
Abstract
Background:
Increased public attention toward health and quality-of-life issues has led to more intensified screening for various medical conditions, including hypothyroidism. A falling serum thyrotropin (s-TSH) at initiation of levothyroxine (LT4) treatment has been reported in the United Kingdom between 2001 and 2009, indicating a falling TSH threshold, which may lead to less benefit from therapy and possibly overtreatment. The aim of this study was to investigate changes in s-TSH threshold used by general practitioners to initiate LT4 therapy between 2001 and 2015 in Copenhagen.
Methods:
Retrospective analysis was conducted of all s-TSH measurements between 2001 and 2015 performed at the general practitioners' joint laboratory merged with The Danish Register of Medicinal Products Statistics and The Danish National Patient Registry. For each year, both the median s-TSH at therapy initiation and the estimated treatment threshold were calculated from all s-TSH measurements performed in that year, representing the s-TSH level where the estimated probability of starting LT4 therapy was 50%.
Results:
A total of 929,684 individuals with 2,975,277 s-TSH measurements were included in the calculations. The size and composition of the study population remained virtually unchanged. During the study period, the number of performed s-TSH measurements increased from 110,886 to 292,911 (164%), and the number of patients initiating LT4 therapy increased from 786 to 1825 (132%), though this was comparably unchanged from 2010 to 2015. The median s-TSH at therapy initiation decreased from 10 mIU/L (interquartile range 5.2–29.7 mIU/L) in 2001 to 6.8 mIU/L (interquartile range 5.1–11 mIU/L) in 2015, while the estimated treatment threshold decreased from 28.3 mIU/L [confidence interval 21.0–40.2 mIU/L] in 2001 to 14.2 mIU/L [confidence interval 12.0–18.0 mIU/L] in 2007. In 2015, 25% of patients started LT4 therapy with s-TSH ≤5 mIU/L, and during the entire period, 50% of patients started therapy with a single s-TSH measurement >5 mIU/L.
Conclusions:
This study performed on a sizeable primary care population demonstrates a considerable fall in the threshold for initiating LT4 therapy in hypothyroid patients. This increases the risk of futile treatment as well as overtreatment.
Introduction
In recent decades, there has been increasing focus on health and quality-of-life aspects in the management of various disease entities. This has led to a more pronounced anticipation of early diagnosis and subsequent treatment of diseases such as hypothyroidism in the patient community. Hypothyroidism is a common endocrine disease characterized by a wide range of symptoms caused by an insufficient production of thyroid hormones (1). However, classical hypothyroid symptoms are not specific to the condition and may be related to other diseases and conditions (2). It is likely that patients initiating levothyroxine (LT4) treatment as a result of symptoms not related to hypothyroidism will only have limited, if any, benefit from LT4 therapy, while they risk adverse events.
The European Thyroid Association (ETA) and the American Thyroid Association (ATA) recommend LT4 to patients <70 years with overt hypothyroidism serum thyrotropin (s-TSH) of >10 mIU/L or a s-TSH of 4–10 mIU/L combined with a low level of serum thyroxine (s-T4). Treatment is recommended in subclinical hypothyroidism (s-TSH above the normal range with s-T4 within reference limits) if patients exhibit symptoms, are pregnant, or are attempting to become pregnant. In both subclinical and overt hypothyroid patients, the ETA recommends a s-TSH of 0.4–2.5 mIU/L throughout the gestation period (3). In elderly patients, a more conservative approach is recommended (4,5), though no randomized controlled trials exist on cardiovascular outcomes in subclinical hypothyroidism among the elderly (6). Very recent data underline that no improvement in quality of life has been documented when treating subclinical hypothyroidism in the elderly (7). The ETA and ATA guidelines recommend that an elevated s-TSH should be confirmed within two to three months before initiating substitution therapy in order to take spontaneous fluctuations in thyroid function into account (4,5).
Taylor et al. reported a trend toward a lower s-TSH (from a median of 8.7 mIU/L in 2001 to a median of 7.9 mIU/L in 2009) upon initiating LT4 treatment in the United Kingdom, which may indicate a reduction in the treatment threshold and, furthermore, an increased risk of overtreatment (8). Additionally, Cerqueira et al. demonstrated a doubling in the use of LT4 replacement therapy in Denmark from 1997 to 2008 (9). LT4 has become the most and the third most prescribed medication in United States and the United Kingdom, respectively (10). Given the risks associated with overtreatment, it is imperative that only patients actually benefitting from LT4 therapy receive medication.
Both the incidence of therapy initiation and the level of s-TSH at therapy initiation are sensitive to increased monitoring. Even if the treatment threshold stays the same, increased monitoring will find more people with a s-TSH above the reference range. Assuming that patients with a high s-TSH and many symptoms (11) are already being discovered promptly, then any further patients discovered through increased use of s-TSH measurement with an elevated s-TSH and initiating LT4 therapy will inevitably lower the median s-TSH at the start of therapy, regardless of patients not starting LT4 therapy despite an elevated s-TSH.
Hence, the treatment threshold is to be estimated directly and independently of the increasing monitoring by including both s-TSH measurements that lead to LT4 therapy and those that do not. Thus, this study calculated the estimated treatment threshold (ETT), which is robust against changes in monitoring and thus useful in epidemiological studies when investigating changes in treatment threshold during changing case-finding intensity. However, ETT is difficult to utilize in the clinical setting, unlike the median s-TSH at the start of therapy, which is more easily interpreted but vulnerable to changes in s-TSH monitoring.
The primary aim was to investigate changes in the TSH threshold when initiating LT4 therapy in hypothyroidism among general practice in Copenhagen between 2001 and 2015, presented as both changes in the ETT and as final s-TSH before therapy.
Methods
In Denmark, citizens have direct access to primary care and hospital care at no cost. Approximately 98% of Danish citizens are listed with a general practitioner (GP), and Danish GPs are gatekeepers to more specialized patient care by specialized consultants as well as in- and outpatient hospital care.
In the Copenhagen Municipality and former Copenhagen County, with approximately 1.2 million inhabitants, there was only one laboratory serving GPs from 2000 to 2015, the Copenhagen General Practitioners' Laboratory (CGPL). The CGPL served a total of 739 GPs in 567 practices (2010) with a broad range of blood tests and clinical physiological tests.
The constitution of the population serviced by the CGPL remained virtually unchanged with regard to size, age, and sex distribution between 2001 and 2015. The Copenhagen Primary Care Laboratory (CopLab) database contains all results from the CGPL from July 1, 2000, to December 31, 2015.
All Danish citizens are registered with a unique civil registration number, which enables person-level linkage across nationwide registers. (12) The present study linked the relevant data from the CopLab database to: (i) The Danish Civil Registration System (12), which provides information on vital status; (ii) The Danish National Patient Register (NPR) (13), which contains recorded information on all hospital contacts in Denmark since 1977, with individual diagnoses registered according to the World Health Organization (WHO)'s International Classification of Diseases (ICD-10 system) (14); and (iii) The Danish National Prescription Registry (DNPR) (15), which contains data on prescribed drugs sold in Danish pharmacies since 1994, including information on person-level dispensed prescriptions and prescriber information. All prescriptions from outpatient clinics, GPs, and after hospital admissions in Denmark are completed at community pharmacies. Medications in this study were identified by the Anatomical Therapeutic Chemical Classification codes. (16) Iodine fortification in Denmark did not change between 2001 and 2015.
Inclusion criteria
Inclusion criteria were all s-TSH measurements included in the CopLab Database (Fig. 1).
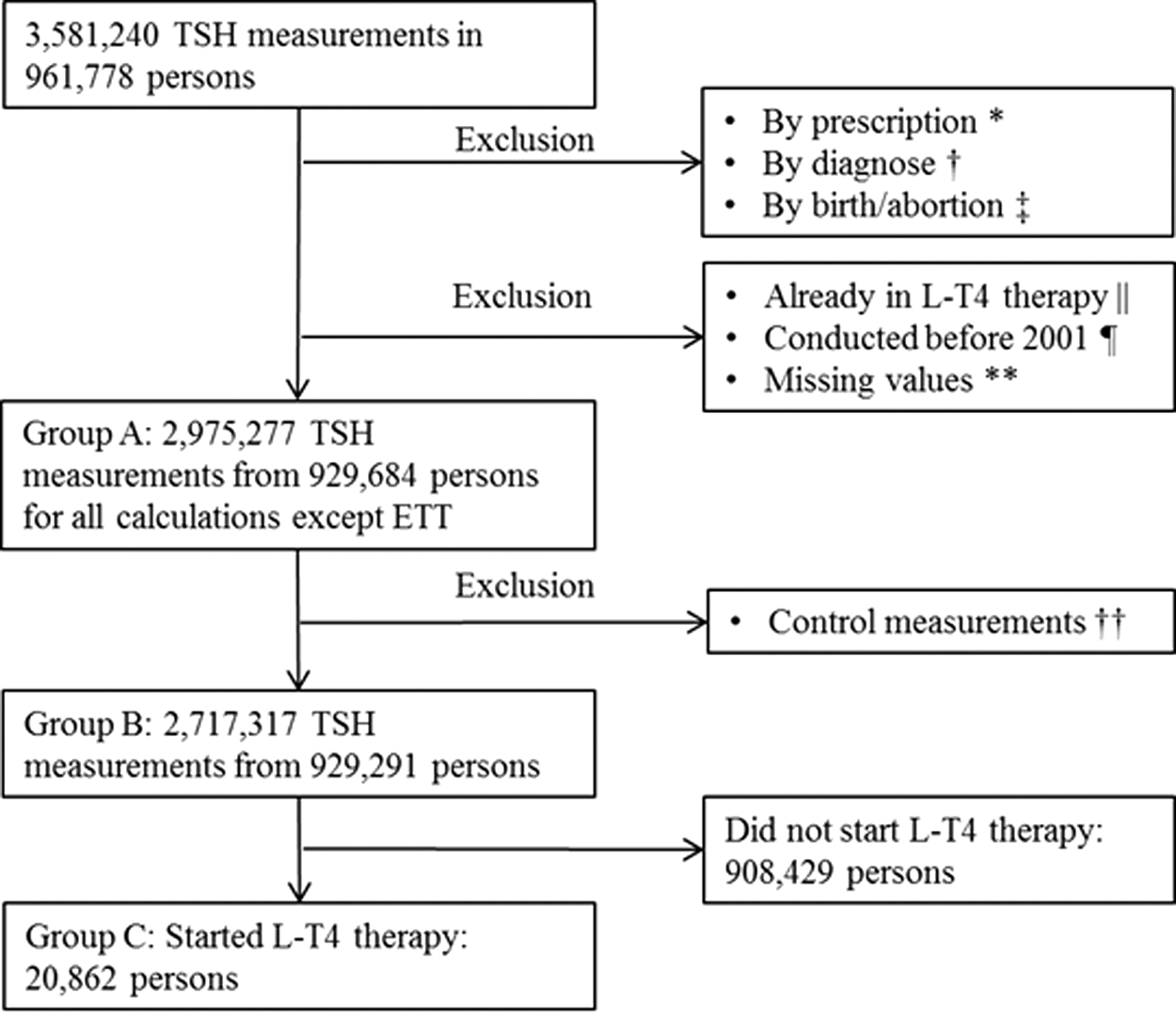
Flow chart of the number of serum thyrotropin (s-TSH) measurements and patients in the study. Measurements and patients may belong to multiple exclusion criteria. *Patients taking the following medication: amiodarone, lithium, propylthiouracil, thiamazol, carbimazol, monoclonal antibodies, and protein kinase inhibitors: 86,733 measurements and 2981 persons. †Patients having a previous diagnosis of hyperthyroidism, thyroid cancer, or pituitary disease: 133,818 measurements and 8631 persons. ‡Patients who had an abortion or birth within 12 months before or after s-TSH measurement: 11,131 measurements and 1452 persons. ||Patients already on levothyroxine (LT4) therapy: 356,504 measurements and 14,108 persons. ¶Measurements conducted before 2001: 20,432 measurements and 3262 persons. **Missing values: 31,022 measurements and 2260 persons. ††If a control measurement belonged to a measurement with a missing value, both measurements were excluded, sometimes resulting in a person being excluded from the study.
Exclusion criteria
Exclusion criteria were all s-TSH measurements conducted before 2001. Measurements from individuals with a current or previous diagnosis of hyperthyroidism (ICD-10 = DE05.0–9), thyroid cancer (ICD-10 = DE73.9), or pituitary disease (ICD-10 = DE23.0–9) were excluded (Fig. 1). s-TSH measurements conducted within six months after a dispensed prescription of thyroid-interfering drugs (amiodarone, lithium, propylthiouracil, thiamazole, carbimazole, monoclonal antibodies, and protein kinase inhibitors) were also excluded. Also, all s-TSH measurements within 12 months before or after a registered birth (ICD-10 = DZ33.8) or abortion (ICD-10 = DO03.0–9) were excluded. To omit all patients already under treatment for hypothyroidism, all measurements from patients with a redeemed LT4 prescription within the previous three years of each s-TSH measurement were excluded. Since guidelines recommend at least two s-TSH measurements before initiating LT4 therapy, due to a tendency of spontaneous normalization of s-TSH, all s-TSH measurements were excluded for which another measurement was present in the four months after, which was estimated to be sufficient time for a confirmatory s-TSH measurement. Inclusion of these control measurements would have artificially raised the ETT. In total, 257,960 control s-TSH measurements were removed by this criterion, retaining 2,717,317 measurements for analysis.
s-TSH analyses
s-TSH was determined in serum by the commercially available ADVIA Centaur/CentaurXP s-TSH method (Bayer/Siemens, Tarrytown, NY). The results are traceable to the WHO reference material IRP 80/558. The s-TSH assay was subject to external quality control through participation in the Labquality external quality assessment service (Helsinki, Finland). The results (n = 282) from Labquality through the entire study period (2003–2015) confirmed the reliability of the assays, and the results from CGPL deviated <12% from the method mean in >95% of the results. The normal range reported to GPs from CGPL was 0.2–5.0 mIU/l for s-TSH, though 0.4 mIU/l is utilized for treatment indication cutoff (4). Measurements ≥10 mIU/L were reported without decimals. s-TSH measurements were reported with a lower (<0.02 mIU/L) and upper (>135 or >150 mIU/L) limit. After performing a sensitivity analysis on the primary outcome, the observations outside the report limits were included with their value set to the value of the limit.
Definition of hypothyroidism
The Danish and European guidelines recommend LT4 therapy if s-TSH is >10 mIU/L in adults <70 years. regardless of s-T4 and symptoms, and this study divided patients according to s-TSH at LT4 initiation into the following groups: s-TSH <0.4, 0.4–2.5, 2.5–5.0, 5.0–10, and >10 mIU/L (5).
LT4 therapy initiation
A s-TSH measurement was defined as having initiated LT4 therapy if it was the closest observation prior to a first redeemed prescription and the prescription was within six months of blood sampling. Patients were considered to have stopped therapy if there was >36 months between redeeming an LT4 prescription and the ensuing blood sample. Thus, patients could have more than one initiation of therapy.
Statistical analyses
The ETT is defined as the estimated s-TSH value, where it was equally likely that a person would start LT4 therapy or not within each year, calculated from all s-TSH measurements conducted each year at the CGPL and information on prescriptions from the DNPR. The probability of therapy initiation within a year for a given level of s-TSH was modeled as a logistic function on the natural logarithm of the s-TSH level. The model parameters were estimated by generalized estimating equations (GEE) to account for dependency between measurements from the same subject (17). The confidence intervals (CI) for these treatment threshold estimates were calculated using bootstrap.
The median s-TSH level at therapy initiation and interquartile range (IQR) were calculated using only the measurements defined as having initiated LT4 therapy.
Comparisons of rates or counts between 2001 and 2015 were conducted using Poisson regression using GEE. p-Values <0.05 were considered significant. All statistics analyses were conducted on servers at Statistics Denmark using the statistical programs SAS® v9.4 (SAS Institute, Cary, NC) and R v3.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 929,684 individuals with 2,975,277 s-TSH measurements were included in the study (Table 1). The median s-TSH in the data set changed from 1.3 mIU/L (IQR 0.9–2 mIU/L) in 2001 to 1.6 mIU/L (IQR 1.1–2.2 mIU/L) in 2015. The median ages were 53 years (IQR 36–70 years) and 55 years (IQR 40–68 years) in 2001 and 48 years (IQR 32–66 years) and 54 years (IQR 38–68 years) in 2015 for women and men, respectively. The female/male ratio of patients starting LT4 therapy in the study remained approximately six.
Characteristics of Included s-TSH Measurements, Individuals, ETT, and Patients Starting LT4 Therapy
ETT is defined as the estimated s-TSH value, where it was equally likely that a person would start LT4 therapy or not within each year. s-TSH values >10 mIU/L are reported without decimals. The age of a person was defined at the age at the first s-TSH measurement within each year.
All included measurements and individuals (Fig. 1, Group A).
Measurements excluding controls in all included individuals (Fig. 1, Group B).
Patients starting LT4 therapy (Fig. 1, Group C).
s-TSH, serum thyrotropin; ETT, estimated treatment threshold; LT4, levothyroxine; IQR, interquartile range; CI, confidence interval.
During the study period, 310 patients had an intermission in LT4 therapy and started therapy twice, while eight patients had two intermissions and were considered to have started LT4 therapy three times. Thus, 20,862 unique individuals started LT4 therapy 21,188 times from 2001 to 2015.
The median s-TSH level leading to the subsequent institution of LT4 therapy decreased gradually from 10 mIU/L (IQR 5.2–29.8 mIU/L) in 2001 to 6.8 mIU/L (IQR 5.1–11 mIU/L) in 2015 (Table 1). During the same period, the number of patients initiating LT4 therapy increased from 786 in 2001 to 1825 in 2015. The median s-TSH that led to LT4 therapy among patients >80 years of age decreased from 13.5 mIU/L (IQR 6.5–36 mIU/L; n = 92) in 2001 to 7.3 mIU/L (IQR 5.8–12 mIU/L; n = 91) in 2015.
The ETT of s-TSH for LT4 therapy initiation was 28.3 mIU/L [CI 21.0–40.2 mIU/L] in 2001 falling to 14.2 mIU/L [CI 12.0–18.0 mIU/L] in 2007 where it remained relatively unchanged for the rest of the study period (Fig. 2). A trend shift was observed between the period 2001–2006 and the later period 2007–2015. In the former period, the ETT gradually fell to 21.1 mIU/L [CI 16.6–28.3 mIU/L] in 2006, and in the latter period, the ETT remained constant after an initial drop to 14.2 mIU/L [CI 12.0–18.0 mIU/L] in 2007.
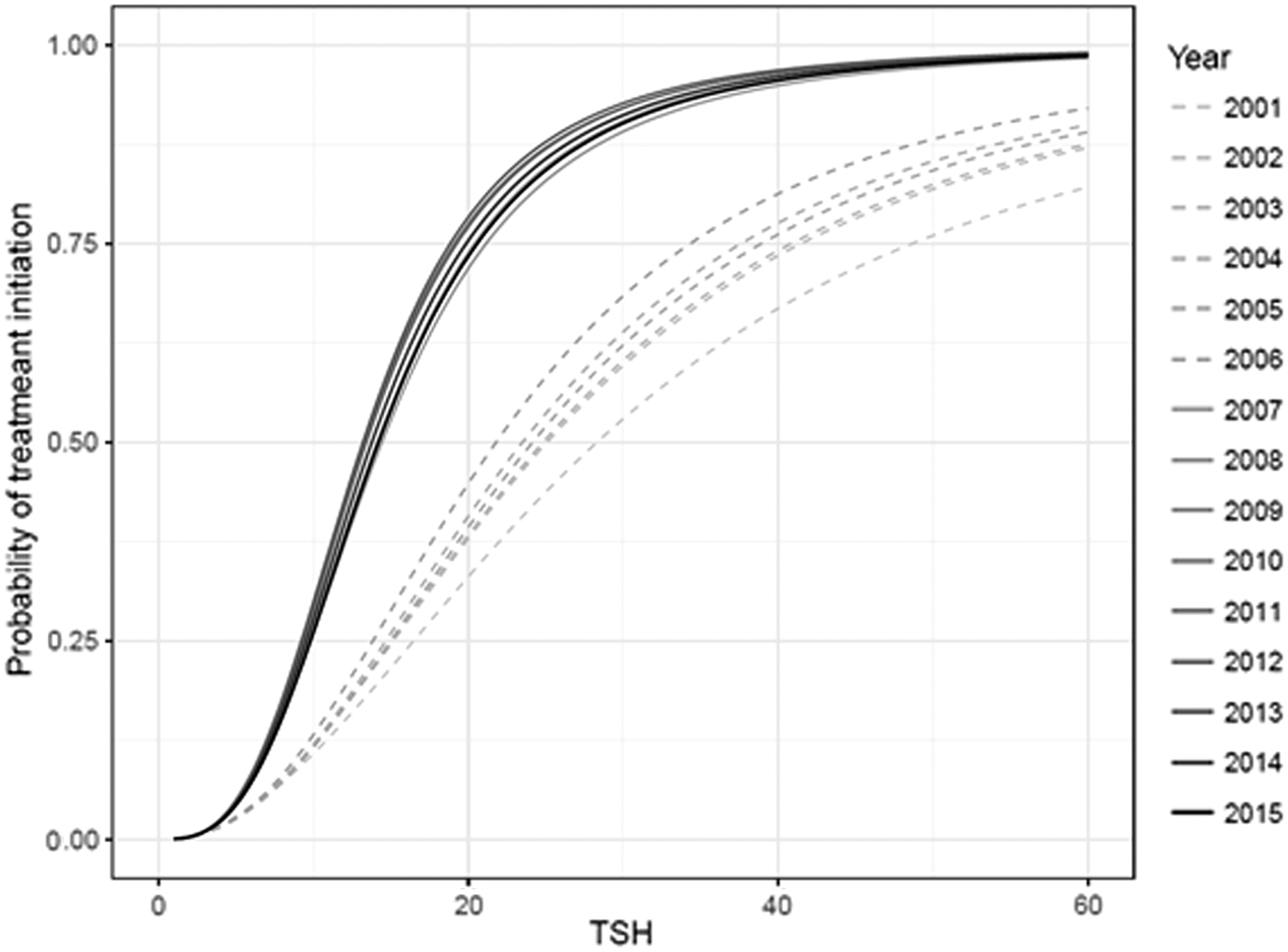
Estimated probability of starting LT4 therapy as a function of s-TSH. The estimated treatment threshold (ETT) is located at the 0.50 value on the y-axis.
Changes in the number of patients initiating LT4 therapy in a given s-TSH interval are shown in Table 2 and Figure 3. The percentage of patients initiating LT4 therapy with s-TSH levels >10 mIU/L decreased from 50% in 2001 to 26% in 2015, while patients with a s-TSH interval of 5–10 mIU/L starting therapy increased from 26% in 2001 to 49% to 2015 (p < 0.001). The percentage of patients starting LT4 therapy with a s-TSH of 2.5–5 mIU/L increased from 5% to 13% between 2001 and 2015. Subgroup analyses of patients in this s-TSH interval revealed that 29% were women aged 18–40 years in 2001, while this percentage increased to 49% in 2015.
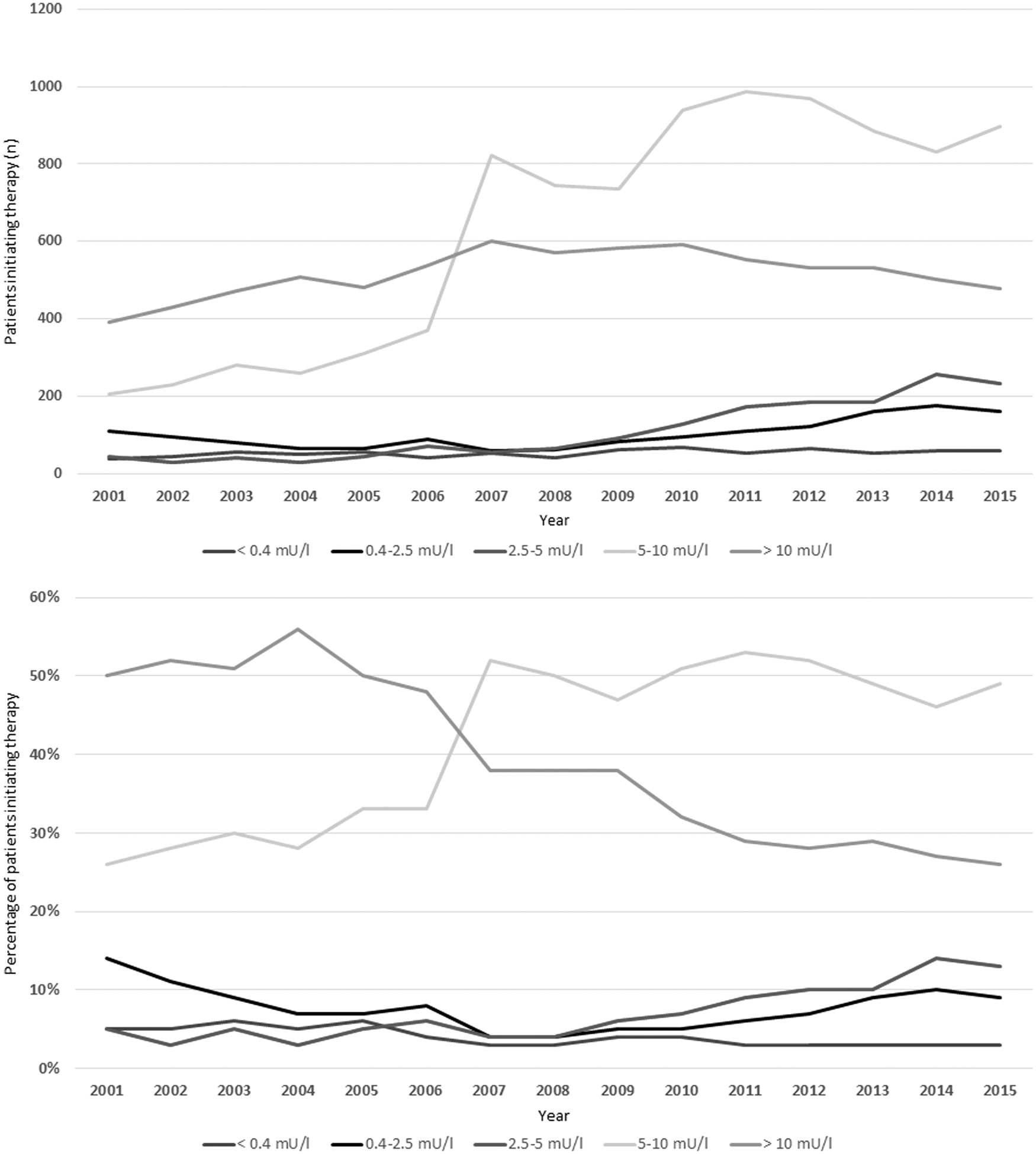
Patients initiating therapy each year according to s-TSH group (Table 2) presented as number of persons (upper graph) and percentage (lower graph).
Number of Patients Initiating LT4 Therapy Grouped by Last s-TSH Before Therapy
Of last s-TSH before therapy.
The number of individuals with a s-TSH measurement increased significantly from 99,041 in 2001 to 243,941 in 2015 (p < 0.001), corresponding to an increase in conducted s-TSH measurements from 110,886 in 2001 to 292,911 in 2015 (Fig. 4). Of note, the number of prescriptions did not increase further from the 2010–2011 level, while the number of s-TSH measurements continued to increase during the entire period.

Total number of s-TSH measurements, persons tested, and number of patients initiating LT4 therapy each year. Light- and dark-gray bars = persons examined and s-TSH measurements (left axis). Black line = number of new LT4 prescriptions (right axis).
The number of analyzed s-TSH measurements >5 mIU/L from each unique individual prior to instituted LT4 therapy fluctuated slightly during the study period, without showing any trend. Between 2001 and 2015, the percentage of LT4 prescriptions preceded by a single s-TSH measurement >5 mIU/L was 50%, varying between 45% and 58% of cases, and only between 26% and 39% of prescriptions were preceded by two or more s-TSH measurements above 5 mIU/L.
Discussion
A decrease in treatment threshold is reported, expressed as a significant decrease of the ETT between 2001 and 2015 from 28.3 to 13.9 mIU/L and a corresponding fall in s-TSH at treatment initiation from a median of 10 mIU/L in 2001 to a median of 6.8 mIU/L in 2015. The latter is in agreement with the findings by Taylor et al. in the United Kingdom, where a decrease in median s-TSH at therapy initiation from 8.7 mIU/L in 2001 to 7.9 mIU/L in 2009 was reported (8). This change is even more pronounced in the current study.
While the decrease in s-TSH at therapy initiation is seen over the whole study period 2001–2015, the ETT was relatively stable from 2007 onward. This suggests that development in s-TSH at therapy initiation from 2007 to 2015 may be heavily influenced by an increased case-finding effort.
During the study period, the number of LT4 prescriptions increased by 130%, which is in accordance with a Danish study by Cerqueira et al., reporting an increasing number of LT4 prescriptions in Denmark from 1997 to 2008 (9), and the study by Taylor et al., describing an increasing rate of LT4 prescriptions among British GPs (8), while in the United Kingdom and the United States, LT4 became the third and most prescribed medication in 2016, respectively (10).
Between 2006 and 2007, a remarkable change was observed for the ETT, the level of s-TSH at treatment initiation, and the number of patients starting LT4 therapy with a s-TSH between 5 and 10 mIU/L. The likely explanation is that in December 2006, the CGPL implemented a mandatory measurement of thyroid peroxidase antibodies (TPO-antibodies) if s-TSH was >5 mIU/L and free thyroxine was normal, thereby increasing the attention on mild hypothyroidism. Symptoms combined with elevated TPO-antibodies may have swayed more GPs into prescribing LT4 treatment, despite patients having a s-TSH <10 mIU/L. However, the ETA guidelines only recommend using TPO-antibodies for investigating the cause of hypothyroidism and not for the decision to start treatment (5).
The continuously increasing number of conducted s-TSH measurements from 2001 to 2015 may have led to increased findings of clinical and mild hypothyroidism, hereby leading to an increase in the annual LT4 prescription rate. Since ETT did not change from the 2007 level, these data suggest that the increase in LT4 prescription rate from 2007 onward originates primarily from early discovery by increased s-TSH screening. The prescription rate leveled out in 2010, while the median s-TSH at therapy initiation continued to decline thereafter, which is similar to the findings by Taylor et al. who reported that the prescription rate leveled out in 2006 in the United Kingdom, while the median s-TSH at therapy initiation continued to decline (8). This may be explained by the early discovery of hypothyroidism and prompt initiation of LT4 therapy before further the development of overt hypothyroidism and an increase in s-TSH.
The fact that the rate of new prescriptions leveled out in 2010 while the number of s-TSH measurements continued to increase throughout the period suggests that few hypothyroid patients remain undiagnosed. Theoretically, diagnosing and treating most of all hypothyroid patients each year would decrease median s-TSH of all conducted measurements. However, this cannot be documented because the mandatory iodine fortification of salt initiated in 2000 in Denmark increased s-TSH in the general population (Table 1) (18).
The benefits of the increased prescription rate of LT4 for mild hypothyroidism (Table 2) are uncertain. The risks associated with a s-TSH below the reference interval were described in a Scottish study of 17,684 patients on LT4 therapy, where the authors reported an increased risk of cardiovascular problems and osteoporotic fractures in patients with suppressed s-TSH (19). This risk has also been documented in other studies (20,21). However, subclinical hypothyroidism has also been linked to both an increased risk of myocardial infarction (22) and a decreased risk of all-cause mortality (23,24). Therefore, the treatment of subclinical hypothyroidism remains disputed (5).
An international discussion on thyroid dysfunction screening has been going on for many years (25,26), but screening is not conclusively deemed to be either advantageous (27) or disadvantageous (28). Cappola et al. documented an association between low s-TSH within the euthyroid range and multiple adverse events, including mortality, among patients >65 years of age, pointing toward a beneficial effect of a more conservative LT4 treatment regime among the elderly (29). Further, a recent large clinical trial found no benefits on tiredness score and hypothyroid symptoms when treating subclinical hypothyroidism in elderly patients (7). The ETA guidelines recommend a conservative LT4 regime in elderly patients (5). No Danish screening programs were published from the Danish General Practitioners' or Endocrinologists' societies between 2000 and 2015. Nonetheless, an increased focus on social media concerning general symptoms and a possible relation to thyroid disease may have led to increased contact with GPs. The fact that mild hypothyroidism and unspecific symptoms are prevalent in the general population makes it plausible for patients to suggest hypothyroidism as the likely cause—thereby leading to increased diagnosis of clinical as well as mild hypothyroidism—and also possibly initiating LT4 therapy in patients with s-TSH within the reference range. These patients may exhibit symptoms related to nonthyroidal disease such as stress, depression, or even a wish of optimizing general well-being when getting older. Patients presenting with multiple symptoms suggestive of hypothyroidism with a s-TSH within the reference range but without another plausible explanation to the symptoms might lead to GPs trying to help their patient through LT4 treatment, despite the recommendations formulated in professional guidelines.
From 2001 to 2004, an increase was observed in median s-TSH before therapy from 10 to 12 mIU/L, while the number of patients starting LT4 therapy increased from 786 to 910. This change is probably a result of relatively more patients starting LT4 therapy in 2001 with a s-TSH of 0.4–2.5 mIU/L (Table 2 and Fig. 3). The high number of patients initiating LT4 therapy in this early period of the study with a s-TSH within the reference range could partly consist of patients treated for goiter. The effect of LT4 therapy on nontoxic goiter has been refuted (30,31), which could explain the decrease from 2001 to 2007 in the group with a s-TSH from 0.4 to 2.5 mIU/L (Table 2).
During this study, an increasing number of individuals initiated therapy with a s-TSH between 2.5 and 5 mIU/L. The majority of these patients were women aged between 25 and 45 years, which may be related to infertility guidelines in Denmark, recommending LT4 therapy if s-TSH is >2.5 mIU/L (3). This may also be influenced by an international ongoing discussion concerning whether to lower the upper limit of the reference range for s-TSH to 2.5 mIU/L (32,33).
Number of measurements before therapy
Spontaneous remission has been reported in up to 40% of cases with subclinical hypothyroidism (34), and it is recommended to confirm hypothyroidism with multiple s-TSH measurements before initiating therapy (5). In this study, 50% of patients starting LT4 therapy only had a single s-TSH measurement >5 mIU/L before redeeming the first LT4 prescription, indicating a risk of premature treatment. An incidental elevated s-TSH discovered at hospital may be followed up by a GP or vice versa, which might explain some of the solitary s-TSH measurements before therapy. However, this cannot explain that in 2015, 70% of patients initiated LT4 therapy with fewer than two s-TSH measurements >5 mIU/L, and another scientific explanation for this observation is not evident. It could be speculated that patient demand and/or doctors' impatience have influenced this, which again may be influenced by societal expectations of health and quality of life.
Strengths and Limitations
First, a major strength of this study is the very large number of s-TSH measurements included from almost one fifth of the Danish population. Second, all information on prescriptions are derived from the DNPR, and information on previous and concomitant diagnoses are derived from the NPR, with reporting mandatory in both registries. Combining CopLab, DNPR, and NPR offers a unique and comprehensive look into the treatment practices of GPs in the Copenhagen area. Third, all s-TSH analyses were measured at the same laboratory with the same assay, and were subjected to internal and external quality control. Fourth, all s-TSH measurements were included, not only those that led to an LT4 prescription, which to the authors' knowledge has not been done before. This avoids the bias, potentially caused by increased case-finding effort, of the indirect evaluation of the treatment thresholds done previously.
Limitations include the lack of information on symptoms from medical charts, which are important when considering treating mild hypothyroidism and the elderly (5). Access to measurements conducted at hospitals was not available. However, the vast majority of patients with hypothyroidism are managed in primary care.
Conclusion
From 2001 to 2015, in the Copenhagen area, a falling s-TSH threshold for the initiation of LT4 therapy is reported. The number of s-TSH measurements almost tripled in the period, and the rate of new prescriptions reached a plateau in 2010, suggesting that few patients with hypothyroidism remain undiagnosed. The majority of patients started LT4 therapy without more than a single s-TSH measurement >5 mIU/L. Measuring TPO-antibodies appears to have influenced the s-TSH threshold considerably.
This study points to an international trend in treating hypothyroidism, with an increased chance of futile treatment and consequent risk of overtreatment.
Footnotes
Acknowledgments
This study was funded by external private funds, without any influence on any part of this study. Data handling and ethical issues of this study were approved by the Faculty of Health Science, University of Copenhagen (
Author Disclosure Statement
No competing financial interests exist.