
Abstract
Objective:
The authors' institution—a safety net, university, and tertiary-care hospital located in West Texas—has a high number of hospital admissions for complicated thyrotoxicosis. It was hypothesized that unfavorable socioeconomic conditions result in increased risk of poor outcomes in hyperthyroid patients, and increased rates of hospitalization for thyrotoxicosis in West Texas. The primary aim of this study was to identify factors associated with admission for complicated thyrotoxicosis in patients living in the Panhandle and Llano Estacado of Texas.
Method:
A retrospective chart review of patients aged ≥18 years with a diagnosis of thyrotoxicosis evaluated at the authors' institution from January 2011 to January 2017. Patients were divided into two groups: a hospitalized group, consisting of patients who required hospitalization for complicated thyrotoxicosis, and an outpatient group. Demographics, clinical, and biochemical data were reviewed to identify factors associated with hospitalization for complicated thyrotoxicosis.
Results:
The hospitalized group consisted of 80 patients, and the outpatient group consisted of 294 patients. Thyrotoxicosis accounted for 0.05% of all-cause hospital admissions during the study period. Patients with thyrotoxicosis and a lack of health insurance had 12 times higher odds of being hospitalized for complicated thyrotoxicosis compared to patients with commercial insurance. Conversely, the odds of hospitalization for complicated thyrotoxicosis were reduced by 63% in patients with a higher median income, and by 33% in those with college or university studies versus high school studies. Thirty-two percent of patients hospitalized for complicated thyrotoxicosis presented with thyroid storm, and this accounted for 7% of the studied cohort.
Conclusion:
Socioeconomic conditions are the main factors associated with the odds of being admitted to a hospital in West Texas for complicated thyrotoxicosis, including thyroid storm. Patients without healthcare insurance have higher odds of admission, while patients with higher education and living in areas of higher income have lower odds of hospital admission due to thyrotoxicosis.
Introduction
Thyrotoxicosis, especially when caused by hyperthyroidism, is a condition that can be managed in the outpatient setting in most cases. Thyroid storm is a rare complication of thyrotoxicosis in which the hypermetabolic state results in acute decompensation of multiple organs and carries a mortality rate of about 10% (1,2).
Several studies have been conducted to try to determine factors that could allow the clinician to identify those patients who are at higher risk of developing complicated thyrotoxicosis or thyroid storm (3). Larger goiters have been associated with more severe symptoms, and older age with a higher risk for cardiovascular complications of thyrotoxicosis (3). On the other hand, no correlation has been found between the severity and duration of symptoms until diagnosis (4), genetic factors contributing to the development of hyperthyroidism in the case of Graves' disease (5), or levels of thyroid hormone in serum (3,6). Twenty years ago, a study conducted in Maryland by Sherman et al. (7) reported that poor socioeconomic conditions are a risk factor for complicated thyrotoxicosis and thyroid storm. Nonetheless, the role of socioeconomic factors in the development of complicated thyrotoxicosis is hardly mentioned in the thyroid literature, and to the authors' knowledge, no measures have been implemented by healthcare policy makers to address this in the United States.
A nationwide survey conducted in Japan estimated an incidence of thyroid storm of 0.20 cases per 100,000 per year. It occurs in 0.22% of all thyrotoxic patients, and in 5.4–10% of patients hospitalized for thyrotoxicosis (2,8). An unusually high number of admissions for complicated thyrotoxicosis and thyroid storm have been noticed at the authors' institution. University Medical Center (UMC) is a safety net, public, tertiary-care hospital, located in the city of Lubbock, Texas, affiliated with Texas Tech University Health Sciences Center School of Medicine (TTUHSC-SOM). The hospital covers the Panhandle and Llano Estacado of Texas, an area of 37,500 square miles that includes counties from West Texas and Eastern New Mexico, with a population of 1,230,000 in 2013. The dispersion of the population and long distances to specialized centers, the limited number of endocrinologists in the area (90,000 adult patients per endocrinologist in West Texas vs. 48,000 adult patients per endocrinologist in the United States) (9), and a high percentage of the population with no insurance (15.4% of the population <65 years without medical insurance in Lubbock compared to 10.1% for the entire country) (10) represent challenges for healthcare delivery within this area.
It was hypothesized that socioeconomic factors, as described 20 years ago, still result in disparities in regard to the outcome of hyperthyroid patients in some regions in the United States (7). The study aimed to identify risk factors for complications of thyrotoxicosis requiring hospitalization in patients living in the Panhandle and Llano Estacado of Texas. If the hypothesis is correct, the results should increase awareness of this problem, and help illustrate the need for strategies aimed to reduce hospitalizations for this ambulatory care-sensitive condition.
Methods
Study cohort
After approval by the Texas Tech University Health Sciences Center Institutional Review Board, a retrospective review was conducted of records of adult patients with an ICD-9 and ICD-10 diagnosis of hyperthyroidism or thyrotoxicosis treated at the institution between January 1, 2011, and January 1, 2017. The diagnosis of thyrotoxicosis was verified by reviewing clinical notes and laboratory data; patients were excluded if the diagnosis of thyrotoxicosis could not be confirmed. Patients were separated into two groups: outpatient group and hospitalized group. Patients managed exclusively in the outpatient setting were allocated in the former, and those hospitalized for thyrotoxicosis at any point during the course of their disease were allocated in the latter. Patients who were hospitalized for thyrotoxicosis at the university hospital but who had also been seen as outpatients before or after their hospitalization were assigned to the hospitalized group and excluded from the outpatient group, while those who had been seen as outpatients but admitted in a different facility for complicated hyperthyroidism at any point of the course of their disease were excluded from the analysis due to lack of availability of the data from their hospital stay.
For the analysis of the clinical and laboratory data, all subjects from the outpatient group with a thyrotropin (TSH) >0.02 mIU/L at the time of their initial visit were excluded. Patients with higher TSH levels due to therapy for hyperthyroidism but with a definitive diagnosis of thyrotoxicosis were still included for the analysis of demographic data that would not be altered, regardless of the disease status at the time of the patient's visit.
Data collection
Demographic, clinical, laboratory, and outcome data were collected from the electronic medical records system. U.S. Census Bureau 2012–2016 American Community Survey five-year estimates (11) were used to calculate median income in 2016 inflation-adjusted dollars of the residence ZIP code for patients from the state of Texas and New Mexico. Google Maps® was used to calculate the distance between the center of the patient's residence ZIP code and TTUHSC-SOM. The severity of thyrotoxicosis in hospitalized patients was categorized retrospectively using the Burch–Wartofsky point scale (12). The Burch–Wartofsky score was used as an outcome measure for hospitalized patients, along with hospital length of stay, inpatient mortality, and the need for intensive care unit or step down unit admission.
Statistical analysis
Means (standard deviation), frequencies (percentage), or medians with interquartile range (IQR) of the different variables were determined, as deemed appropriate, for each group. Differences between groups were assessed using the two-tailed Wilcoxon rank-sum test for continuous data, or chi-square test for categorical data. The association between hospital admission and demographic factors that were significantly different between groups was assessed using odds ratios (OR) and confidence intervals (CI), and refined in three stages. At the first stage, unadjusted OR for admission were calculated for each factor independently. At the second stage, predictors that showed significance at the previous stage were arranged in three blocks according to their theoretical nature: personal, socioeconomic, and clinical factors. Multiple logistic regression analyses were performed to calculate the adjusted OR within each block of variables. At the third stage, only significant predictors at the previous stage were included in the refined multiple regression model. Correlations between some clinical parameters and outcome measures were calculated utilizing Spearman's rho. The significance level was set at 0.05, and Bonferroni correction was used to control familywise error when multiple significance tests were performed. All statistical analyses were performed using Stata v13.1 (StataCorp, College Station, TX).
Results
During the six-year period, 414 new patients were referred for evaluation and management of hyperthyroidism to the outpatient clinic. Ninety-five patients were hospitalized at the university hospital with a diagnosis of thyrotoxicosis. After the initial screening, 120 patients from the outpatient group and 15 patients from the hospitalized group were excluded from further analysis (Fig. 1). The final data set for demographic analysis consisted of 374 cases of thyrotoxicosis, of which 294 cases were allocated to the outpatient group and 80 to the hospitalized group. In a second screening, aimed for analysis of the clinical data, 84 subjects with a serum TSH >0.02 mIU/L were excluded. All 84 patients were from the outpatient group, as none of the patients in the hospitalized group had a TSH >0.02 mIU/L. The final cohort for the later analysis consisted of 290 patients, with 210 allocated to the outpatient group and 80 to the hospitalization group (Fig. 1). The total number of admissions at UMC during the study period was 162,217, excluding newborns. Admissions for complicated thyrotoxicosis affected 21% of the hyperthyroid patients in the cohort and accounted for 0.05% of all-cause hospital admissions during the six-year study period.
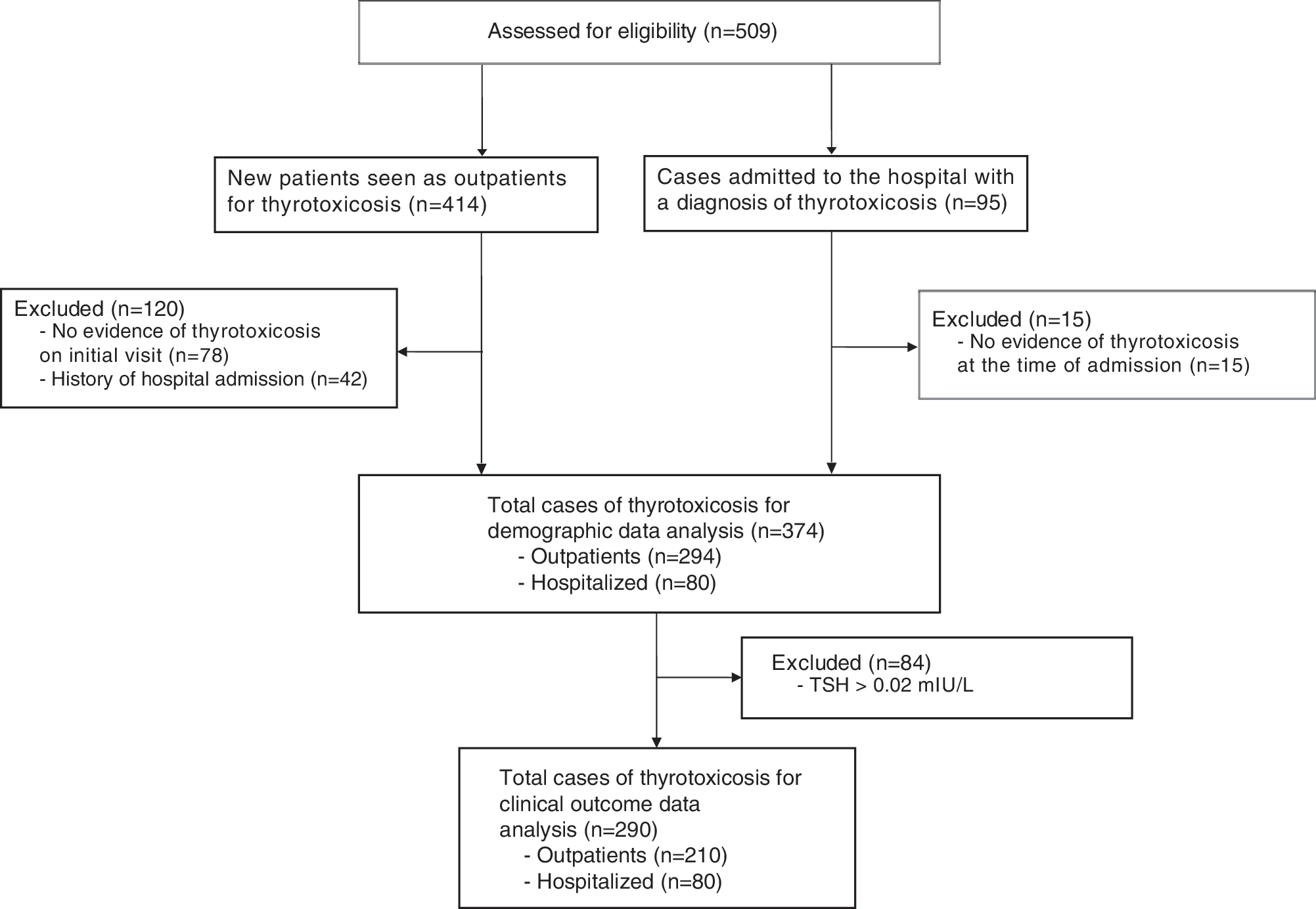
Schematic representation of patient selection and distribution in the different groups. TSH, thyrotropin.
Graves' disease was the most common cause of thyrotoxicosis in both groups, accounting for 58.5% and 88.8% of the cases in the outpatient group and hospitalized group, respectively (see Appendix Table A1 for more details). Table 1 summarizes the demographic characteristics of patients in the outpatient and hospitalized groups. Females accounted for the majority of hyperthyroid patients in both groups, but the percentage of male patients in the hospitalized group was higher than in the outpatient group. The distribution of patients was significantly different with respect to ethnicity, with a lower percentage of Hispanic/Latino patients in the hospitalized group compared to the outpatient group. In regards to health insurance coverage, hospitalized patients were more likely to have no health insurance (self-pay) or Medicaid coverage than patients in the outpatient group. Commercial insurance or Medicare coverage was less frequent in the hospitalized group (31%) than in the outpatient group (72%). Hospitalized patients were also more likely to be single, divorced, or widowed. Concerning education, the distribution among the different categories within this variable was significantly different. Twice as many subjects in the outpatient group had higher education (51%) compared to hospitalized patients (26%). Similarly patients in the outpatient group were less likely to have less than a high school education (13%) compared to the hospitalized group (20%). Finally, the estimated median income by ZIP code was significantly lower in the hospitalized group ($42,000) than in the outpatient group ($47,000).
Demographic Characteristics of Thyrotoxic Patients Allocated to Outpatient and Hospitalized Groups
Number and (% of group) are shown for each category, except for age, ZIP median income, and ZIP distance, as indicated.
Includes local and nonlocal county indigent program (n = 17), state correctional (n = 5), Texas department of criminal justice (n = 3), military (n = 1), veterans administration (n = 1), and other government program (n = 1), liability (n = 1).
SD, standard deviation; IQR, interquartile range.
Clinical data were obtained for thyrotoxic patients with TSH levels <0.02 mIU/L. For the outpatient group, the data were obtained at the time of the initial clinic visit, and for the hospitalized group, they were obtained at the time of hospital admission. Compared to the outpatient group, patients in the hospitalized group weighed significantly less (73.9 kg vs. 79.4 kg), had a lower body mass index (26.5 kg/m2 vs. 29.1 kg/m2), and had a higher heart rate (124 bpm vs. 87.3 bpm). In regards to liver function tests, total bilirubin was significantly higher for the hospitalized group (0.8 mg/dL vs. 0.5 mg/dL), and no significant differences were observed in aspartate and alanine aminotransferase levels. Similarly, compared to the outpatient group, serum free thyroxine (fT4; 5.5 ng/dL vs. 3.3 ng/dL), free triiodothyronine (fT3; 16.5 pg/mL vs. 9.8 pg/mL) and thyroid stimulating immunoglobulin (TSI; 387.3% vs. 324.7%) levels were significantly higher and thyroid gland size (32.7 g vs. 20.5 g) was significantly larger in hospitalized patients (see Appendix Table A2 for more details). When analyzing the clinical data without excluding patients with a TSH >0.02 mIU/L, glomerular Filtration Rate and corrected calcium were significantly higher in the hospitalized patients than in the outpatients (162 mL/min/1.73 m2 vs. 127 mL/min/1.73 m2 and 9.7 mg/dL vs. 9.4 mg/dL, respectively). Otherwise, there was no major difference in regards to the data analysis.
Table 2 shows precipitating factors and outcome measures for the hospitalized group. Sixty-nine percent of patients either had no diagnosis of hyperthyroidism before admission or had a previous diagnosis of hyperthyroidism but were not compliant with medication. Only 14% were deemed as treated suboptimally. In regards to the severity of thyrotoxicosis, 23 (28.7%) subjects were categorized as having complicated thyrotoxicosis, 31 (38.8%) as impending storm, and 26 (32.5%) as thyroid storm (7% of the analyzed cohort). Nearly half of the hospitalized patients required intensive care unit or step down unit admission. The length of hospitalization ranged from 1 to 15 days, with most patients requiring >48 hours in hospital. The median length of stay was three days for complicated thyrotoxicosis (range 1–14 days) and impending storm (range 1–15 days) and four days for thyroid storm (range 1–9 days). Twelve patients were admitted to the hospital more than once for thyrotoxicosis, one of whom was admitted three times for a diagnosis of complicated thyrotoxicosis. No patient died while in hospital.
Precipitating Factor and Outcome Measures of Thyrotoxic Hospitalized Group
Number of patients (% of group) are shown for each category.
Includes bacterial infection (n = 2), diabetes ketoacidosis (n = 2), thyroidectomy (n = 1), inability to tolerate medication (n = 1), recurrent hyperthyroidism (n = 1), amiodarone-induced thyrotoxicosis (n = 1), and patient instructed to discontinue treatment by provider (n = 4).
ICU, intensive care unit.
Points assigned to the hospitalized patients in the different criteria per the Burch–Wartofsky scale are detailed in Table 3. Cardiac manifestations were the most predominant, with 51% of patients presenting with a heart rate >140 bpm or atrial fibrillation. Cardiovascular dysfunction criteria contributed a median percentage of 50 of the total Burch–Wartofsky score. The next most prominent score was for the gastrointestinal criteria, contributing a median percentage of 6.7 of the total Burch–Wartofsky score. No correlation was found between Burch–Wartofsky score and thyroid gland size or thyroid hormone levels. Similarly, higher serum fT4 and fT3 levels were not associated with a higher score on the cardiovascular criteria of the Burch–Wartofsky scoring system. Moreover, even when excluding patients who were on beta blockers or calcium channel blockers at the time of visit from the outpatient group, serum fT4 and fT3 levels as high as those observed in hospitalized patients were also observed in several patients in the outpatient group.
Points Assigned to the Hospitalized Patients in the Different Criteria per the Burch–Wartofsky Point Scale
Agitation.
Delirium, psychosis, extreme lethargy.
Seizure, coma.
Diarrhea, nausea/vomiting, abdominal pain.
Unexplained jaundice.
Pedal edema.
Bibasilar rales.
Pulmonary edema.
Table 4 presents the OR and adjusted OR for factors that were significantly different between the outpatient and hospitalized groups and that could represent risk factors for hospitalization due to complicated thyrotoxicosis. A final OR model for socioeconomic factors and hospital admission risk for complicated thyrotoxicosis is shown in Figure 2. Not having healthcare insurance coverage (self-pay) or having “other” insurance coverage (which for the most part includes patients under indigent support programs) were factors associated with higher odds of hospital admission for complicated thyrotoxicosis. Contrary to that, having higher education and living in a ZIP code with higher median income were factors associated with lower odds of hospital admission for thyrotoxicosis. Interestingly, being Hispanic/Latino was another factor associated with lower odds of hospitalization.
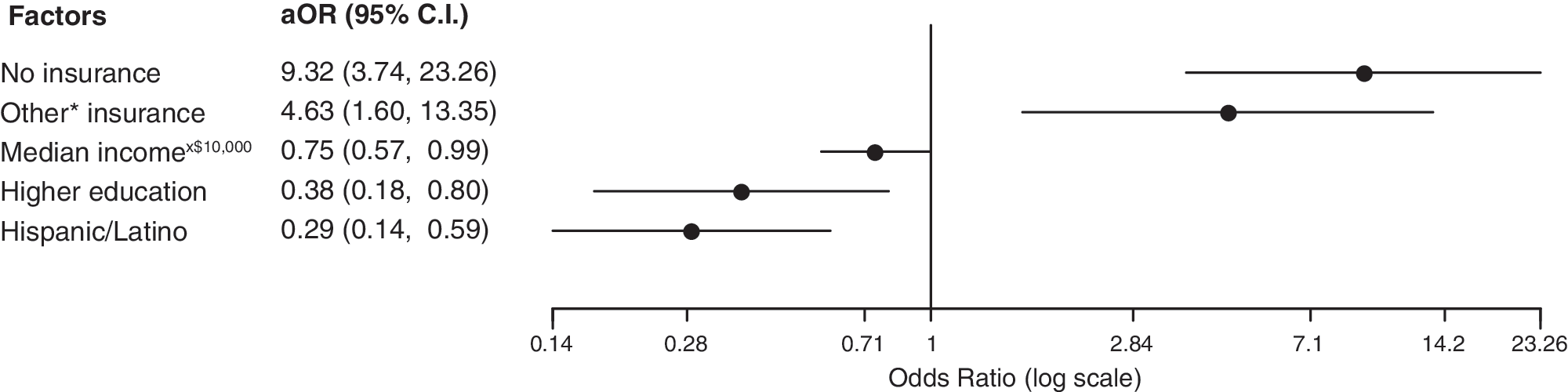
Odds ratio model for socioeconomic factors and hospital admission risk for complicated thyrotoxicosis. *Includes local and nonlocal county indigent program (n = 17), state correctional (n = 5), Texas department of criminal justice (n = 3), military (n = 1), veterans administration (n = 1), and other government program (n = 1), and liability (n = 1).
Factors Associated with Hospital Admission due to Complicated Hyperthyroidism
Statistically significant values are shown in bold.
Adjusted for the other factors within the same block of variables.
Adjusted for the other factors included in the final model.
OR for each $10,000 increase in median income of residency area (zip code).
OR for each 10-mile increase in distance from residency to hospital.
OR, odds ratio; AOR, adjusted odds ratio; CI, 95% confidence interval; TMNG, toxic multinodular goiter.
Discussion
The present results show that there is a strong association between socioeconomic factors and the outcomes of hyperthyroid patients. Patients with a higher level of education (higher education vs. high school) and living in areas with a higher median income are less likely to be hospitalized for complicated thyrotoxicosis. On the other hand, patients with no healthcare insurance coverage or under indigent support programs have increased odds for hospital admission due to complicated thyrotoxicosis. Moreover, 38% of patients who met the criteria of thyroid storm upon admission had no insurance coverage, and 77% had no higher education, suggesting that patients of lower socioeconomic status not only have a higher risk of admission but also might have more severe symptoms at the time of presentation. The findings concur with those published in 1996 by Sherman et al. who also reported that thyrotoxic patients without insurance coverage or with Medicaid were more likely to present with complicated thyrotoxicosis (7). More than 20 years later, socioeconomic factors continue to determine the risk for complicated thyrotoxicosis, a condition that could be avoidable with appropriate ambulatory care in some regions of the United States.
It is well known that chronic conditions such as diabetes mellitus, coronary artery disease, stroke, and emphysema follow a rising prevalence in patients with lower income and a lack of insurance coverage (13,14). In the United States, these patients are less likely to have regular office visits to a health professional compared to those with a higher income (13). Lack of access to outpatient care results in more medical crises and emergency hospitalization, and ultimately this increases the inefficient use of medical services, resulting in higher rates of hospital admissions for conditions that could typically be managed in the ambulatory setting and a substantially higher cost per case than privately insured patients (15). In the current data set, close to 70% of cases of thyroid storm were either precipitated by medication noncompliance or were patients with a new diagnosis of thyrotoxicosis upon presentation to the emergency department, and 80% of this subset of patients had no healthcare insurance or Medicare coverage. It is likely that a considerable number of admissions within this subset of patients could have been avoided with improved access to healthcare. If this had been the case, the rates of thyroid storm would be <10%, closer to the rates of thyroid storm previously described for the United States (1).
Interestingly, Hispanic/Latinos were found to have lower odds for hospitalization for complicated thyrotoxicosis. This finding was unexpected because in the United States, Hispanics are a disadvantageous ethnic group in regards to education, socioeconomic status, and quality of medical care (14). These findings cannot be explained by an underrepresentation of Hispanic/Latinos in the cohort because the percentage of this group in the sample was similar to that of the population of the city of Lubbock, as reported by the Census Bureau in 2010 (38% vs. 32.1%, respectively). Previous studies have suggested that there are racial/ethnic differences in the prevalence of thyrotoxicosis and Graves' disease, potentially resulting from genetic and environmental exposure differences (16,17). Similarly, differences in the susceptibility for complicated thyrotoxicosis among ethnic groups could potentially explain the association between Hispanic ethnicity and the lower admission rate for complicated thyrotoxicosis, a matter that would need to be studied further.
Other institutions with a patient population similar to that in this study have also reported findings that suggest an association between unfavorable socioeconomic factors and poor outcomes of thyrotoxic patients (18, 9). A study conducted in Los Angeles County—University of Southern California Medical Center (LAC-USC) reported hospitalization rates for complicated thyrotoxicosis of 0.088% of total hospital admissions (18), which is similar to the present study. Both hospitals, UMC and LAC-USC, are university, safety net, public tertiary-care hospitals that serve a high percentage of a population that lacks access to routine medical care. When compared to recently published data from a nationwide survey from Japan, a country with a universal healthcare insurance system, the rate of hospitalization for thyrotoxicosis was five times higher in the authors' institution (2). Furthermore, the rate of thyroid storm was twice as high in the present group of hospitalized patients for thyrotoxicosis as in the group hospitalized in LAC-USC (32% UMC vs. 16.6% LAC-USC), but six times higher than those described in the Japanese population (2).
Similarly, a study conducted at a county-subsidized hospital that has a high percentage of patient population with either no insurance or Medicaid compared patients who underwent thyroidectomy as their initial treatment for Graves' disease to those treated medically. Of the patients treated surgically, 94% were either uninsured or had Medicaid insurance compared to 56% of those treated medically (19), suggesting that socioeconomic factors may play a role in therapy offered to or chosen by patients and providers, likely because clinicians have already recognized that disadvantageous socioeconomic factors are a risk factor for poor outcomes in thyrotoxic patients. Surgery, which results in a fast resolution of symptoms without the need for frequent clinic visits and laboratory testing, might be viewed as a more suitable and effective treatment option for patients with limited access to medical care.
Limitations to this study are acknowledged. The fact that the control group was composed of patients seen in a specialty clinic could have skewed the data, as patients of lower socioeconomic status have limited access to specialty care. Additionally, no data on admissions for thyrotoxicosis are available at second- or third-level hospitals in the area, and as the university hospital is a referral center, it could be seeing higher rates of more severe cases of thyrotoxicosis and missing those milder cases.
Conclusion
The results suggest that in the United States, unfavorable socioeconomic conditions are associated with an increased odd of life-threatening complications of thyrotoxicosis, requiring hospital admission that could potentially be avoided with a timely ambulatory care consultation. Access to healthcare and education are factors that should be targeted as attempts are made to improve the population health and decrease healthcare costs. As unfavorable socioeconomic conditions are recognized as a risk factor for poor outcomes for thyrotoxic patients, the effectiveness and success of different treatment modalities available for thyrotoxicosis should be reevaluated accounting for socioeconomic factors in order to allow better treatment decisions to be made for these patients.
Footnotes
Acknowledgments
Abstract presented as a poster at the 2018 American Thyroid Association Meeting in Washington, DC.
Author Disclosure Statement
None of the authors have conflicts of interest to disclose, and we all have adhered to the ethics guidelines.
Appendix
Clinical Data of Outpatient and Hospitalized Thyrotoxic Groups
| Parameter | Outpatient | Hospitalized |
|---|---|---|
| Weight, kg * | 79.4 (20) | 73.9 (19) |
| BMI, kg/m2 ** | 29.1 (6.6) | 26.5 (5.4) |
| Heart rate, bpm ** | 87.3 (17.6) | 124 (24.4) |
| Hemoglobin, g/dL * | 13.8 (1.6) | 12.9 (2.1) |
| WBC count, k/IUL | 7.3 (3.2) | 8.1 (3.9) |
| Platelet count, k/IUL ** | 245.5 (92.1) | 209.6 (70.5) |
| AST, IU/L | 28.1 (19.8) | 30.5 (20) |
| ALT, IU/L | 39.9 (65.4) | 32.4 (26.8) |
| Total bilirubin, mg/dL * | 0.5 (0.3) | 0.8 (0.8) |
| GFR, mL/min/1.73 m2 | 141.1 (54.3) | 162 (76.7) |
| Corrected calcium, mg/dL | 9.6 (0.6) | 9.7 (0.7) |
| TSH, mIU/L | 0 (0) | 0 (0) |
| fT4, ng/dL ** | 3.3 (2.5) | 5.5 (2.5) |
| fT3, pg/mL ** | 9.8 (7.5) | 16.5 (8.5) |
| fT4/fT3 | 0.4 (0.7) | 0.4 (0.1) |
| Positive TSI, n (%) | 175 (83.3) | 58 (86.6) |
| TSI level, when positive ** | 324.7 (110.9) | 387.3 (107.4) |
| Thyroid gland size (g), median (IQR) ** | 20.5 (14.3–32.9) | 32.7 (19.1–55.2) |
All data are the mean (standard deviation) unless otherwise specified.
p < 0.01; ** p < 0.001.
SD, standard deviation; BMI, body mass index; WBC, white blood cells; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GFR, glomerular filtration rate; TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine; TSI, thyroid stimulating immunoglobulin; IQR, interquartile range.