
Abstract
A 59-year-old woman with locally invasive poorly differentiated thyroid cancer with synchronous lung, mediastinal, and bone metastases and a somatic BRAFK601E mutation with contraindication for antiangiogenic drugs was treated with dabrafenib and trametinib. During treatment, serum levels of thyroglobulin increased as early as day 7 up to 10-fold over baseline at week 4. Concurrently, clinical hyperthyroidism occurred, with free triiodothyronine and free thyroxine levels increasing to 6.6 and 4.4 times their upper reference limit. Fludeoxyglucose positron emission tomography/computed tomography at one and two months after treatment initiation showed a PERCIST metabolic response with a 82% decrease in fludeoxyglucose uptake, whereas disease remained morphologically stable according to RECIST criteria. A diagnostic radioactive iodine whole-body scan performed when the patient was thyrotoxic with an undetectable serum thyrotropin level, in the absence of any exogenous thyrotropin stimulation, showed high radioactive iodine uptake in the lung, mediastinum, and skull metastases. A biopsy performed two months after treatment initiation showed a more differentiated growth pattern and a decrease in the mitotic activity compared to baseline. An increase of thyroglobulin and thyroid peroxidase was observed at both the protein and mRNA levels. Sodium–iodide symporter mRNA expression increased by >750 times over its initial level, and sodium–iodide symporter protein expression became detectable under treatment. A decrease in general status due to thyrotoxicosis led to treatment discontinuation. Thyrotoxicosis resolved rapidly and radioactive iodine uptake decreased by >90%. This clinical case shows that redifferentiation itself is not necessarily associated with an antitumor effect.
Introduction
Radioactive iodine (RAI) administration is the first-line treatment of patients with metastatic differentiated thyroid cancer (DTC). Unfortunately, the tumors of one third of patients do not take up RAI, and two-thirds of patients with significant RAI uptake are not cured (1). These patients end up being refractory to RAI (2). Drugs targeting angiogenesis have proven to be efficient in these patients, and two drugs have been approved after successful Phase III trials: sorafenib in the DECISION trial, with a significant prolonged progression-free survival (PFS) compared to placebo (median PFS 10.8 months vs. 5.8 months; hazard ratio [HR] = 0.59 [confidence interval (CI) 0.45–0.76], p = 0.001) and an objective response rate of 12%; and lenvatinib in the SELECT trial, with a significant prolonged PFS compared with placebo (median PFS 18.3 months vs. 3.6 months; HR = 0.21 [99% CI 0.14–0.31], p < 0.001) and an objective response rate of 65% (3,4). Moreover, drugs targeting the mitogen-activated protein kinase (MAPK) pathway have also been used in thyroid cancer patients because of the high prevalence of activating somatic alterations of genes encoding effectors in the MAPK signaling cascade and its consequences on increased cell growth and dedifferentiation (5,6). They are indeed found in up to 98% of papillary thyroid carcinomas (PTC), with BRAF and RAS point mutations being the most frequent ones (6). BRAF mutations (mainly represented by the p.V600E hot-spot mutation) are present in 60–70% of PTC and in 33–40% of poorly differentiated thyroid cancer (PDTC), or fatal non-anaplastic thyroid cancer (7 –9). Dabrafenib and vemurafenib, two anti-BRAF drugs, are used as single drug therapy or in association with a MEK inhibitor, trametinib, in DTC, with tumor response rates ranging from 26% to 54% with dabrafenib, vemurafenib, and a combination of dabrafenib with trametinib (3,10 –12). There is so far no experience on the association of vemurafenib and cobimetinib (a MEK inhibitor) in thyroid cancer, a combination developed in melanoma patients. In patients treated for BRAFV600E melanoma, vemurafenib and dabrafenib have shown their ability to improve survival as a single therapy (13,14), and the combination of a BRAF and a MEK inhibitor is safe and more effective than single-agent kinase inhibitors (15 –17). These treatments are given for prolonged periods of time in the absence of adverse events and until disease progression, and despite their efficacy, they may decrease the quality of life.
The activation of the MAPK pathway in thyroid cancers is associated with cell dedifferentiation with a decrease in RAI uptake. In BRAFV600E-mutated thyroid cancer cell lines, sodium–iodide symporter (NIS) expression and/or the proper localization of the NIS protein is suppressed, thus decreasing or abolishing the ability of thyroid cells to concentrate RAI (18 –20). In human BRAF-mutated PTC, there is a low expression of NIS and a low tumor differentiation score (8,21 –24). In a mouse model of thyroid cancer harboring a BrafV600E mutation, the cancer is insensitive to RAI treatment, and the treatment of these mice with small molecule inhibitors of either MEK or mutant BrafV600E reduces the proliferative index of the tumor and partially restores thyroid-specific gene expression (25). Furthermore, a high inhibition of ERK signaling with potent anti-MEK drugs was shown to be essential to maximize BRAFV600E thyroid cancer redifferentiation, providing a rationale for treating patients with a combination of BRAF and MEK inhibitors (26).
Attempts to redifferentiate the tumor and enhance RAI uptake in these patients have been challenging for the last three decades, with retinoic acid being the first tested compound; after initially encouraging results, they could not be confirmed (27).
Two preliminary clinical pilot studies in RAI-refractory patients showed an increase in RAI avidity and tumor response following RAI treatment after treatment with the MEK inhibitor selumitinib or the BRAF inhibitor dabrafenib in patients with RAS- or BRAFV600E-positive disease (28,29). In patients treated with selumetinib, the improved RAI uptake appeared to more effective in patients with RAS-positive tumors compared to those with a BRAFV600E mutation. A potential advantage of combined treatments with kinase inhibitors followed by RAI therapy is in the short exposure to kinase inhibitors and hence a limited amount of adverse events, and the potential to delay long-term treatment with kinase inhibitors in patients who become amenable to RAI therapy.
Here, tumor response and changes in scintigraphic, pathologic, and biological characteristics are presented in a patient with a BRAFK601E
(NM_004333.4:c.1801A>G;
Methods
Pathology
The sections obtained from tissues were fixed in 10% neutral-buffered formalin, embedded in paraffin blocks, and stained with hematoxylin and eosin for histological examination. The diagnoses were assessed according to the World Health Organization classification of thyroid malignancy, and Turin criteria were used for the diagnosis of PDTC (30). Immunohistochemical analyses were performed on serial sections 5 μm thick prepared from selected paraffin-embedded tissue with primary antibodies directed against the following proteins: thyroid peroxidase (TPO), thyroglobulin (Tg), NIS, and Ki67.
BRAF mutation
Screening for BRAF mutations in exon 11 and 15 was performed using the Sentosa NSCLC SQ Panel® CE-IVD kit (Vela Diagnostics, Hamburg, Germany) covering the main hot-spot region of the BRAF gene (but not complex nucleotide variants or fusions) (NM_004333.5; exons 11 and 15), as well as the following genes: KRAS (NM_033360.3; exons 2–4); NRAS (NM_002524.4; exons 2–4); EGFR (NM_005228.4; exons 18–21); PIK3CA (NM_006218.2; exons 10 and 21); KIT (NM_000222.2; exons 11, 13, and 17); CTNNB1 (NM_001904.3; exon 3); FGFR3 (NM_000142.4; exons 7, 9, and 14); PTEN (NM_000314.6; exons 5, 7, and 9); TP53 (NM_000546.5; exons 5, 7, and 8); and RET (NM_020975.5; exon 16). For 113 hot-spot mutations (SNV), the clinical sensitivity is 100% [confidence interval (CI) 95–100%], and the clinical specificity is 100% [CI 97.63–100%], with a reproducibility ≥99.99% [CI 99.96–100%], as reported in the Conformité Européenne In Vitro Diagnostic notice. Individual test acceptance requires a depth coverage >1000 × (for all 113 targeted hot-spot positions) to pass the quality control CQ check. The analyses were performed in a NF-EN_ISO15189_SH_REF02 certified medical laboratory (COFRAC No. 8-4000) according to the manufacturer's recommendation.
Tg and thyrotropin measurements
Tg was measured using a chemiluminescent immunoenzymatic “sandwich” assay (Access® Thyroglobulin; Beckman Coulter, Villepinte, France) with an analytical detection threshold of 0.1 ng/mL. Tg antibodies were measured using the Access® Thyroglobulin Antibody II assay (Beckman Coulter).
Serum thyrotropin (TSH) was measured using the Access hypersensitive TSH (hTSH) assay (Beckman Coulter, Fullerton, CA), with a reference range of 0.38–5.33 mIU/L and with an analytical detection threshold of 0.01 μIU/mL. Serum free triiodothyronine (fT3) and free thyroxine (fT4) were measured using the Access fT3 assay and the Access fT4 assay, respectively (Beckman Coulter), with reference ranges of 3.8–6.0 pmol/L for fT3 and 7.9–14.4 pmol/L for fT4.
Imaging
Fluorodeoxyglucose (18FDG) positron emission tomography/computed tomography (PET/CT) was performed using a Discovery 690 (General Electric Medical Systems, Waukesha, WI) 60 minutes after the injection of 4 MBq/kg of 18FDG and under conditions of normoglycemia. The maximum 18FDG uptake was defined as the maximum standardized uptake value (SUV) of the lesion with the highest uptake (SUVmax). PET Response Criteria in Solid Tumors (PERCIST) were used to define tumor metabolic response measuring the peak standardized uptake value corrected for lean body mass (SULpeak).
A RAI whole-body scan (WBS) and single photon emission computed tomography (SPECT)/CT were acquired one day after the administration of 185 MBq (5 mCi) of 123I, in the absence of any exogenous TSH stimulation, with a conventional NaI(Tl) gamma camera equipped with a 5/8″-thick crystal (Discovery NM/CT 670; GE Healthcare, Chicago, IL). A semi-quantitative analysis was performed on planar images in order to estimate the uptake of lesions. Correction for physical decay, geometric mean attenuation compensation, and correction for background activity were applied.
A three-phase CT scan of the thorax, abdomen, and pelvis was performed with helicoidal 64-b GE CT, 2.5 mm thickness, after the injection of 1.5 mL/kg of iodinated contrast medium, and acquisition at the neck artery (35 seconds after injection), thorax, and abdomen. Response Evaluation Criteria in Solid Tumors (RECIST) were used to establish morphological tumor response.
Real-time quantitative reverse transcription polymerase chain reaction
Total RNA was isolated from thyroid biopsies using a NucleoSpin RNA II kit (Macherey-Nagel, Düren, Germany). The quality of RNA preparations, based on the 28S/18S ribosomal RNA ratio, was assessed using the RNA 6000 Nano Lab-On-Chip (Agilent Technologies, Santa Clara, CA). Total RNA (0.5 μg) was reverse transcribed using RevertAid Premium Reverse Transcriptase (Fermentas; Thermo Fisher Scientific, Waltham, MA) and random hexamer primers in a total reaction volume of 20 μL of polymerase chain reaction (PCR) buffer according to the manufacturer's protocol for 30 minutes at 55°C. Real-time quantitative reverse transcription PCR was performed, as described previously (31). The primers and probes, designed with the Primer Express 1.5 program (Applied Biosystems, Foster City, CA), were as follows: NIS primers: sense, 5′-cca tcc tgg atg aca act tgg-3′; antisense 5′-aaa aac aga cga tcc tca ttg-3′, TaqMan fluorescent probe 5′-FAM-aga act ccc cac tgg aaa caa gaa gcc c-TAMRA; TG primers: sense 5′-agc agt ttc tgc gtg gga g-3′; antisense 5′-agc ggc gtc tct gat aga agc-3′, TaqMan fluorescent probe 5′-FAM-cgc ctg gcg gct cag tct acc tt-TAMRA; TPO primers: sense 5′-acg cct ctg cga ggt gc-3′, antisense 5′-tgc aaa tca ccg tcg agg-3′, TaqMan fluorescent probe 5′-FAM-tgc tga tcg gag gct tcg cag g-TAMRA; housekeeping gene PPIA primers: sense 5′-gtc aac ccc acc gtg ttc tt-3′, antisense 5′-gtg gtg tct ttg gga cct tgt-3′, TaqMan fluorescent probe 5′-FAM-agc tca aag gag acg cgg ccc a-TAMRA. Oligonucleotides were purchased from Eurofins Genomics (31). mRNA levels after dabrafenib/trametinib treatment were compared to those measured before treatment (t-test with a significance level of <0.05).
Patient
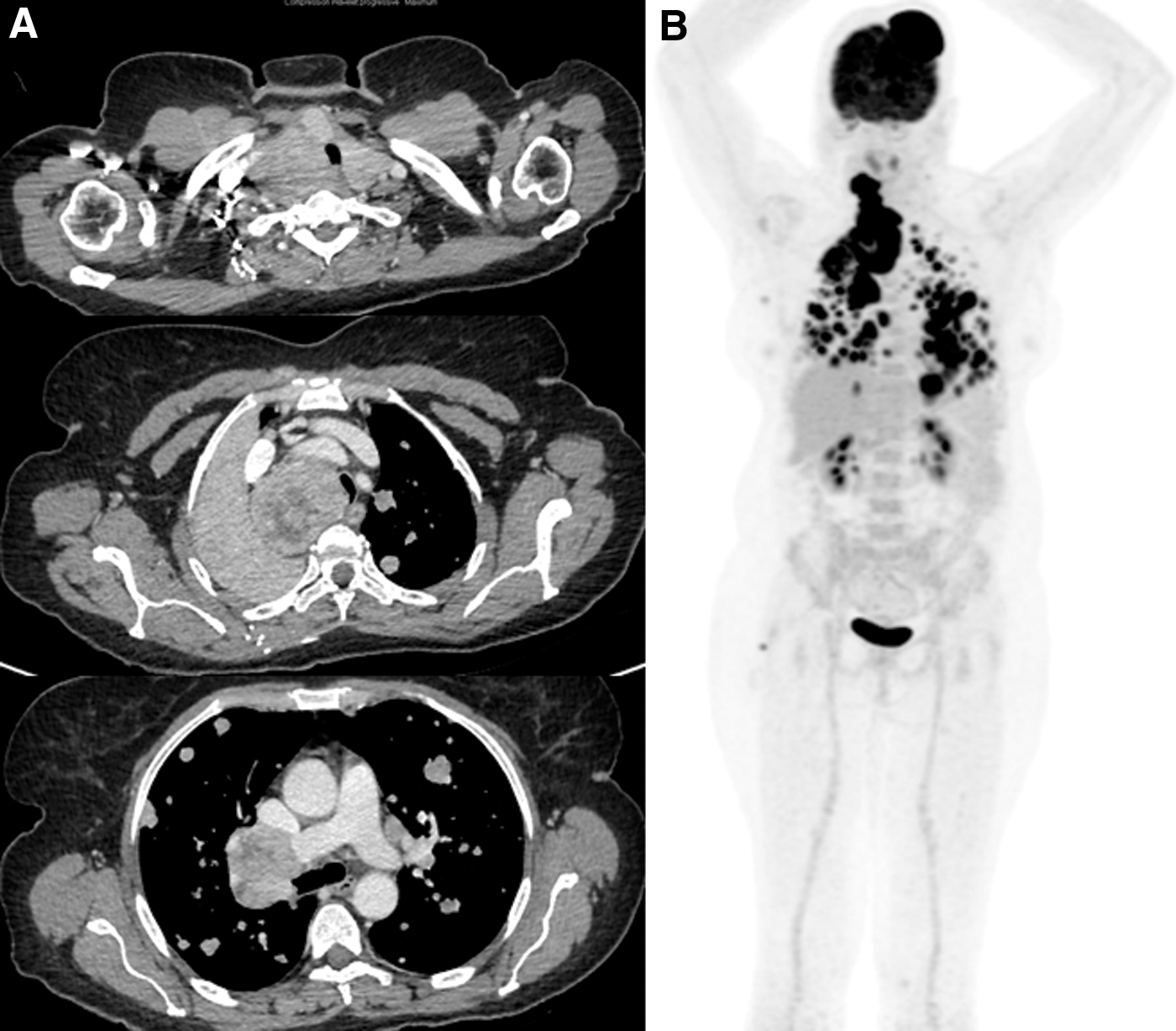
A 59-year-old woman was referred to Gustave Roussy for a locally invasive thyroid cancer diagnosed because of short breath with synchronous lung, mediastinal, and bone metastases. Due to local invasion with tracheal invasion, in a context of diffuse distant metastases, the primary tumor was considered non-resectable (Fig. 1). A primary tumor biopsy showed a PDTC, with a high mitotic count (Ki67: 10%). Immunochemistry was positive for Tg in 40% of the cells, positive for TTF1 and PAX8, and negative for TPO (<5%) and NIS. The initial TSH level was 0.32 mIU/L, with normal fT3 (5 pmol/L) and fT4 levels (9.2 pmol/L) and an elevated Tg level at 4660 μg/L. On baseline 18FDG PET/CT, SUVmax was 30.4 and SULpeak 21.7.
(
Due to tumor invasion of the trachea and of the primary right bronchus, the patient was considered at high risk of bleeding and was excluded from a treatment with an anti-angiogenic drug. In the context of a BRAFK601E mutation, known to confer constitutive activation of BRAF protein (and in the absence of mutations in any of the other genes tested by the panel described in the Methods section with a median depth coverage of 11,080 × ), the patient was treated with dabrafenib and trametinib. Dabrafenib was given at a dose of 150 mg twice a day and trametinib at a dose of 2 mg once daily.
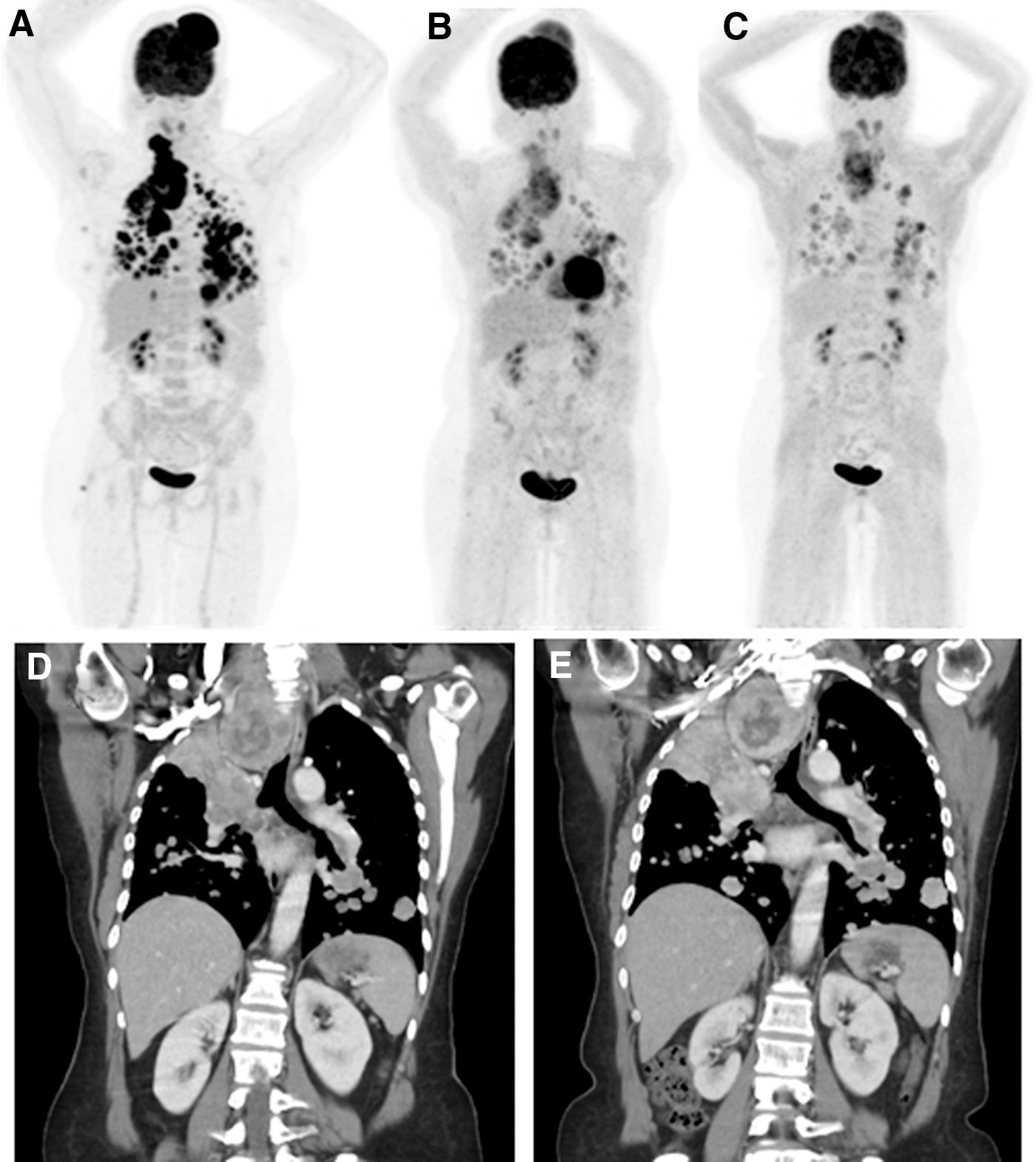
The patient was seen every 7–14 days for two months. An increase in Tg level was observed as soon as seven days after initiation of dabrafenib/trametinib, and it increased to 10-fold over baseline at four weeks (49,710 μg/L; Fig. 2). Grade 1 weight loss, asthenia, and tachycardia gradually developed and were considered to be secondary to hyperthyroidism, with fT3 increasing to 6.6 times its upper normal limit (40.5 pmol/L) and fT4 at 4.4 times its upper normal limit (57 pmol/L) six weeks after treatment initiation (Fig. 2). No other toxicity was observed. 18FDG PET/CT at one month after treatment initiation showed a PERCIST metabolic response, with a decrease of 82% in 18FDG uptake. 18FDG PET/CT at two months after treatment initiation showed stable metabolic disease compared to the 18FDG PET/CT performed one month after treatment initiation (Fig. 3), whereas CT evaluation showed stable disease based on RECIST criteria (Fig. 3).
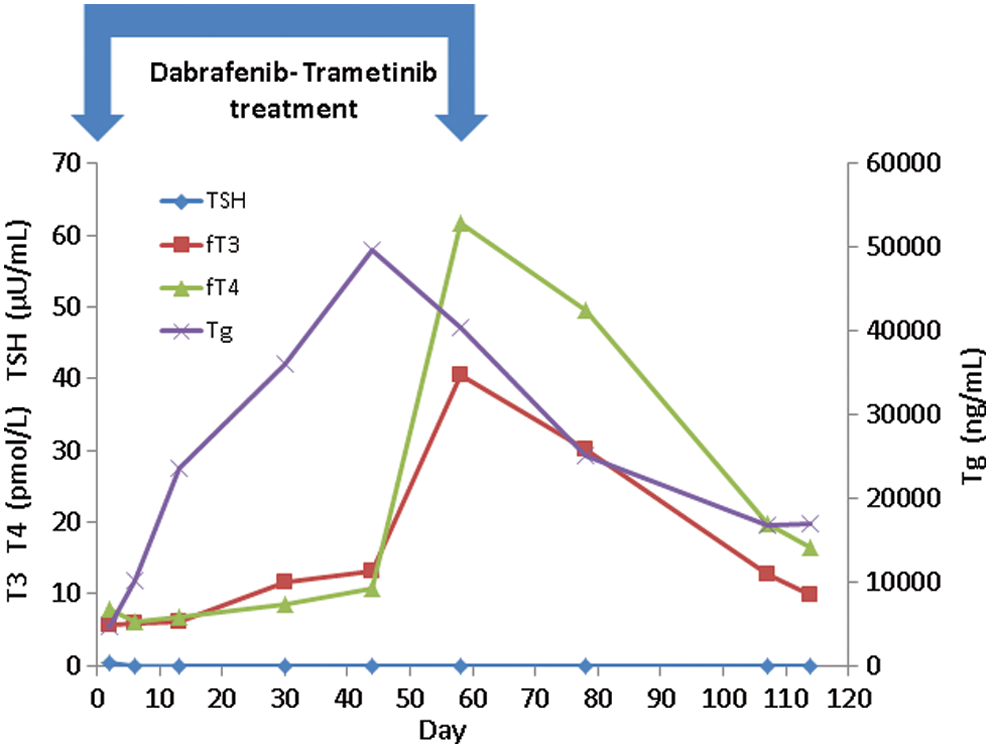
Free triiodothyronine (fT3), free thyroxine (fT4), and thyroglobulin (Tg) serum levels during follow-up. Color images are available online.
18FDG PET/CT (
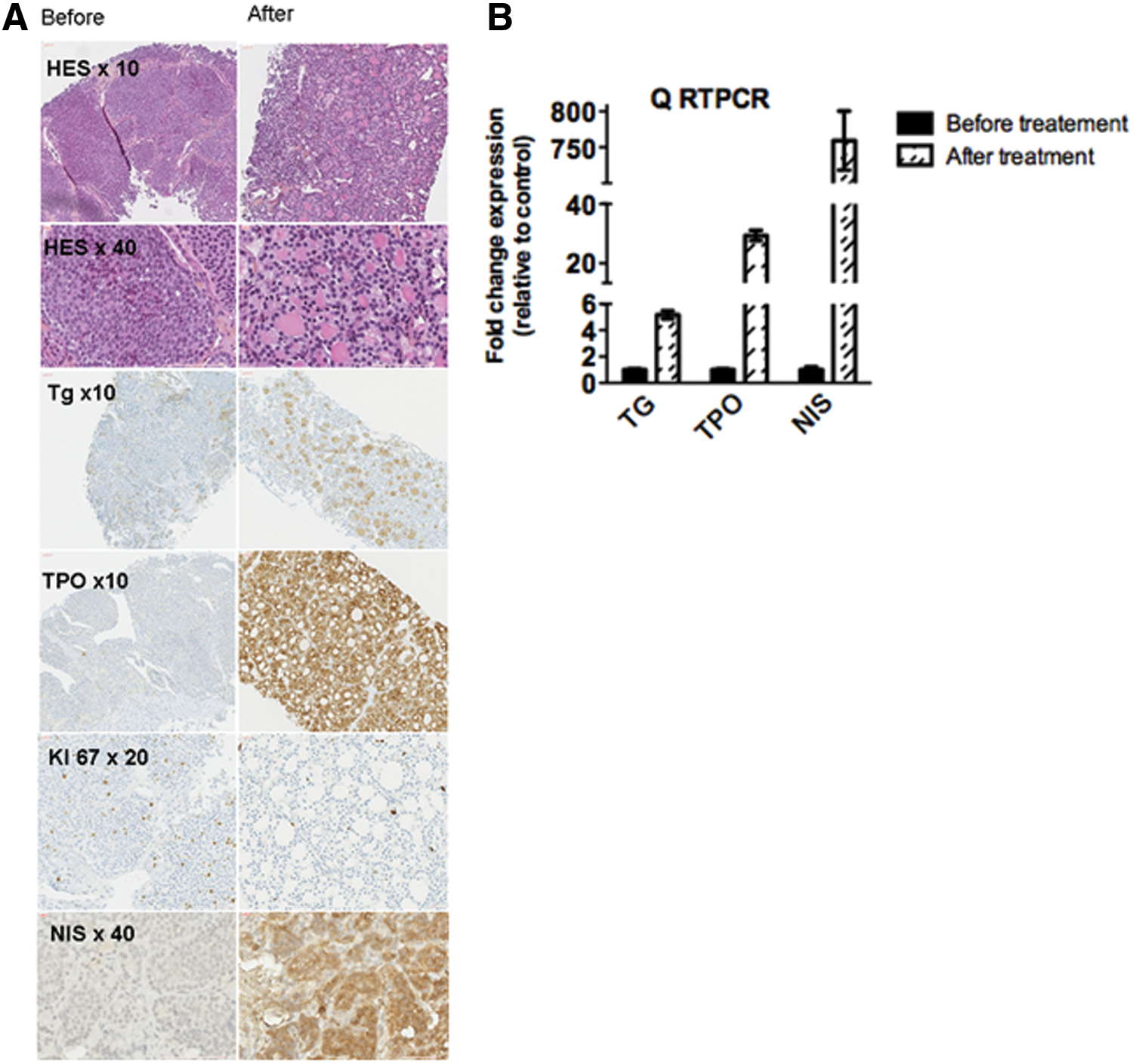
The biopsy from the primary thyroid tumor performed two months after initiation of dabrafenib/trametinib showed a more differentiated growth pattern of the carcinoma, with a microfollicular appearance and intraluminal colloid material. The mitotic activity decreased with a Ki67 < 5% compared to 10% at baseline. Immunohistochemistry (IHC) showed an increase in Tg and TPO expression and the appearance of NIS expression. mRNA levels of Tg increased by 5.1-fold (p < 0.0018), TPO by 29.3-fold (p < 0.0009), and NIS by 747.4-fold (p < 0.0012; Fig. 4).
(
The diagnostic WBS performed two months after initiation of dabrafenib/trametinib treatment, at a time when the patient was thyrotoxic and without any exogenous TSH stimulation, showed high RAI uptake in the lung, mediastinum, and skull metastases (Fig. 5).
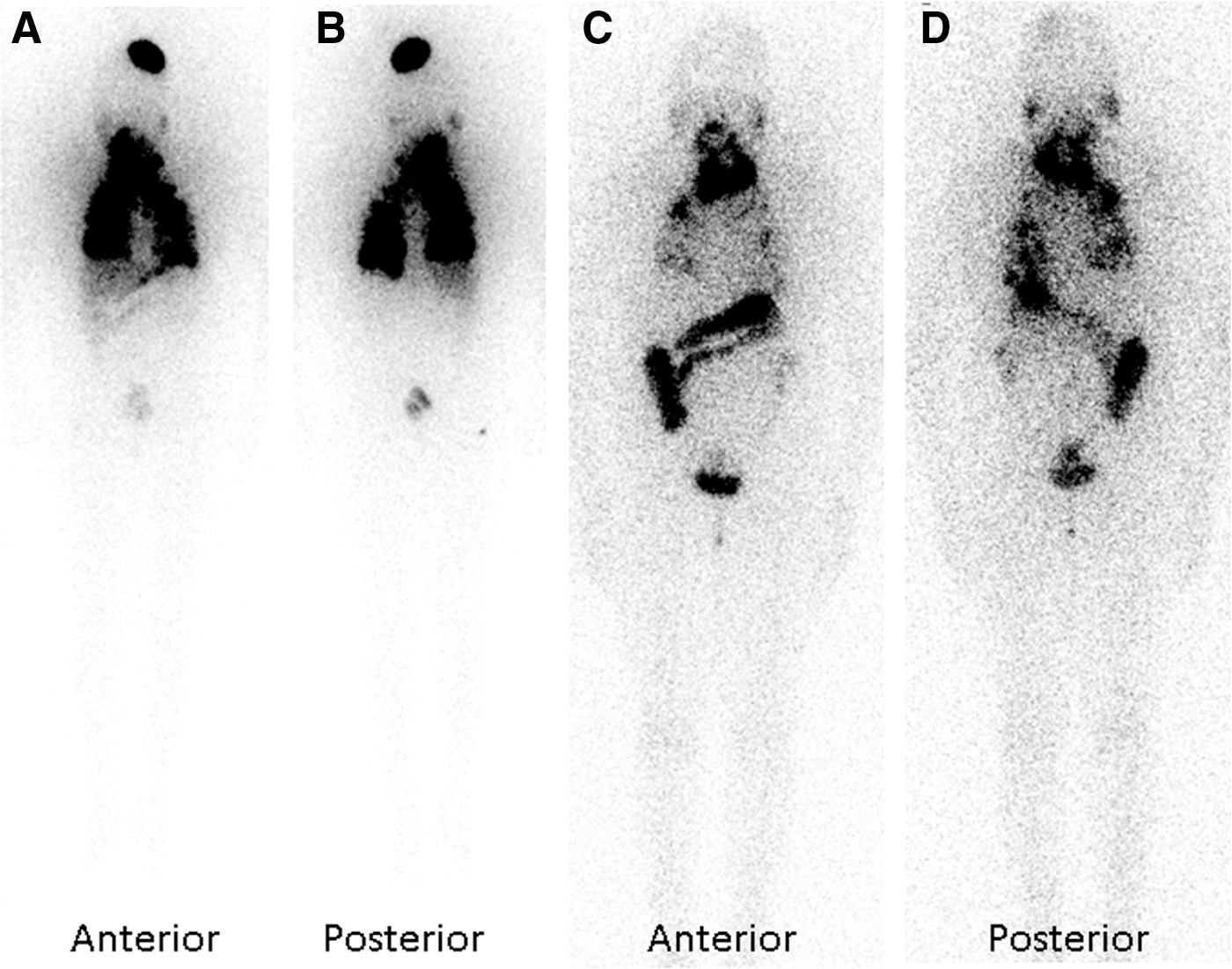
Diagnostic whole-body scan performed during dabrafenib/trametinib treatment (
However, at two months of treatment, the general status of the patient declined, with dyspnea, weight loss, and tachycardia, despite stable structural disease. These symptoms were attributed to thyrotoxicosis and led to discontinuation of the treatment. Despite RAI uptake by the tumor, a high activity of RAI was not administered because of the potential risk of a transient increase in tumor size following RAI therapy that may have induced an acute airway distress in this patient who did not want to take any risk of tracheotomy, and because of a high risk of dysphagia and impaired swallowing.
After discontinuation of the systemic treatment, the patient's symptoms indeed resolved within a month. Blood levels of fT3 and fT4 normalized, the TSH level became detectable, and the serum Tg level decreased to baseline levels. A repeat WBS with 185 MBq (5 mCi) 123I and without any exogenous TSH stimulation showed a dramatic decrease of RAI uptake of the tumor by 90%.
Discussion
BRAFV600E is the most frequent BRAF mutation detected in DTC. It represents >95% of all BRAF mutations (6 –9,32). Among rare alterations in exon 15 of BRAF, the BRAFK601E mutation is the most frequent, representing 64% of rare BRAF mutations and 3% of all BRAF mutations (32). In thyroid cancer, this mutation was described as occurring almost exclusively in PTC with low-risk clinicopathologic features. On the other hand, BRAF mutations other than BRAFV600E have been described as exhibiting RAS-like behavior, consistent with observations of the occurrence of BRAFK601E mutations in the follicular variant of PTC (33). The patient described here did not suffer from a low-risk thyroid cancer but presented with locally advanced disease. The initial oligosymptomatic presentation, despite a large tumor burden, suggests a slow occurrence of her tracheal compression and a slow tumor growth.
She was deemed to be at high risk of bleeding, given the tracheal and bronchial invasion, one of the side effects feared with potent antiangiogenic drugs (34). The association of dabrafenib and trametinib has not been shown to be superior to dabrafenib alone in thyroid cancer (12), but in melanoma patients, the combination therapy has been shown to be more efficient and better tolerated (15 –17). Tumor responses in BRAFK601E -mutated melanoma patients have been reported with trametinib alone (35,36). The better tolerance of the dabrafenib/trametinib combination in patients with melanoma led to the administration of the two drugs in this case, despite the RAS-like behavior of the BRAFK601E mutation present in the patient's tumor.
No morphological tumor response was observed, but a clear redifferentiation was observed, with clinical, biochemical, metabolic, and histological effects. The clinical and biological effects included thyrotoxicosis occurring as early as day 7 after initiation of the therapy with a dramatic increase in blood levels of thyroid hormones and Tg at day 45. The increase in serum Tg, a sign of tumor redifferentiation, has been described with dabrafenib and with vemurafenib, but has never been described with antiangiogenic drugs (VEGFR) (4). These redifferentiation effects were transient and disappeared rapidly after withdrawal of dabrafenib/trametinib treatment. The metabolic effects included both a decrease in 18FDG uptake, one of the main prognostic criteria in refractory RAI patients, and a high RAI uptake, which disappeared after dabrafenib/trametinib withdrawal (37). Finally, the histological effects included changes in the histology, with a decrease in Ki67 labeling index and an increase in NIS, Tg, and TPO expression at both the protein and mRNA levels.
Despite this redifferentiation effect, a high activity of RAI was not administered to the patient. Treatment of goiter with RAI can induce a transient increase in goiter size without clinical impact in up to 17% of patients (38). However, in this patient, given the tracheal compression, she was considered to be at risk for acute respiratory failure following RAI treatment. In that case, a tracheotomy with a long tracheal prosthesis would have been necessary. Even though the risk can be considered low and has to be balanced with the natural history of the underlying disease that will lead to airway distress and death in the absence of treatment, this decision was prompted by the refusal of the patient to consider an intervention that could compromise her airway. The observed differentiation did not result in a clear benefit for the patient. Unfortunately, the combination therapy did not result in a tumor response as defined by RECIST. Tumor responses during dabrafenib/trametinib treatment have been reported in 50% of BRAFV600E RAI-refractory DTC and in 65% of anaplastic thyroid cancers (12,39). Targeting tumors with RAS or RAS-like mutations remains a challenge. Trametinib has shown efficiency in BRAFK601E melanoma patients. However, to the authors' knowledge, there are no data on single therapy with trametinib in RAS or RAS-like mutated RAI-refractory DTC patients. On the other hand, redifferentiation has been described with trametinib alone in patients without tumors harboring the BRAFV600E mutation (40). Thus, it must be acknowledged that there was no strong rationale for choosing combined BRAF and MEK inhibition in this patient other than limited treatment options and a perhaps a more limited toxicity profile. The observed redifferentiation effect might have been related to the combination of the BRAFK601E mutation, which is a RAS-like mutation with a low MAPK output (compared to the BRAFV600E mutation), and a strong inhibition of the MAPK pathway with the dabrafenib/trametinib combination.
In conclusion, the patient presented here showed redifferentiation of a tumor harboring a BRAFK601E mutation under dabrafenib/trametinib treatment, with an increase in thyroid hormone production and increased expression of NIS, Tg, and TPO at both the mRNA and the protein levels. Concurrently, RAI uptake increased and FDG uptake decreased. Mechanisms leading to tumor cell redifferentiation rather than to tumoricidal and antiproliferative effects still need to be elucidated.
Footnotes
Author Disclosure Statement
S.L. has a research grant from Novartis. L.L. has participated in advisory boards for Novartis. For all other authors, no competing financial interests exist.