reference ranges for the general population at the authors' laboratory are 0.35–4.94 mIU/L for TSH and 0.70–1.48 ng/dL for fT4.
IQR, interquartile range; SD, standard deviation; p2.5–p97.5, 2.5th and 97.5th percentiles.
TSH values were significantly and highly correlated among trimesters, and so were fT4 levels (not shown). TSH was significantly and inversely correlated with fT4 in the first and third trimesters (first trimester: Spearman's ρ = −0.249, p < 0.001; second trimester: Spearman's ρ = −0.078, p = 0.216; third trimester: Spearman's ρ = −0.132, p = 0.043) and with thyroid volume in the first (Spearman's ρ = −0.259, p < 0.001), second (Spearman's ρ = −0.319, p < 0.001), and third (Spearman's ρ = −0.247, p < 0.001) trimesters. On the other hand, a significant and direct correlation was found between fT4 levels and thyroid volume in the first (Pearson's r = 0.175, p = 0.003) and second (Pearson's r = 0.129, p = 0.042) trimesters.
Factors influencing thyroid function during pregnancy
In the first trimester, pregnant women with positive thyroid autoimmunity had TSH values that were significantly higher than those with negative thyroid antibodies (1.81 mIU/L [0.81–2.31 mIU/L] vs. 1.29 mIU/L [0.86–1.98 mIU/L], p = 0.010). However, no differences were observed in fT4 levels in the same period (1.03 ± 0.12 ng/dL vs. 1.05 ± 0.12 ng/dL, p = 0.157). No differences in thyroid function were found between women with isolated antithyroglobulin antibodies compared to those with anti-TPO positivity. Both women with antithyroglobulin positivity and with anti-TPO antibodies had significantly higher TSH levels in the first trimester (1.79 mIU/L [0.80–2.31 mIU/L], p = 0.028, and 1.84 mIU/L [0.80–2.67 mIU/L], p = 0.011, respectively) than those with negative autoimmunity (1.29 mIU/L [0.86–1.98 mIU/L]).
There were no differences in thyroid function (i.e., TSH or fT4 levels) across the study period between participants with an adequate median UIC (i.e., 150–249 μg/L) and participants with a median UIC of either <150 μg/L or ≥500 μg/L (not shown). Furthermore, no correlation was observed between UIC and thyroid volume (Spearman's ρ = 0.024, p = 0.691).
Pregnant women with a BMI of ≥30 kg/m2 showed TSH levels that were significantly higher than those of participants with normal weight in the first trimester (1.78 mIU/L [1.11–2.21 mIU/L] vs. 1.29 mIU/L [0.89–1.89 mIU/L], p = 0.031). There were no significant differences in fT4 levels (1.03 ± 0.10 vs. 1.04 ± 0.09 ng/dL, p = 0.796) or in thyroid volume (8.5 ± 2.5 vs. 7.7 ± 2.7 mL, p = 0.127) between these groups during the same pregnancy period. Comparisons were made between all BMI categories, but differences in TSH were significant between obese and normal BMI women only.
When compared to nonsmoker participants, smokers showed significantly lower fT4 values (1.02 ± 0.11 vs. 1.05 ± 0.09 ng/dL, p = 0.031) and higher thyroid volume (8.4 ± 2.9 vs. 7.6 ± 2.6 mL, p = 0.026) in the first trimester. Differences in TSH levels were not seen between both groups during the same pregnancy trimester (1.45 mIU/L [0.92–2.32 mIU/L] vs. 1.33 mIU/L [0.90–1.96 mIU/L], p = 0.379).
Thyroid nodules assessed by echography
Echography allowed the detection of thyroid nodules in a total of 115 participants. The overall prevalence was 28.8% [CI 24.4–33.5%]. Table 3 depicts a summary of the main features of pregnant women according to the presence/absence of thyroid nodules. When compared to participants without thyroid nodules (n = 285), those with nodules (n = 115) were significantly older, showed significantly higher thyroid volume, and had significantly lower TSH values repeatedly across the pregnancy period. fT4 levels were significantly higher in the group of participants with nodules only in the first trimester.
Mean Features of Pregnant Women Stratified According to the Presence/Absence of Thyroid Nodules Detected by Echography
Unless specified, variables are represented as M ± SD or median (IQR) according to parametric or nonparametric distribution, respectively. Continuous variables were compared using the Student's t-test or Mann–Whitney U-test according to parametric or nonparametric distribution, respectively. Categorical variables were compared using the chi-square test.
Of the 115 pregnant women with thyroid nodules, 24 (i.e., 6% of the overall population) had clinically significant nodules. The size of at least one nodule was ≥1 cm in 22 of them. The other two had multiple thyroid nodules (one woman had five nodules and a thyroid volume of 39.8 mL, and the other one had multiple cystic nodules). Women with clinically significant nodules showed a significantly higher thyroid volume (12.4 ± 8.2 vs. 7.5 ± 2.5 mL, p = 0.032) and consistently lower TSH values throughout pregnancy (first trimester: 0.74 mIU/L [0.16–1.57 mIU/L] vs. 1.48 mIU/L [0.94–2.19 mIU/L], p = 0.011; second trimester: 0.64 mIU/L [0.13–1.30 mIU/L] vs. 1.45 mIU/L [1.04–2.05 mIU/L], p < 0.002; third trimester: 0.92 mIU/L [0.19–1.74 mIU/L] vs. 1.93 mIU/L [1.37–2.58 mIU/L], p < 0.001) compared to women without nodules. When compared to the RP women, the results were rather similar: women with clinically significant thyroid nodules had higher thyroid volumes and lower TSH values in the three trimesters of pregnancy. Furthermore, in the first trimester, TSH levels were <0.13 mIU/L (i.e., lower than the p2.5 of the RP) in 25% of participants.
On the other hand, nonsignificant thyroid nodules were detected in 91 participants. These women had between one and four nodules (76.9% had ≤2 nodules), all of them <1 cm. When the pregnant women with nonsignificant thyroid nodules were compared to those without nodules, the former were significantly older (34.2 ± 3.7 vs. 33.0 ± 4.1 years, p = 0.015) and showed a higher thyroid volume (9.3 ± 2.8 vs. 7.5 ± 2.5 mL, p < 0.001) and lower TSH values in the first and second trimesters (first trimester: 1.19 [0.61–1.75] vs. 1.48 [0.94–2.19 mIU/], p = 0.002; second trimester: 1.28 mIU/L [0.84–1.83 mIU/L] vs. 1.46 mIU/L [1.04–2.05 mIU/L], p = 0.020). In the first trimester, TSH levels were below the 2.5th percentile of the RP in three participants.
Women with clinically significant nodules had consistently lower TSH levels compared to women with nonsignificant nodules, and the differences were statistically significant in the second and third trimesters.
It is important to note that among the 16 participants who had TSH values below the 2.5th percentile of the RP in the first trimester, nine (56.3%) had thyroid nodules. Furthermore, nodules were clinically significant in six cases.
Independent association between TSH and other variables
The multivariate models allowed significant and independent associations to be found between TSH and some of the variables. On the one hand, TSH levels were higher in patients with a BMI ≥30 kg/m2 than in those whose BMI was <30 kg/m2 in the first trimester (β = 0.31 [CI 0.02–0.61]; p = 0.039). On the other hand, TSH was lower in patients with thyroid nodules than in those without them (β = −0.21 [CI −0.41 to 0.01]; p = 0.043). Finally, TSH was inversely related to thyroid volume (β = −0.09 [CI −0.12 to −0.07]; p < 0.001).
Discussion
In this longitudinal study, the reference values of TSH and fT4 in the three pregnancy trimesters have been established for a northern Spanish population of healthy pregnant women. Furthermore, the study demonstrates that thyroid nodules are common among iodine-sufficient pregnant women, with a prevalence rate close to 30%, and that they are associated with low TSH values during pregnancy.
The reference ranges for thyroid function found in this study, which are consistent with those obtained in most studies performed in Spain or elsewhere, confirm that there is a decrease in circulating TSH levels in those who are pregnant compared to those who are not pregnant (16 –21). The 97.5th percentile TSH level calculated in the RP in the first trimester, (i.e., 4.16 mIU/L) is similar to that proposed by the latest guidelines of the ATA (i.e., 4 mIU/L) (1). In agreement with previous studies, the data show significant differences in TSH and fT4 values across pregnancy, with the first one continuously increasing, and the second one continuously decreasing, from the first to the third trimester. There are some facts that should be borne in mind to examine the analytical findings in pregnant women. It is well known that gestational age influences TSH and fT4 reference values (22 –25). It is also accepted that TSH reference values corresponding to the general population are valid for pregnant women until the sixth or seventh week of pregnancy. The lowest TSH value was observed at the end of the first trimester, between weeks 9 and 12, concurrently with the highest peak in hCG (4,16,17,25). Therefore, the assessment of the reference ranges of TSH and fT4 in the pregnancy weeks corresponding to the routine analytical controls of pregnancy performed at the authors' institution should allow pregnant women to be properly stratified as healthy or as having thyroid dysfunction. fT4 levels were determined instead of total T4 or fT4 index, which may be more accurate during pregnancy (1), since fT4 is the determination procedure used at the authors' hospital.
The prevalence rate of thyroid autoimmunity in the pregnant population in this study was 18.8%. As documented by previous literature, antithyroid antibodies were associated with higher TSH values in the first trimester (16,23). This consistent finding supports that pregnant women with antithyroid antibodies should be excluded to establish reference values, a recommendation that is in agreement with the main clinical guidelines (1,6,7). It must be noted that since 40% of the pregnant women with positive thyroid autoimmunity in this study had isolated antithyroglobulin antibodies, which is a fairly high rate, the exclusive assessment of anti-TPO antibodies would substantially underestimate the prevalence of thyroid autoimmunity, at least in this population. In a recent study, the exclusion of the antithyroglobulin positive women, after having previously excluded women positive for anti-TPO antibodies, did not influence the reference ranges of thyroid hormones (26). However, it is noticeable that in the population used in this study, women with antithyroglobulin antibodies had similar TSH levels compared to those with anti-TPO antibodies, as well as TSH levels that were higher than those in women with negative autoimmunity. Other studies have also shown higher TSH values and a higher prevalence of thyroid dysfunction in women with antithyroglobulin antibodies compared to those with negative antibodies (27,28).
The median UIC found in the overall population in this study reflects an adequate iodine status according to the WHO classification. The systematic intake of iodine supplements by the participants in this study may explain this result. Whether either abnormally low or high UIC are associated with higher TSH values during pregnancy is a matter of controversy. Shi et al. found that pregnant women with UIC >500 μg/L had TSH levels higher than those whose UIC was within the appropriate range (29). However, the results are in agreement with others in that there were no differences in maternal TSH and/or fT4 according to iodine status (30,31). The participants in this study with UIC either <150 μg/L or ≥500 μg/L showed similar TSH and fT4 levels to those of pregnant women with adequate UIC. Nevertheless, the findings might be explained by the fact that UIC was assessed only once. This practice may not be sufficient to categorize pregnant women properly into iodine sufficient or iodine deficient: on the one hand, the analytical method shows large intra-individual variability; on the other hand, levels are influenced by recent iodine intake, either in the diet or via iodine-containing supplements (32).
The results concerning other factors influencing thyroid function in the pregnant population—namely obesity and smoking—are in agreement with the previous literature (4,25,30,33). Pregnant women with a BMI ≥30 kg/m2 showed first-trimester TSH values that were higher than those for normal-weight participants. On the other hand, although there were no differences in TSH levels between pregnant smokers and nonsmokers, the former group had higher thyroid volumes and showed lower fT4 levels in the first trimester than the latter.
Studies including thyroid echography to select a RP to establish reference values of thyroid function in pregnant women are scarce. In one of them, 541 Indian pregnant women underwent echography, and those with findings suggestive of thyroiditis (hypogenicity) and/or thyroid nodules were excluded from the calculations (8). The study showed an association between hypogenicity and higher TSH values. Another study, carried out with 466 Iranian pregnant women, used thyroid echography to establish the fT4 index (9). For this purpose, the authors excluded pregnant women showing alterations in echogenicity and/or goiter. However, nodular disease was not listed among the exclusion criteria.
This study did exclude pregnant women with clinically significant nodules from the RP, mainly thyroid nodules ≥1 cm. The authors are aware that the criteria to define “clinically significant” thyroid nodules are arbitrary to some extent. The cutoff was based on the ATA clinical guidelines recommendation to evaluate, generally, only nodules >1 cm, since they have a greater potential to be clinically significant thyroid cancers and also because they could potentially alter thyroid function (12,13). The detection of multiple thyroid nodules irrespective of size was also categorized as clinically significant. It is thought that a multinodular thyroid precludes considering these women as healthy. Therefore, they should also be excluded from the RP. The fact that women with clinically significant nodules had consistently lower TSH values across pregnancy (i.e., in all three trimesters) lends further support to the approach to exclude them from the calculations to establish the reference ranges of thyroid function.
In the literature, the prevalence rates of thyroid nodules in iodine-deficient pregnant women range between 14.6% and 33.2% (30,34), and have been associated with older ages and higher parity (10,11,34,35). The prevalence rates of thyroid nodules in non-pregnant women reported by other authors seem to be rather similar (34,36). Upon examination with echography, thyroid nodules were detected in roughly 30% of the overall population. Recent studies showed similar prevalence rates, despite differences in iodine status between various populations, which were iodine deficient, and the present study population (10,34). An association was also found between thyroid nodules and higher age. However, no association with parity was observed in the present population.
In this study, women with thyroid nodules had lower TSH values throughout pregnancy and higher fT4 levels in the first trimester than those without nodules. Previous studies addressing this issue found controversial results. One of them documented similar fT4 but significantly lower TSH levels in women with thyroid nodules compared to those without nodules in a cohort of 221 Chinese pregnant women (11). However, Sahin et al. were unable to find significant differences in first-trimester TSH levels among pregnant women according to the presence or absence of thyroid nodules (10). Nevertheless, iodine status constitutes a major difference between these two studies and ours: while mild and severe iodine-deficient pregnant women were recruited for the Chinese and Turkish cohorts, respectively, the present cohort consisted of pregnant women belonging to an iodine-sufficient population. A better iodine status favoring autonomous function in pre-existing nodules is a scenario that should not be ruled out, since hormone production in autonomous thyroid nodules depends on the available amount of iodine (1). It should also be considered that TSH values in women with thyroid nodules could have been decreased before pregnancy.
The current study highlights that small thyroid nodules, which are usually considered nonsignificant (13), may influence TSH levels during pregnancy. In the current study population, pregnant women with such nodules also showed TSH levels that were significantly lower than those of pregnant women in whom an echography had discarded the presence of nodules. However, it has to be noted that most women with nonsignificant nodules had TSH values within the normal reference range. Previous studies considered overall thyroid nodules, that is, they did not analyze associations with TSH or fT4 levels according to the number and/or size of nodules. The present finding is somehow unexpected and might be explained by the independent association found between low TSH and high thyroid volume: decreased TSH values in women with nonsignificant nodules could have been caused by the effect of hCG on a larger amount of thyroid tissue. In any case, more studies in iodine-sufficient populations of pregnant women are warranted to confirm thse findings further.
In summary, this is the first time that the association between TSH/fT4 levels and thyroid nodules has been addressed in a cohort of iodine-sufficient pregnant women. Reference values and ranges of TSH and fT4 have been established in this population. This information will allow pregnant women attending the authors' hospital to be properly categorized into dysfunctional or healthy according to thyroid function. Remarkably, thyroid nodules are frequently found in iodine-sufficient pregnant women and are associated with low TSH values across pregnancy.
Footnotes
Acknowledgments
We want to thank the pregnant women included in the study, and the midwives and obstetricians of the Women's Care Centers of Andraize and Buxtintxuri for their active involvement in the recruitment phase of this study. Thanks to the Navarra Biomed Foundation, especially to Berta Ibáñez, for the methodological advice provided. We also thank Ramón Montes for his critical revision of the final version of this manuscript. This work was supported in part by the Fundación de Endocrinología, Nutrición y Diabetes de Navarra.
Author Disclosure Statement
No competing financial interests exist.