
Abstract
Background:
Elderly patients with differentiated thyroid cancer (DTC) tend to have more advanced disease at presentation, for which high activities of radioiodine (RAI) are often recommended. However, the 2015 American Thyroid Association guidelines recommend that empirically administered activities of RAI >150 mCi should be avoided in patients >70 years of age, based on calculated bone-marrow exposure according to two dosimetry-based studies. This study aimed to evaluate the effect of RAI treatment on bone-marrow function in elderly DTC patients.
Methods:
DTC patients ≥70 years of age who received RAI treatment and on whom a complete blood count was performed before and after treatment were included. Blood counts within one year before RAI and one year following treatment were compared in order to assess for marrow suppression. The impact of demographic, clinical, and laboratory variables on complete blood count were assessed.
Results:
One hundred fifty-three treatments in 122 patients met inclusion criteria, with a mean patient age of 76 ± 4.3 years, and 75% were women. High-risk features at presentation included T4 disease in 17%, lymph node metastases in 34%, and distant metastases in 14%. Mean RAI activity was 136.8 ± 48 mCi (82% ≥ 100 mCi, 66% ≥ 150 mCi). Of 153 RAI treatments analyzed, 114 (74%) were first treatments, 28 (18%) second treatments, seven (5%) third treatments, and four (3%) fourth treatments. At 0–3 months after RAI treatment, there was a statistically significant decrease in platelets (238 ± 66 vs. 216 ± 69 × 109/L, 10% decrease; p < 0.001), white blood cells (WBC; 6.9 ± 2 vs. 6.1 ± 1.9 × 109/L, 13% decrease; p < 0.001), and hemoglobin (Hb) in women (12.8 ± 1.1 vs. 12.4 ± 1.1 g/dL, 3% decrease; p = 0.01). Mean platelets, WBC, Hb in women, and lymphocytes remained decreased (but within the reference range) one year after treatment. Subgroup analysis demonstrated platelet suppression only with activities ≥100 mCi, and WBC and Hb suppression only with activities ≥150 mCi, with mean values within the reference ranges. There were no clinically significant cytopenia events during follow-up.
Conclusions:
Empiric RAI treatment in elderly patients causes mild bone-marrow suppression, with little clinical significance. Activities of 150–200 mCi can be safely used when indicated.
Introduction
Management of elderly patients with differentiated thyroid cancer (DTC) poses a unique challenge. While advanced age is an adverse prognostic factor requiring a more aggressive therapeutic approach, treatment of the elderly is often complicated by comorbidities, which increase the risk of surgery, radioiodine (RAI) treatment, and local or systemic therapies. Several studies have evaluated DTC in older adults/elderly patients (with various definitions of “elderly,” ranging from >65 years to >75 years), showing more aggressive disease on presentation with higher disease stage, greater tumor size, more distant metastases, and more poorly differentiated histology when compared to younger patients (1 –8). Following treatment, older patients also have higher recurrence rates of up to 39% (3) and higher disease-related mortality (4). According to these data, elderly patients often require higher activities of RAI compared to younger patients.
Concerns regarding the safety of RAI in elderly patients were raised in two dosimetry-based studies from 2006 (9,10). In these studies, whole-body dosimetry was performed following thyroid hormone withdrawal (THW), and the maximum tolerable activity (MTA)—the administered activity that would deliver 200 cGy to the blood—was calculated. The conclusion of both studies was similar, calculating that activities of <140 mCi rarely exposed blood to >200 cGy except in the very elderly, and administered activities of 200–250 mCi frequently exceeded the calculated MTA in patients ≥70 years of age. Based on these studies, the 2015 American Thyroid Association (ATA) guidelines on thyroid cancer recommended that empirically administered activities of RAI >150 mCi should be avoided in patients >70 years of age (recommendation 73B) (11). In light of more severe DTC in elderly patients requiring higher activities of RAI, and the concern raised by dosimetry studies, the effect of various RAI activities on bone-marrow function was studied in patients ≥70 years of age.
Methods
Study design, subjects, and data collection
The electronic records at Rabin Medical Center, a tertiary university-affiliated medical center, were reviewed for all elderly patients (≥70 years of age) who were treated with RAI between 2002 and 2016. Inclusion criteria for the study were: patients with documented DTC treated with total thyroidectomy (with or without neck dissection), RAI treatment with ≥30 mCi, age ≥70 years at the time of RAI treatment, data on complete blood count (CBC) within one year before RAI and more than one year following treatment, and access to the complete electronic medical record. Inclusion was per treatment (and not per patient), as patients could have several treatments, some included and some excluded (e.g., treatments with or without sufficient data on blood counts). Decision on the activity of RAI was at the discretion of the treating physician, with consideration for patient preferences. In cases where several RAI treatments were administered, some before 70 years of age and some after, only treatments after 70 years of age were included with documentation of the cumulative activity and the number of previous treatments. Exclusion criteria included histopathological diagnoses other than DTC, active concomitant malignancy (other than basal cell carcinoma), current treatment with chemotherapy, kinase inhibitors or immunotherapy, and recent hemorrhage (within six months before RAI) with a decrease in hemoglobin (Hb) of ≥1.5 g/dL.
The following data were collected from the patient files: demographics, medical history and physical examination, sex, tumor size and histology, tumor-node-metastasis (TNM) stage according to the American Joint Committee on Cancer (AJCC) eighth edition (12), blood creatinine level, age at the time of treatment, preparation with recombinant human TSH (rhTSH) or THW, current RAI activity, cumulative RAI activity, and CBC before and after RAI treatment, including Hb, mean corpuscular volume, white blood cells (WBC), absolute neutrophil count, lymphocytes, and platelets count. Additional data were collected for hospitalizations, acute infections, blood transfusions, platelet transfusions, or treatment with granulocyte colony-stimulating factor within one year following RAI treatment. Cytopenia events were defined as a decrease in blood counts requiring transfusions or administration of colony-stimulating factors.
Whole-blood samples were processed by the ADVIA 2120i Hematology System analyzer (Siemens Healthcare Diagnostics, Deerfield, IL) and the Sysmex XN-1000 analyzer (Sysmex Corp., Kobe, Japan). Intervals assessed for bone-marrow function were: baseline values (before RAI), 0–3 months, 3–6 months, 6–12 months, and >12 months after RAI treatment. Appropriate reference ranges of Hb were used for men and women.
The study protocol was approved by the Institutional Research Ethics Committee.
Statistical analysis
All statistical analyses were performed with IBM SPSS Statistics for Windows v.25.0 (IBM Corp., Armonk, NY). Associations between two categorical variables were examined using the chi-square test and Fisher's exact test. Associations between continuous and quantitative variables were examined using the Mann–Whitney nonparametric U-test. A paired-sample t-test was used to compare values at each time point to baseline values. Pearson correlation coefficients were calculated to determine the association between RAI administered activity and marrow suppression. A two-sided p-value of <0.05 was considered statistically significant for all analyses.
Results
Patients
Two hundred forty-two RAI treatments in DTC patients who were ≥70 years old at the time of treatment were eligible for analysis. Seventy-eight treatments were excluded due to: missing data on CBC (n = 49), missing clinical data (n = 24), active concomitant cancer or anticancer treatment (n = 5), or <70 years old at the time of treatment (patients who had treatments both before and after the age of 70 years; Fig. 1). Finally, 153 treatments in 122 patients met the inclusion criteria and were analyzed (Table 1).
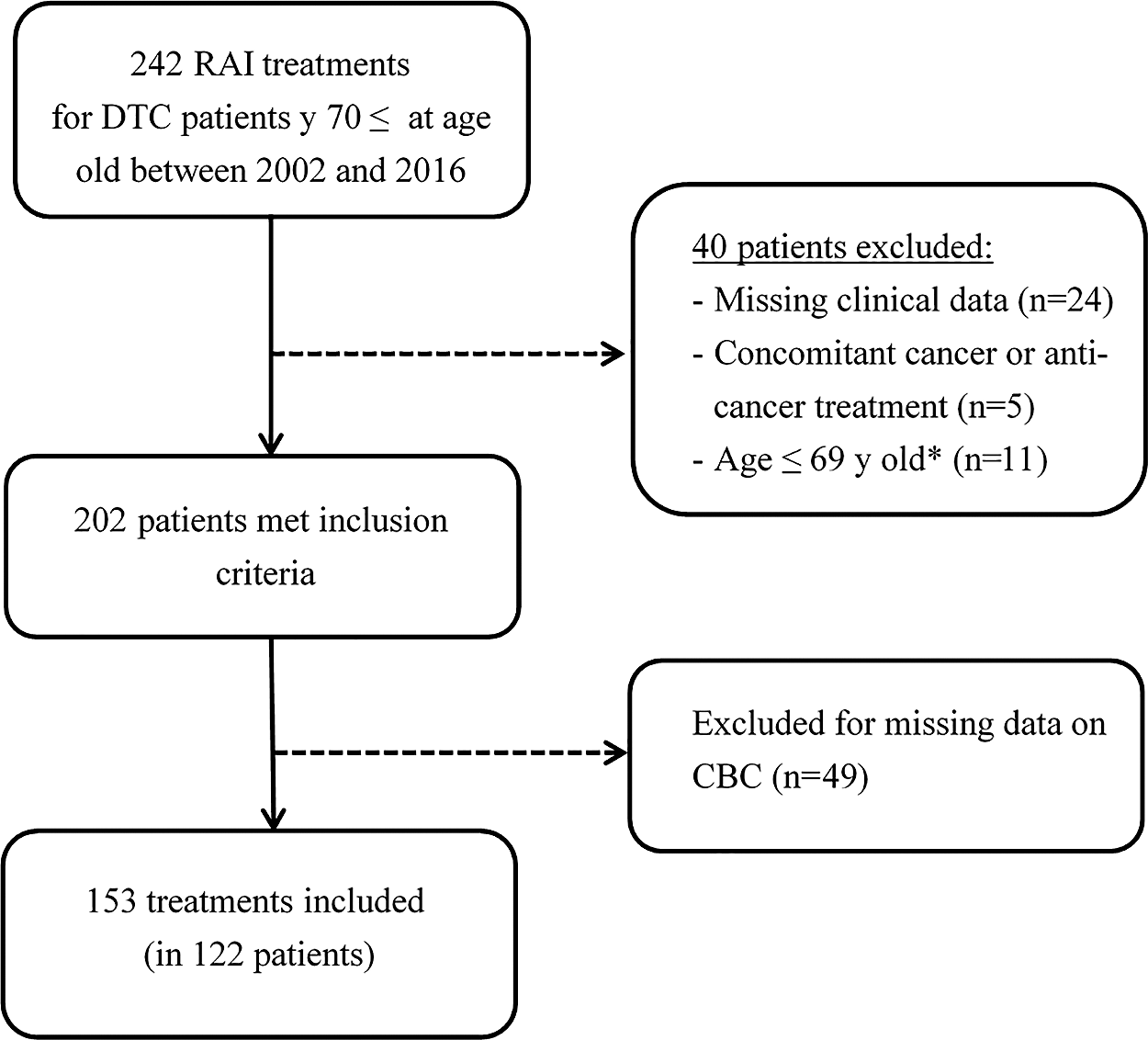
Inclusion flow chart (per treatment). *Patients who had two or more RAI treatments, some >70 years of age and some <70 years old. RAI, radioiodine; DTC, differentiated thyroid cancer; CBC, complete blood count.
Baseline Characteristics
AJCC, American Joint Committee on Cancer; PTC, papillary thyroid cancer; RAI, radioiodine; rhTSH, recombinant human thyrotropin; TNM, tumor-node-metastasis.
Mean age at RAI treatment was 76 ± 4.3 years, with a median age of 75 years. The mean primary tumor diameter was 22.4 ± 15 mm, and 75% of patients were women. Tumor histology was papillary thyroid cancer in 90% of patients (classic variant 66%, follicular variant 19%, tall cell 5%), follicular carcinoma in 6%, and poorly differentiated cancer in 4% of patients. High-risk features at presentation included T4 disease in 17%, lymph node metastases in 34%, and distant metastases in 14%. Twenty-six percent of patients had stage III–IV according to the AJCC eighth edition staging system. Serum creatinine was 0.93 ± 0.3 mg/dL at the time of treatment, and in seven patients the estimated glomerular filtration rate (eGFR) was <45 mL/min (range 22.5–44.4 mL/min), categorized as chronic kidney disease (CKD) stage 3–4. Other comorbidities included hypertension in 67% of patients, diabetes mellitus in 22%, ischemic heart disease in 22%, and paroxysmal atrial fibrillation treated with anticoagulation in 9%.
RAI treatment
Of 153 RAI treatments analyzed, 114 (74%) were first treatments, 28 (18%) second treatments, seven (5%) third treatments, and four (3%) fourth treatments. The mean time between repeated treatments was 15.6 ± 11 months (range 6–53 months), with mean administered RAI activity of 136.8 ± 47.5 mCi (median 150 mCi). The mean cumulative activity was 183.6 ± 132 mCi. A low activity of <100 mCi was administered in only 18 (12%) treatments. Higher activities were given to 88% of treatments as follows: 100–149 mCi in 35 (22%) patients, 150 mCi in 60 (39%) patients, 151–199 mCi in 19 (12%) patients, and ≥200 mCi in 21 (14%) patients. Most patients were prepared with THW (77%).
Bone-marrow function
At 0–3 months after RAI treatment, there was a small but statistically significant decrease in Hb (13 ± 1.2 vs. 12.8 ± 1.2 g/dL, 1.6% decrease; p < 0.01), WBC (6.9 ± 2 vs. 6.1 ± 1.9 × 109/L, 13% decrease; p < 0.001), and platelets (238 ± 66 vs. 216 ± 69 × 109/L, 10% decrease; p < 0.001; Table 2). The decrease in WBC was mostly due to lymphocyte counts (1.8 ± 0.7 vs. 1.5 ± 0.6 × 109/L; p < 0.001), with no significant change in neutrophil counts, and the decrease in Hb was found in women (12.8 ± 1.1 vs. 12.4 ± 1.1 g/dL, 3% decrease; p = 0.01), with no significant change in men (despite a mean Hb below the reference range at baseline). Mean Hb in women, WBC, and platelet levels remained suppressed for >12 months, but were within the reference range throughout follow-up (Fig. 2). None of the patients required treatment for cytopenia with colony-stimulating factors, blood transfusions, or platelet transfusions during the first year of follow-up.
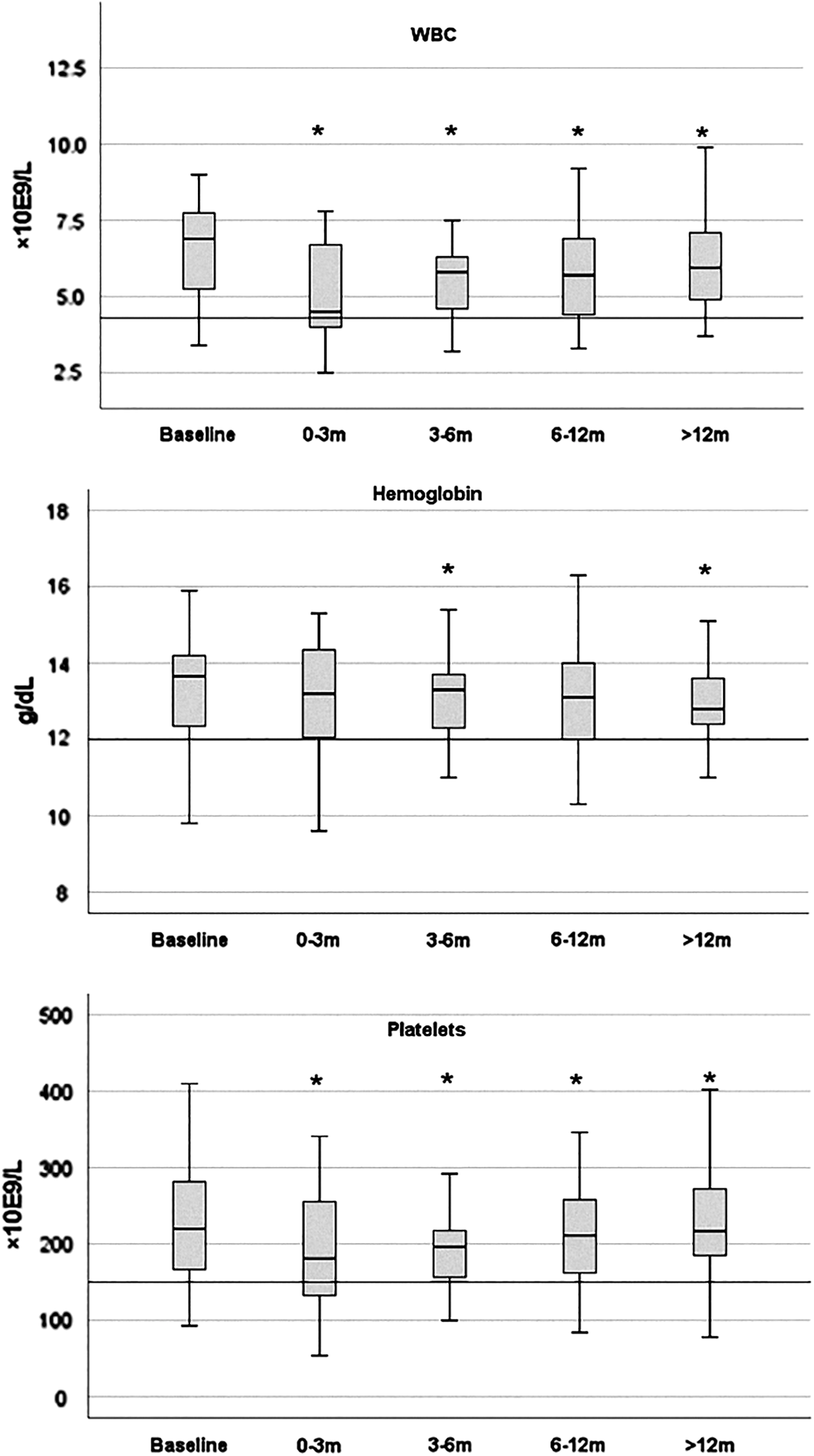
Marrow suppression in treatments with high activities of RAI (>150 mCi, n = 40). WBC, white blood cells. *Blood counts decreased compared to baseline (p < 0.05).
Blood Counts Before and After RAI Treatment
Numbers in each column relate to number of available CBCs at that time point (in parentheses). p-Values relates to comparison with baseline CBC only for patients included at each time point (and not to mean ± SD at baseline).
Paired sample t-test compared to baseline levels.
WBC, white blood cell; n.s., not significant; CBC, complete blood count.
The administered RAI activity correlated with the decrease in platelets (r = −0.33, n = 95, p = 0.01) and WBC (r = −0.2, n = 95, p = 0.04) at three months, but did not correlate with the decrease in Hb. On subgroup analysis, the most sensitive blood line was platelets, which decreased following treatment with ≥100 mCi (Table 2). WBC and Hb were significantly suppressed only in patients treated with ≥150 mCi. The decrease in the ≥150 mCi group was significant for platelets (236 ± 66 vs. 204.63 × 109/L, 16% decrease; p < 0.01), WBC (6.9 ± 2 vs. 5.9 ± 1.8 × 109/L, 17% decrease; p < 0.01), and Hb (13.2 ± 1.3 vs. 12.9 ± 1.3 g/dL, 2.3% decrease; p < 0.01). Further analysis for patients treated with 150 mCi (n = 60), >150 mCi (n = 40), or >200 mCi (n = 21) is presented in Table 2. The degree of marrow suppression was comparable in the three groups, with a decrease of mean platelets of 16%, 18%, and 16%, a decrease of mean WBC of 22%, 23%, and 17%, and a mean Hb of 2.3%, 3.1%, and 5.3% in the = 150, >150, and ≥200 mCi groups, respectively. The number of treatments and cumulative activity was not significantly associated with marrow suppression, as detailed in Table 3. Of note, the baseline WBC levels (before each treatment) decreased between the first and the second (p = 0.04) and third (p = 0.03) treatments. In four patients treated with a fourth course of RAI therapy (cumulative activity 657 ± 138 mCi), the maximal suppression during follow-up of the mean platelet count was 22%, of the mean WBC 31%, and of the mean Hb 2.2%, but all remained within the reference ranges.
Bone-Marrow Suppression According to Treatment Number and Cumulative Dose
Time between the first and second treatments 14.6 ± 9.8 months, between second and third treatments 14 ± 4.5 months, and between third and fourth treatment 25.6 ± 23.6 months.
Paired sample t-test compared to baseline levels.
Significantly lower than WBC before the first treatment.
Patients with an abnormal blood count at baseline did not have clinically significant cytopenia events following RAI. Eight patients had leukopenia at baseline (2.7–3.9 × 109/L), which remained stable after treatment (3.5 ± 0.4 vs. 3.9 ± 1.1 × 109/L; not significant [n.s.]). Twenty-four patients had anemia at baseline (9.8–11.8 g/dL), which remained stable (11.3 ± 0.5 vs. 11.2 ± 0.8 g/dL; n.s.), and nine patients had thrombocytopenia at baseline (93–147 × 109/L), which remained stable (123 ± 23 vs. 122 ± 35 × 109/L; n.s.).
Age, creatinine at the time of the treatment, rhTSH use versus hormone withdrawal, and tumor size did not predict a decline in blood indexes. Female sex was associated with an odds ratio of 2.77 for a decline in blood counts, but this did not reach statistical significance. Though creatinine and eGFR did not correlate with bone-marrow suppression when used as continuous variables, outcomes in patients with CKD stage 3–4 were also evaluated (there were no patients with CKD stage 5). Seven patients with a mean age of 77.4 years (range 75–81 years) were treated with 155 ± 20 mCi with no statistically significant decrease in blood counts and no cytopenia events.
Discussion
Elderly patients diagnosed with DTC often have advanced disease requiring aggressive therapy (1 –4). While several studies demonstrated thyroid surgery is safe in the elderly (13 –19), there is an ongoing debate regarding the safety of RAI therapy in this population. The 2015 ATA guidelines on thyroid cancer recommend that empirically administered amounts of RAI >150 mCi should be avoided in patients >70 years of age (11). This recommendation is based on two dosimetry-based studies published in 2006, showing that the MTA, commonly defined as 200 rads (cGy) to the blood, is potentially exceeded in a significant number of elderly patients (9,10). These studies were based on formulations by Benua and Leeper (first published in 1962) to estimate radiation exposure of the bone marrow, based on blood samples drawn after administration of 1–5 mCi (10). This dosimetric approach has been used successfully for several decades, but the actual impact of exceeding the calculated MTA, especially in elderly patients, is unknown. Only one previous study evaluated marrow suppression specifically in elderly patients, in which 15 patients were treated with RAI (median activity of 203 mCi) with no clinically important marrow toxicity (20). Given the discrepancy between the need for high activities of RAI to treat the disease and the theoretical risk for bone-marrow suppression, a real-life study was performed evaluating bone-marrow function following RAI treatment in patients aged ≥70 years.
The study demonstrates that administration of adjuvant RAI therapy (88% ≥ 100 mCi and 65% ≥ 150 mCi) results in only mild bone-marrow suppression. While there was a statistically significant reduction in Hb in women, WBC and platelets at 0–3 months that persisted for more than one year, the mean ± standard deviation values remained within the reference range, and none of the patients had a clinically significant cytopenia event (requiring transfusions or colony-stimulating factors). Even with repeated treatments, where a gradual decline in WBC levels was seen, values remained within the reference range. The most sensitive blood components were platelets, with significant suppression starting at RAI activities of 100–149 mCi, while WBC and Hb were suppressed only at activities of ≥150 mCi. The degree of suppression was mild for Hb (M = 1.6%) and more pronounced for platelets (M = 10%) and WBC (M = 13%). This pattern of marrow suppression is in agreement with previous studies, demonstrating a significant decrease in platelets and WBC, with relative sparing of Hb (21 –23). The characteristic sensitivities of the various blood lines to radiation was evaluated in several animal models, and it was found that lymphopenia occurs almost immediately after marrow radiation exposure, followed by neutropenia, thrombocytopenia, and lastly by anemia (24). Notably, the results do support the previously published dosimetry-based estimates, as bone-marrow suppression was mostly significant in the ≥150 mCi group, but this radiation-induced damage seems to be mild and have limited clinical impact. Sub-analysis for patients treated with increasingly higher activities of 150, >150, and >200 mCi did not demonstrate statistically significant differences. Possible explanations for this finding include subgroups that are too small to reach statistical significance, a mixed population prepared with either rhTSH or THW, or heterogeneity in bone-marrow absorbed doses within each activity group due to differences in age, body mass index, body composition, or creatinine clearance that may alter RAI pharmacokinetics, especially in the elderly.
Compared to previous studies, the current results indicate that bone suppression in the elderly is not substantially different from that reported in younger patients (21,22,25 –29). Prinsen et al. (21) evaluated bone-marrow suppression in 331 patients (M age = 47.5 ± 17.2 years) following administration of a median 150 mCi, and showed that post-treatment platelets and leukocytes were transiently decreased (e.g., leukocytes decreased from 7.0 ± 2.1 × 109/L at baseline to 5.8 ± 2.1 × 109/L at six months; p < 0.01). A minor percentage of patients had cytopenia, but none required medical intervention. Molinaro et al. (22) examined the rate of persistent cytopenia one year after a single RAI treatment (M age = 47 ± 14.6 years, mean activity 126 ± 43 mCi), and demonstrated a statistically significant mild decline in WBC and platelet counts that persisted for at least one year after ablation. Two additional studies evaluated marrow suppression following high cumulative activities of RAI administered under dosimetric guidance (mean activity >250 mCi) and again demonstrated small but statistically significant decreased blood counts (25,26). Age at the time of treatment correlated with the decrease in blood counts in one study (26) but not in another (25). Overall, mild marrow suppression following RAI is common in all age groups and rarely requires medical intervention.
The use of relatively high activities of RAI in the present cohort reflects more advanced disease at presentation, with 17% T4 disease, 34% with lymph node metastases, and 14% with distant metastases. This is in accordance with previous studies showing more advanced disease in elderly patients (1 –8,30). Chereau et al. (1) studied disease presentation and outcomes in older (65–75 years; 450 patients) and very old patients (>75 years; 128 patients), and found that very old patients are more likely to have an advanced TNM stage (III/IV) and greater tumor size, number of tumors, and extracapsular invasion compared to young and older patients. In terms of recurrence, Hollenbeak et al. (3) reported outcomes in 2883 patients aged ≥65 years from the Surveillance, Epidemiology, and End Results Medicare-linked databases, showing a 39% risk of recurrence, which is significantly higher than reported in younger groups. Extent of disease and older age were associated with higher risk of recurrence. Therefore, more aggressive treatment is recommended in the elderly, which can be safely delivered with adjuvant RAI therapy according to the data presented here.
The value of dosimetric-based therapy versus empiric RAI treatment in patients with metastatic disease is a matter of debate (31). For RAI to be effective, it is necessary to deliver a tumoricidal radiation dose to the metastatic foci (32,33). Assuming that higher administered activities of RAI would be more likely to deliver therapeutic lesional radiation doses, some centers use dosimetry to define the MTA, followed by treatment with the highest activity that can be safely given. However, dosimetry is not widely available, and most centers use empiric fixed activities of RAI depending on tumor histology, location, and extent of the disease. Whether a dosimetry-based approach is superior to empiric therapy depends on both efficacy and safety. Deandreis et al. compared 231 patients with metastatic DTC treated with RAI by an empiric fixed activity at the Gustave Roussy Institute in France, with 131 patients treated with a dosimetric-based approach at the Memorial Sloan Kettering Cancer Center in the United States (31). This study was the first to compare the two approaches in a large population of patients with metastatic disease, but it was limited by confounding factors of different patient populations from different institutions with various clinical disease profiles (34). With these limitations in mind, there was no evidence of superiority of either approach. In terms of safety, the major concern with empiric therapy is in patients with chronic renal failure and in the elderly. Deandreis et al. could not compare the safety of both approaches in these populations due to the retrospective nature of the study and missing data in medical records. In the absence of head-to-head comparisons for safety, the present data are reassuring regarding empiric-based treatments in elderly patients using activities of 150–200 mCi. In the seven patients with CKD stage 3–4 included in the present study, there were no cytopenia events, but outcomes in this small group cannot be generalized, and patents with CKD stage 3–5 should to be referred to experienced centers, preferably with dosimetry capabilities.
This study has several limitations. First, given the retrospective design of the study, treatment varied between patients in terms of RAI dosing and preparation with rhTSH versus THW. Preparation with rhTSH, which was used only in 23% of included patients, was previously reported to result in a lower bone-marrow absorbed dose (35). With the increased use of rhTSH in patients without distant metastases, and especially in the elderly population, less bone-marrow suppression can be expected (36). Second, the sample size of 153 patients and follow-up of one to two years cannot exclude the risk of long-term damage to the bone marrow. However, Prinsen et al. showed that both platelet and leukocyte counts normalized to baseline levels at five years after RAI treatment, which implies that bone-marrow toxicity is time limited (21). Third, CBCs were evaluated grouped into three-month periods, which may miss more subtle dynamics in bone-marrow function following RAI. These time groups are similar to those used in previous studies (21,22), and they were established based on the limited number of CBCs available for each patient during the first year of follow-up, and the use of paired-sample statistics in which each patient is her/his own control (pre and post therapy). The study design and the available data did not allow assessment of shorter time periods while maintaining statistical power. Finally, predictors for bone-marrow suppression were not found except for RAI activities, with the most pronounced suppression in patients treated with ≥150 mCi. It is possible that with a larger data set, other known risk factors such as chronic renal failure or pre-existing bone-marrow abnormalities would predict marrow suppression.
In conclusion, RAI therapy causes marrow suppression in the elderly at activities of 100–200 mCi, which is mild and of little clinical significance. Physicians treating elderly DTC patients should weigh the potential benefits of high-activity RAI therapy with this mild risk of marrow suppression on an individual basis for optimal outcomes.
Footnotes
Author Disclosure Statement
The authors have no financial relationships relevant to this article to disclose.