
Abstract
Background:
Early pregnancy fetal growth is a relevant determinant of pregnancy outcome and child health during later life. During the first trimester, fetal growth depends on the transfer of maternal thyroid hormone, and optimal thyroid hormone availability is ensured via stimulation of the maternal thyroid by human chorionic gonadotropin (hCG). The potent stimulatory effects of hCG on gestational thyroid function and its clinical relevance with early fetal growth remain unknown and need to be examined.
Methods:
This study comprised 46,186 mothers for whom early pregnancy thyrotropin (TSH), free thyroxine (fT4), triiodothyronine, thyroperoxidase antibodies, hCG, as well as ultrasound crown-rump length (CRL) measurements were available. Data were also available on potential confounders, including maternal age, parity, anthropometrics, and fetal sex.
Results:
There was a negative association of TSH with CRL and a positive association of fT4 with CRL, with effect estimates of roughly 0.1 standard deviation (SD) across the full ranges. However, when taking into account thyroid stimulation by hCG, an impaired thyroidal response to hCG stimulation was associated with up to a 0.2 SD lower CRL (high hCG with high TSH) and up to a 0.6 SD lower CRL (high hCG with low fT4). Even within the normal range of TSH and fT4, an impaired thyroidal response to hCG stimulation was associated with a lower CRL.
Conclusions:
Low maternal thyroid function during the first trimester is associated with a modestly lower CRL. However, an impaired thyroidal response to hCG stimulation is associated with a considerably lower CRL for which effect estimates are in the range of or even supersede those of well-known risk factors. These data can help to improve the identification of pregnancies at high risk of fetal growth restriction and adverse pregnancy or child outcomes.
Introduction
Adaptations of the fetus to a suboptimal intrauterine environment can have major consequences for subsequent growth, development, and the risk of disease during later life (1). It is becoming increasingly clear that adverse health effects can already be induced during the first trimester, as cell proliferation and differentiation rates are highest and important stages in organ development take place. First-trimester fetal growth is a reflection of early fetal adaptations and maturation. Previous studies have shown that fetal growth restriction during the first trimester is associated with a higher risk of miscarriage, preterm delivery, small-for-gestational-age newborns, as well as compensatory accelerated growth and an adverse cardiovascular risk profile during childhood (2 –7). The identification of determinants of first-trimester fetal growth is important to identify high-risk pregnancies that may benefit from closer monitoring. Thyroid hormone is a well-known regulator of growth and development in practically all tissues of the human body, and maternal thyroid disease has been associated with pre-eclampsia, premature delivery, and child neurodevelopment (8). Furthermore, previous studies consistently have shown that a higher maternal free thyroxine (fT4) concentration during the first or second trimester is associated with a decline in mid- and late-pregnancy fetal growth and/or lower birth weight, especially in male newborns (9 –11). However, the association of maternal thyroid function with first-trimester fetal growth remains to be elucidated.
Fetal thyroid hormone production starts around the 14th week of pregnancy. Therefore, fetal thyroid hormone availability during the first trimester solely depends on the placental transfer of maternal thyroid hormone (8,12,13). Human chorionic gonadotropin (hCG) is a pregnancy-specific hormone that exerts thyrotropic activity via its weak affinity for the thyrotropin (TSH) receptor (12,14). hCG concentrations peak around the 10th week of pregnancy, which leads to an increase of up to 50% in maternal fT4 concentrations (15,16). This increase in thyroid hormone availability safeguards sufficient thyroxine transfer to the developing fetus and thus facilitates the high rate of fetal growth and development (12). Previous studies have shown that the hCG-mediated increase in thyroid hormone is impaired in women with thyroid autoimmunity (i.e., thyroperoxidase antibody [TPOAb] positive women) (17). However, the role of thyroid stimulation by hCG as well as TPOAb positivity in relation to first-trimester fetal growth remain to be elucidated.
The current study investigated the association of maternal thyroid function with first-trimester fetal crown-rump length (CRL), including the role of thyroid stimulation by hCG, thyroid autoimmunity, and fetal sex. Given the biological relevance and timing of thyroid stimulation by hCG, it was hypothesized that decreased functional thyroid capacity would be associated with impaired fetal growth. Therefore, it was expected that an impaired thyroidal response to hCG stimulation (e.g., a high hCG with a high TSH or a low fT4), as a marker of a lower functional thyroid capacity, would be associated with a lower CRL.
Methods
Patient enrollment
This study was performed in the International Peace Maternity and Child Health Hospital (IPMCH), a large community hospital providing secondary and tertiary care in Shanghai, P.R. China. The project was approved by the Ethics Committee of IPMCH (no. GKLW2012-49). Eligible women were those who underwent first-trimester prenatal screenings at the hospital between January 2013 and December 2016. A total of 52,027 women were enrolled during the first trimester, all of whom had TSH, fT4, T3, and TPOAb concentrations or CRL data available. Women who underwent in vitro fertilization (IVF), who had a twin pregnancy or fetal loss, who used thyroid interfering medication, or who had a history of thyroid disease were excluded.
Data collection
During the hospital visit, all data were prospectively collected by nurses, residents, and gynecologists using electronic patient files. Fasting blood samples were drawn from the median cubital vein, and the serum was separated by centrifugation within six hours. TSH, fT4, T3, and TPOAb concentrations were measured using the Architect i2000 immunoassay (Abbott, Chicago, IL) according to the manufacturer's protocol. Measurements for T3 were only performed in a subset of 9975 women who presented during 2015. hCG was measured in serum using a solid-phase two-site chemiluminescent immunometric assay on an Immulite 2000 XPi system (Siemens Healthcare Diagnostics, Deerfield, IL) from January 2015 to December 2016, and thus was only available in a subset of 29,453 women. All participants underwent real-time transabdominal ultrasound with a full bladder. Certified medical doctors, unaware of thyroid function test outcomes, measured the CRL by ultrasound using a 5–7 MHz curvilinear array transducer (Shimadzu, Kyoto, Japan) on a frozen monitor image with electronic calipers. Data on maternal age, parity, education level, and last menstrual period (LMP) were collected via interviews at first clinical presentation during which also height and weight were measured to calculate body mass index (BMI). Of all the women, <0.1% smoked or consumed alcohol at presentation to the hospital. Data were also available on potential confounders, including maternal age, parity, anthropometrics, and fetal sex, as these factors are associated with maternal thyroid function and early fetal growth (1,5,18).
Statistical analyses
Reference ranges for TSH (0.03–3.6 mIU/L) and fT4 (11.7–19.8 pmol/L) were defined by the 2.5th and 97.5th percentiles of the entire population of women who presented to the hospital January 2013 and December 2016 after exclusion of twin pregnancies, women who became pregnant after IVF, women who used thyroid interfering medication, women who had pre-existing thyroid disease, and TPOAb-positive women. Linear regression models were used to study the association of TSH, fT4, T3, or hCG with CRL. Model assumptions were checked with residual plots, outlier exclusions, and by utilizing three to five restricted cubic splines to assess potential nonlinearity. The study investigated whether the association of TSH, fT4, or T3 with CRL differed according to the hCG concentrations by adding a product interaction term of TSH, fT4, or T3 (continuous) with hCG (continuous) to the model, as has been done previously (17,19,20). This variable in the model tests the hypothesis that the association of TSH, fT4, or T3 with CRL differs according to low or high hCG concentrations (21). Subsequently, heat maps (in which red indicates a higher CRL and blue indicates a lower CRL) were constructed to quantify the differences in CRL further according to combinations of hCG or TPOAbs and TSH, fT4, or T3. Additionally, if the interaction term reached statistical significance, differences were also further quantified by showing mean CRL values according to thyroid function and hCG cutoffs. These were chosen based on statistical power for validity of the presented mean and the expected effect based on the heat-map analysis. CRL values are typically used to determine pregnancy duration. However, for the current study, standardization of CRL for gestational age was necessary for optimal analysis. Therefore, CRL values were transformed to standard deviation scores standardized to gestational age of pregnancy determined according to the LMP. The main analyses were repeated after women with a large difference between the LMP and CRL were excluded to exclude any misclassification of LMP due to an irregular menstrual cycle for example (an estimated difference of ±10 mm, which was roughly the highest and lowest 10% of the population). For variables with missing data, multiple imputation according to the Markov chain Monte Carlo method was used by creating and pooling five imputed data sets for analyses. The imputation model included maternal BMI (missing in 1.5%) and LMP (missing in 3.1%). Furthermore, maternal age, gestational age, education, marital status, parity, CRL, TSH, fT4, total T3, and TPOAb concentrations were added as prediction variables only. No significant differences in descriptive characteristics were found between the original and imputed data sets. All statistical analyses were performed using R v3.03 (package rms and visreg) or SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY).
Results
After exclusions, the final study population comprised 46,186 women (Fig. 1), descriptive characteristics of whom are shown in Table 1. In the study population, the mean maternal age was 30.1 (standard deviation [SD] = 3.6), the median BMI was 20.8 (range 17.6–25.2), and 52.5% (24,245) of the women were pregnant with a male fetus. The median TSH was 1.17 mIU/L (range 0.1–3.2 mIU/L), the median fT4 was 14.8 pmol/L (12.1–18.6 pmol/L), and the median T3 was 2.2 nmol/L (1.7–2.9 nmol/L), and 10% (4621) of the study population was TPOAb positive according to the manufacturer cutoff.

Flow chart exhibiting the selection of the study population.
Descriptive Statistics of the Study Population
SD, standard deviation; BMI, body mass index; hCG, human chorionic gonadotropin; TSH, thyrotropin; fT4, free thyroxine; T3, triiodothyronine; TPO, thyroperoxidase.
A higher TSH was associated with a lower fetal CRL, with an approximately 0.1 SD lower CRL across the full range of TSH (p = 0.0033; Fig. 2A). A higher fT4 was associated with a higher fetal CRL, with an approximately 0.1 SD higher CRL across the full range of fT4 (p = 0.0030; Fig. 2B). Furthermore, neither T3 (p = 0.4817; Fig. 2C) nor the ratio of T3/fT4 was associated with CRL (data not shown).

The association of maternal thyroid function with crown-rump length (CRL) in early pregnancy. Plots show the linear regression models for (
Previous studies have shown that the association of maternal thyroid function with birth weight is more prominent in male-fetus pregnancies (11). In order to investigate if these differences are already established during the first trimester, analyses were subsequently stratified according to fetal sex. The effect estimates of the association of TSH or fT4 with CRL were twice as large for male-fetus pregnancies as for female-fetus pregnancies (Fig. 3A–D; p for sex–TSH interaction = 0.0497 [βmale sex = 0.024, βfemale sex = 0.012]; and sex–fT4 = 0.031 [βmale sex = 0.011, βfemale sex = 0.005)). The association of T3 with CRL was similar between fetal sexes (p for sex–T3 interaction = 0.71).
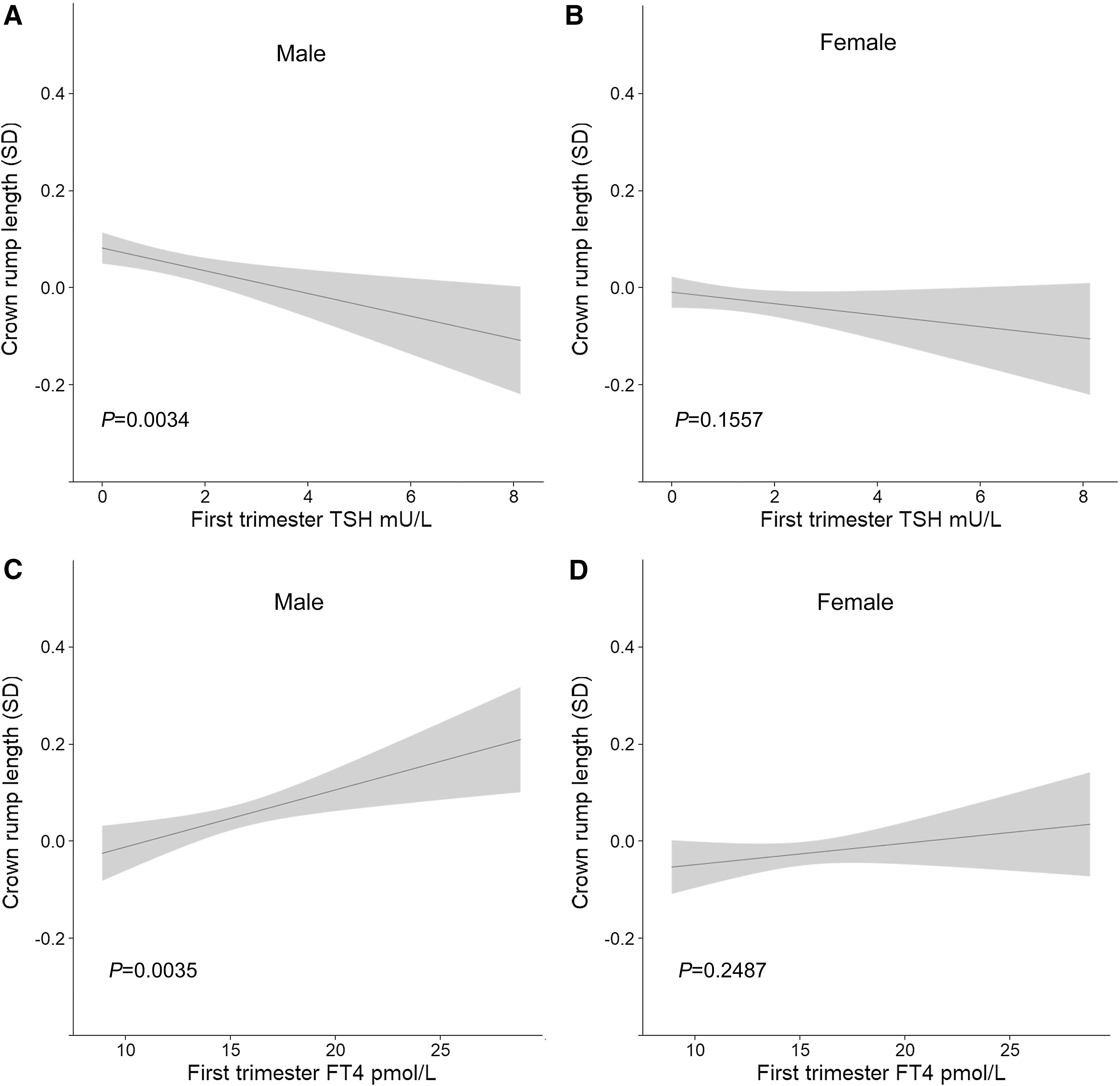
The association of TSH and fT4 with CRL in early pregnancy in male and female fetuses. Plots show the linear regression models for TSH (upper panels) or fT4 (lower panels) and CRL in male (left panels) and female (right panel) fetuses, as well as fT4 and CRL in male (
TPOAb positivity was associated with a 0.009 SD lower CRL compared to TPOAb-negative women (Table 2), and this result did not differ according to fetal sex.
Mean CRL According to TPOAb Status and Fetal Sex
Data adjusted for maternal age, parity, BMI, hCG, education level, hypertension, diabetes, and fetal sex (when applicable).
CRL, crown-rump length; TPOAb, thyroperoxidase antibodies; SE, standard error.
Thyroidal response to hCG and CRL
During the first trimester, fetal thyroid hormone availability solely depends on the placental transfer of maternal thyroid hormone. In turn, adequate maternal thyroid hormone production during the first trimester is ensured through additional stimulation of the thyroid by high hCG concentrations. Therefore, the study investigated whether a low functional thyroid capacity as reflected by impaired thyroid stimulation by hCG (i.e., a high hCG with a high TSH or low fT4) is associated with fetal CRL. In continuous analyses, women with a high TSH despite a high hCG had up to a 1.5 SD lower CRL, while the same TSH concentration was not associated with CRL in women with a lower hCG (Fig. 4A; p for interaction = 0.0197). When stratified into groups, a TSH >2.0 mIU/L despite a high hCG was associated with a 0.2 SD lower CRL (Table 3), indicating outlier effects in the continuous analyses. In continuous analyses, women with a lower fT4 despite a high hCG had up to a 0.8 SD lower CRL, while the same fT4 concentration was not associated with CRL in women with a lower hCG (Fig. 4B; p for interaction = 0.0247). When stratified into groups, a fT4 < 14 pmol/L despite a high hCG was associated with up to a 0.5 SD lower CRL (Table 3).
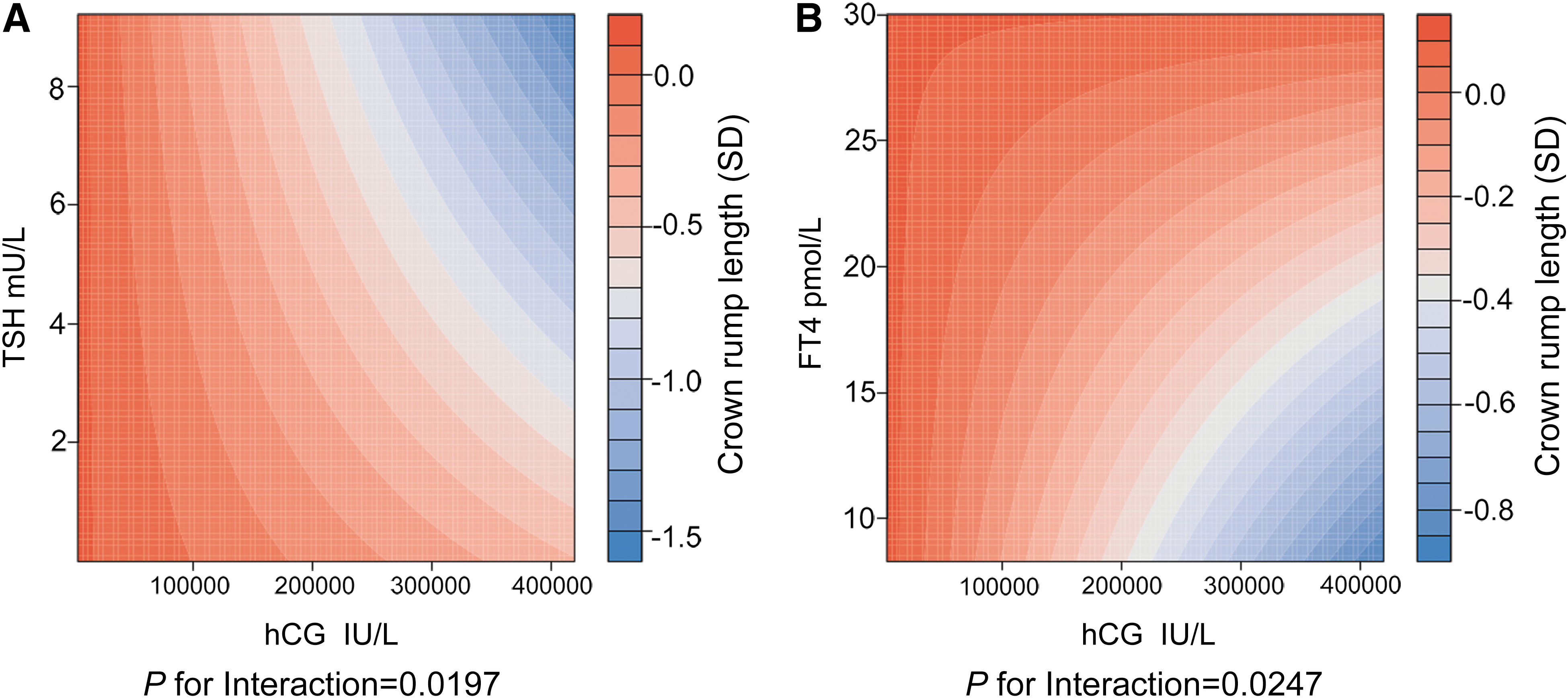
The thyroidal response to hCG and CRL. The figure displays a heat map for the association of last menstrual period (LMP)-adjusted CRL (red color indicates lower CRL, blue color indicates higher CRL) according to the interaction of (
Association of TSH and fT4 Cutoffs with CRL Stratified by hCG
All analyses are adjusted for maternal age, BMI, parity, education level, hypertension, diabetes, and fetal sex. “Full range” means no exclusions were made based on TSH or fT4 concentrations. “Within reference range” means within only women with a TSH or fT4 within the reference range defined as the 2.5th–97.5th percentiles were included for analyses. The comparison group were women with either a TSH <2.0 mIU/L (left) or a fT4 > 14.0 pmol/L (right) and a similar hCG concentration.
Compared to hCG and TSH/fT4 effects alone; 1 SD CRL = 9.5 mm.
Even within the reference range for TSH and fT4, considerable differences were identified when the thyroidal response to hCG was assessed. In women with a normal TSH, a high-normal TSH despite high hCG was associated with up to a 0.8 SD lower CRL in continuous analyses (p for interaction = 0.0456; Fig. 5A) but only 0.2 SD in stratified analyses. In women with a normal fT4, a low-normal fT4 despite a high hCG was associated with up to a 0.8 SD lower CRL (p for interaction = 0.0027; Fig. 5B) in continuous analyses and 0.6 SD in stratified analyses (Table 3).
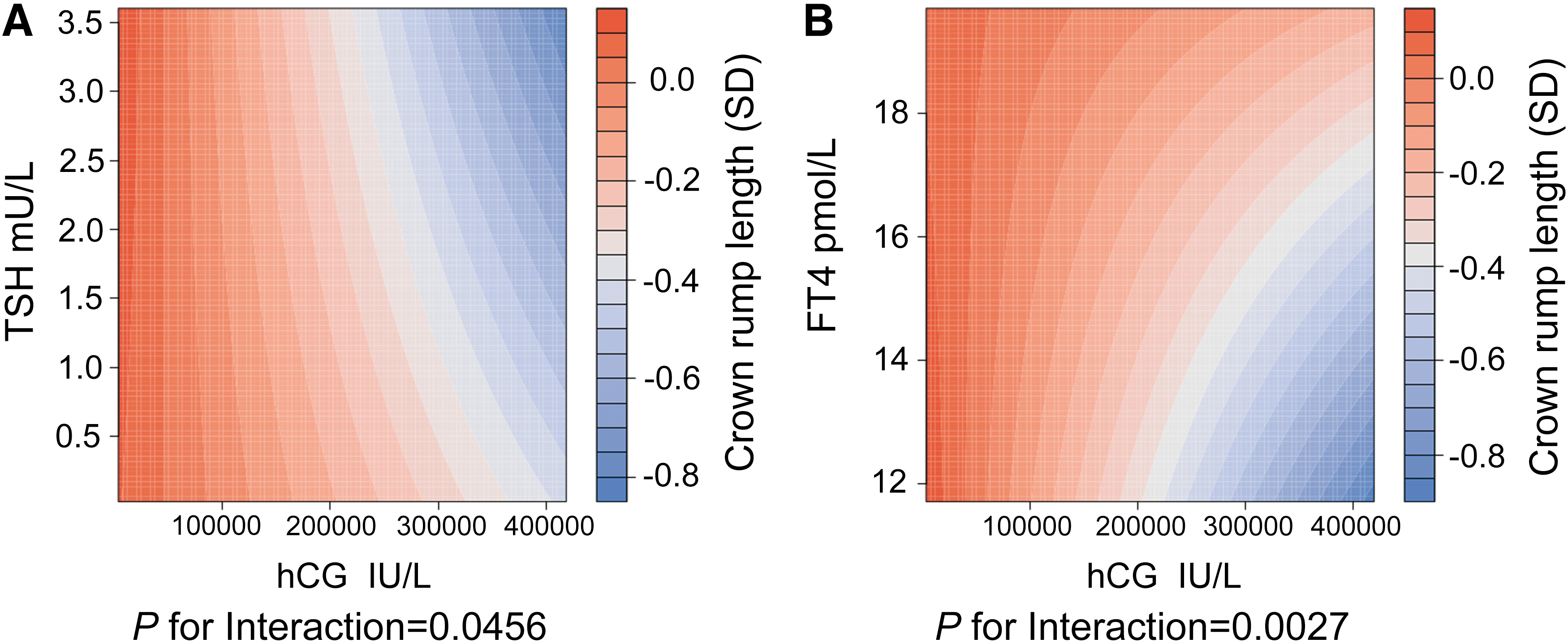
The thyroidal response to hCG and CRL in the normal range. The figure displays a heat map for the association of LMP-adjusted CRL (red color indicates higher CRL, blue color indicates lower CRL) according to the interaction of (
There was a negative association of hCG with CRL (Supplementary Fig. S1). There were no fetal sex–specific differences in the association of thyroidal response to hCG and CRL (p for sex–TSH–hCG interaction = 0.507 and sex–fT4–hCG = 0.877). All analyses remained similar after exclusion of women with a large difference between the LMP and CRL (data not shown).
Discussion
The current study investigated the association of maternal thyroid function and the thyroidal response to hCG stimulation with fetal growth during the first trimester. The main finding is that while the findings from other studies can be replicated showing that lower absolute maternal thyroid function is associated with a slightly lower CRL, it is actually an impaired thyroidal response to hCG stimulation that is associated with suboptimal early fetal growth. Women with an impaired thyroidal response to hCG stimulation had a 0.8–1.5 SD lower CRL—effect estimates that are similar or even larger than well-known risk factors such as maternal smoking and BMI.
Thyroid hormone is an important stimulator of fetal growth and development, but fetal thyroid hormone availability during early pregnancy solely depends on the placental transfer of maternal thyroid hormones. To the best of the authors' knowledge, this is the first study to investigate the effects of maternal thyroid function on early fetal growth. The large sample size of the current study showed that lower maternal thyroid function is associated with a lower CRL during the first trimester. These overall effect estimates were relatively small, ranging between 0.1 and 0.2 SD difference in CRL across the full range of TSH and fT4 concentrations. Overall, there was no association of T3 with CRL. This is most likely because T3 does not cross the placenta and/or because T3 is bound to thyroid hormone binding proteins and thus reflects an inactive form of thyroid hormone.
While absolute TSH and fT4 concentrations have been associated with various adverse pregnancy outcomes (8), more recent data show that an impaired functional thyroid capacity as reflected by an impaired thyroidal response to hCG can be used to improve the identification of women at high risk for premature delivery and pre-eclampsia (17,20,22). The current study shows that an impaired thyroidal response to hCG stimulation was associated with up to 0.6 SD lower CRL. These effect estimates are larger than those reported for well-known risk factors of early fetal growth restriction such as maternal age, smoking, ethnicity, and fetal sex (1,5,23). A smaller first-trimester CRL is associated with a higher risk of adverse pregnancy outcomes, including premature delivery and low birth weight, as well as disease during childhood and later life (1 –4,7). As such, women with an impaired thyroidal response to hCG could benefit from more intense follow-up. The results of the current study further emphasize that suboptimal thyroid stimulation by hCG during pregnancy may be the underlying mechanism for previous studies that show that low maternal thyroid function is associated with a higher risk of adverse outcomes.
When taking into account the physiology that hCG stimulates maternal thyroid function during early pregnancy, it transpired in the current study that it is not the absolute TSH or fT4 concentration but an impaired thyroidal response to hCG stimulation that is associated with a clinically meaningful lower CRL. The current study defined impaired thyroid stimulation as a high TSH or low fT4 despite high hCG concentrations. An impaired thyroidal response to hCG most likely is a reflection of decreased functional thyroid capacity. A recent study indicated that TPOAb-positive women have an impaired thyroidal response to hCG stimulation. Even in euthyroid women without a history of thyroid disease or autoimmunity, a decreased functional thyroid capacity may be exposed during a state of increased thyroid demand such as pregnancy or during controlled ovarian hyperstimulation (17,20,24). Alternatively, the combination of a high hCG with a low fT4 or high TSH could reflect hCG isoforms less potent for the TSH receptor or very rare TSH receptor defects. It is important to note that not all women who were studied exhibited hCG concentrations at the time of blood measurement that were high enough to distinguish true differences in functional thyroid capacity. This leaves open the possibility that women with a high risk of a lower CRL were not identified as such because they underwent blood sampling outside of their hCG peak. However, the cross-sectional data are similar to the timing and type of measurements that are available for decision making in clinical practice. Therefore, the results of the current study suggest that the additional measurement of hCG concentrations can improve the interpretation of maternal thyroid function tests and may allow clinicians to improve the identification of women at higher risk of pregnancy complications related to suboptimal thyroid hormone availability.
Similar to a previous study focusing on birth weight, this study found that the effects of maternal thyroid function on early fetal growth are larger in male-fetus pregnancies than in female-fetus pregnancies (11). Considerable fetal sex–specific differences exist in placental gene expression, placentation markers, and the risk of adverse pregnancy outcomes (25 –27). These and other data have led to the hypothesis that carrying a male fetus demands a higher degree of metabolic adaptation because male fetuses have increased growth compared to female fetuses at the cost of a less optimal placentation (23,28). It is speculated that lower maternal thyroid hormone availability leads to a suboptimal metabolic response, which is more likely to affect male-fetus pregnancies due to the higher metabolic demand compared to female-fetus pregnancies. However, while fetal sex–specific differences were identified for the association of absolute TSH and fT4 concentrations with CRL, fetal–specific differences could not be identified in the association of the thyroidal response to hCG stimulation with CRL. This may imply that any fetal sex–specific differences in the effects of thyroid hormone on growth and development only occur after the first trimester. Alternatively, the fetal sex–specific differences identified in this study and other studies could be confounded by fetal sex–specific differences in placental angiogenic factors (such as soluble FMS-like tyrosine kinase and placental growth factor) (27,29) or by fetal sex–specific differences in hCG isoforms other than β-hCG that are known to have a more potent stimulating effect on the TSH receptor (30 –32). Further implementation of gestational thyroid physiology in research studies is needed to improve the identification of high-risk pregnancies and clinically relevant effects on fetal growth and adverse pregnancy outcomes.
To the best of the authors' knowledge, this is the first study to investigate the association of maternal thyroid function and the thyroidal response to hCG stimulation with fetal growth during the first trimester. For these analyses, extensive, prospectively collected data were available on a wide range of maternal thyroid function parameters and potential confounders for a large group of unselected women. A potential limitation of this study is that only a single measurement of maternal thyroid function, hCG, and CRL was available during the first trimester. In theory, the results could thus not be generalizable to earlier pregnancy because TSH, fT4, T3, hCG, and CRL measurements performed between weeks 9 and 12 of pregnancy may not optimally reflect thyroid function or fetal growth during the first nine weeks.
Another potential limitation is that this study only included Chinese women from the Shanghai area, and therefore these results are not necessarily generalizable to other areas in the world or even within China. Besides obvious ethnic or genetic differences, the percentage of women who smoke or consume alcohol or who are primi- or multiparous is considerably lower than women in Europe or the United States. However, studies on the important time frame of the first trimester with numbers similar to that of current study are practically impossible to obtain in Europe or the United States, considering that Chinese women present to hospital much earlier during pregnancy.
In addition, the Shanghai area is mildly iodine deficient, but even though it is unknown whether iodine status during pregnancy can affect the thyroidal response to hCG stimulation, iodine status during pregnancy is not associated with fetal growth and thus is unlikely to interfere with the results of this study (33). Although a low iron status is associated with a lower birth weight and with a lower thyroid function, further studies are needed to identify whether iron status affects the thyroidal response to hCG stimulation (34,35).
Finally, it is important to note that the observational nature of this study limits any causal inference, and the results cannot be extracted to potential treatment effects.
In conclusion, this study shows that an impaired thyroidal response to hCG is associated with a clinically meaningful lower CRL during the first trimester. These data suggest that an adequate thyroidal response to hCG stimulation is important for an uncomplicated pregnancy. Furthermore, the additional measurement of hCG may improve the clinical interpretation of thyroid function tests during pregnancy. If the concept that an impaired functional thyroid capacity is associated with a higher risk of adverse pregnancy outcomes is studied further and clinically leveraged, this could improve the clinical identification of high-risk pregnancies and be followed by interventional studies aimed at improving clinical outcomes. More studies are needed in order to replicate these findings and to define further optimal thyroid status during pregnancy.
Footnotes
Acknowledgments
We gratefully acknowledge the contributions and efforts of all pregnant women who participated in this study and the doctors and nurses involved in data collection and patient care. This work was supported by grants from the National Natural Science Foundation of China (81471516, 81501274), National Key Research and Development Program of China (2016YFC1000203), and the Foundation of Shanghai Municipal Commission of Health and Family Planning (15GWZK0701).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1