
Abstract
Background:
The iodine nutritional status of the Chinese population has been greatly improved in recent years. Therefore, the reference values for thyroid volume (Tvol) in children with sufficient iodine intake need to be updated. The study aimed to update the reference values for Tvol in children with sufficient iodine intake in order to define goiter in the context of sustained iodine sufficiency.
Methods:
A cross-sectional study was conducted in children with sufficient iodine intake in China. Twice-repeated 24-hour urine samples were collected from each child to estimate habitual daily iodine intake. Serum thyroid function tests were measured. Tvol was assessed by ultrasound. From the sample of euthyroid children with sufficient iodine intakes, the 50th and 97th percentiles for Tvol by age and body surface area (BSA) were calculated using quantile regression.
Results:
A total of 679 children aged 8–13 years with sufficient iodine intake (188 μg/day [145–235 μg/day]) were included in the analysis. The mean Tvol of the children was 4.1 ± 1.6 mL, and no differences were found between boys and girls in any age or BSA group. Quantile regression models demonstrated that BSA was a strong positive predictor of Tvol (p < 0.0001), while age only had a significant effect on median Tvol (p = 0.013). Sex was not a significant predictor of Tvol in children.
Conclusions:
The reference values for Tvol in Chinese children have been updated. This study indicates that the upper limit of (97th percentile) Tvol was dependent on BSA, while the median Tvol was determined by both age and BSA.
Introduction
Thyroid volume (Tvol, mL) and goiter rates in children have been regarded as sensitive indicators reflecting long-term population iodine nutrition (1,2). Iodine deficiency can lead to enlarged Tvols and goiter (3). A goiter rate of ≥5% in school-age children is one of the criteria for defining iodine-deficient populations (1).
In the past, goiter caused by severe iodine deficiency was prevalent in many regions globally (4). With successful implementation of iodine fortification programs, iodine nutrition has been greatly improved in much of the world (5). Severe iodine deficiency and visible goiter are no longer common, and normal values for Tvol in children may thus have changed. In addition, many epidemiological studies in regions with known iodine sufficiency or excessive iodine exposures have reported goiter rates >5%, and goiter rates vary substantially across studies (6). Current reference ranges for Tvol may not be appropriate in settings of long-term sufficient iodine nutrition.
In 2004, the World Health Organization (WHO)/International Council for the Control of Iodine Deficiency Disorders (ICCIDD)/United Nations International Children's Emergency Fund (UNICEF) developed reference intervals for Tvol in school-age children with sufficient iodine nutrition based on body surface area (BSA), age, and sex (7,8). The reference ranges used in China were proposed in 2007 and are based on age (2). A previous study found that goiter rates as defined by WHO/ICCIDD/UNICEF and by the Chinese reference were widely divergent (33% vs. 10.9%) (6). A recent workshop held by the Shandong Endemic Disease Control committee suggested that present reference ranges for Tvol in China were inaccurate and too high, while the 97th percentiles (P97s) proposed by WHO/ICCIDD/UNICEF classified an inordinate proportion of children as goitrous. Therefore, the reference ranges for Tvol in Chinese children need updating.
Between 2010 and 2015, the iodine deficiency disorders (IDD) program in China entered a phase of sustainable iodine sufficiency (9). The present study assessed children's iodine intake and thyroid function. The aim was to establish normal reference values for Tvol by ultrasound in 8- to 13-year-old euthyroid Chinese children with sufficient iodine intake.
Methods
Subjects
The study recruited 2242 children with long-term exposure to different iodine intake levels in order to study the upper safe intake level of iodine for children. Twice-repeated 24-hour urine samples from each child were used to estimate habitual daily iodine intake. Blood samples were also collected to assess thyroid function. A detailed description of the study population and design has been previously reported (10).
This study included children with sufficient iodine intake and excluded those with excessive or insufficient iodine intake. Based on prior results defining upper levels of iodine for children and on the recommended intake levels of iodine from present Chinese dietary reference intakes (10,11), 90–250 μg/day was defined as sufficient iodine intake for children aged 7–10 years, while 110–300 μg/day iodine intake was considered sufficient for 11- to 14-year-olds. In addition, children who were missing thyroid volume data and those with thyroid dysfunction or positive thyroid antibodies were excluded. A flow chart is presented in Figure 1.
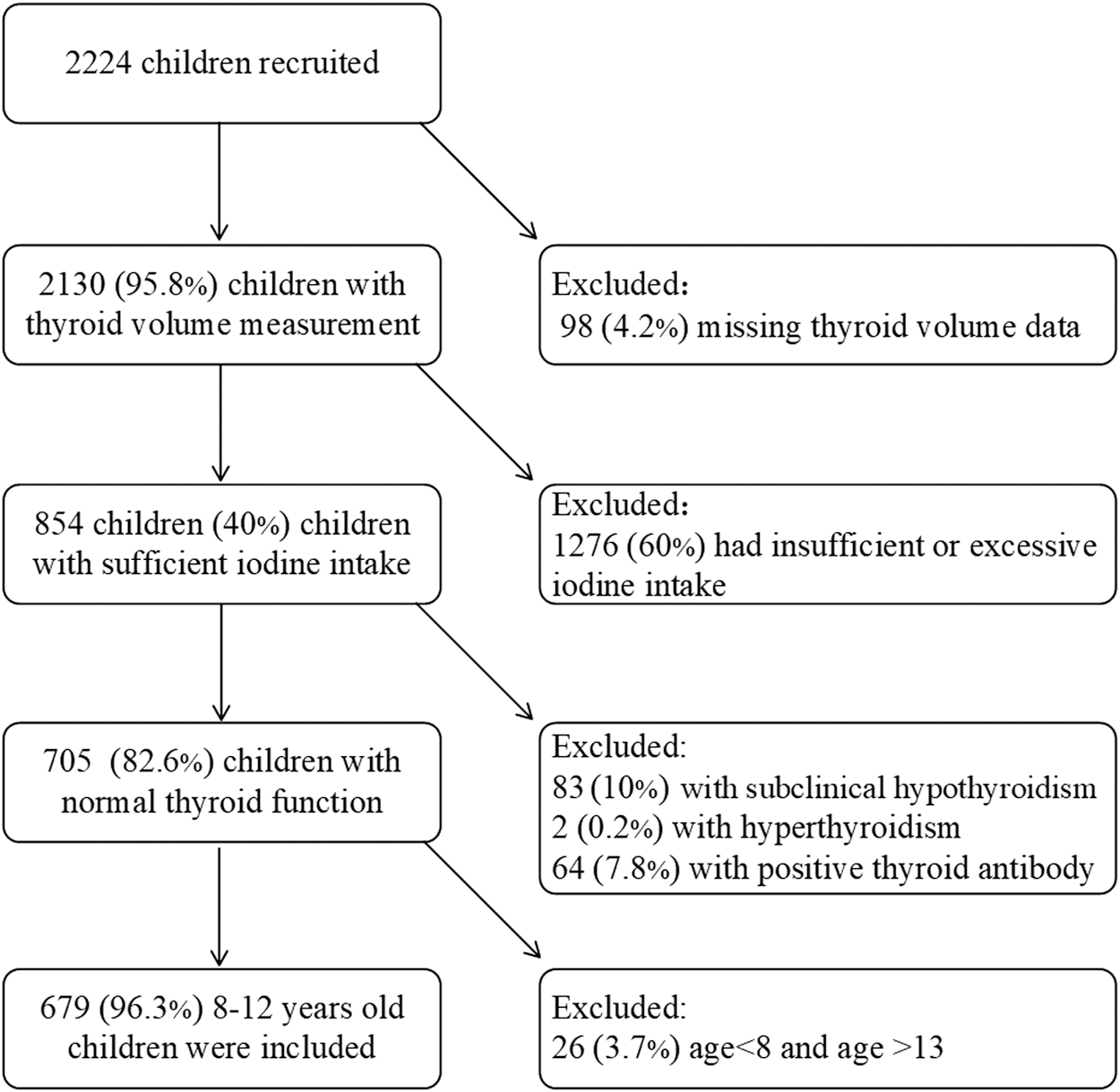
Flow chart of the study.
Anthropometry
Height and weight were measured using standardized procedures. Height was recorded to the nearest millimeter and weight to the nearest 100 g. BSA (m2) was calculated using the formula: BSA = weight (kg)0.425 × height (cm)0.725 × 0.007184 (7).
Thyroid volume measurements
Tvol was measured by a single trained operator using the HaiYing HY5511 ultrasound service (HaiYing Electronics Co.) equipped with a 7.5 MHz linear transducer and a probe length of 4 cm. Before the study, the technique of the operator was validated against that of an experienced radiologist who specializes in ultrasound. During the study, in order to monitor measurement reliability, the thyroid volumes of 50 randomly selected children were measured twice; the mean difference between the two measurements was close to zero (3.2 ± 1.0 mL vs. 3.2 ± 1.1 mL, p = 0.5).
Measurements were performed while subjects sat upright in a straight-backed chair with the neck extended. For each thyroid lobe, the maximal width (w) was measured in the transverse section, and the maximal length (l) and depth (d) were determined in the longitudinal section. The volume of each lobe was calculated using the formula proposed by Brunn et al.: Tvol (mL) = 0.479 × w (cm) × l (cm) × d (cm) (12). The Tvol was the sum of both lobes (the isthmus was not included).
Serum thyroid function measurements
Blood samples were collected and thyroid function measurements were carried out in the clinical laboratory of Tianjin Medical University General Hospital. Concentrations of serum thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) were analyzed using an ADVIA Centaur automatic chemiluminescence immunoassay (Siemens Healthcare Diagnostics). TSH, fT3, and fT4 values for all children included in the study were within reference intervals.
Urinary iodine concentration measurements and iodine intake calculation
Urinary iodine concentrations (UIC) from two collections were measured by spectrophotometric detection of the Sandell–Kolthoff reaction with ammonium persulfate digestion at the Key Laboratory of Hormone and Development (Ministry of Health), Metabolic Diseases Hospital, and the Tianjin Institute of Endocrinology, Tianjin Medical University.
The habitual (or usual) daily iodine intake for each child was estimated using the best linear unbiased predictor (BLUP), computed by PC-SIDE software, which was developed by Iowa University. The BLUP is a weighted average of the child's two-day average intake and the group's mean intake, and has the smallest prediction error variance among all linear and unbiased predictors of usual intake. The weights are proportional to the ratio of the within-child variability in iodine intake to the total observed variability.
Statistical and data analysis
All data analyses were performed with SAS v9.3 (SAS Institute). Means and standard deviations are used to describe normally distributed continuous variables, while medians and interquartile range are used to present skewed variables. Differences in variables between included and excluded children and between boys and girls were analyzed by t-tests, Wilcoxon tests, and chi-square tests. Thyroid volume was transformed to normality with Ln transformation. Transformed data were used to calculate percentiles based on the Gaussian distribution, which were then transformed back to the linear scale. Pearson correlation analysis was used to test the relationship between thyroid volume and covariates. Quantile regression models were used to estimate 50th percentile and 97th percentile of thyroid volume in children in relation to age, BSA, and iodine intake.
The reported p-values are two-sided, and p < 0.05 was defined as significant.
Results
Sample characteristics
As presented in Figure 1, of 2224 total children who participated the study, 679 were included for the analysis of Tvol reference intervals. Supplementary Table S1 presents the baseline characteristics of both included and excluded children. Compared to the excluded group, children included in the analysis were more likely to be girls, and their age, height, weight, BSA, and habitual daily iodine intakes were significantly lower (p < 0.001).
Iodine nutrition and thyroid function of included children
As displayed in Table 1, the median UICs for spot urine samples and 24-hour urine samples in the included children were 229 μg/L (137–417 μg/L) and 219 μg/L (136–348 μg/L), respectively, and there were no significant differences between boys and girls (p > 0.05). The habitual daily iodine intake of included children was 188 μg/day (145–235 μg/day), and the iodine intake of boys was significantly higher than that of girls (p = 0.012). No differences were found between fT3, TSH, and Tvol in boys compared to girls, but fT4 was slightly higher in boys (p < 0.001).
Iodine Intake, Thyroid Function, and Tvol Thyroid Function in Included Children by Sex
Values are median (IQR) or mean ± SD.
Significantly different compared to boys (p < 0.01); #no differences were found between boys and girls (p > 0.05).
Tvol, thyroid volume; UIC, urinary iodine concentration; fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin; IQR, interquartile range; SD, standard deviation.
Relationships between Tvol and age, BSA, and iodine intake
Tvol in children was positively correlated with BSA (r = 0.60, p < 0.0001), age (r = 0.47, p < 0.0001), and iodine intake (r = 0.39, p < 0.0001). Medians and 97th percentiles of Tvol by age and BSA are presented in Table 2. No differences in Tvol were found between boys and girls in either age group (p > 0.05). Similarly, there was no difference in Tvol between boys and girls in each BSA group (p > 0.05).
Median and 97th Percentile Values for Tvol According to Age and Body Surface Area in 8- to 13-Year-Old Children
BSA, body surface area.
Figure 2 presents a summary of quantile regression results for covariates and Tvol. The quantile regression estimates with 90% confidence limits for BSA, age, and iodine intake on LnTvol are shown. BSA had a substantial and uniform effect over the whole range of Tvol, such that the Tvol of children increased as BSA increased (p < 0.0001). In addition, Tvol of children increased slightly with increasing iodine intake. On the other hand, age only had a significant effect on the 50th percentile of Tvol (p = 0.013), and sex was not a significant predictor for Tvol (p > 0.05, data not shown).
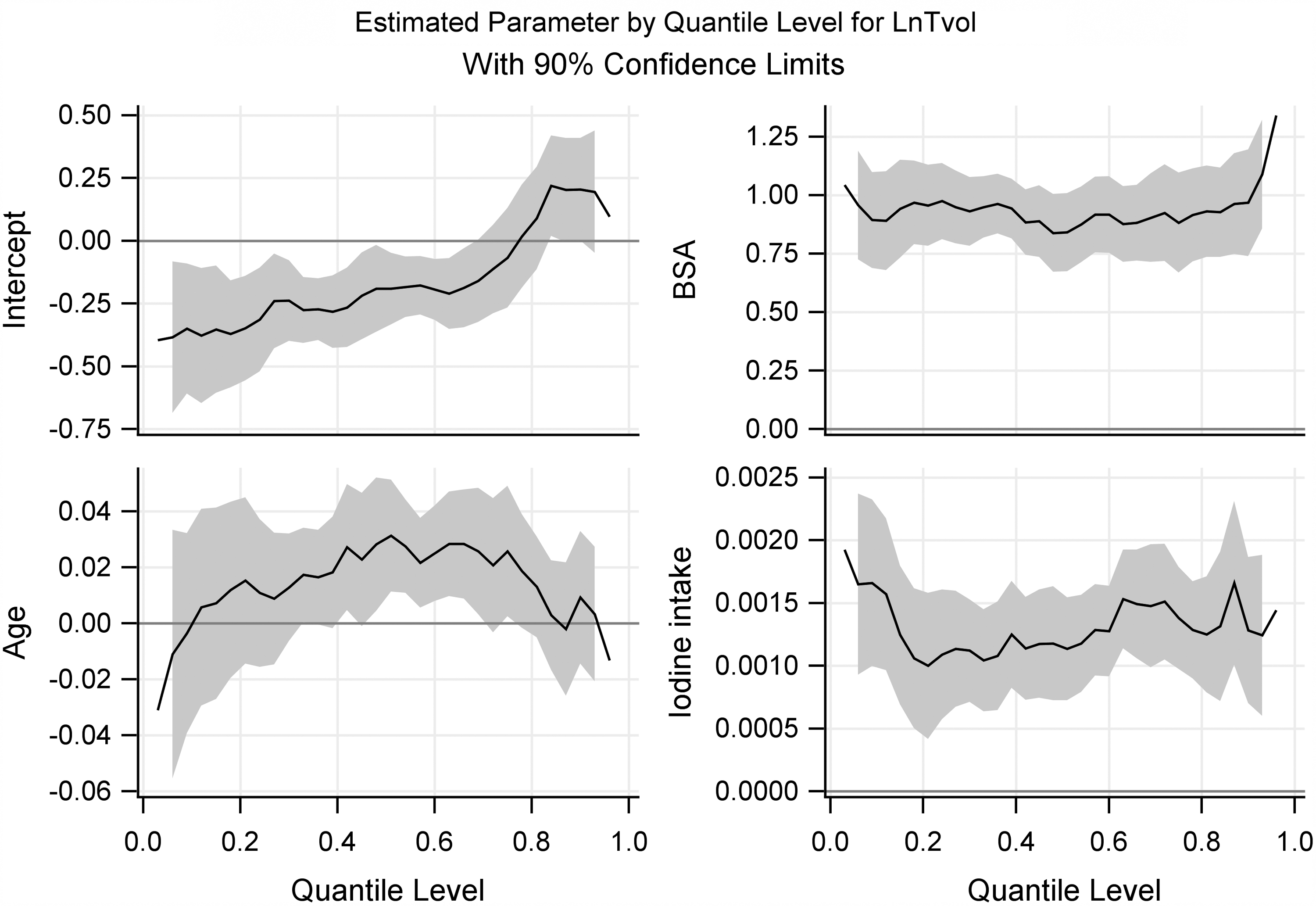
Quantile regression estimates for LnTvol model.
Age- and BSA-specific reference 50th and 97th percentile of Tvol
Given the effects of BSA, age, and iodine intake on Tvol, the age- and BSA-dependent reference values for Tvol for children with sufficient iodine intake were estimated using quantile regression models. As shown in Figure 2, age was a strong predictor of the 50th percentile of Tvol, and BSA had a substantial effect on Tvol over the whole range. Table 3 shows the 50th percentile estimates of Tvol for children by age and BSA. Table 4 shows the 97th percentile estimates of Tvol for children. However, age was not found to be a significant predictor of the 97th percentile of Tvol (p = 0.88).
50th Percentile [Confidence Interval] Estimates of Tvol for Children with Sufficient Iodine Intake by Age and BSA
Quantile regression models adjusted by BSA, age, and iodine intake.
—, no qualified subjects.
97th Percentile [Confidence Interval] Estimates of Tvol for Children with Sufficient Iodine Intake by Age and BSA
Quantile regression models adjusted by BSA, age, and iodine intake.
Discussion
China is a country with a long history of iodine deficiency. The government introduced universal salt iodization (USI) in 1994. By 2000, USI had virtually eliminated IDD in China (13). From 2010 to 2015, the IDD program in China progressed to a phase of sustained iodine sufficiency (9). The current age-based reference ranges for diagnosing endemic goiter in China were originally developed in 2007 (2). Iodine nutrition in China has changed substantially since then, and updates are needed.
Several prior studies have evaluated thyroid volumes in children from different regions. A study conducted in 11-to 14-year-old children in Italy showed that the overall prevalence of goiter was 8% (65/813), and the mean Tvol was 5.7 ± 2.1 mL (median = 5.4 mL) (14). In Japan, the goiter prevalence was 5.8%, the mean Tvol was 3.3 ± 1.5 mL, and the median Tvol was 2.5 mL (15). In Switzerland, the goiter prevalence was 0% (7), as defined by WHO/ICCIDD Tvol references (16). The goiter prevalence in children from six provinces in China was 6.7% (42/627) based on Chinese criteria, and their median urinary iodine was above the requirement levels (100–200 μg/L) (17). Goiter rates of 33% and 10.9% were previously reported according to WHO and Chinese criteria, respectively, in children from Shandong province (6). The reports of goiter prevalence are variable among different areas, especially when using different Tvol thresholds to diagnose goiter. Such differences make it difficult to compare and interpret goiter rates across regions.
Comparing the thyroid volumes of school-age children in China and abroad, it was found that the WHO median (P50) and 97th percentile (P97) values for thyroid volumes reported by Zimmermann et al. (8) were lower than those in the present study. A study recently conducted by Zhe et al. in Zhejiang Province, China (18), also reported higher Tvol than the WHO references. All sites in the study by Zimmermann et al. were iodine sufficient, as defined by a median UIC between 100 and 300 μg/L (1). However, their median UIC varied from 118 μg/L (11–446 μg/L) to 288 μg/L (51–12,764 μg/L). A study conducted in China found that the mean Tvol differed significantly by UIC levels (100–199 μg/L, 200–299 μg/L, ≥300 μg/L) (19). In addition, spot UIC can be used to represent the iodine nutrition of populations (1), but it is has not been validated as a biomarker in individual children. Twenty-four-hour urine samples are more accurate and reproducible than spot urine samples for evaluation of iodine status in school-age children (20). The present study aimed to ensure that thyroid volume in children with sufficient iodine intake was being assessed by accurately estimating individual iodine intakes through twice-repeated 24-hour urine sample collections.
It was found that several factors influence Tvol. Inter-observer and inter-equipment variation in ultrasonographic thyroid measurement can give rise to reported differences in thyroid volume (21). This study employed an experienced sonographer; when thyroid volume measurements were repeated in a subsample of children, there was no difference between the two measurements. A study conducted in Italy demonstrated a significant correlation between thyroid volumes and variables including family history of goiter in first- and second-degree relatives, reported use of iodized salt, and residence in rural areas (14). This study suggested that iodine deficiency in childhood causes a subtle enlargement of the thyroid (22). Tvol by ultrasound has previously been reported to be strongly correlated with age, sex, body weight, height, and BSA (8,22 –27). The reference interval for Tvol in school-age children set by WHO/ICCIDD/UNICEF was based on BSA, age, and sex (7,8). This study found that BSA, age, and iodine intake were strongly correlated with thyroid volume in children, but there were no differences in Tvol between boys and girls.
Quantile regression models were further used to analyze the relationships between thyroid volume and covariates. It was found that age was a strong predictor of only the median Tvol, while BSA had a substantial and uniform effect over the whole range of Tvol. Therefore, the reference for median of Tvol in children should be adjusted by both age and BSA. Similar results were seen in the study by Zou et al. (26), who also found that age and BSA were the main predictors of Tvol.
The present results differ from some prior studies. The median value of Tvol according to age was slightly lower than in schoolchildren from Tuscany (22), while it was higher than the data reported by Zimmermann et al. (8). In a study conducted in Switzerland, the goiter prevalence using the 97th percentile from the original normative data of Gutekunst and Martin-Teichert and the WHO/ICCIDD recommended cutoff values was 3.9% and 0%, respectively (7,28). The Tvol values of Gutekunst and Martin-Teichert are 20–42% lower than the WHO/ICCIDD threshold (16). There can be substantial discrepancies when goiter prevalence is established using differing Tvol criteria. The reasons for differences across studies are likely complex, and may include body size, ethnicity, dietary habits, and exposure to environmental goitrogens, as well as differing concentrations of iodine in food and water.
Because iodine nutrition in China has changed, it is important to update the criteria for diagnosing endemic goiter. Data from this study can provide guidance for the determination of goiter in Chinese children. There are some limitations to this study, including a relatively small sample size for the Tvol analysis, and the lack of an international sample. Study strengths include the use of twice-collected 24-hour urine samples to estimate iodine intake, and the inclusion only of children with sufficient iodine intake. Urinary iodine varies markedly, and chance variation may have caused inclusion of more children with iodine intake in the higher range compared to the low range based on iodine excretion in the population from which they were selected. In conclusion, reference values for Tvol for children have been established by BSA and age. It was found that the median Tvol level is determined by both age and BSA of children, while the upper limit of Tvol for defining goiter in children was more dependent on BSA.
Footnotes
Acknowledgments
We thank the Shandong Institute for Endemic Disease Control and Research for their strong support and help in the field investigation. We appreciate the cooperation and participation of teachers, students, and their caregivers. This study was supported by the National Natural Science Foundation of China (NSFC grant nos. 81330064 and 71774115) and Science Foundation of Tianjin Medical University (no. 2017KJ235). Study ID number: NCT02915536 (registered at the
Author Disclosure Statement
None of the authors declares a conflict of interests.
Supplementary Material
Supplementary Table S1