
Abstract
Background:
This study aimed to compare the effectiveness and safety of long-term methimazole (MMI) and radioiodine (RAI) in the treatment of toxic multinodular goiter (TMNG).
Methods:
In this randomized, parallel-group trial, 130 consecutive and untreated patients with TMNG, aged <60 years, were enrolled and randomized to either long-term MMI or RAI treatment. Both groups of patients were followed for 60–100 months, with median durations of 72 and 84 months in the MMI and RAI groups, respectively.
Results:
In the MMI and RAI groups, 12 and 11 patients, respectively, were excluded because of side effects, choosing other modes of treatment and not returning for follow-up; 53 and 54 patients, respectively, completed the study for 60–100 months. In the MMI group, two patients (3.8%) experienced subclinical hypothyroidism, and 51 (96.2%) remained euthyroid until the end of study. The dosage of MMI to maintain euthyroidism was 6.3 ± 2.0, 4.5 ± 0.9, and 4.1 ± 1.0 mg daily during the first, third, and fifth years of continuous MMI treatment. One patient had elevated liver enzymes, and three developed skin reactions during the first three months, but no adverse effects from MMI occurred from 4 to 100 months of therapy. In the RAI group, 22 (41%) became hypothyroid, 12 (22%) had persistence or recurrence of hyperthyroidism, and 20 (37%) became euthyroid after 16.7 ± 2.7 mCi 131I.
Conclusion:
Long-term, low-dose MMI treatment for 60–100 months is a safe and effective method for treatment of TMNG, and is not inferior to RAI treatment.
Introduction
Toxic multinodular goiter (TMNG), distinguished from Graves' disease by Plummer in 1928 (1), is defined as a structurally and functionally heterogeneous thyroid enlargement and the presence of autonomously hyperfunctioning thyroid nodules (2). It is a common cause of thyrotoxicosis, especially in areas of iodine deficiency (3).
Autoimmunity does not play a role in the formation of TMNG. Therefore, ablation therapy—both thyroidectomy and radioiodine (RAI) treatment—has been considered as an appropriate treatment for TMNG (4,5). Many physicians prefer RAI therapy (5 –7), and thyroidectomy is performed for large goiters and coexisting thyroid cancer or hyperparathyroidism, or nodules that are resistant to other treatment modalities (8).
Antithyroid drugs are highly effective in the control of hyperthyroidism and are used to achieve euthyroidism before ablation therapy in older patients and in those with cardiovascular disorders (4). Treatment of TMNG with antithyroid medications for more than six months is not recommended because thyrotoxicosis recurs in 95% of patients once treatment is discontinued (9). The 2016 American Thyroid Association guidelines suggest that in the elderly, comorbidities with increased surgical risk or associated with decreased life expectancy, and those who are poor candidates for ablative therapy, antithyroid treatment may be a better option and, occasionally, long-term, low-dose treatment with MMI may be appropriate (5).
A recent meta-analysis showed that long-term antithyroid drug treatment was associated with low rates of complications and higher remission rates than short-term treatment in patients with Graves' disease (10). Data on experiences with long-term antithyroid treatment of TNMG are scarce. However, others have suggested that this treatment modality is not efficacious (11). The objective of this study was to examine the safety and effectiveness of long-term methimazole (MMI) therapy in comparison to RAI treatment of patients with TMNG.
Methods
Trial design and oversight
A randomized, parallel-group trial was conducted between April 2005 and September 2016 in Tehran, an area of iodine sufficiency (12). The research protocol was approved by the ethics committee of the Research Institute of Endocrine Sciences, and informed consent was obtained from all patients.
Untreated patients with TMNG, aged ≤60 years, were recruited and were randomized at a ratio of 1:1 to undergo MMI therapy for at least 60 months or to be treated with RAI. All patients were followed every two to three months in the first year and then every six months for the duration of follow-up.
Patients
Patients with MNG who had a first diagnosis of hyperthyroidism were considered eligible if they had not been treated with antithyroid drugs, RAI, or thyroidectomy. Key inclusion criteria were age ≤60 years, thyrotropin (TSH) <0.4 mIU/L, free thyroxine (fT4) >23 pmol/L, and/or triiodothyronine (T3) >200 ng/dL, and no history or evidence of cardiovascular disease, cirrhosis, or chronic kidney disease. Key exclusion criteria included Graves' disease, pregnancy, breast-feeding, use of amiodarone or iodine, and altered mental function. Eventually, 130 patients with TMNG met the inclusion exclusion and were enrolled in the study. All patients had a MNG on palpation and thyroid scintigraphy, and/or TSH receptor antibodies <1.0 IU/mL.
Procedures
After randomization, information on baseline clinical variables (e.g., age, sex, and smoking behavior) was obtained, and goiter size was documented. At each visit, symptoms of thyroid dysfunction was assessed, thyroid weight (in grams) was estimated by an experienced thyroidologist (F.A.) by palpation, and a complete physical examination, including detection of signs of thyroid dysfunction, was performed. Non-fasting venous blood samples were taken before treatment and again at each visit for determination of serum fT4, T3, and TSH concentrations.
Sixty-five patients received 10–20 mg MMI daily for the first month. The starting dose was selected on the basis of goiter size and severity of hyperthyroidism. The titration method was then used to taper the MMI dose as the patient became euthyroid in order to maintain serum fT4 and TSH concentrations between 10 and 23 pmol/L and 0.4 and 5.06 mIU/L, respectively. Four patients had side effects and changed to other modalities, three chose thyroidectomy, and five were lost to follow-up. The remaining 53 patients were treated for 60–100 months.
Of 65 patients randomized to the RAI group, five chose other treatment modalities and five were lost to follow up (Fig. 1). The remaining 54 patients received RAI according to the following formula:
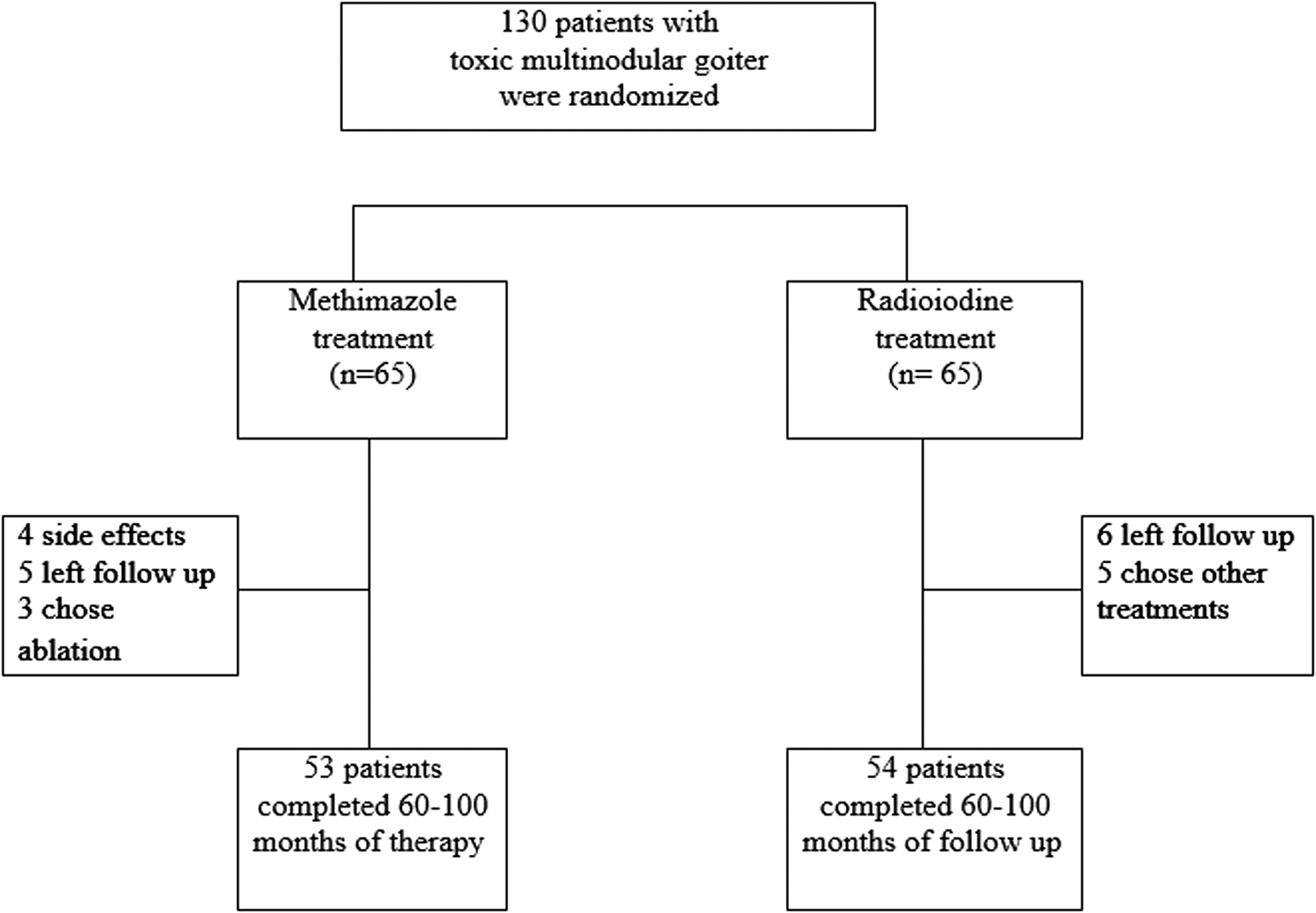
Study enrollment and follow-up of patients with toxic multinodular goiter (TMNG).
In 12 patients from the RAI group with severe thyrotoxicosis, pretreatment with MMI for one to three months was given to deplete thyroid hormone stores. MMI was omitted for five days before and after RAI administration, and stopped entirely 10 weeks after RAI treatment. In both the MMI and RAI groups, beta-blocker medications were administered as needed during the first month of treatment.
Additional treatment
In the RAI group, subclinical hyperthyroidism and subclinical hypothyroidism were not treated. When subclinical hypothyroidism occurred in the MMI group, the dose of MMI was decreased.
Definitions
Hyperthyroidism was considered as TSH <0.4 mIU/L (reference range 0.4–5.06 mIU/L) with fT4 > 23 pmol/L (reference range 9–23 pmol/L) and/or T3 > 200 ng/dL(reference range 75–200 ng/dL), while subclinical hyperthyroidism was defined as TSH <0.4 mIU/L with serum fT4 and T3 within the reference range. Overt hypothyroidism was considered as TSH above the upper limit of normal (i.e., 5.06 mIU/L for the Tehranian population) (13) with fT4 < 9 pmol/L. Subclinical hypothyroidism was defined as TSH >5.06 mIU/L with normal serum fT4 and T3 concentrations.
Study outcomes
The primary outcome was sustained euthyroidism up to eight years of follow-up following either MMI or RAI treatment. Key secondary outcomes were the occurrence of both clinical and subclinical hypo- and hyperthyroidism during long-term MMI or RAI treatment. Safety of long-term MMI therapy was assessed on the basis of adverse events that occurred during treatment. Expected adverse events included agranulocytosis, skin reactions, hepatic side effects, and arthralgia.
Statistical analysis
The sample size for the trial was based on the primary aim of the study to detect non-inferiority if an increase in the risk is at least 10%, that is, lower bound of confidence interval for risk ratio (MMI vs. RAI) >1.1 (non-inferiority margin is 10%) with a type 1 error (α error) of 0.05 (one-sided) and a power of at least 80. An attrition rate of about 20% was considered. Baseline and outcome variables were compared using the Kruskal–Wallis test followed by a post hoc test (Dunn's multiple comparison). In each case, significant difference was assessed by one of the following tests: Mann-Whitney for continuous and chi-square and Fisher's exact test for categorical variables. Time-to-treatment success (euthyroidism) was documented using a Kaplan–Meier curve. Cox proportional hazards models were performed to assess the strength of association between study variables.
The primary hypothesis was that MMI treatment would be non-inferior to RAI therapy with regard to the primary outcome, with a margin of 10% for the upper boundary of the confidence interval of the risk ratio. Non-inferiority was established for the primary outcome if the lower limit of the one-sided 97.5% confidence interval of the risk ratio was >10%. A p-value of <0.05 was considered significant. Statistical analysis was performed using SPSS v9.05 (SPSS Inc., Chicago, IL).
Results
Study patients
Baseline clinical and laboratory characteristics of the two groups are shown in Table 1. There was no significant difference in sex, smoking, goiter size, and serum concentrations of fT4, T3, and TSH between the two groups.
Baseline Characteristics of the Two Study Groups
Data shown are the mean ± SD unless otherwise indicated.
Normal TSH: 0.4–5.06 mIU/L; fT4: 923 pmol/L; T3: 75–200 ng/dL.
fT4, free thyroxine; T3, triiodothyronine; TSH, thyrotropin; SD, standard deviation.
Effect of treatment
MMI group
The starting dose of MMI was 14 ± 5 mg/day. By the end of the first year of treatment, 33 (62%) patients were euthyroid, and 15 (28%) patients had subclinical hyperthyroidism. By the end of 60 months of MMI treatment, all 53 patients were euthyroid. However, from month 72 to month 96 of the study, two (3.8%) patients experienced an exacerbation of their subclinical hyperthyroidism. The remaining patients had normal serum fT4, T3, and TSH concentrations. The mean requirement of daily MMI dose to maintain normal thyroid function was 6.3 ± 2.0, 4.7 ± 1.2, 4.5 ± 0.9, 4.3 ± 1.0, 4.1 ± 1.0, and 4.0 ± 1.3 mg (median 4 mg) after one, two, three, four, five, and eight years of study, respectively. The decreasing dose of MMI over time was not related to initial levels of fT4, T3, or TSH or to goiter size. Mean estimated goiter weight decreased from 48 ± 6 to 41 ± 7 g (p < 0.001) by the end of the study.
RAI group
The administered activity of 131I ranged between 15 and 29 mCi (555–1073 MBq), and the mean activity was 16.7 ± 2.7 mCi (618 ± 100 MBq). By the end of the study, 24 (4%) patients achieved euthyroidism, of whom eight (33.3%), six (25%), and three (12.5%) had been subclinically hyperthyroid at the end of the first, second, and third year after RAI therapy, respectively, although by the end of the fourth year, all 24 patients were euthyroid. Eighteen (33.3%) patients became hypothyroid and required levothyroxine treatment, and 12 (22.2%) patients had either persistence or recurrence of hyperthyroidism, requiring further treatment of hyperthyroidism. Of these 12 patients, six became hypothyroid after a second RAI treatment, four attained euthyroidism following one to three additional RAI treatments, and two had multiple recurrences of hyperthyroidism and required four RAI treatments plus intermittent MMI treatment. The success rate (both euthyroidism and hypothyroidism) was 78% after the first RAI treatment and 96% following additional RAI treatments.
Mean estimated goiter weight decreased 38% from 50 ± 6 to 31 ± 6 g (p < 0.001) by the end of the study. The difference in decrease in goiter size was significantly higher in the RAI versus the MMI group (19 vs. 5 g; p < 0.001).
Figure 2 shows Kaplan–Meier curves for achievement of euthyroidism in the two groups. Of patients on long-term MMI, 51 (96.2%) became euthyroid by the end of the second year of treatment, while after one dose of RAI only 17 (31%) patients became euthyroid without additional treatments. Taking into account that the aim of RAI treatment is to attain euthyroidism with or without levothyroxine therapy, this aim was reached by 29 (53.7%) and 42 (78%) patients at the second and eighth years of treatment, respectively. Baseline characteristics of patients treated with RAI based on their thyroid status outcome are shown in Table 2. There was no difference in age, goiter size, and RAI activity at baseline among these groups, but baseline serum fT4 and T3 between those who became euthyroid or became hypothyroid after 131I treatment and patients who remained hyperthyroid were significantly different. Patients who had persistence or recurrence of hyperthyroidism after RAI treatment had significantly higher serum T3 levels before therapy compared to the other two groups. Table 3 shows the number of patients with different thyroid functional status in the RAI group; 24 (44%), 12 (22%), 9 (17%), and 3 (5%) patients showed recurrence of overt and subclinical hyperthyroidism by one, two, three, and four years after RAI treatment, respectively.
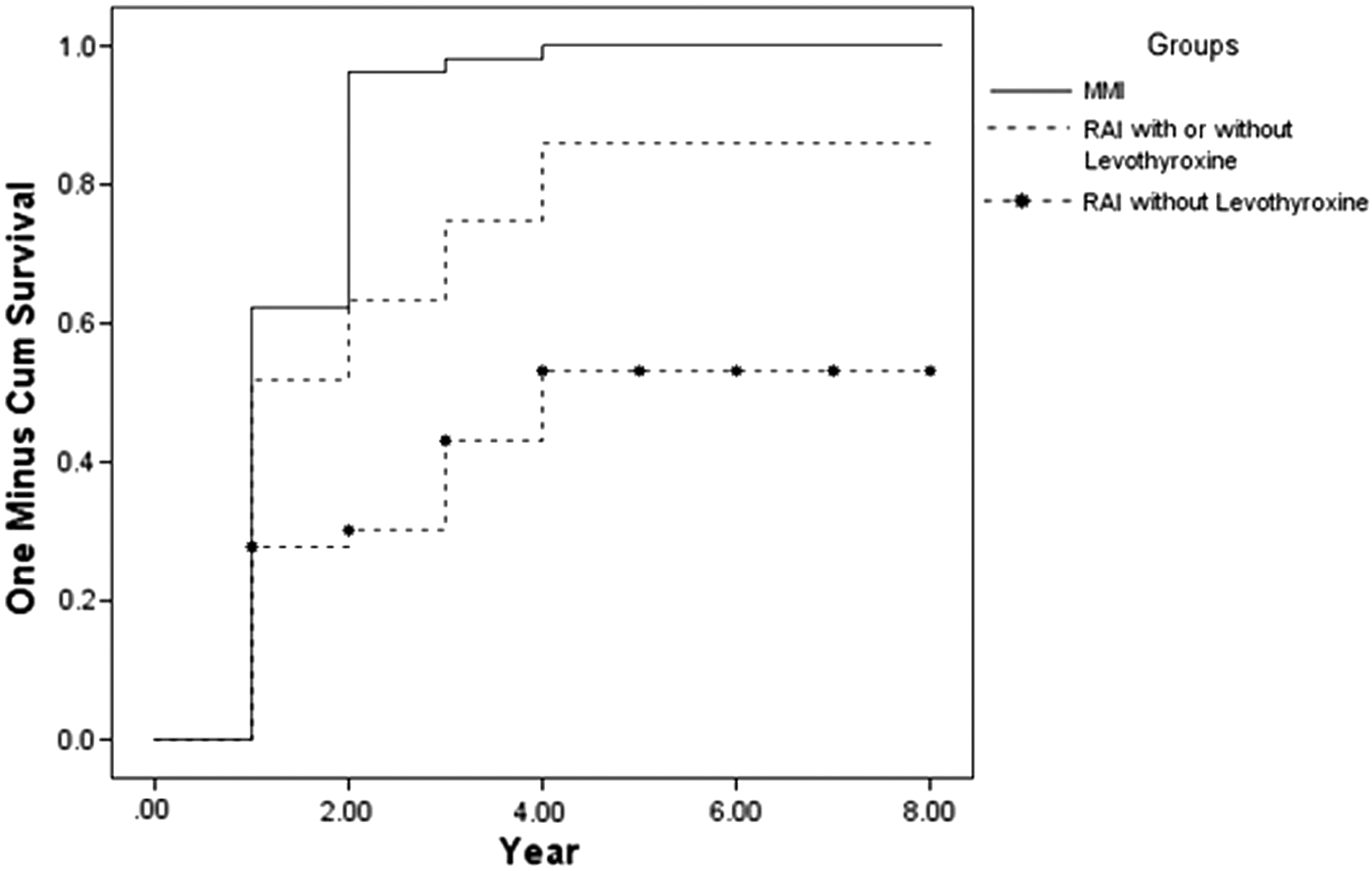
Kaplan–Meier curves for attainment of euthyroidism in TMNG patients treated with long-term methimazole (——) radioiodine (RAI) treatment. The lower line (---•---) demonstrates euthyroidism following one dose of RAI, without additional treatment. The upper line (------) shows the percentage of patients who achieved euthyroidism with or without levothyroxine treatment. A log-rank test showed a significant difference in sustained euthyroidism between the two groups (p < 0.05).
Baseline Characteristics of Patients Treated with Radioiodine According to Their Thyroid Function Status Outcome
Data are presented as the mean ± SD.
Kruskal–Wallis test.
p < 0.05 in comparison to hyperthyroidism for fT4.
p < 0.05 in comparison to hyperthyroidism for T3.
RAI, radioactive iodine.
Different Thyroid Function Status Among 54 Patients with Toxic Multinodular Goiter Over Eight Years After One Dose of Radioiodine Treatment
All subclinical hyperthyroidism subjects converted to one of the other three groups (euthyroid, overt hyperthyroid, or overt hypothyroid) during eight years of follow-up.
Safety and adverse events
Adverse effects of MMI occurred in the first three months of treatment. Three patients developed skin reactions and were shifted to treatment with propylthiouracil, while one had elevation of liver enzymes and chose RAI therapy. From month 4 to month 100 of long-term MMI treatment, no other side effect related to MMI was reported. Mild anterior neck pain, nausea, palpitation, and abdominal discomfort were experienced by six patients receiving RAI, and symptoms were managed by symptomatic treatment. No serious side effects such as cardiovascular complications or cancer were observed in either group.
Discussion
The present study reports for the first time a head-to-head trial comparing the effectiveness and safety of long-term MMI versus RAI therapy in patients with TMNG. The results show that long-term treatment with MMI is both effective and safe and non-inferior to RAI treatment. In fact, only 11% of patients with TMNG experienced exacerbation or overt hyperthyroidism during a median of 78 months of long-term MMI treatment, whereas the remaining 89% experienced euthyroidism with normal fT4, T3, and TSH concentrations until the end of the study. It is noteworthy that the mean required dose of MMI to maintain euthyroidism decreased from 14 ± 5 mg/day at the start of treatment to 4.7 ± 1.2 mg/day by the second year, and remained low until the end of study. Therefore, 50% of the patients with TMNG, required ≤4 mg/day of MMI to maintain normal thyroid function.
Adverse effects of MMI usually occur during the first three to six months of treatment, and tend to be associated with high MMI doses (14). In the present study, there was a low rate of side effects from MMI compared to previous reports. This might be partly related to low to moderate initial doses of MMI (10–20 mg daily) and subsequent titration to 5–7.5 mg as a daily maintenance dose.
The natural history of TMNG is not similar to Graves' disease and does not have repeated episodes of remission and relapse of hyperthyroidism (2). Therefore, ablative treatment has been considered as the treatment of choice (5 –8). Antithyroid drugs have been employed mostly for preparation of ablation (4) and treatment with antithyroid drugs for more than six months for TMNG was previously not recommended routinely (15).
The findings of the present study regarding RAI treatment are in concordance with those previous studies. The usual dose of 150 μCi/g of thyroid was administered. A meta-analysis has shown equally successful outcomes after the estimated and calculated dosage of RAI (16). The success rate (both euthyroidism and hypothyroidism) was 78% after the first treatment and 96% following additional RAI treatments, which is close to the 85–100% success rates that have been previously reported (7). During a median of 80 months of follow-up, 41% of RAI treated patients became hypothyroid. In the largest retrospective study of 346 patients with hyperfunctioning thyroid nodules, the occurrence of hypothyroidism was 28%, 46%, and 60% after 5, 10, and 20 years of RAI treatment, respectively (17). Decrease in goiter size was estimated at 38% in the present study, which is in accordance with the approximately 40% reduction reported in previous studies (7). It should be noted that the RAI activity selected for this study was at the low end of the spectrum recommended for the treatment of hyperthyroidism. It is believed that the lower the administered RAI activity, the more likely it is that additional therapy will be required (5 –7). Thus, success, defined as euthyroidism or hypothyroidism, is higher after RAI therapy. However, the time taken to achieve euthyroidism is shorter with MMI.
In the management of elderly patients with hyperthyroidism, the time period needed to achieve euthyroidism may be important. The present study shows that 42% of patients in the RAI group and only 17% in MMI group had hyperthyroidism (both overt and subclinical) by the end of their first year of treatment.
The non-inferiority of long-term MMI treatment in restoring normal thyroid function suggests that it is a valid alternative to ablation in the treatment of patients with TMNG. It has been shown that in patients with Graves' disease on long-term MMI therapy, there were fewer variations in serum TSH levels than in those taking levothyroxine for RAI-induced hypothyroidism (18), and the former patients have better neuropsychology test results than the latter (19). Physicians have considered antithyroid drugs for treatment of TNMG inappropriate because of the possibility of an exacerbation of the hyperthyroidism during treatment and recurrence of hyperthyroidism after discontinuation of medication. However, an exacerbation of overt hyperthyroidism occurred in only 3.8% of patients during eight years of long-term MMI therapy in the present study. In addition, findings from this and previous studies (10,17) show that side effects related to MMI are very rare in patients on long-term MMI therapy.
Why does a longer period of MMI therapy cause a reduction in the requirement of MMI dosage? Similar observations have been reported during long-term MMI therapy for Graves' disease. It can in part be explained by the restoration of a dysregulated immune system (20). Does long-term euthyroidism decrease the autonomous process or does MMI administration per se influence the autonomy of the thyroid nodules? Thyroperoxidase antibodies were not measured at the initial visit, and no data on thyroid antibodies during the follow-up were available. Therefore, the possibility of a confounding autoimmune process cannot be ruled out entirely. The possibility of these and other mechanisms should be investigated in the future.
The strengths of the present study are that it reports the largest sample of patients with TMNG in an iodine-sufficient region who received long-term MMI treatment, it is prospective in design, and it reports a comparison with the results of RAI therapy.
The following limitations should be considered while considering the findings of this study. First, the study population is from an iodine-sufficient West Asian country, and it is unclear whether its results are generalizable. Second, the size of goiter in this study was two to three times the normal thyroid size. Therefore, the findings may not be effective in TNMG patients with very large goiters. Third, the study was performed in patients ≤60 years of age, and the findings may not apply to older patients. Lastly, since this study was not designed as a double-blinded trial, there may have been biases related to selection and attainment.
In conclusion, continued low-dose MMI treatment is an effective and safe method for treatment of TMNG. It is not inferior to RAI therapy and may be considered to be appropriate for some patients with TMNG.
Footnotes
Acknowledgments
We are indebted to Ms. Niloofar Shiva for critical editing of English grammar, and to Ms. Tahereh Fakhimi for preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.