
Abstract
Background:
The recent introduction of noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) in the World Health Organization classification of thyroid tumors has significantly modified the risk of malignancy of cytological diagnoses. In fact, while this tumor was previously classified as a carcinoma (the encapsulated, noninvasive form follicular variant of papillary thyroid carcinoma), it is now considered a neoplasm with low malignant potential. Given that the cytological features of NIFTP are not specific and overlap with other pathologic entities, there is no specific cytological diagnostic category for NIFTP. To obtain more robust information about the cytological findings associated with NIFTP, published articles were systematically reviewed, and a meta-analysis of the data was conducted.
Methods:
The review was conducted according to PRISMA guidelines. A comprehensive literature search of the PubMed/MEDLINE and Scopus databases was conducted using a combination of terms “noninvasive,” “encapsulated,” “follicular variant,” “NIFTP,” and “thyroid cancer.” The search was updated to June 2018, and references of the retrieved articles were also screened. Only original articles reporting the classification of histologically proven NIFTPs with cytological findings according to The Bethesda System for Reporting Thyroid Cytopathology were eligible for inclusion.
Results:
The literature search revealed 117 articles, of which 15 were included in the study. All studies were retrospective. A total of 915 NIFTP cases were retrieved. The incidence of cases cytologically classified according to the Bethesda system was as follows: non-diagnostic 3%, benign 10%, atypia of undetermined significance or follicular lesion of undetermined significance 30%, follicular neoplasm or suspicious for a follicular neoplasm 21%, suspicious for malignancy 24%, and malignant 8%. Mild heterogeneity between the studies was found. Publication bias was absent.
Conclusions:
This meta-analysis shows that the cytological diagnoses associated with NIFTP by fine-needle aspiration cytology includes a wide spectrum of findings. The majority of cases are cytologically indeterminate, and the remainder may be read as non-diagnostic, benign, or malignant. In order to develop an accurate presurgical diagnosis of these cases, further cytological and/or molecular characteristics need to be identified.
Introduction
T
Methods
Conduct of review
This present systematic review was conducted according to PRISMA guidelines (see Supplementary Table S1).
Search strategy
A comprehensive literature search was conducted using the online databases of Pubmed/MEDLINE and Scopus by searching papers reporting NIFTP cases using a combination of the terms “noninvasive,” “encapsulated,” “follicular variant,” “NIFTP,” and “thyroid cancer” in order to find articles with data on the classification of fine-needle aspiration cytology (FNAC) samples as NIFTP, according to TBSRTC. This allowed a large number of studies that reported histologically proven NIFTP and which contained information on the presurgical cytological specimens to be identified. A beginning date limit was not used. The search was updated up until June 8, 2018, and no language restrictions were used. To try to expand the search, references of the retrieved articles were also screened to identify additional studies.
Study selection
Only original articles reporting NIFTP cases with a histological assessment and a classification of their FNAC samples were initially considered as eligible for inclusion. The main exclusion criteria were articles with overlapping patient or nodule data and case reports. In addition, papers reporting only some TBSRTC categories were excluded because these results did not allow the distribution of NIFTP among the six categories of TBSRTC to be known and the incidence of each cytological class to be calculated. Two researchers (M.B. and P.T.) independently reviewed titles and abstracts of the retrieved articles, applying the selection criteria. Then, all authors independently reviewed the full text of the remaining articles to determine their final inclusion.
Data extraction
For each included study, the following information was extracted independently by two investigators (M.B. and P.T.) in a piloted form: (i) study data (authors, year of publication, and country of origin), (ii) number of cases of NIFTP evaluated, and (iii) distribution of NIFTP within TBSRTC categories. Data were cross-checked, and any discrepancies were discussed and mutually solved.
Study quality assessment
The risk of bias of the included studies was assessed independently by two reviewers (M.B. and P.T.) through the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool for the following aspects: patient selection, index test, reference standard, flow, and timing. Risk of bias and concerns about applicability were rated as low, high, and unclear risk.
Statistical analysis
A proportion meta-analysis calculation was used to obtain the pooled rate of NIFTP assessed in TBSRTC categories. For statistical pooling of data, the DerSimonian and Laird method (random-effects model) was used (7). In this model, pooled data represent weighted averages related to the sample sizes of studies. Pooled data were presented with confidence intervals (CI) and displayed using a forest plot. The I 2 index was used to quantify the heterogeneity among the studies, and significant heterogeneity was defined as an I 2 >50%. Egger's test was carried out to evaluate the possible presence of a significant publication bias. Statistical analyses were performed using StatsDirect (StatsDirect Ltd., Altrincham, United Kingdom).
Results
Eligible articles
The comprehensive literature search identified 117 articles. An initial review of the titles and abstracts excluded 98 articles. A further four articles were excluded because they only reported NIFTP cases that were either FN/SFN or SM on FNAC (8,9) or did not include the whole spectrum of the Bethesda system categories (6,10). Hence, it was not possible to calculate the rate of NIFTP within the overall diagnostic categories of FNAC. In the end, 15 articles (4,5,11 –23) were included in the study (see Supplementary Fig. S1).
Qualitative analysis (systematic review)
Included studies were published by authors from the United States, Canada, Europe, and Asia. The majority of these studies reported series of histologically proven NIFTP in which the cytological diagnoses were retrospectively reviewed for the publication. Other studies reported NIFTP nodules in which the possibility of a NIFTP lesion had been suggested on cytological evaluation and was then confirmed on histopathology. Only two papers used liquid-based cytology. Data on the cytological assessments could be clearly identified in all these manuscripts, and the true percentage of each FNAC category was calculated. Table 1 details the main publication characteristics and findings of the included studies. A quality assessment of the studies is reported in Table 2.
Main Characteristics of the Included Studies
All data refer to NIFTP with a proven histological diagnosis. All studies reported conventional cytological examinations of smears except two studies (5,15), which used liquid-based cytology.
FNAC, fine-needle aspiration cytology; NIFTP, noninvasive follicular thyroid neoplasms with papillary-like nuclear features.
Quality Assessment of the Studies According to QUADAS-2
QUADAS-2, Quality Assessment of Diagnostic Accuracy Studies; L, low risk of bias; H, high risk of bias; U, unclear risk of bias.
Quantitative analysis (meta-analysis)
Overall, the included articles reported 915 histologically proven NIFTP lesions for which a preoperative FNAC was available. The pooled rate of each FNA category is shown in Figure 1 and details of the results are reported in Table 3. In all Bethesda categories, there was mild heterogeneity between the studies, while publication bias was always absent. The most prevalent cytological category was AUS/FLUS (30%). Because the large majority of cases were classified as Bethesda III, IV, or V, these three classes were considered for sub-analysis. The pooled rate of NIFTP with a presurgical cytology diagnosis in class III–IV was 52% [CI 42–62], with heterogeneity (I 2 88% [CI 82–91] and without publication bias (p = 0.32). The pooled rate of NIFTP with a cytology diagnosis in III–IV–V was 78% [CI 71–84] with heterogeneity (I 2 80% [CI 66–86] and no publication bias (p = 0.21). Subsequently, to resolve the heterogeneity between the studies, the pooled results from those studies with a larger series of NIFTP were analyzed. There were seven studies with ≥50 cases reporting 729 NIFTP (4,5,13,16,18,22,23), and these articles were chosen for this sub-analysis. The pooled results were quite similar to those summarized above: non-diagnostic FNAC 4%, benign 13%, AUS/FLUS 27%, FN/SFN 24%, SM 22%, and M 9%. There was mild heterogeneity in all these results. However, publication bias was only present in non-diagnostic FNAC. In addition, the pooled prevalence of FNAC classified as III–IV was 51%, and the pooled prevalence of cases classified as III–IV–V was 74%.
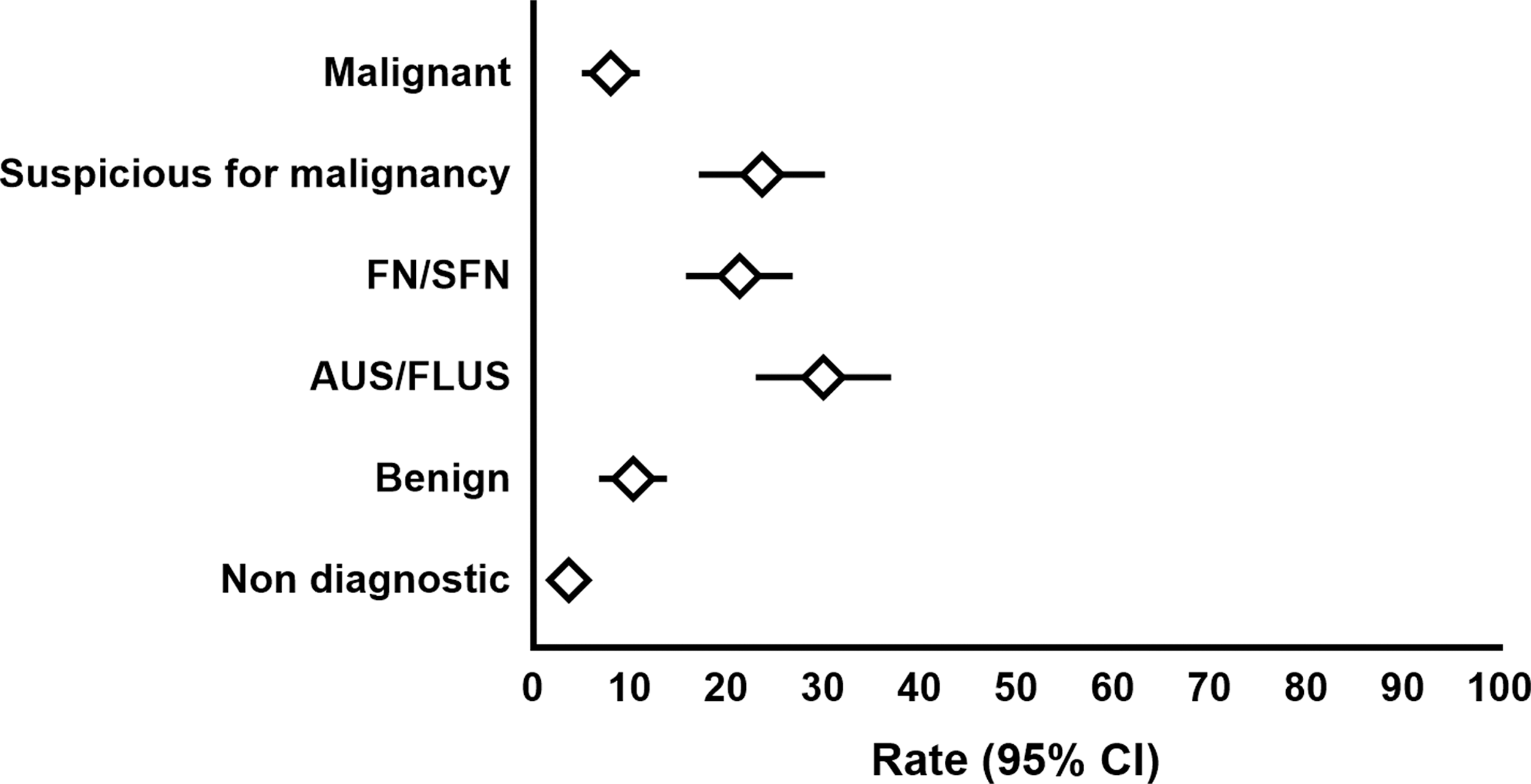
Forest plot of the pooled rate (confidence interval) of noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) in the six diagnostic categories of the Bethesda system (random effect).
Proportion of NIFTP in the Cytological Classes of the Bethesda System
Absence of heterogeneity was set at I 2 < 50%. Publication bias was analyzed using the Egger test. A significant test identified the presence of publication bias.
CI, confidence interval; AUS/FLUS, atypia of undetermined significance or follicular lesion of undetermined significance; FN/SFN follicular neoplasm or suspicious for a follicular neoplasm; SM, suspicious for malignancy; M, malignant.
Discussion
NIFTP is a recently described entity among thyroid tumors (3), which is considered to have an indolent behavior. Therefore, these cases are considered similar to low malignant potential lesions that need a simple lobectomy (without subsequent radioiodine therapy) and then clinical follow-up (3). Alternatively, performing a total thyroidectomy is also a consideration (24). Thus, detecting these tumors before surgery would have a significant impact for the management of patients in clinical practice. To date, while FNAC diagnosis is pivotal in identifying benign and malignant thyroid nodules, it does not have the ability to predict a NIFTP lesion confidentially. Several examples of retrospective data have been reported, but there is no clear evidence that there is a way to predict the presence of a NIFTP cytologically (25). The present study was specifically undertaken to provide more robust information on the cytological TBSRTC categories associated with NIFTP in the currently available literature (references in Table 1). Fifteen relevant studies were retrieved, and 915 cases of NIFTP were described in these papers. The most important result was that using FNAC, three in four NIFTP were read as AUS/FLUS or FN/SFN (Fig. 2) or SM; only 8% were classified as malignant, and a non-negligible number of cases were cytologically benign (10%) or not adequate for diagnosis (3%). These findings were confirmed when meta-analysis was performed only on those papers with a larger series of cases.

Cytohistological correlation in a case of NIFTP in a 35-year-old female with a 2.2 cm nodule evaluated by ultrasound-guided fine-needle aspiration. (
First and foremost, the introduction of the NIFTP concept has perturbed the cytopathology community. The low malignant potential of resected encapsulated NI-EFVPTC has been known for years. The change in name (with the disappearance of the term “carcinoma”) and the downgrading of this entity to a low potential malignant lesion that requires simple lobectomy have prompted cytopathologists to investigate whether this tumor might be detected in FNAC samples in order to guide the subsequent surgical treatment and tailor the management of patients. In this study, a significant proportion of NIFTP were classified as cytologically indeterminate into the AUS/FLUS DC. AUS/FLUS DC is a problematic and heterogeneous category, comprising cases that present diagnostic difficulties due to poorly preserved, poorly fixed, or poorly stained specimens (26) or comprising paucicellular specimens with mild atypia, either architectural (microfollicular structures) or cytological (nuclear atypia), that are qualitatively and quantitatively insufficient to place the FNAC into either the FN/SFN DC or the SM or M diagnostic categories (26). The incidence of cases placed into the AUS/FLUS category should not be superior to 10% according to the new version of TBSRTC in order to maintain a high diagnostic accuracy of thyroid FNAC. However, as shown by this study in which NIFTP lesions were found to be most commonly associated with AUS/FLUS diagnoses, it is assumed that there may be an increase in AUS/FLUS cases in the future, which may be higher than the recommended 10% (1). Moreover, since NIFTP is ultimately a histological diagnosis and hence a surgical disease, limited surgery (lobectomy) is recommended for these cases to confirm the cytological suspicion. In the United States, presurgical triage can also be done by carrying out molecular tests for indeterminate FNA results, thus refining the role of cytology. However, the fact that the majority of NIFTP cases in the meta-analysis (30%) were placed into the AUS/FLUS DC reflects the diagnostic difficulties related to NIFTP. Since atypical nuclear changes in NIFTP are subtle (beyond that of a benign aspirate but insufficient to warrant a SM diagnosis), most cases fall in this category, as suggested also by Strickland et al. (1,2,8). In addition, according to the present study, a non-negligible number of NIFTP were cytologically classified as benign (10%). Unfortunately, it is not known if the benign diagnoses were due to the cytopathologist missing slight nuclear atypia or if they were not missed but considered to be of reactive nature, or if there was a problem related to the sampling (i.e., normal thyroid instead of the lesion). Since NIFTP are lesions of low malignant potential, these missed diagnoses would probably not have any impact on the quality of life of these patients, but a long follow-up is needed to confirm this assumption. Eight percent of all reported NIFTP cases were diagnosed as malignant. Considering that the 2015 American Thyroid Association guidelines suggest both lobectomy and total thyroidectomy as treatment options for low-risk PTC, there should not be any important medicolegal issues related to this “false-positive” diagnosis (24,25).
Undoubtedly, awareness of the NIFTP and the vast number of articles that have been written concerning the cytopathologic features of the NIFTP suggest that on routine cytology, this entity had an impact on cytopathologists (at least the authors of the present paper) who now pay more attention to subtle nuclear atypias. In the future, as data on prospective evaluations of cytology findings and NIFTP histologies become available, cytopathologists may place less cases into the SM and M categories (reserved only for very suspicious or clear-cut cases of PTC, as suggested by the revised version of TBSRTC), but this will result in an increase in AUS/FLUS diagnoses (1). When dealing with nuclear atypia, cytopathologists have the possibility of a NIFTP in mind, and they would like to avoid a false-positive diagnosis. This perspective change will also affect the manner in which NIFTP will be diagnosed in the future. In the authors' opinion, a diagnosis of “malignant” by cytology will reduce in frequency, as only clear-cut cases of PTC will be cytologically classified (9).
Limitations and strengths of the present review have to be discussed. Almost all studies included in the review were retrospective, and the authors reviewed FNAC samples of NIFTP specifically for the publications. This study design could introduce a bias. It was found that NIFTP may be associated with all cytological categories (I–VI of TBSRTC). Therefore, it must be considered that there is a selection bias in almost all included studies because NIFTP was searched for at histology, and some other cases whose lesion was cytologically classified as non-diagnostic, benign, or indeterminate by FNAC may not have undergone surgery. Consequently, the incidence of NIFTP cytologically classified as Bethesda I–IV might be higher than we found. On the contrary, the percentage of NIFTP read as malignant when using FNAC could be overestimated. As further evidence, this finding was present particularly in those articles with a small sample size.
In conclusion, the present meta-analysis shows that the diagnosis of NIFTP by FNAC remains a significant challenge. In fact, the majority of these cases are cytologically assessed as indeterminate, and the others may be read as non-diagnostic, benign, or malignant. Further cytological investigations are needed in order to develop a tailored management of these cases.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.