
Abstract
Background:
Elevated postoperative serum calcitonin (Ctn) level indicates persistent/recurrent disease in patients with medullary thyroid carcinoma (MTC). Its location is a challenge. The aim of our study was to compare the disease detection rates of F-18-Dopa (fluoro dihydroxyphenylalanine) positron emission tomography (PET)/computed tomography (CT), whole-body (WB) magnetic resonance imaging (MRI), F-18-FDG (fluorodeoxyglucose) PET/CT, WB CT scanning, neck ultrasonography, and bone scintigraphy in MTC patients with increased Ctn levels and unknown localization of the source.
Methods:
We compared the independent reading of each imaging procedure with a reference assessment for structural disease defined by pathology or concordance between two imagings or with subsequent follow-up. The detection rate of each imaging modality was determined in per patient, per organ, and per lesion analysis.
Results:
Thirty-six consecutive patients (21 females, mean age: 57 years, sporadic MTC in 26 cases, median serum Ctn level: 760 pg/mL; range: 21–10,121) were analyzed. The reference assessment localized disease in 24 (64%) patients with 74 lesions detected in the thyroid bed (8), in neck lymph nodes (15), mediastinal lymph nodes (6), lungs (1), liver (2), bones (3), and other site (1). At the patient level, the detection rates were 64% (CI 0.48–0.80) for F-18-Dopa PET/CT with early acquisitions, 40% (CI 0.24–0.56) for F-18-FDG PET/CT, 40% (CI 0.24–0.56) for WB MRI, and 48% (CI 0.31–0.66) for WB CT scan.
Conclusions:
In MTC patients with increased Ctn and no known distant metastases, F-18-Dopa PET/CT is more sensitive to detect structural disease than any other imaging modality, including WB MRI.
Introduction
Calcitonin (Ctn) is a highly sensitive and specific tumor marker of medullary thyroid carcinoma (MTC) (1,2). Postoperatively, high levels of Ctn due to residual disease are frequently observed, particularly in patients with a high number of metastatic lymph nodes at initial diagnosis. Elevated Ctn levels correlate with tumor burden (3). When Ctn levels are less than 150 pg/mL and neck ultrasonography (US) is normal, other imagings are not recommended, because in most cases, they fail to localize residual disease (4 –6). The clinical challenge is, however, to localize the disease when a surgical resection can be curative. In a previous study, we found that the best imaging methods to explore MTC with postoperative elevated Ctn levels consisted in neck US in combination with chest computed tomography (CT) scan, liver magnetic resonance imaging (MRI), and bone scintigraphy or spine MRI (7). The performances of fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT were found to be disappointing, except for patients with short Ctn doubling time (7 –11).
F-18-Dopa (fluoro dihydroxyphenylalanine) PET/CT is abnormal in 66–75% of MTC patients with elevated Ctn levels (12). In these studies, all patients have persistent disease since they have a postoperatively elevated Ctn level (1,13 –17). The detection rate per patient or the patient-based sensitivity is highly dependent on the tumor burden and the Ctn levels of the patients studied, and the per-lesion sensitivity or the lesion detection rate is highly dependent on the other imaging modalities performed. There are, to our knowledge, no studies comparing F-18-Dopa PET/CT with a standardized morphological imaging workup.
We aimed to compare, in MTC patients with detectable Ctn and unknown localization of the source, F-18-Dopa PET/CT and whole-body (WB) MRI with F-18-FDG PET/CT, WB CT scan, neck US, and bone scintigraphy to localize recurrent/persistent disease.
Materials and Methods
Patients
Consecutive patients with MTC referred to our center for management between September 2014 and September 2016 were prospectively recorded if they presented the following criteria: (i) initial surgery consisting in total thyroidectomy with or without neck dissection, (ii) detectable Ctn levels greater than 20 pg/mL, (iii) absence of unequivocal argument for metastatic lesions in a previous imaging workup if performed (generally with neck and abdominal US or neck and thoraco-abdomino-pelvic CT scan or liver MRI and in some cases spine MRI), and (iv) absence of specific systemic treatment. They underwent the complete following assessment by F-18-Dopa PET/CT, F-18-FDG PET/CT, WB CT scan, WB MRI, neck US, and bone scintigraphy performed within four months. Thirty-six patients were enrolled in the study and we collected the following data: type of initial neck dissection, size of the primary lesion, site of the primary lesion, presence and location of metastatic lymph nodes at initial surgery, pTNM (tumor-node-metastasis) classification, RET protooncogene mutation status, postoperative Ctn level, Ctn and CEA (carcinoembryonic antigen) levels at the time of imaging assessment, and Ctn and CEA doubling times.
Image acquisition and analysis
F-18-Dopa PET/CT
F-18-Dopa PET/CT was performed using a time of flight General Electric DISCOVERY 690 PET/CT device. PET images were acquired at the time of the tracer injection (150 MBq of F-18-Dopa) for early images and recorded from the apex of the skull to the midthighs in 3D mode, 7–10 beds, 2 minutes/bed position, and then, a second acquisition was performed 20 minutes after injection for late images from the apex of the skull to the midthighs. Before PET acquisition, a low-dose CT acquisition for attenuation correction and anatomical correlation was performed with the same longitudinal field of view. The same CT acquisition was used for the early and late acquisitions. PET images were reconstructed on a 2562 matrix, using an iterative algorithm (ordered-subset expectation maximization—2 iterations 24 subsets) and postfiltering (3-points Z filter—weighting factors 1:2:1). CT images were reconstructed on a 5122 matrix using the usual filtered back-projection algorithm. After reconstruction, the final slice thickness was 3.27 and 2.5 mm regarding, respectively, PET and CT. Patient fasted for four hours before the examination.
F-18-FDG PET/CT
F-18-FDG PET/CT was performed using a time of flight General Electric DISCOVERY 690 PET/CT device. PET images were acquired 60 minutes after tracer injection (2–3 MBq/kg of FDG) and recorded from the apex of the skull to the midthighs in 3D mode, 7–10 beds, 2 minutes/bed position. Before PET acquisition, a low-dose CT acquisition for attenuation correction and anatomical correlation was performed with the same longitudinal field of view. PET images were reconstructed on a 2562 matrix, using an iterative algorithm (ordered-subset expectation maximization—2 iterations 24 subsets) and postfiltering (3-points Z filter—weighting factors 1:2:1). CT images were reconstructed on a 5122 matrix using the usual filtered back-projection algorithm. After reconstruction, the final slice thickness was 3.27 and 2.5 mm regarding, respectively, PET and CT. Patient fasted for 4–6 hours before the examination and had a venous glycemia with a median level of 5.3 mmol/L (range: 3.9–10.8).
CT scan
A 3-phase CT scan of the neck, thorax, abdomen, and pelvis was performed with helicoidal 64-b General Electric CT, 2.5 mm thickness: first an acquisition without contrast media injection on the abdomen; then, after the injection of 1.5 mL/kg of iodinated contrast media, an acquisition at the arterial (35 seconds after injection) on the neck, thorax, and abdomen and at the porto-venous phase (90 seconds) of the abdomen and pelvis.
Whole-body MRI
WB MRI was performed with two devices using the same protocol (Optima MR450w, 1.5T, General Electric and Discovery MR750w, 3T, General Electric). The protocol was defined as follows: T2-weighted axial sequences with fat suppression of the thorax, abdomen, and pelvis with 7 mm of slice spacing; diffusion-weighted axial sequences (b0, b800); and T1-weighted sequence without and with dynamic injection of contrast media on the abdominal part of the body with 2.5 mm slice spacing.
Bone scintigraphy
Bone scintigraphy was performed using a double-headed camera equipped with low-energy, high-resolution collimators (NM/CT 670 General Electric Medical System). It consisted of a 16 cm/min speed WB bone scan, and in spot lateral views of the ribs and skull and on any equivocal uptake, done 3–4 hours after the injection of 10 MBq/kg of 99m-technetium hydroxymethylene diphosphonate. Any suspect bone uptake was more thoroughly analyzed with a single-photon emission computed tomography (SPECT)/CT to assess whether the signal reflected a metastatic lesion or not.
Per patient imaging analysis
Three nuclear physicians and two radiologists read each imaging modality unaware of other results.
The reference assessment for structural disease was as follows: pathology when available, concordance between two imaging modalities, and/or confirmation of the lesion during follow-up. In each case, we determined the normality or abnormality of each type of imaging technique compared with the reference assessment, considering that all patients had residual/recurrent disease since they had a detectable Ctn level. Imaging considered uncertain significance was classified as abnormal for the statistical analysis. We also recorded whether the imaging procedure resulted in a therapeutic management change: surveillance alone versus surgery, external beam radiation therapy, or systemic treatment.
Per organ and per lesion imaging analysis
For each patient, we determined the abnormality of each imaging modality. Distinct organs were considered as follows: thyroid bed, neck lymph nodes, mediastinal lymph nodes, lungs, bone, liver, and other organs. We identified the best imaging procedure or the best combination of imaging procedures according to each organ considered.
True-positive lesions were defined as follows: metastatic cells on pathology after surgery or lesion described on at least two types of imaging or confirmed on follow-up.
False-positive lesions were defined as follows: absence of metastatic cells on pathology after surgery or a lesion described on only one type of imaging and not confirmed on follow-up.
Maximum standardized uptake value (SUVmax) of each lesion was measured on F-18-FDG and F-18-Dopa PET by using a volume of interest, with SUV being expressed by the most commonly used definition of SUV (g/mL) = [Tissue activity (Bq/mL)/injected activity (Bq)/body weight (g)]. For F-18-FDG PET/CT and F-18-Dopa PET/CT, SUVmax and size of each lesion were noted. For F-18-Dopa, we also collected the early SUVmax.
Sizes of the lesions were measured on WB CT scan and neck US, consisting in the largest diameter for organ lesion and the shortest axis for metastatic lymph node.
In case of more than 10 lesions in a single organ, 10 were considered for the statistical analysis.
Calcitonin and CEA doubling time
Calcitonin and CEA were collected at the time of F-18-Dopa imaging procedure (Ct2) and at least one year before (Ct1), and the Ct doubling time (CtDT) was calculated as follows: CtDT = (0.693 × Dt)/[Ln (Ct2/Ct1)] with Dt being the interval of time between the two measurements (15,18).
Statistical analysis
Quantitative data were expressed in mean or median and standard deviations, and qualitative data were expressed in percentage. The detection rate was calculated as the percentage of patients with a positive examination and a residual disease, among the patients who performed the examination. For neck US, only neck lesions were taken into consideration and for bone scintigraphy, only bone lesions were taken into consideration. Correlations between Ctn level more or less than 150 pg/mL or the CEA positivity or the Ctn DT more or less than 12 months or the presence of an RET mutation and the detection rate were searched with chi-square tests for each variable. All reported p-values are two sided and the significance level was 0.05. Analyses were performed using SAS statistical software (SAS Institute, Inc., Cary, NC) version 9.4.
Results
Patient characteristics
Thirty-six MTC patients were prospectively included. Clinical characteristics are summarized in Table 1. Ten (28%) patients had a germ line RET mutation: seven patients were index cases and three were diagnosed by genetic screening. All patients underwent total thyroidectomy with neck dissection. The median interval of time between the initial surgery and F-18-Dopa PET/CT was 8.3 years (range: 0.1–35.7). In 34 cases, a morphological assessment had previously been performed and was normal in 32 cases and doubtful in 2 cases, and in the last 2 cases, the study assessment was the first postoperative assessment. Median Ctn level was 760 pg/mL (range: 21–10,121) and median CEA level was 12 ng/mL (range: 1–578). Five patients had a Ctn level below 150 pg/mL. Median Ctn doubling time was 1.5 years (range: 0.4–20.7). The Ctn doubling time was shorter than 6 months in 2 (6%) patients, between 6 and 12 months in 5 (14%) patients, and longer than 12 months in 29 patients (81%).
Clinical Characteristics of the 36 Patients
N, node; RET mutation, rearrange during transfection mutation.
F-18-Dopa PET/CT and bone scintigraphy were performed in all 36 patients, F-18-FDG PET/CT in all patients except one because of a high level of glycemia, WB MRI in all except one because of claustrophobia, neck US in all patients except one because of refusal of the patient, and WB CT scan in 33 patients because of contrast agent allergy or kidney failure.
Per patient analysis
All patients had an elevated Ctn level, indicating residual disease (Fig. 1). Structural disease was detected in 23 of the 36 patients (64%). F-18-Dopa PET/CT was abnormal in 24 cases, F-18-FDG PET/CT in 16 cases, WB MRI in 15 cases, WB CT scan in 16 cases, and neck US in 11 cases. F-18-Dopa, PET/CT was falsely positive in one case (esophageal diverticulum), F-18-FDG PET/CT in two cases (inflammatory neck lymph nodes), and WB MRI in one case (metabolic bone disease). We did not observe a false-positive WB CT scan. The detection rates were 64% (CI 0.48–0.80) for F-18-Dopa PET/CT, 40% (CI 0.24–0.56) for F-18-FDG PET/CT, 40% (CI 0.24–0.56) for WB MRI, 48% (CI 0.31–0.66) for WB CT scan, and 31% (CI 0.16–0.47) for neck US.
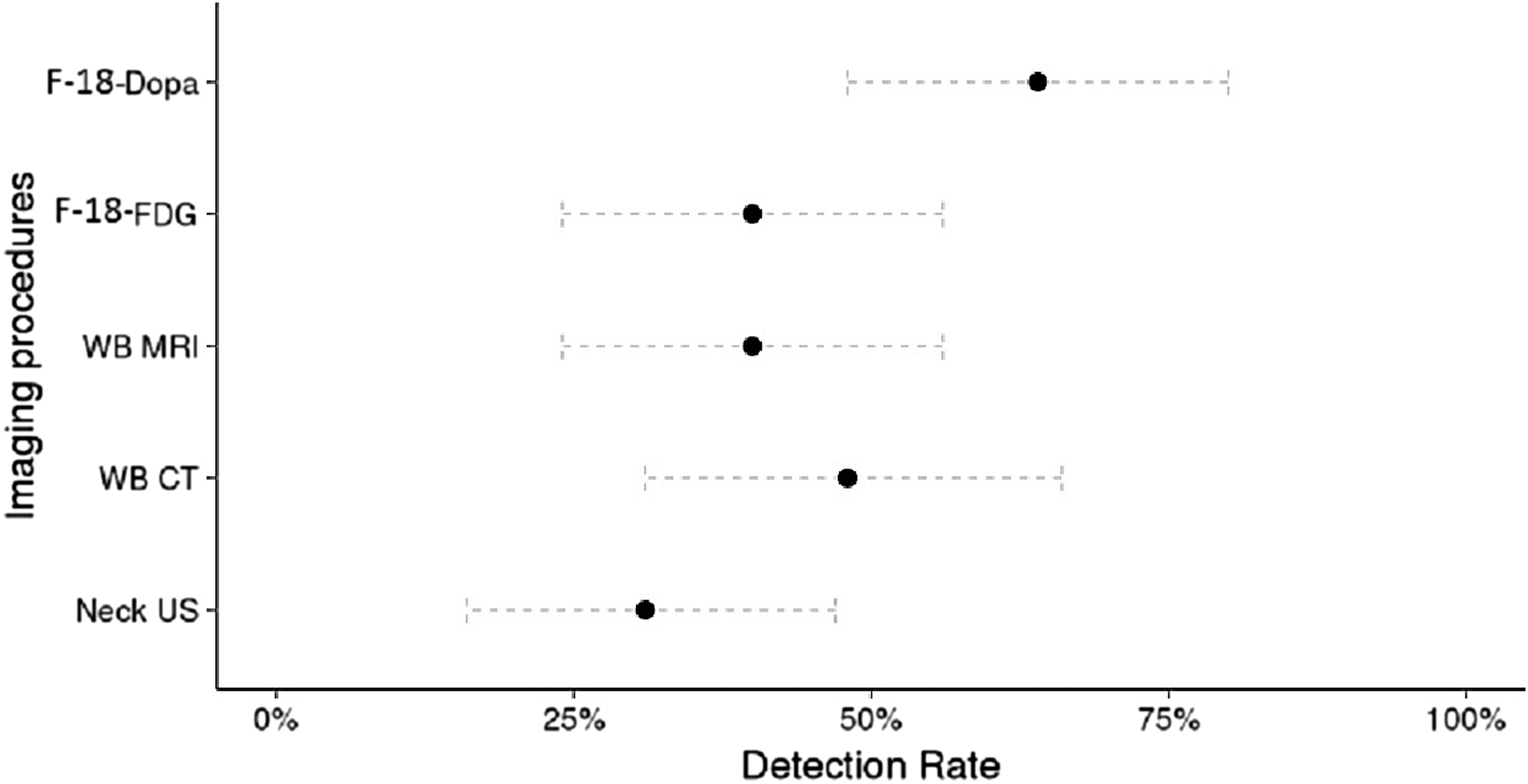
Per patient detection rate (with confidence interval) of each imaging procedure. For neck US detection rate, only neck disease was taken into consideration. US, ultrasonography.
The sensitivity of F-18-Dopa PET/CT was higher in patients with Ctn levels >150 pg/mL compared with patients with Ctn levels <150 pg/mL (33% vs. 90% p = 0.002). Lesions detected with F-18-Dopa in patients with Ctn <150 pg/mL were located in the thyroid bed in one case, in neck lymph nodes in two cases, in thyroid bed and neck lymph node in one case, and in bone in one case. The two thyroid bed relapses were also detected by neck US, but not the neck lymph nodes. Tumor sizes ranged from 5 to 12 mm and Ctn levels were 23, 32, 41, 97, and 120 pg/mL.
The sensitivity of F-18-Dopa PET/CT was higher in patients with CEA ≥10 pg/mL than those with CEA <10 pg/mL (92% vs. 50%, p = 0.03). There was no relationship between F-18-Dopa PET CT and Ctn doubling time (<12 months vs. >12 months, p = 0.42).
The sensitivity of F-18-FDG PET/CT was higher in patients with Ctn doubling time <12 months than those with Ctn doubling time >12 months (86% vs. 33%, p = 0.04) and was higher in patients with sporadic MTC than in those with RET germ line mutations (62% vs. 0%, p = 0.001), with a median Ctn level higher in sporadic patients compared with patients with RET germ line mutations (1330 pg/mL vs. 579 pg/mL) and a comparable median Ctn doubling time (1.56 years vs. 1.13 years). There was no relationship between F-18-FDG PET CT and Ctn (p = 0.23) or CEA levels (p = 0.88). The population was too small to perform a multivariate analysis.
There was no relationship between the sensitivity of WB MRI and WB CT with Ctn levels (p = 0.39 and p = 0.06, respectively), CEA levels (p = 0.06 and p = 0.77, respectively), or Ctn doubling time (p = 0.34 and p = 0.29, respectively). There was no relationship between the sensitivity of any of the used imaging techniques (F-18-Dopa, F-18-FDG, WB MRI, and WB CT) and the interval of time between surgery and the actual imaging with a median interval of time of 8.1 months (p = 0.28; p = 0.85; p = 1.0 and p = 0.76, respectively).
Per lesion analysis
We identified 74 lesions among 23 patients with abnormal findings consistent with structural disease (Table 2). Eight lesions were found in the thyroid bed, 32 in neck lymph nodes, 17 lesions in mediastinal lymph nodes, 1 lesion in the lungs, 4 lesions in bone, 11 lesions in the liver (including 10 for 1 patient and 1 lesion in the liver in another one), and 1 lesion in an arm muscle. The median size of the lesions excluding bone lesions was 10 mm (range: 4–16).
Interest of F-18-Dopa in Combination with Other Techniques for Lesion Detection
F-18-Dopa, fluoro dihydroxyphenylalanine; LN, lymph node; MRI, magnetic resonance imaging; NA, not applicable; US, ultrasonography; WB CT, whole-body computed tomography.
Early acquisition of F-18-Dopa PET/CT detected 62 (84%) of the 74 lesions, whereas late acquisition only detected 46 (62%) of the lesions. None of the lesions was detected on the late acquisition only. On F-18-Dopa PET/CT, the median early SUVmax was 3.5 (0.9–13.9) and the median late SUVmax was 2.5 (0.6–13). On F-18-FDG PET/CT, the median SUVmax was 1.5 (1.1–3.3).
The per lesion detection rates were 84% (CI 0.75–1) for F-18-Dopa, 45% (CI 0.34–0.57) for F-18-FDG, 23% (CI 0.13–0.33) for WB MRI, and 32% (CI 0.21–0.44) for WB CT scan. The per lesion detection rate for one F-18-Dopa was 100% in the thyroid bed (8/8); 97% in neck lymph nodes (31/32); 100% in chest lymph nodes (17/17); 100% in bone (4/4); 0% in the liver (0/11); 100% in the lungs (1/1), and 100% in other locations (1/1). For F-18-FDG, the per lesion detection rate was 50% in the thyroid bed (4/8); 63% in neck lymph nodes (20/32); 47% in chest lymph nodes (8/17); 0% in the bone (0/4); 0% in the liver (0/11); 0% in the lungs (0/1), and 100% in other locations (1/1). For WB MRI, the per lesion detection rate was 50% in the thyroid bed (4/8); 16% in neck lymph nodes (5/32); 18% in chest lymph nodes (3/17); 0% in the bone (0/4); 100% in the liver (11/11); 100% in the lungs (1/1), and 0% in other locations (0/1). For WB CT, the per lesion detection rate was 50% in the thyroid bed (4/8); 31% in neck lymph nodes (10/32); 29% in chest lymph nodes (5/17); 0% in the bone (0/4); 9% in the liver (1/11); 100% in the lungs (1/1), and 0% in other locations (0/1). For neck US, the per lesion detection rate was 63% in the thyroid bed (5/8) and 38% in neck lymph nodes (12/32). For bone scintigraphy, the per lesion detection rate was 25% in the bone (1/4). F-18-Dopa PET/CT was more sensitive than any other imaging modality, except for liver metastases where liver MRI was more sensitive.
The per lesion detection rate of F-18-Dopa PET/CT was not related to early SUVmax (<3.5 vs. ≥3.5; p = 0.11), late SUVmax (<2.4 vs. ≥2.4; p = 0.08), nor to the size of the lesions (<10 mm vs. ≥10 mm; p = 0.26), CEA level (<10 ng/mL vs. ≥10 ng/mL; p = 1.00), nor to the Ctn doubling time (<12 months vs. ≥12 months; p = 0.59). The per lesion detection rate of F-18-FDG PET/CT correlated with the size of the lesions (<10 mm vs. ≥10 mm; 28% vs. 100%; p < 1.3 × 10−7).
Among the 74 lesions, 73 were detected on F-18-Dopa PET/CT and WB MRI, and 64 were detected on F-18-Dopa PET/CT and WB CT. Detection of the lesions according to the imaging modalities is shown in Table 2. The combination of F-18-Dopa PET with liver MRI and neck US detected all 74 lesions.
We found five lesions of uncertain significance with F-18-Dopa (three in the neck and two in the bone), nine with F-18-FDG (eight in the neck and one in the bone), five with WB MRI (all in the bone), and zero with WB CT, neck US, or bone scintigraphy. All lesions with uncertain significance were considered abnormal in the analysis.
Therapeutic changes
Therapeutic changes occurred after imaging assessment in 8 of the 36 (22%) patients of the cohort. It consisted in neck surgery in seven cases (Fig. 2) and external beam radiation targeting a bone lesion in one case. In the seven cases who underwent surgery, F-18-Dopa PET/CT was abnormal in all cases, F-18-FDG PET/CT was abnormal in five, WB MRI in five, WB CT scan in six, and neck US in six. Among the seven patients undergoing reoperation, the Ctn level became undetectable in one and decreased by more than 50% in two cases, with Ctn levels that fell from 194 to 34 pg/mL and from 3568 to 1386 pg/mL, respectively. Bone scintigraphy did not disclose the bone lesion that was irradiated.
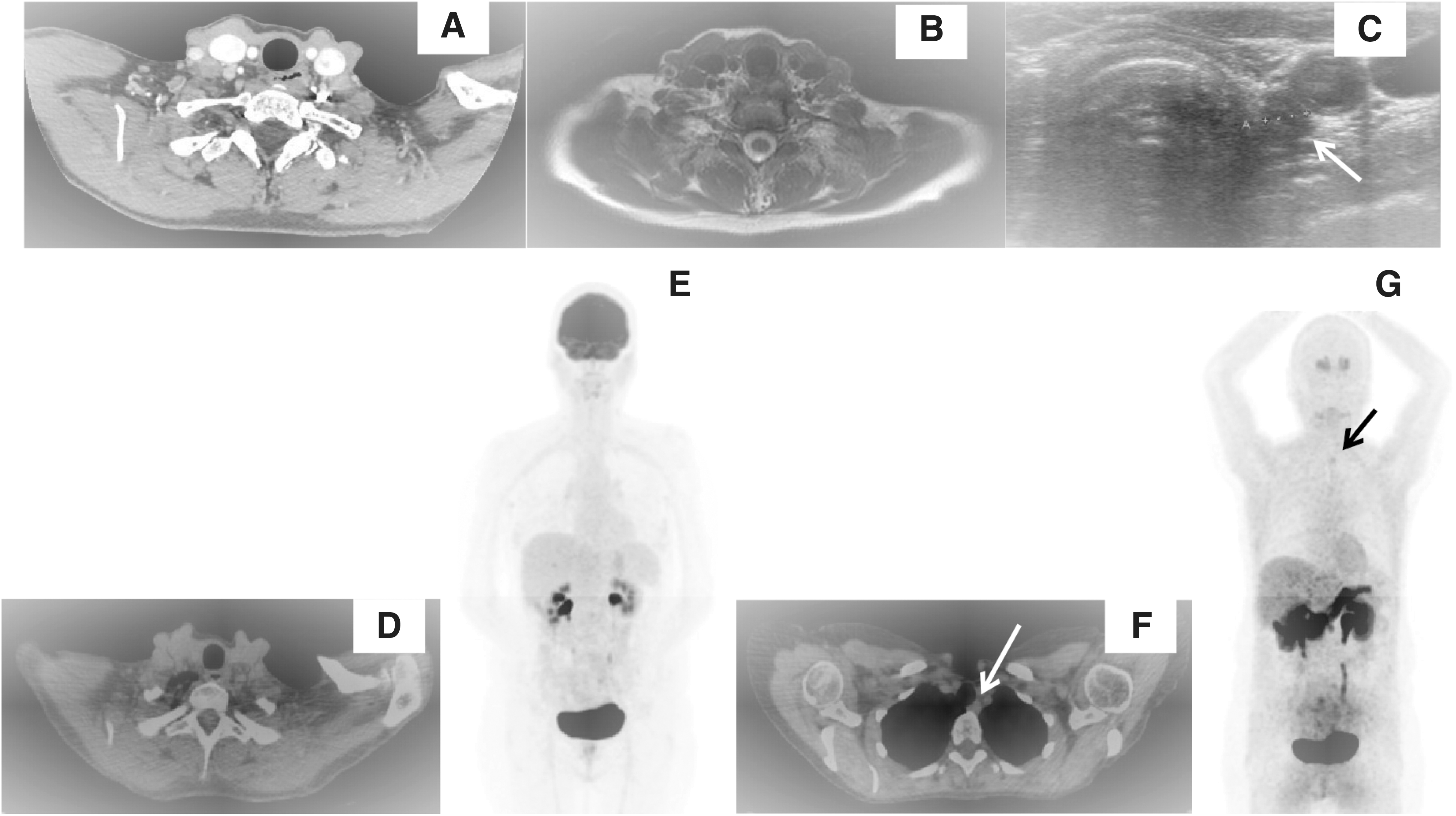
A 56-year-old patient with a single latero-tracheal neck recurrence detected on F-18-Dopa (black and white arrows) and neck US (
Discussion
These results show a higher detection rate of F-18-Dopa for the location of MTC-persistent/recurrent disease compared with WB CT and with WB MRI, with disease localized in 64% of the patients. This is, to our knowledge, the first study comparing F-18-Dopa with WB MRI, F-18-FDG, and WB CT. F-18-Dopa also disclosed a better detection rate than F-18-FDG. This result is in accordance with our previous results showing that F-18-FDG PET/CT has a lower detection rate than conventional imaging combining a WB CT, a dedicated liver MRI, and a spine MRI (7), an observation that is consistent with some but not all studies (16,17,19). The intensity of F-18-FDG uptake is indeed low in most MTC patients. The intensity of F-18-Dopa uptake is also low, but early acquisition clearly increases the level of F-18-Dopa uptake and the number of lesions detected. This intensity of uptake is, however, lower than in midgut neuroendocrine tumors (NETs), resulting in difficulties in interpretation of the images in some cases. Because of elevated Ctn levels, diagnosis of recurrent/persistent disease is certain, and because localization of the disease is challenging, we considered images of uncertain significance abnormal. The consequence is an increase in the sensitivity of F-18-Dopa, and of all other imaging modalities since we applied the same rules for all imaging modalities.
WB MRI and F-18-Dopa have the advantage of being a one-step procedure. In NETs, the first results on the sensitivity of WB MRI compared with C-11-5HPT (-C-11-5 hydroxytryptophan, a precursor in serotonin synthesis), PET/CT, or Ga-68-DOTATOC (Ga-68-DOTA-D-Phe1-Tyr3 octreotide, an analog of somatostatin) PET/CT are disappointing with WB MRI being more sensitive for the detection of liver lesions and abdominal lymph nodes but not for lung, mediastinal lymph nodes, and bowel lesions (18). As of yet, liver MRI remains indeed the best imaging modality for the detection of liver metastases of NET (20,21).
The major limitations of this study are the small number of patients due to the rarity of the disease, the absence of systematic pathological proof of the lesions, and the fact that a few patients did not complete every imaging procedure. Our patients were also highly selected: we included 34 patients with a previous normal or doubtful imaging workup and this evaluation was the initial postoperative analysis in only 2 patients. We therefore favored the inclusion of patients with a low tumor burden and normal neck US and normal CT scans. This is the reason, in our opinion, for the low detection rate of neck recurrences using US. One advantage of F-18-Dopa PET over neck US is, however, the possibility to evaluate retroclavicular and retropharyngeal regions often affected by MTC recurrences and not visible on neck US.
As previously reported, the detection rate of F-18-Dopa was lower in patients with low Ctn levels (<150 pg/mL), but it was still significant with disease located in 33% of the cases. We think that it is interesting to localize morphological disease when Ctn levels are below 150 pg/mL, because these patients did typically not have distant metastases and they may be amenable to locally curative treatments (22).
In contrast, when Ctn levels are above 150 pg/mL, the imaging assessment is more frequently positive, but there is also an increased risk for (multi)metastatic disease. The visualization of all lesions may guide the treatment decision, which may consist of focal treatment modalities, systemic treatment with tyrosine kinase inhibitors in case of RECIST progression, or in a combination of both.
Importantly, following F-18-Dopa imaging, 7 (19%) of the 36 patients benefited from changes in treatment management. However, the Ctn level became undetectable only in a single case, and there was a decrease by more than 50% in only two cases.
The F-18-Dopa detection rate did not correlate with the Ctn doubling time or the presence of a germ line RET mutation.
F-18-FDG PET/CT was more sensitive in sporadic patients, most probably because they had higher Ctn levels even though we did not find a correlation between FDG sensitivity and Ctn levels. The limited numbers included in the study can be an explanation for this result.
In the per lesion analysis, we reported false-positive lesions in one case for F-18-Dopa, in two cases for F-18-FDG, and in one case for WB MRI. These false-positive readings were associated with an esophageal diverticulum (F-18-Dopa), inflammatory nodes (F-18-FDG), and lung nodules (WB MRI). The risk of false-positive lesions should always be taken into consideration when the indication for surgery is established based on a single-imaging modality.
The reference assessment for structural disease combining several modalities, including F-18-Dopa with early acquisition, was negative in 36% (13/36) of the cases. This is partly explained by the pattern of residual disease; we often observed small miliary metastatic lesions in lymph nodes, liver, and lung. The size of these lesions is particularly small and difficult to detect on functional imaging because it is under the spatial resolution of scintigraphy or PET/CT. Moreover, for lymph node lesions, conventional imaging (CT scan and MRI) is very often considered normal because the shortest size of the lymph nodes is often under 15 mm.
Based on our results, MTC patients with elevated Ctn levels with normal or doubtful neck US and neck and chest CT scan should be evaluated with F-18-Dopa PET/CT and liver MRI. In case of a doubtful F-18-Dopa uptake, especially if its location is unusual, further confirmation with cross-sectional imaging and, if possible, fine needle aspiration cytology with measurement of Ctn levels in the aspirate should be performed.
In conclusion, in MTC patients with increased Ctn levels and uncertain localization of the source, F-18-Dopa PET/CT is more sensitive than any other imaging modality, including WB MRI, to detect structural disease. If early acquisition images are performed, F-18-Dopa PET/CT can detect disease in 33% and 90% of the patients with Ctn levels below and above 150 pg/mL. Late acquisition imaging appears to be of limited value.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.