
Abstract
Background:
This study aimed to evaluate the role of 18F-choline (18F-FCH) positron emission tomography (PET)/computed tomography (CT) in high-risk differentiated thyroid cancer (DTC) patients with suspected relapse. It also compared 18F-FCH-PET/CT results with those of fludeoxyglucose (18F-FDG)-PET/CT and evaluated the additional diagnostic value and clinical impact of the combined use of these two tracers. Finally, it assessed the association between the clinical, biochemical, and histological parameters and 18F-FCH-PET/CT and 18F-FDG-PET/CT results.
Methods:
The study prospectively enrolled high-risk DTC patients treated with thyroidectomy and radioactive iodine therapy and presenting high/increasing thyroglobulin levels under thyrotropin suppression, negative/inconclusive neck ultrasound, and negative 131I whole-body scan. All patients underwent 18F-FDG-PET/CT and 18F-FCH-PET/CT within 30 days of each other. Experienced nuclear medicine physicians examined the images of both procedures, and an integrated analysis of the two PET/CT modalities was also conducted. For each modality, a patient-based analysis (PBA) and lesion-based-analysis (LBA) was performed. On PBA, sensitivity, specificity, negative predictive value, positive predictive value, and accuracy were calculated. On LBA, only sensitivity was calculated. The standard of reference was based on clinical, imaging, and histological data.
Results:
Twenty-five high-risk DTC patients were included; DTC relapse/persistence was confirmed in 23 patients. On PBA, 18F-FDG-PET/CT, 18F-FCH-PET/CT, and the integrated evaluation of the two imaging modalities showed the following rates: sensitivity, specificity, negative predictive value, positive predictive value, and accuracy were 69.6%, 100%, 22.2%, 100%, and 72% versus 56.5%, 100%, 16.7%, 100%, and 60% versus 82.6%, 100%, 33.3%, 100%, and 84%, respectively. When compared with 18F-FDG-PET/CT, the integrated analysis of these two imaging procedures changed the clinical management in 4/23 (17%) patients. On LBA, the sensitivity rates of 18F-FDG-PET/CT, 18F-FCH-PET/CT, and the combined evaluation of the two modalities were 58.7%, 38.1%, and 66.7%, respectively; when only lymph node involvement was considered, the rates were 56.3%, 53.1%, and 68.8%, respectively. Serum thyroglobulin doubling time (Tg-DT) <12 months was significantly associated with positive 18F-FCH-PET/CT. A trend toward a significant association was also found between positive 18F-FDG-PET/CT and both Tg-DT <12 months and DTC aggressive subtypes.
Conclusion:
18F-FCH-PET/CT may add important information during the follow-up of high-risk DTC patients. 18F-FCH-PET/CT may be considered a useful complementary tool in patients affected by non-aggressive DTC subtypes, with Tg-DT <12 months, high risk of lymph node spreading, and negative or doubtful 18F-FDG-PET/CT.
Introduction
In differentiated thyroid cancer (DTC) patients, it is unusual to find evidence of structural disease persistence or recurrence after thyroidectomy and radioactive iodine therapy (RAI)—the so-called “initial therapy” (1). However, in DTC patients who are at high risk according to the 2015 American Thyroid Association (ATA) guidelines (1), the risk of disease relapse ranges from 30% to 55% (1). In this setting, the clinical outcome one year after initial treatment is often associated with biochemically persistent/recurrent disease, and patients with complete response account for only 31% (1 –3). Thus, prompt diagnostic localization of structural disease in such patients is relevant and requires different approaches. Although neck ultrasonography (US) is the pivotal imaging procedure in detecting locoregional DTC persistence/recurrence, some US findings may remain inconclusive. In addition, in the case of suspicious extra-cervical disease, an additional whole-body imaging procedure seems to be mandatory (1). Fludeoxyglucose (18F-FDG) positron emission tomography (PET)/computed tomography (CT) is able to detect DTC relapse with a sensitivity ranging from 50% to 100% (1,4). Its use is suggested in patients with a negative radioiodine whole-body scan (WBS) and increased suppressed (Tg-on) or thyrotropin (TSH)-stimulated thyroglobulin (Tg) and/or short Tg doubling time (Tg-DT; i.e., <12 months) (1,5). By contrast, its sensitivity is lower in patients affected by less aggressive DTC subtypes (6) with long Tg-DT (5). 18F-choline (18F-FCH) is a PET tracer able to evaluate cell membrane turnover. High 18F-FCH uptake has been observed in benign and malignant lesions, and its clinical usefulness has been demonstrated in prostate cancer and hepatocarcinoma (7 –10). More recently, this tracer has proved useful in detecting hyperfunctioning parathyroid gland in patients with proven primary hyperparathyroidism and negative or inconclusive 99mTc-sestamibi parathyroid scans (11). Overall, radiolabeled choline seems a useful alternative to FDG, especially in those tumors characterized by low glucose metabolism.
Only scant data on the use of choline PET/CT in DTC patients are available, and only two case reports have described a potential role of this tracer in evaluating persistence/recurrence of disease in patients affected by high-risk DTC in whom 18F-FDG-PET/CT findings are inconclusive (12,13).
The present study was undertaken to investigate the diagnostic impact of 18F-FCH-PET/CT performed in a large series of high-risk DTC patients with suspected persistence/relapse of the disease after initial treatment. Accordingly, the diagnostic accuracy of 18F-FCH-PET/CT in localizing the structural persistence was analyzed, these findings were compared with those of 18F-FDG-PET/CT, and the potential diagnostic improvement yielded by combining these two PET modalities was calculated. In addition, the study aimed to evaluate the association between the principal clinical, biochemical, and histological parameters and 18F-FCH-PET/CT and 18F-FDG-PET/CT results.
Methods
Patient population
The study period ran from December 2013 to January 2017, and two nuclear medicine departments (Galliera Hospital, Genoa, Italy, and Oncology Institute of Southern Switzerland, Bellinzona, Switzerland) were involved. Consecutive high-risk DTC patients without distant metastases at the time of first diagnosis, who had been treated with total thyroidectomy and radioactive iodine therapy (RAI), and who presented measurable/increasing Tg-on with negative Tg autoantibodies (TgAb) at the one-year follow-up examination were prospectively selected.
Among these, patients who fulfilled the following criteria were enrolled: (i) no 131I uptake outside the thyroid bed on post-therapeutic 131I WBS; (ii) negative diagnostic 131I WBS performed one year after the initial therapy under exogenous stimulation; and (iii) negative or inconclusive neck US findings deemed not amenable to fine-needle aspiration biopsy.
All these patients had been staged according to the Tumor-Node-Metastasis/American Joint Committee on Cancer seventh edition (14) and had at least two serum Tg-on measurements in the first 12 months of follow-up.
In these subjects, a second-line imaging by 18F-FDG-PET/CT and 18F-FCH-PET/CT within 30 days of one another was proposed. Patients who refused one or both studies were excluded from the study. The Institutional Review Board approved the study, and patients in the final study series gave their informed consent.
Laboratory methods
Serum Tg and TgAb were measured by Elecsys® e601 (Roche Diagnostics) according to the manufacturer's specifications. Kinetics of serum Tg were computed on the basis of two consecutive Tg-on measurements performed prior to the PET/CT examinations. Data were eligible if the concurrent TSH levels were suppressed (i.e., TSH <0.2 mIU/L) and the time between measurements was less than six months. Tg-DT was calculated using the formula: Tg-DT = (0.693 × dt)/ln(r1/r2), where dt is the time between the Tg assays, and r1 and r2 are the results of the first and second Tg assays, respectively (15).
PET/CT
All patients fasted for at least six hours before 18F-FDG-PET/CT scanning in order to minimize blood insulin levels and glucose utilization by normal tissue and underwent examination one hour after intravenous injection of 3 MBq/Kg of 18F-FDG. The data were obtained in each center using a dedicated PET/CT system. The protocol in both centers involved an initial CT acquisition followed by a PET study. CT parameters used for acquisition included 140 kV, 80 mA, 16 slices helical, 0.5 s per rotation, and pitch 6:1, with a slice thickness of 3.25 mm equal to that of PET. CT images were reconstructed to a 512 × 512 matrix. PET was acquired by sequential fields of views, each covering 12 cm, over an acquisition time of three minutes. PET acquisition was performed in 3D with a matrix of 128 × 128. Data obtained from CT acquisitions were used for low-noise attenuation correction of PET emission data and for fusion of attenuation-corrected PET images with corresponding CT images. The patients were instructed to void before imaging. No oral or intravenous contrast agents were administered or bowel preparation applied for any patient.
18F-FCH-PET/CT was performed in the fasting state (six hours), and a 18F-FCH activity of 3 MBq/kg was administered intravenously. Data were acquired 40 minutes after the injection by means of the abovementioned PET/CT system. PET was performed over an acquisition time of three minutes in the same manner as for 18F-FDG-PET/CT and displayed on the same workstation. The same CT parameters were also used.
Image interpretation
18F-FDG-PET/CT and 18F-FCH-PET/CT studies were interpreted visually by two different expert nuclear medicine physicians on patient-based analysis (PBA) and lesion-based analysis (LBA) by using dedicated software to review the fused PET/CT images. Semi-quantitative analysis was done by using maximum standardized uptake values (SUV-max) and SUV-mean values, respectively. However, no SUV-max or SUV-mean cutoff values have been introduced, and SUV parameters were calculated for each lesion just to support visual interpretation. On 18F-FDG-PET/CT and 18F-FCH-PET/CT, any focal and nonphysiological uptake, corresponding to any cervical thoracic detectable lesion on low-dose CT (i.e., lymph nodes and lung nodules), was considered as positive. In addition, any focal uptake corresponding to any abdominal parenchyma or bone segments with or without associated CT findings was considered as positive.
Finally, all PET/CT images were reviewed by two other experienced nuclear medicine physicians masked to the previous PET/CT analysis in order to evaluate the performance of 18F-FDG-PET/CT combined with 18F-FCH-PET/CT using the same criteria described above.
In case of disagreement between the readers, the procedure provided a face-to-face comparison in order to reach a consensus review of discordant findings.
Standards of reference
Analysis was performed per patient and per lesion (see below). Histology was the preferred reference standard of the study to calculate the accuracy of imaging procedures. Diagnostic sensitivity was defined as the ratio between the number of positive findings in the imaging procedures and the number of histologically proven DTC relapse/persistence cases. When the postsurgical proof was not available, a multidisciplinary follow-up, including periodic physical examination, serum Tg determination, neck US, and other imaging procedures when clinically indicated (e.g., 131I diagnostic WBS, CT, 18F-FDG-PET/CT, and magnetic resonance imaging), was adopted as the reference standard according to Pacini et al. (16) and the ATA guidelines (1). In particular, those patients with negative morphological and functional imaging were considered as free from structural disease. Regarding LBA, only diagnostic sensitivity was calculated due to the lack of true-negative and false-positive findings.
Statistical analysis
The main descriptive statistics include absolute and relative (%) frequencies, mean, standard deviation, median, minimum, maximum, and interquartile range. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for each diagnostic modality (i.e., 18F-FDG-PET/CT, 18F-FCH-PET/CT, and combined use of the two modalities) for PBA, while only sensitivity was assessed for LBA due to the lack of true-negative and false-positive findings. Fisher's exact test was adopted to compare NPV and PPV, and McNemar's exact test was used to compare sensitivity, specificity, and accuracy of detection rates among detection methods on the same subjects. A two-sample Wilcoxon rank-sum (Mann–Whitney) test was adopted to test differences in Tg and Tg-DT times between detection methods. Logistic regression analysis was used to address the main factors associated with PET/CT positivity. All analyses were conducted using Stata v14.2 (StataCorp) software. Two-tailed probabilities are reported, and a p-value of 0.05 was adopted to define nominal statistical significance.
Results
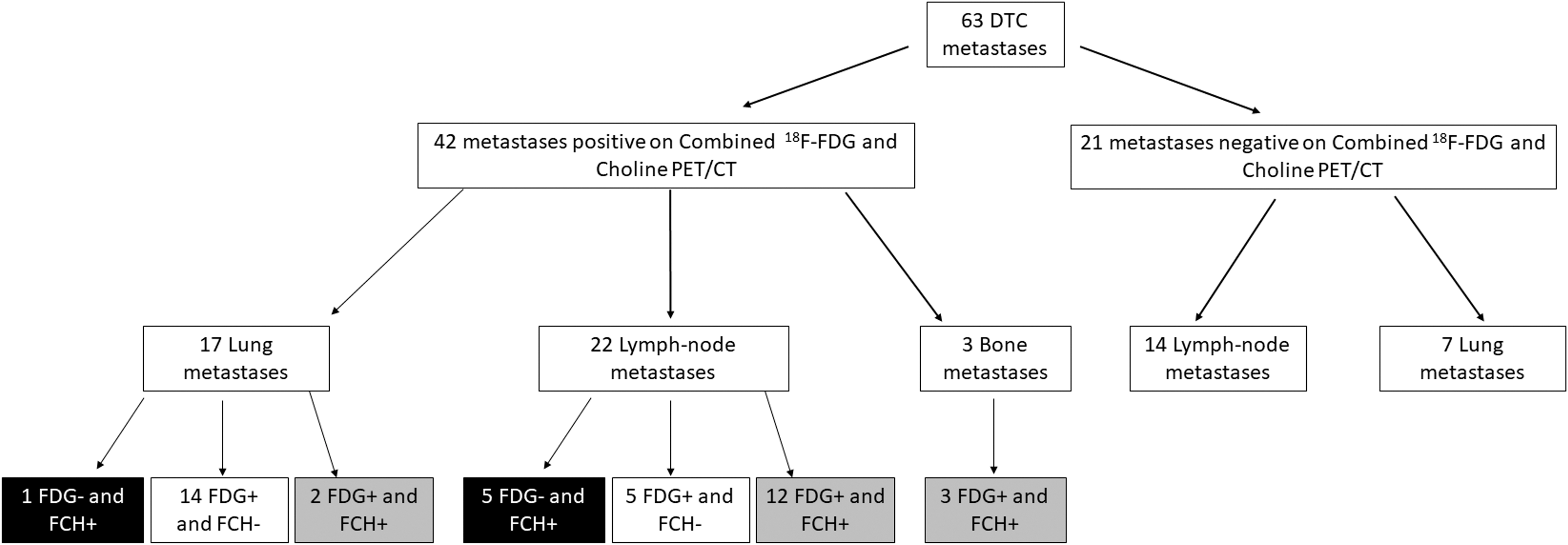
According to the study design, a series of 25 high-risk DTC patients were finally enrolled. DTC relapse/persistence was confirmed in 23/25 patients. Histopathology was available in 14 patients. The median follow-up was 20 months (range 18–26 months). Lymph node metastases were proved in 12 patients, lung metastases in seven patients, bone metastases in three patients, and concomitant lymph node and lung metastases in one patient. Overall, 63 metastatic sites were confirmed (36 lymph node, 24 lung, and 3 bone metastases). The main clinical, histological, and biochemical characteristics of all patients are summarized in Table 1.
Features of the Final Series of Patients
IQR, interquartile range; Tg, thyroglobulin levels under TSH suppression; DT, doubling time.
On PBA, 18F-FDG-PET/CT and 18F-FCH-PET/CT were positive in 16/23 and 13/23 recurrent patients, respectively. The combination of these two imaging procedures was positive in 19 cases. In particular, two out of the four false-negative patients on both 18F-FDG-PET/CT and 18F-FCH-PET/CT were affected by very small lymph node metastases of the neck central compartment, histologically confirmed one year later. The other two patients were affected by tiny and bilateral lung metastases identified by subsequent high-resolution lung CT. Indeed, no false-positive results were found. Table 2 summarizes the difference in terms of sensitivity, specificity, NPV, PPV, and accuracy between 18F-FDG-PET/CT, 18F-FCH-PET/CT, and 18F-FDG-PET/CT combined with 18F-FCH-PET/CT according to PBA.
Patient-Based Analysis: Diagnostic Performance for Each Single Diagnostic Modality
McNemar exact test vs. 18F-FDG-PET/CT combined with 18F-FCH-PET/CT.
F-FDG, fludeoxyglucose; PET, positron emission tomography; CT, computed tomography; 18F-FCH, 18F-choline; NPV, negative predictive value; PPV, positive predictive value.
Nine patients showed discordant findings between 18F-FCH-PET/CT and 18F-FDG-PET/CT (i.e., three with positive 18F-FCH-PET/CT and negative 18F-FDG-PET/CT; six with the opposite pattern).
When the clinical impact of the combined use of 18F-FCH-PET/CT and 18F-FDG-PET/CT versus 18F-FDG-PET/CT alone (i.e., the current standard of care) was evaluated, the integrated analysis changed the clinical management in 4/23 (17%) recurrent patients, particularly in 3/7 (43%) FDG-negative patients. By revealing three FDG-negative single metastases (two lymph node and one lung metastases), the addition of 18F-FCH-PET/CT led to a surgical approach in three patients affected by non-aggressive DTC, who were otherwise candidates for empirical RAI treatment (Figs. 1 and 2). In addition, in one patient affected by left cervical lymph node metastases already detected on 18F-FDG-PET/CT, one additional contralateral lymph node metastasis was detected by 18F-FCH-PET/CT, prompting a bilateral neck dissection (Fig. 3).

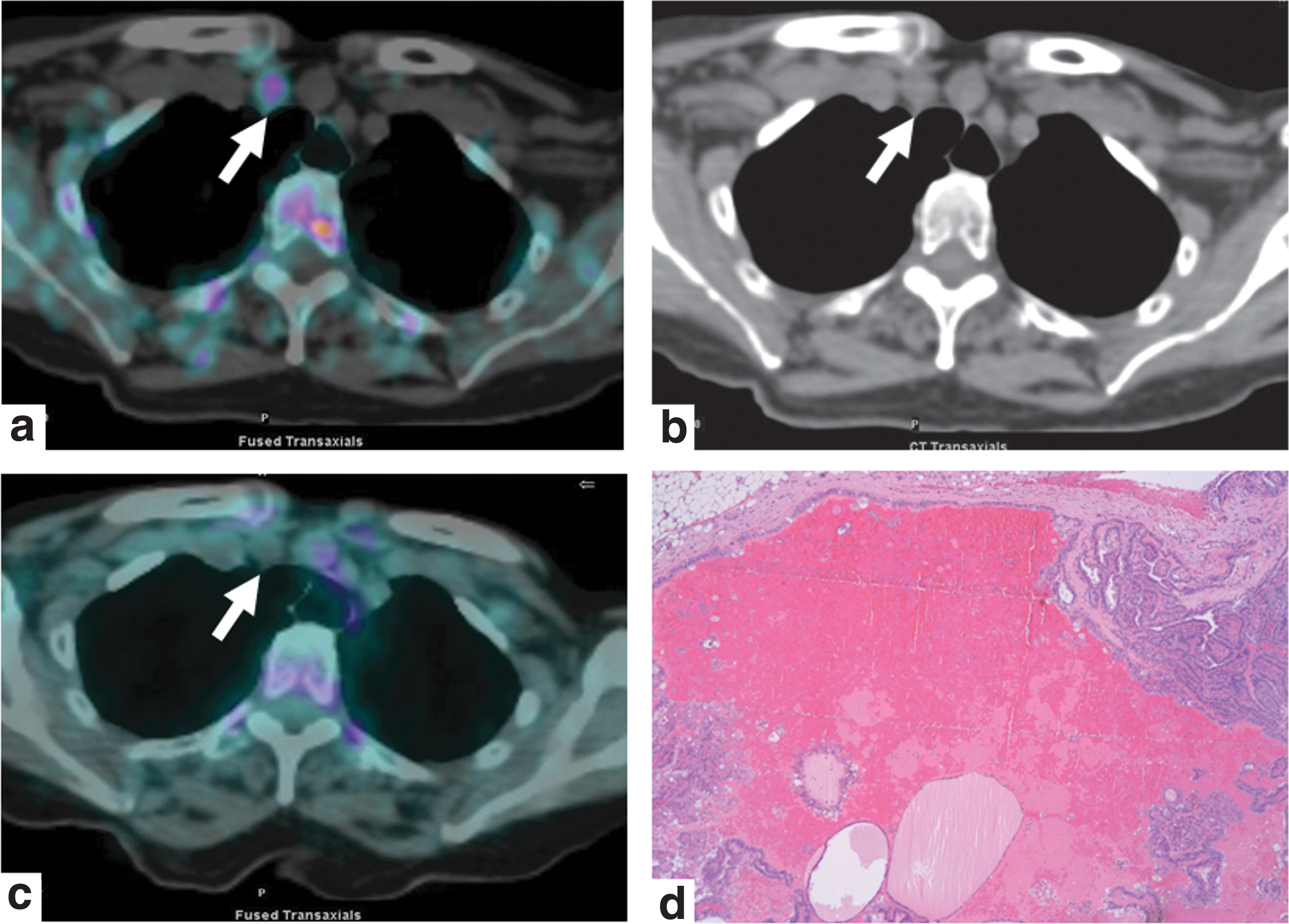
A 66-year-old female affected by a non-aggressive variant of papillary thyroid cancer (PTC; pT3mN1b) treated with thyroidectomy, right lymphadenectomy, and radioactive iodine (RAI). Ten months later, increased suppressed thyroglobulin (Tg-on) was 15.6 ng/mL with a doubling time (DT) of eight months. Neck ultrasound (US; not shown) identified a hypoechoic and calcified left latero-cervical lymph node and an inconclusive fine-needle aspiration biopsy result (i.e., cytology and Tg measurement in the washout fluid) was obtained due to the calcified shell. 18F-choline (18F-FCH) positron emission tomography (PET)/computed tomography (CT) showed a focal uptake (

A 66-year-old male affected by a non-aggressive variant of PTC (pT4N1a) treated with thyroidectomy, central compartment lymph node dissection, and RAI. Twenty months later, Tg-on was 6.28 ng/mL with a DT of 9.8 months. 18F-FCH-PET/CT showed a single focal uptake (
A 74-year-old female affected by an aggressive variant of PTC (pT3mN1b) treated with thyroidectomy, left cervical lymph node dissection, and RAI. Twelve months later, Tg-on was 4.1 ng/mL with a DT of 8.58 months. Neck US (not shown) detected an enlarged lymph node with cystic and solid components in the right retro-clavicular region positioned under the brachiocephalic trunk and not amenable to safe fine-needle aspiration biopsy. 18F-FCH-PET/CT showed focal uptake (
On LBA, 18F-FDG-PET/CT, 18F-FCH-PET/CT, and 18F-FDG-PET/CT combined with 18F-FCH-PET/CT revealed 35/63, 24/63, and 42/63 metastases, respectively. When the lymph node localizations were considered, no significant differences in terms of sensitivity were observed between 18F-FDG-PET/CT and 18F-FCH-PET/CT (Table 3). For this question, the integrated analysis of these two imaging procedures proved to be the most sensitive diagnostic approach. 18F-FDG-PET/CT was found to be significantly more sensitive than 18F-FCH-PET/CT in detecting lung metastases (Fig. 4), but no differences in terms of the identification of bone metastases were ascertained (Table 3 and Fig. 5). 18F-FDG-PET/CT showed more lymph node and lung metastases than 18F-FCH-PET/CT in eight patients. 18F-FCH-PET/CT showed more lymph node and lung metastases than 18F-FDG-PET/CT in four patients. Overall, 26 (41%) lesions were found with a mismatching metabolic pattern (Fig. 6). In particular, six (10%) FDG-negative lesions proved positive on 18F-FCH-PET/CT, and 19 (30%) lesions showed an opposite pattern.

A 72-year-old female affected by an aggressive variant of PTC treated with thyroidectomy, bilateral lymphadenectomy, and RAI (pT3N1b). Over the following two years, Tg-on showed a progressive increasing trend reaching 8.3 ng/mL with a DT of 6.7 months. 18F-FCH-PET/CT was negative (

A 43-year-old male affected by an angio-invasive follicular thyroid carcinoma (pT3N0) treated with thyroidectomy and RAI. One year after treatment, Tg-on was 5.53 ng/mL with a DT of 1.3 months. 18F-FCH-PET/CT and 18F-FDG-PET/CT showed focal uptake (
Detailed description of lesion-based analysis evaluating the matching and mismatching results between 18F-FCH-PET/CT and results and 18F-FDG-PET/CT.
Comparison of Sensitivity Performances on the Lesion-Based Analysis
McNemar exact test vs. 18F-FDG-PET/CT combined with 18F-FCH-PET/CT.
When the association between clinical, biochemical, and histopathological parameters of each patient was analyzed using logistic regression, it was found that the Tg-DT was the only parameter significantly associated with evidence of structural disease on 18F-FCH-PET/CT. On the other hand, a trend toward a significant association was observed between positive findings on 18F-FDG-PET/CT, Tg-DT, and aggressive subtype (Table 4).
Factors Associated with 18F-FCH-PET/CT and 18F-FDG-PET/CT Positivity (Logistic Regression Modelsa)
From a stepwise estimation algorithm, starting from a full model also including age, sex, and T, N, and Tg values.
McNemar exact test vs. 18F-FDG-PET/CT combined with 18F-FCH-PET/CT.
OR, odds ratio; CI, confidence interval.
Discussion
To the best of the authors’ knowledge, this is the first structured study regarding the diagnostic role of 18F-FCH-PET/CT and the clinical impact of the association of 18F-FDG-PET/CT and 18F-FCH-PET/CT in a series of well selected high-risk DTC patients with suspected persistence/recurrence of disease after initial therapy and negative post-therapeutic and diagnostic 131I-WBS. The study also compared 18F-FCH-PET/CT findings with those of 18F-FDG-PET/CT. As the main result, 18F-FCH-PET/CT was able to detect DTC localizations in patients with negative 18F-FDG-PET/CT, and the association of the two imaging procedures directly influenced the clinical management in 17% of patients by revealing unknown or adjunctive sites of disease (three lymph nodes and one lung metastases) amenable to surgery. In all these cases, histological confirmation was available, and interestingly three out of these four patients were affected by non-aggressive DTC subtypes.
These two imaging modalities should be considered complementary, in that the sensitivity of the combination of 18F-FDG-PET/CT and 18F-FCH-PET/CT proved higher than that of 18F-FDG-PET/CT and 18F-FCH-PET/CT alone on both PBA and LBA. Although the level of significance was not reached, this relative diagnostic advantage should not be neglected, given the extreme importance of identifying structural disease in patients who may subsequently benefit from a more tailored therapeutic approach. In addition, the impact of the relatively small sample size on the statistical power of the tests used should be considered.
Although 18F-FCH-PET/CT proved less sensitive than 18F-FDG-PET/CT, the presence of a high number of mismatched findings between these two modalities paves the way for their combined use, especially in patients who may benefit from surgery with curative intent. This finding was particularly evident with regard to the evaluation of the neck and upper mediastinum, where 23% of the lymph node metastases detected by the combination of the two PET procedures were FDG-negative. In this anatomical area, on LBA, the association of 18F-FDG-PET/CT and 18F-FCH-PET/CT was more sensitive than 18F-FDG-PET/CT alone. By contrast, 18F-FDG-PET/CT was significantly more sensitive than 18F-FCH-PET/CT in detecting lung metastases, and only 1/24 lesions showed an FDG-negative and FCH-positive pattern. All three bone metastases were well depicted by both 18F-FDG and 18F-FCH-PET/CT scans.
When the association of 18F-FDG-PET/CT and 18F-FCH-PET/CT results was analyzed with the relevant clinical, biochemical, and histopathological parameters, the only parameter significantly associated with 18F-FCH-PET/CT was Tg-DT. In the same setting, a marked trend toward significance was observed between 18F-FDG-PET/CT results and both Tg-DT values and aggressive histological subtype. In this context, it could be speculated that 18F-FCH-PET/CT should be considered an important additional diagnostic option in the case of patients affected by high-risk DTC with non-aggressive subtypes, short Tg-DT, and high probability of lymph node spreading. From this point of view, a possible explanation for the higher sensitivity of 18F-FDG-PET/CT in detecting lung metastases could be the well-known accuracy of 18F-FDG-PET/CT in revealing more aggressive sites of DTC relapse. Indeed, 8/13 lung metastases that proved positive on 18F-FDG-PET/CT and negative on 18F-FCH-PET/CT were found in patients with aggressive DTC subtypes.
Despite the encouraging results, some limitations should be addressed. First, this study was conducted on a relatively small number of patients. However, the patients were carefully selected, treated, and monitored in accordance with homogeneous protocols in two referral centers. Second, histopathological confirmation was not available in all patients. However, 12/23 patients with positive findings on combining 18F-FDG-PET/CT and 18F-FCH-PET/CT underwent surgery, and the presence of disease was proved. In the other patients, a multidisciplinary follow-up of at least 18 months was available.
Conclusions
18F-FDG-PET/CT was confirmed to be the most sensitive molecular imaging procedure in detecting DTC persistence/relapse after initial therapy in patients with negative 131I-WBS. However, 18F-FCH-PET/CT may detect adjunctive sites of disease and impact on clinical management in a not negligible number of patients. Thus, 18F-FCH-PET/CT should be considered in the case of patients at high risk of structural relapse with negative radioiodine 131I-WBS and 18F-FDG-PET/CT and short Tg-DT (i.e., <1 year). Further data on a larger number of patients are necessary to confirm these results.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.