
Abstract
Background:
The concept of a dynamic risk-stratification scheme has been suggested for individualized management of patients with papillary thyroid carcinoma (PTC). However, there is no specified follow-up strategy for patients with an indeterminate response.
Methods:
This study evaluated 403 PTC patients who had an indeterminate response during the first 12–24 months after initial therapy. All patients underwent total thyroidectomy with radioactive iodine remnant ablation. Patients were further classified into three groups based on risk of structural persistence/recurrence: a Tg+ group (detectable thyroglobulin [Tg], regardless of antithyroglobulin antibody [TgAb] or imaging findings; 196 patients), a TgAb+ group (positive results for TgAb with undetectable Tg, regardless of imaging findings; 46 patients), and an Image+ group (nonspecific findings on neck ultrasonography or faint uptake in the thyroid bed on whole-body scan, with undetectable Tg and negative results for TgAb; 161 patients).
Results:
With a median of 9.6 years (interquartile range 7.7–11.2 years) of follow-up, 56 (14%) PTC patients had structural persistent/recurrent disease: 50 (89%) at locoregional sites and six (11%) at distant sites. The recurrence rate in Tg+, TgAb+, and Image + groups were 26.5%, 8.7%, and 0%, respectively. The median time to detection of structural persistent/recurrent disease from the initial thyroid surgery was 3.7 years (interquartile range 2.5–6.3 years). The optimal cutoff stimulated Tg level to predict structural persistent/recurrent disease was 3.1 ng/mL in the Tg+ group. This classification system revealed higher predictability of structural persistent/recurrent disease than the tumor-node-metastasis staging system and American Thyroid Association risk stratification (proportion of variation explained: 15.7% vs. 2.4% and 0.9%, respectively). Six (3%) patients with distant metastatic disease were all classified in the Tg+ group, and all had lung metastasis.
Conclusions:
The findings suggest a more individualized follow-up strategy for patients with an indeterminate response. More careful evaluation, including early evaluation of distant metastasis, is necessary in patients with elevated Tg levels. However, for patients testing positive for TgAb or those with only nonspecific imaging findings, regular follow-ups of Tg and TgAb levels and neck ultrasonography are sufficient.
Introduction
I
An indeterminate response is defined as biochemical or structural findings that cannot be classified as either benign or malignant, and it is based on three clinical findings: serum thyroglobulin (Tg) levels, antithyroglobulin antibody (TgAb) levels, and imaging findings such as neck ultrasonography (US) or diagnostic whole-body scan (DxWBS) (4). The clinical outcome of patients with an indeterminate response is reported to be intermediate, between incomplete and excellent responses, and the structural persistence/recurrence rate in these patients is around 13–20% (7,8). The ATA guidelines recommend continued observation with appropriate serial imaging and serum Tg monitoring for patients with an indeterminate response (4). However, this management recommendation is vague and not specific.
This study evaluated the clinical outcome of patients with an indeterminate response, and further classified them into three groups according to serum Tg and TgAb levels and imaging findings. The aim was to propose more specific follow-up protocols in patients with an indeterminate response according to Tg, TgAb levels, and imaging findings.
Methods
Study participants
The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea (2018-0656). This retrospective cohort study evaluated 2356 DTC patients who underwent total thyroidectomy (TT) with radioactive iodine (RAI) remnant ablation between 2003 and 2007 at the Asan Medical Center. Patients without adequate follow-up data to determine DRS (n = 311) and those with distant metastasis at diagnosis (n = 21) were excluded from the study. The initial response to therapy in each patient was assessed. A total of 404 patients had an indeterminate response to initial therapy according to criteria from previous studies (7,8). A total of 403 patients with papillary thyroid carcinoma (PTC) were analyzed in the present study after excluding one patient with follicular carcinoma.
Follow-up protocol after initial therapy
Study participants underwent TT with/without prophylactic central neck or therapeutic central neck and lateral neck dissection (9). All patients underwent subsequent RAI remnant ablation according to the protocol established by the Department of Endocrinology and Metabolism of the Asan Medical Center (10). After initial therapy, all patients took levothyroxine for thyrotropin suppression and were regularly followed as previously reported (8,11). During the first 12–24 months after initial therapy, neck US and/or DxWBS were performed with measurement of stimulated thyroglobulin (sTg) and TgAb, and the response to initial therapy was assessed. Patients with an indeterminate response remained under continued observation with appropriate serial imaging of nonspecific lesions and serum Tg monitoring every 6–24 months (4). If nonspecific findings became suspicious over time, further evaluation with additional imaging or biopsy was performed (4). Additional diagnostic imaging studies, such as computed tomography (CT), magnetic resonance imaging, or whole-body fluorodeoxyglucose positron emission tomography/CT scan, were also performed in some patients as needed (8).
Definitions
Patients were classified according to the eighth edition of the American Joint Committee on Cancer/Union for International Cancer Control tumor-node-metastasis (TNM) staging system and ATA risk-stratification system (low, intermediate, and high risk of recurrence) (4,12). An indeterminate response was defined as follows: (i) nonspecific findings on neck US or faint uptake in the thyroid bed on DxWBS, (ii) sTg detectable but <10 ng/mL, or (iii) positive results for TgAb but with the levels remaining stable or declining during the first 12–24 months after initial therapy (4). Detectable Tg was defined as sTg ≥1 ng/mL, and a positive result for TgAb was defined as TgAb >60 IU/mL (4,8). Nonspecific imaging findings were defined as lesions that are difficult to distinguish between recurrent thyroid cancer and nonrecurrent benign lesions with neck US or faint uptake in the thyroid bed on DxWBS (4,13,14).
The primary outcome of this study was the development of structural persistent/recurrent disease, which was defined as pathologically or cytologically proven metastatic lesions and/or metastatic lesions in other distant organs using imaging studies, with biochemical evidence during follow-up (7,8).
Statistical analysis
R v3.4.0 was used to perform statistical analysis (R Foundation for Statistical Computing;
Results
Baseline characteristics of PTC patients with an indeterminate response to initial therapy
The baseline characteristics of the 403 PTC patients who showed an indeterminate response to initial therapy are shown in Table 1. The mean age of patients was 48.0 ± 11.8 years, and 300 patients (74.4%) were <55 years of age. Among all patients, 82.4% were female. The mean primary tumor size was 1.4 ± 1.1 cm, and 51.1% of tumors were >1 cm. Cervical lymph node (LN) metastasis was found in 234 (58.1%) patients. According to the TNM staging system, 158 (39.2%), 234 (58.1%), and 11 (2.7%) patients were classified as having stage I, II, and III disease, respectively. With the ATA risk-stratification system, 86 (21.3%), 271 (67.2%), and 46 (11.4%) patients were classified as having low, intermediate, and high risk, respectively.
Baseline Characteristics of Patients with PTC who have an Indeterminate Response to Initial Therapy
Continuous variables are presented as mean (standard deviation). Categorical variables are presented as number (percentage).
PTC, papillary thyroid carcinoma; T, tumor; N, node; M, metastasis; TNM, tumor, node, metastasis; ATA, American Thyroid Association.
Characteristics of structural persistent/recurrent disease in patients with an indeterminate response
With a median of 9.6 years (IQR 7.7–11.2 years) of follow-up after initial thyroid surgery, structural persistent/recurrent disease was detected in 56 (13.9%) patients. The median time to detection of structural persistent/recurrent disease from the initial thyroid surgery was 3.7 years (IQR 2.5–6.3 years). Among 56 patients with structural persistent/recurrent disease, 13 (23.2%) had structural persistent/recurrent disease in the central neck/operation bed, 37 (66.1%) in a lateral neck lesion, and six (10.7%) at distant sites. The rates of structural persistent/recurrent disease were significantly different according to the TNM staging (8.2% with stage I, 16.7% with stage II, and 36.4% with stage III; p = 0.006) and ATA risk-stratification systems (4.7% with low risk, 17.0% with intermediate risk, and 13.0% with high risk, p = 0.016; Table 2).
Number of Patients with Structural Persistent/Recurrent PTC According to TNM Staging, ATA Risk, Tg, TgAb, and Imaging Findings
Categorical variables are presented as number (percentage).
1 ng/mL ≤ sTg <10 ng/mL, regardless of TgAb level or imaging findings.
Positive antithyroglobulin antibody with undetectable thyroglobulin, regardless of imaging findings.
Nonspecific findings on neck ultrasonography or faint uptake in the thyroid bed on diagnostic whole-body scanning with undetectable stimulated Tg and negative TgAb.
Tg, thyroglobulin; TgAb, antithyroglobulin antibody; NED, no evidence of disease.
The rate of structural persistent/recurrent disease according to sTg, TgAb, and imaging findings was evaluated (Supplementary Table S1). Structural persistent/recurrent disease was found in 23% and 11% of patients in the groups with detectable sTg alone and positive results for TgAb alone, respectively. No patients with nonspecific imaging findings alone developed structural persistent/recurrent disease during follow-up. However, 35% of patients with nonspecific imaging findings and detectable sTg had structural persistent/recurrent disease. One patient with all three features also had structural persistent/recurrent disease.
Supplementary Table S2 shows structural persistent/recurrent disease according to a combination of TNM staging with sTg, TgAb, and imaging status. Even in patients with stage I disease, the rate of structural persistent/recurrent disease was high in patients with detectable Tg (23.1%), similar to that in patients with stage II/III disease and detectable Tg (27.8%). However, the rate of structural persistent/recurrent disease was low in patients with positive results for TgAb, irrespective of the initial TNM stages (6.3% in patients with stage I and 10% in patients with stage II/III disease).
Subclassification of patients with an indeterminate response
Based on the previous findings, patients were further classified into three groups according to the TNM staging system, sTg, TgAb, and imaging findings at 12–24 months after surgery in order to specify the indeterminate group according to recurrence. The three groups were as follows: the Tg+ group (1 ng/mL ≤ sTg <10 ng/mL, regardless of TgAb level or imaging findings; 196 patients), TgAb+ group (positive results for TgAb with undetectable Tg, regardless of imaging findings; 46 patients), and the Image+ group (nonspecific findings on neck US or faint uptake in the thyroid bed on DxWBS, with undetectable sTg and negative results for TgAb; 161 patients). Figure 1 shows the distribution of TNM stages (stages I, II, and III) and ATA risk-stratification categories (low, intermediate, and high risk) for each group. The distribution of TNM stage and ATA risk was significantly different among the three groups (p = 0.001 and p < 0.001, respectively). The proportion of stage I disease or low-risk patients was the smallest in the Tg+ group (12.8% and 26.5%, respectively), and it was largest in the Image+ group (30.4% and 55.9%, respectively).

Distribution of tumor-node-metastasis (TNM) staging (stages I, II, and III) according to (
In the Tg+ group, structural persistent/recurrent disease was detected in 52 patients (26.5%; Table 2). The mean sTg level was 3.3 ± 2.3 ng/mL and the optimal cutoff sTg level to predict structural persistent/recurrent disease was 3.1 ng/mL using ROC curve analysis (AUC = 0.705 [CI 0.621–0.789]). However, the rate of structural persistent/recurrent disease was significantly lower in the TgAb+ and Image+ groups. Only four (8.7%) patients in the TgAb+ group had structural persistent/recurrent disease during a median of 11 years (IQR 9–13 years) of follow-up, and no patients in the Image+ group had structural persistent/recurrent disease during a median of 10 years (IQR 8–12 years) of follow-up.
DFS rates in patients with an indeterminate response were analyzed in each group (Fig. 2). The 10-year DFS rates of patients in the Tg+, TgAb+, and Image+ groups were 68.9%, 90.3%, and 100%, respectively. There was a significant difference in DFS among the different groups of patients (p < 0.001). The subclassification system yielded a better recurrence prediction, with a PVE of 15.7%, compared to the TNM staging (PVE 2.4%) and ATA risk-stratification (PVE 0.9%) systems.
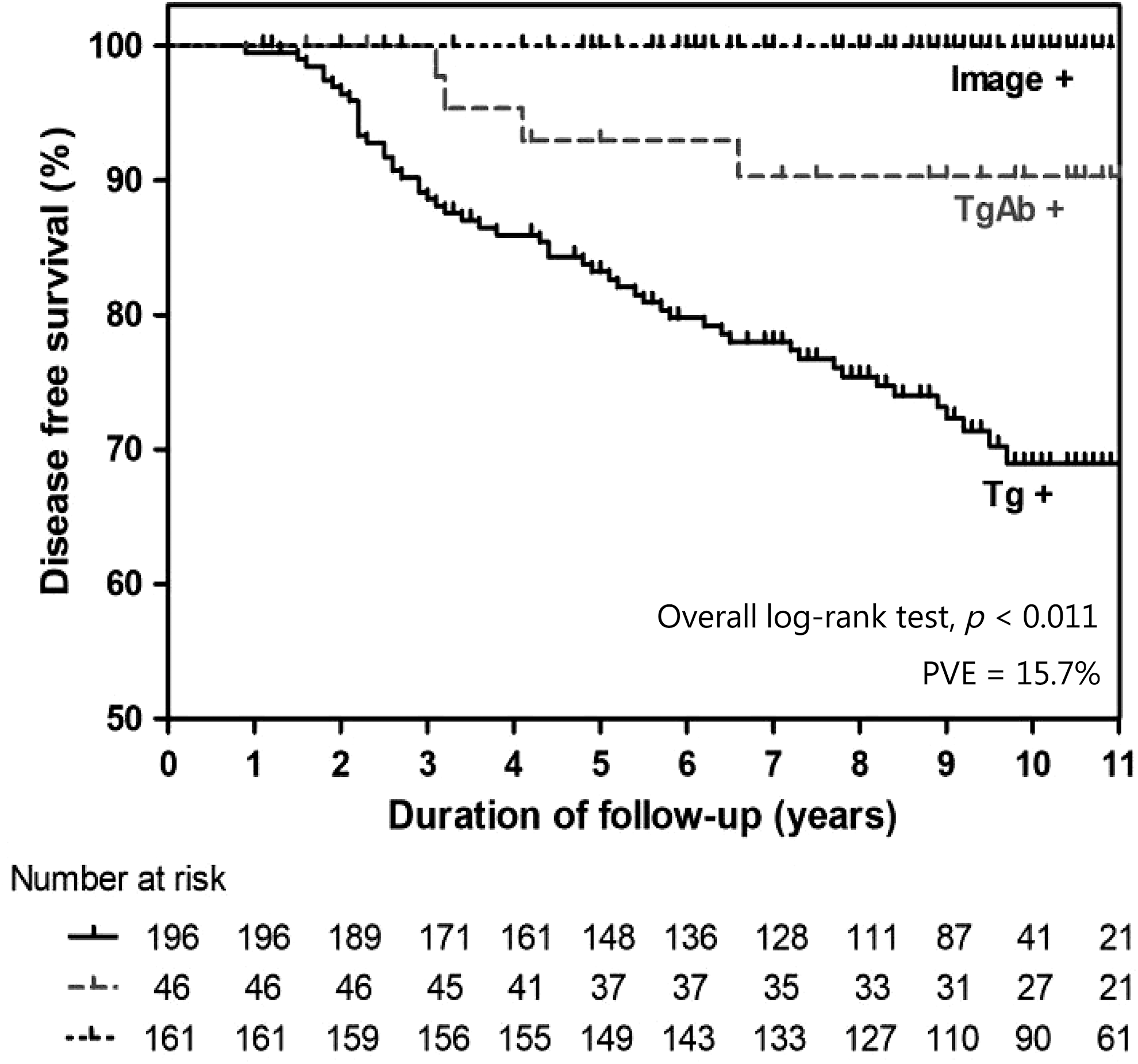
Disease-free survival rates in patients with papillary thyroid carcinoma who have indeterminate response according to stimulated thyroglobulin (sTg), antithyroglobulin antibody (TgAb), and imaging findings: Tg+ group (1 ng/mL ≤ sTg <10 ng/mL, regardless of TgAb level or imaging findings); TgAb+ group (positive TgAb with undetectable sTg, regardless of imaging findings), and Image+ group (nonspecific findings on neck ultrasonography or faint uptake in the thyroid bed on diagnostic whole-body scan, with undetectable sTg and negative TgAb). PVE, proportion of variation explained.
Clinicopathologic features of patients with distant metastasis
During follow-up, six (1.5%) patients were found to have distant metastasis. The detailed clinicopathologic features of these patients are presented in Table 3. All six patients had lung metastasis and were categorized in the Tg+ group according to the new subclassification. Patients 1, 2, 3, 5, and 6 had relatively high sTg levels (>3.1 ng/mL) at the time of initial response evaluation, and patient 4 had a sTg of 1.3 ng/mL with a positive result for TgAb. Patients 1, 2, 3, and 5 had elevated sTg levels, and a chest CT revealed multiple lung nodules consistent with lung metastasis from thyroid cancer. Patient 6 had distant metastasis to the lung and brain. In patient 4, sTg and TgAb levels were stable, but metastatic LNs were detected on neck US and fine-needle aspiration (FNA) cytology. The patient underwent reoperation and RAI therapy; lung metastasis was found on post-RAI scan images.
F, female; M, male; TT c MRND, total thyroidectomy with modified radical neck dissection; I risk, intermediate risk; H risk, high risk; sTg, stimulated thyroglobulin; LN, lymph node; Reop, reoperation; RAI, radioactive iodine; RFA, radiofrequency ablation; RT, radiotherapy; GKS, gamma knife surgery; TKI, tyrosine kinase inhibitor.
Discussion
The present study evaluated the clinical outcome of PTC patients with an indeterminate response in the first 12–24 months after initial therapy including remnant RAI ablation. Structural persistent/recurrent disease was detected in 14% of patients with an indeterminate response during a median of 3.7 years (IQR 2.5–6.3 years) from initial therapy. When patients were classified into groups based on sTg, TgAb, and imaging findings, structural persistent/recurrent disease was most commonly found in the Tg+ group (26.5%). Only 8.7% of patients in the TgAb+ group and none in the Image+ group had structural persistent/recurrent disease. This indicates that a more individualized follow-up strategy is needed in the management of patients with an indeterminate response. To use the group definitions, more frequent and strict assessment of Tg, TgAb, and imaging is necessary for patients with Tg+ group and a more generous follow-up strategy can be adopted for those with TgAb+ and Image+ group patients.
A previous study reported that DRS predicted structural persistent/recurrent disease better than ATA risk stratification or the TNM staging system, with reported PVE rates for ATA risk stratification, TNM staging, and DRS of 12.1%, 8.7%, and 44.6%, respectively (8). Interestingly, the current subclassification system predicted recurrence better than ATA risk and TNM staging in patients with PTC who had an indeterminate response. These findings strongly support that individualized management can be carried out in patients with an indeterminate response according to their Tg, TgAb, and image status.
An elevated postoperative serum Tg level is associated with poor clinical outcome of DTC and is considered an independent predictor of persistent and recurrent disease (17 –21). Previous studies have reported that high sTg values (>10 ng/mL) are associated with poor clinical outcomes, and low sTg values (<1–2 ng/mL) are associated with remission (17 –20). With this background, sTg values of 1–10 ng/mL are classified as an indeterminate response (4,7). In this study, structural persistent/recurrent disease was frequently detected in patients with detectable sTg, and the rate of structural recurrent/persistent disease was not significantly different from biochemical incomplete response (7,8,22). The cutoff sTg level to predict the structural persistent/recurrent disease was 3.1 ng/mL. Furthermore, six patients had metastasis at distant sites. This indicates that stricter and more frequent evaluation of Tg, TgAb, and neck US might be necessary in patients with elevated sTg levels, especially those with sTg >3.1 ng/mL on the initial DRS evaluation after thyroid surgery. Early metastasis workup such as chest CT is needed for these patients when suspected.
TgAb are produced in 10–25% of DTC patients after TT and interfere with Tg measurement (23,24). Previous studies have suggested that trends of increasing or decreasing TgAb are associated with the recurrence of disease in TgAb+ DTC patients (24 –26). In this study, about 10% of patients (4 patients) in the TgAb+ group, having positive results for TgAb with stable or declining levels and undetectable Tg and negative imaging findings during the first 12–24 months after initial therapy, were expected to have structural persistent/recurrent disease, which occurred three to six years after thyroid surgery. This is consistent with previous reports that approximately 8% of patients with decreasing TgAb and undetectable Tg had recurrence of disease (24).
In this study, no patients in the Image+ group had structural persistent/recurrent disease during follow-up. Among the 88 (54.3%) patients with faint uptake on DxWBS, only 66 (40.8%) patients had nonspecific findings on neck US, and eight (4.9%) patients had nonspecific findings on both DxWBS and neck US. Previous studies have suggested that DxWBS contributes little additional information compared to serum Tg levels or neck US (27 –29). Therefore, recent ATA guidelines have opposed the routine use of DxWBS in low- to intermediate-risk DTC patients who have undetectable Tg and negative neck US findings (4). Neck US is a sensitive way to detect locoregional recurrence of DTC and routine evaluation with neck US after thyroid surgery is recommended in various guidelines (4,5,30,31). However there are many nonspecific structures that mimic disease, such as residual thyroid tissue, thyroid and cricoid cartilage, sympathetic ganglia, surgical material, or chronic granulomatous lesions (13,14,31). Nonspecific lesions can be difficult to distinguish between recurrent thyroid cancer and nonrecurrent benign lesions with neck US alone, especially with undetectable serum Tg levels (13,14). Recent studies have also questioned the use of frequent neck US evaluations from the perspectives of cost-effectiveness and because of concerns for false-positive results (32,33). The present results are consistent with previous reports that neck US evaluation in the absence of biochemical evidence of disease seems to have a low positive predictive value for structural persistent/recurrent disease. Relatively conservative management with watchful observation, perhaps with FNA evaluation with selected lesions, can be performed in patients with nonspecific imaging findings, undetectable Tg, and negative results for TgAb due to their low likelihood of recurrence.
There are some limitations to this study. Due to its retrospective design at a single tertiary referral center, the possibility of selection bias should be considered. About 50% of the DTC in this study were small thyroid carcinomas, <1 cm in size, which are known to have an excellent prognosis (34). However, the recurrence rate of patients with an indeterminate response in this study was not different from that of other reports (7,8). Another limitation is that other types of DTC were not evaluated. More studies on follow-up strategies in diverse patients with DTC who have an indeterminate response are needed. Despite these limitations, this study has important strengths, including the long-term follow-up duration and the relatively large cohort.
In summary, 14% of PTC patients with an indeterminate response on the initial DRS evaluation had structural persistent/recurrent disease. An elevated Tg level, especially a Tg >3.1 ng/mL, was the most important risk factor for structural persistent/recurrent disease and was also associated with distant metastasis. Therefore, more careful evaluation, including early evaluation of distant metastasis, might be necessary in patients with elevated sTg levels. For patients with positive results for TgAb or nonspecific imaging findings only, regular follow-up evaluation of Tg and TgAb levels and neck US are sufficient. The findings suggest that a more individualized follow-up strategy for patients with an indeterminate response is needed based on their Tg levels, TgAb status, and imaging findings.
Footnotes
Acknowledgment
This study was supported by a National Research Foundation (NRF) of Korea Research Grant (NRF-2017R1D1A1B03028231).
Author Disclosure Statement
No competing financial interests exist.