
Abstract
Background:
Insufficient production of thyroid hormones results in hypothyroidism, while overproduction results in hyperthyroidism. These are common adult disorders, with hypothyroidism more common in the elderly. Jordan has had past problems with dietary iodine deficiency but there are no published studies assessing the population prevalence of these disorders in the Arab Middle East.
Methods:
A cross-sectional study was conducted in three representative areas of Jordan. There were 7085 participants with a mean age of 40.8 years. Participants completed a questionnaire and had blood taken for thyroid analysis.
Results:
Hypothyroidism: The prevalence of any hypothyroidism (already diagnosed and/or identified by blood testing) was 17.2% in females and 9.1% in males. Undiagnosed prevalence was 8% and 6.2% for females and males, respectively. The prevalence of subclinical hypothyroidism, defined as high serum thyrotropin (TSH) and normal serum-free thyroxine (fT4), was 5.98% among females and 4.40% among males. The prevalence of overt hypothyroidism, defined as high TSH and low fT4, was 2.00% among females and 1.80% among males. Only 53.5% (55.3% for females, 42.1% males) of those previously diagnosed with hypothyroidism had TSH levels within the appropriate range. Hyperthyroidism: The prevalence of any hyperthyroidism (already diagnosed and/or identified by blood testing) was 1.8% in females and 2.27% in males. The undiagnosed prevalence was 1.4% and 2.1% for females and males, respectively. The prevalence of subclinical hyperthyroidism (low TSH and normal fT4) was 1.20% and 1.80% among males and females accordingly. The prevalence of overt hyperthyroidism (low TSH and high fT4) was 0.2% among females and 0.3% among males. About 85.7% (83.3% for females, 100% males) of those previously diagnosed with hyperthyroidism had TSH levels within the appropriate range.
Conclusions:
The results of this study reveal that the total prevalence of thyroid dysfunction among adult females and males in Jordan is very high compared with international statistics, particularly in the rates of undiagnosed cases. This indicates the need for further assessment of the value of screening for adult hypothyroidism in Jordan.
Introduction
Failure of the thyroid gland to produce sufficient amounts of thyroid hormones (thyroxine [T4], triiodothyronine [T3]) results in hypothyroidism, while hyperthyroidism results from raised levels of thyroid hormones (1). Hypothyroidism is common in older people (2). For example, in a study of 1154 women ages 50–72, 39 (3.4%) had hypothyroidism, including 14 (1.2%) previously undiagnosed cases; in that study, hypothyroidism was defined as an elevated thyrotropin (TSH) (3).
Hypothyroidism can cause nonspecific symptoms that reduce a person's quality of life, including depression, lethargy, constipation, weight gain, memory impairment, and poor concentration. However, these symptoms are common as people age and can have many causes, so the possibility of hypothyroidism is easily overlooked. Many will not even seek medical attention since the symptoms are regarded as a natural consequence of getting older (4). In view of this, population screening of adults for hypothyroidism may be worthwhile and lead to useful preventive treatment that would not otherwise be initiated.
Estimates of the prevalence of subclinical thyroid dysfunction in general populations differ substantially and vary according to ethnic group, dietary iodine intake, and the prevalence of antithyroid antibodies (5 –8).
In iodine-replete communities, the prevalence of overt hypothyroidism is between 1% and 2% (9) and the prevalence of subclinical hypothyroidism is between 2.9% (10) and 10% (11); it is more common in older women (12), and 10 times more common in women than in men (9). The most common etiology is chronic autoimmune thyroiditis (13).
Hyperthyroidism is less common than hypothyroidism with prevalence rates of 2% for women and 0.2% for men (12). The prevalence of hyperthyroidism in women is between 0.5% and 2%, and is 10 times more common in women than in men in iodine-replete communities (2,9). The prevalence of subclinical hyperthyroidism in the community varies between 0.7% and 12.4% (11,14,15). This variability is, in part, due to differences in the definition of low serum TSH values and in the patient populations studied (16).
Although adult hypothyroidism and hyperthyroidism are common disorders, there has been no published study that assessed the prevalence of these conditions in the general population in the Arab world. This study is part of the Jordan national hypothyroidism and hyperthyroidism project that also evaluated other objectives, such as degree of disease control, patient compliance with medications, quality of life, and psychological well-being. This report publishes the prevalence of these two conditions, as well as the prevalence of symptoms among patients.
Methods
This is a cross-sectional study that assessed the prevalence of hypothyroidism and hyperthyroidism by sex among the adult general population in Jordan: subclinical hypothyroidism, overt hypothyroidism, overt hyperthyroidism, and subclinical hyperthyroidism.
Study locations were as follows: Central region: Wadi Elseer, Hashemi, Kraibit Elsoog areas in Amman and Wadi Elsair. Southern region: Marj town, Thanniyyeh town, Mazar town, and Soul village in Karak governorate. Northern region: Iydoon, Hay Alshargi, Barhah area in Irbid city and Kharja village.
The planned number of patients to be recruited was estimated at 3500, 1500, and 2000 from the Central, Southern, and Northern regions, respectively. Recruitment was conducted between June 1, 2016, and May 31, 2017, in two stages. Stage one was through a door-to-door outreach program to identify eligible subjects. The research team contacted (already identified) potential participants and invited them to come to the health care center closest to their home or workplace within the study areas. The door-to-door approach was conducted in the middle, north, south, east, and west parts of included cities to ensure that samples from different socioeconomic class areas would be sampled. Due to the difference in the prevalence of thyroid dysfunction disorders by sex, the sample was stratified by sex. A systematic approach of selecting residents was followed according to the target sample size from each area. For example, every fifth house or flat was selected.
Eligible subjects were interviewed at the health care centers in study areas. Research assistants explained the study protocol and obtained consent from participants to take part in the study, to review their medical profiles, as well as to inform their family physician about their participation. Blood samples of subjects with an abnormal TSH were further tested for free thyroxine (fT4). Thyroid peroxidase antibodies were tested for hypothyroid or subclinical hypothyroid patients, while anti-TSH receptor antibodies (TRAbs) were measured for hyperthyroid or subclinical hyperthyroid patients.
Research outcomes
Primary outcomes
Prevalence of thyroid dysfunction disorders by sex and age group in Jordan:
Subclinical hypothyroidism (high TSH and normal fT4),
overt hypothyroidism (high TSH and low fT4),
subclinical hyperthyroidism (low TSH and normal fT4), and
overt hyperthyroidism (low TSH and high fT4).
Secondary outcomes
Assess the prevalence of undiagnosed overt hypothyroidism and overt hyperthyroidism in Jordan.
Assess symptoms of thyroid dysfunction through a thyroid assessment questionnaire.
Assess predictors of prevalence of hypothyroidism.
Eligibility criteria
Inclusion criteria
Jordanian nationals ages 18 to 79 living permanently in the study areas.
Exclusion criteria
Patients with the following conditions were not invited to join the study:
People who have difficulties in communication.
People not permanently residing in the study areas.
People who have a medical condition or are taking drugs that affect TSH secretion or thyroid hormone secretion, absorption, transport, or metabolism (17). These include the following:
○ Antiepileptic drugs: carbamazepine, phenobarbital, phenytoin
○ Anion exchange resins: cholestyramine, colestipol
○ Aspirin if taken long term in doses >2 g/day
○ Steroids if taken long term in higher doses (e.g., prednisolone ≥15 mg/day, hydrocortisone ≥100 mg/day)
○ Other drugs: dopamine, lithium, amiodarone, amphetamine, tamoxifen, heroin, methadone, fenclofenac, mefenamic acid, rifampicin, anabolic steroids, cardiac glycosides (digoxin) (17 –21).
Biochemistry
Serum TSH, fT4, and free triiodothyronine (fT3) were measured by chemiluminescent immunoassays (Advia Centaur; Bayer Diagnostics, Newbury, United Kingdom). Serum TSH had a laboratory reference range of 0.4–4.5 mU/L with an interassay coefficient of variation of 4.4–10.9% over the range of 0.41–24.5 mU/L. The assay was calibrated against the second International Reference Preparation 80/558. The lower limit of reporting for the TSH assay was 0.1 mU/L and the manufacturer's quoted mean functional sensitivity was 0.019 mU/L. The laboratory reference range for fT4 was 9.0–20.0 pmol/L with an interassay coefficient of variation of 8.2–9.8% over the range of 8.2–54.9 pmol/L. Serum TSH and fT4 concentrations were determined in all; in those with serum TSH below normal, serum fT3 (reference range 3.5–6.5 pmol/L, interassay coefficient of variation of 4.2–6.9% over the range 4.0–16.0 pmol/L) was also measured.
Anti-thyroid peroxidase antibodies (TPO) antibodies were measured by the electrochemiluminescence immunoassay (ECLIA) method (Roche) and the reference range in humans is between 0 and 34 IU/mL. Anti-TPO antibodies are more common than anti-Tg antibodies and more indicative for thyroid disease (22).
The TSH receptor is the antigen for TRAbs. TRAbs are present in 70–100% of Graves' disease (85–100% for activating antibodies and 75–96% for blocking antibodies) and 1–2% of normal individuals (23). Serum levels of TRAbs were assessed using an ECLIA (Elecsys and Cobase immunoassay analyzers), with functional sensitivity of at least 10 IU/mL for TRAbs. The reference range for TgAb is <115 IU/mL.
Statistical methods
Sample size calculations
The primary objective of the study was to estimate the prevalence of hypothyroidism and hyperthyroidism in Jordan. It has been reported in the literature that the prevalence of adult hypothyroidism is about 0.3% for males and 0.6% for females, and prevalence of subclinical hypothyroidism is about 2% for males and 3% for females (9). According to the Jordanian Department of Statistics Reports, the size of the Jordanian population was estimated to be 9,798,000 in 2017 (24). Following standard formulas for sample size estimation of one population proportion at a significance level of 0.05 and error margin of 0.01, a sample of size 6760 is needed (25).
The diagnosis of thyroid disorders is assumed to follow a binomial distribution and a 95% confidence level was assumed throughout the analysis. Collected data were analyzed using R Statistical Computing Software version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics, including means, standard deviations, and proportions, are reported. Participants were divided into two groups: known history of thyroid disorders and no history of thyroid disorders. Summaries for each of the two groups are provided. To identify significant factors that distinguish patients with thyroid disorders from normal participants, multiple linear regression with stepwise selection was used.
Study questionnaires
These questionnaires included items on socioeconomic status, risk factors of thyroid dysfunction, and medical and drug history. The chart review form included items on medical and drug history, risk factors such as family history, drug history, history of autoimmune diseases, as well as complications and comorbidities.
The questionnaire and chart review form used for subjects with a known history of hypothyroidism or hyperthyroidism included items on known complications of these diseases or treatment such as symptoms and signs of under- or overtreatment, recent thyroid function tests, and compliance with medications. Participants with results indicating poor control were informed and advised to report this finding to their family physician.
Ethical approval
Ethical approval was obtained from the Ministry of Health, Jordan, Central Ethics Committee and from the Ethics Committee at Mutah University. Further approvals were obtained from the Directorate of Health in Amman, Irbid, and Karak, governorates where the study was conducted.
Results
Characteristics of study participants
A summary of the participants' demographics is provided in Table 1 based on their diagnoses. Seven thousand ninety-two persons participated in the study with a mean age of 40.8 ± 13.6 years. A total of 47.2% of participants were residents in the Amman governorate in the Central region, 31.8% were residents in the Irbid governorate in the Northern region, while the remaining 21.3% were from the Karak governorate in the Southern region. This reflects the population distribution in the middle, north, and south of the country. Rural areas were represented by 13% of study participants. About 54% of the participants have a monthly income of less than 400 JD and 41% of them have an average monthly income of 400–999 JD. Most of the study participants were married (74.7%) and the majority of them were literate (95.8%). About 30% were full-time employees and 34.3% were housewives.
Summary of Participants' Characteristics by Diagnoses History
Numbers in table are percentages.
UNRWA, United Nations Relief and Works Agency for Palestine Refugees in the Near East.
For patients with no present history of hypo- or hyperthyroidism, 70% were females and 30% were males. Among the patients with a present history of these disorders, 89% were females and 11% were males. A summary of the participants' clinical characteristics based on their diagnoses is provided in Table 2 for females and in Table 3 for males.
Summary of Female Participant Clinical Characteristics by History of Thyroid Disorders
SC, subclinical.
Summary of Male Participant Clinical Characteristics by History of Thyroid Disorders
Prevalence of hypothyroidism and hyperthyroidism
This study revealed that both hypo- and hyperthyroidism are highly prevalent in Jordan with a total prevalence of thyroid dysfunction (both hypo- and hyperthyroidism) of 17.2% among adult female and 9.1% among adult male populations (Table 4). The overall prevalence of overt hypothyroidism (high TSH and low fT4) and subclinical hypothyroidism (high TSH and normal fT4), among Jordanians ages 18 or older, was 6.02% for females and 4.39% for males, respectively. The overall prevalence of overt hyperthyroidism (low TSH and high fT4) and subclinical hyperthyroidism (low TSH and normal fT4) was 0.63% for females and 0.46% for males, respectively.
Prevalence of Hypothyroidism and Hyperthyroidism
This study shows that ∼9.05% of Jordanian women and 8.28% of Jordanian men have these conditions without being diagnosed. The prevalence of undiagnosed cases among males in our study was 4.39% for subclinical hypothyroidism and 1.82% for overt hypothyroidism; for females, the prevalence of undiagnosed cases was 5.98% for subclinical hypothyroidism and 1.17% for overt hypothyroidism (Table 3).The prevalence for newly diagnosed overt hypothyroidism and subclinical hypothyroidism was higher than for overt hyperthyroidism and subclinical hyperthyroidism.
Prevalence of hypothyroidism and hyperthyroidism by age group and sex is shown in Figure 1. The prevalence increases steadily with age reaching more than 20% for women older than 60 and more than 10% for males within the same age group.
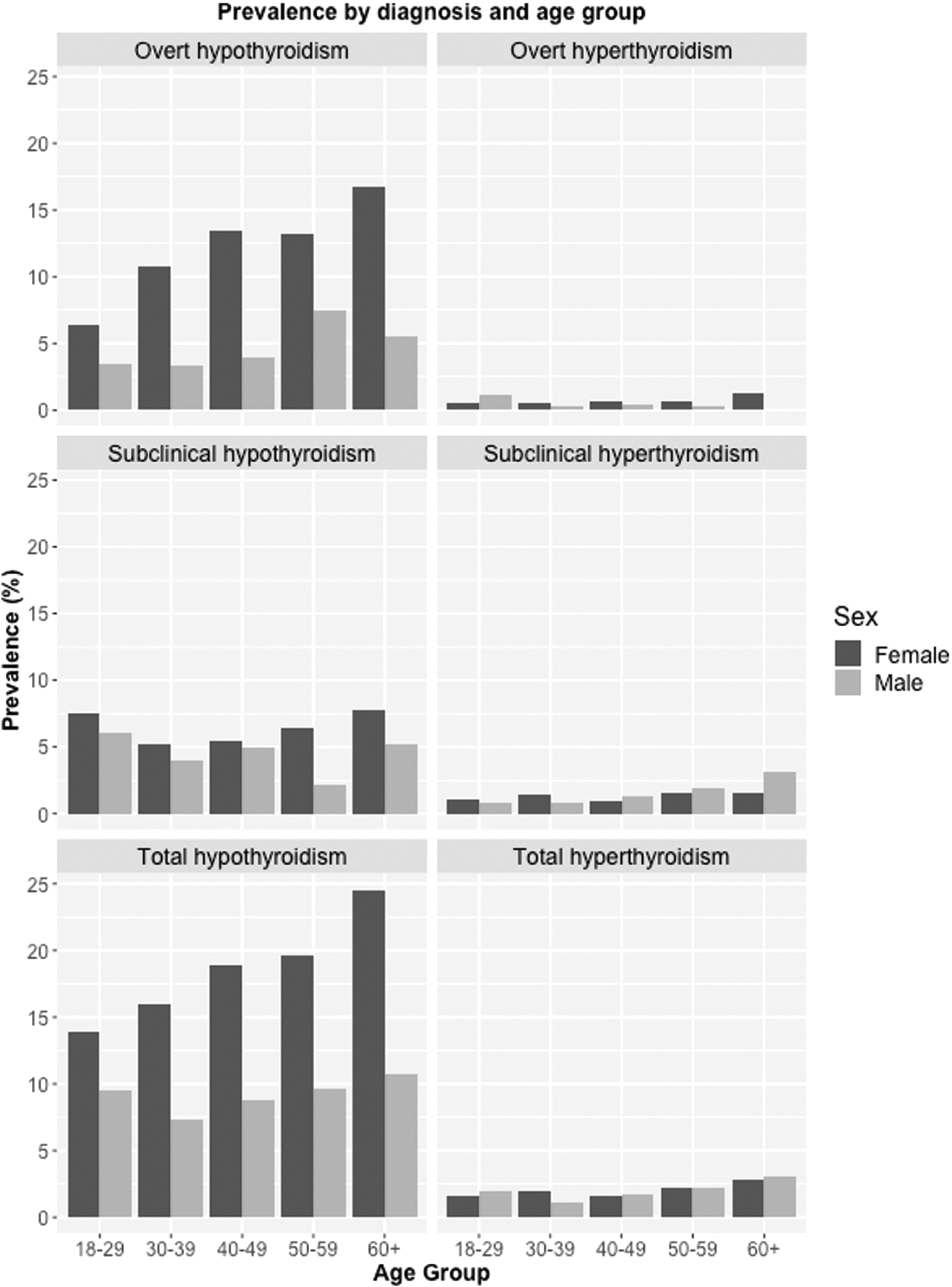
Prevalence by diagnosis and age group.
Control of hypothyroidism and hyperthyroidism
There were 516 patients [456 females (88.4%) and 57 males (11.6%)] with known hypothyroidism and 23 patients (19 females, 4 males) with known hyperthyroidism in the study. Among subjects with known hypothyroidism, only 252 females (55.3%) and 24 males (42.1%) had TSH levels within the reference range of 0.5–4.5 mU/L. A total of 23.1% of males and 11.5% of females were overtreated; and 30.8% of males and 27.9% of females were undertreated with TSH levels >4.5 mU/L. For hyperthyroidism, 83.3% of female patients and 100% of male patients were adequately controlled.
Predictors of prevalence of hypothyroidism and hyperthyroidism
A history of thyroid disorders, sex (female), family history of thyroid disorders, high monthly income (>JD2000), nodule(s), and goiter are the dominant factors for predicting the presence of hypothyroidism (Supplementary Table S1). Patients with a history of thyroid disorders and a personal history of autoimmune disorders, nodule(s), or goiter had a higher probability of being diagnosed with hyperthyroidism. Those who never smoked are less likely to develop hyperthyroidism (Supplementary Table S2). Increasing age and positive personal history of thyroid disorders were positive predictors of having hypothyroidism or hyperthyroidism. Family history was a positive predictor for hypothyroidism but not for hyperthyroidism.
Discussion
To our knowledge, this is the first study to assess the prevalence of adult thyroid dysfunction disorders in the Arab Middle East region. This study shows that prevalence of hypothyroidism and hyperthyroidism is high in Jordan when compared with international statistics. Also, a large proportion of the Jordanian population has undiagnosed hypo- or hyperthyroidism.
In Jordan, the prevalence of overt hypothyroidism (high TSH and low fT4) is around 6% for females and 4.4% for males, which is around 5 times higher than the average figures from iodine-replete countries (9,12). The prevalence of subclinical hypothyroidism (high TSH and normal fT4) is close to reported figures in iodine-replete Western countries. There are no published similar studies from the Middle East region for comparison with these figures. Our findings are consistent with the history of a high prevalence of iodine deficiency in Jordan until 2000. In 1993, the prevalence of goiter among school children was 38%, which dropped to 5% in 2000 after implementing an effective prevention program salt iodization (26). In our sample, 21.7% of patients with hyperthyroidism and 16.1% of patients with hypothyroidism had a history of goiter, which may, at least in part, be associated with the high levels of hypo- and hyperthyroidism found in this study. The high prevalence of hyperthyroidism in Jordan may, in part, be attributed to the misuse of iodine-containing cough syrups, but this hypothesis needs further investigation. The increase in the prevalence of hypothyroidism with age is consistent with figures from Western countries (5).
Most elderly people will not seek medical attention since many unspecific symptoms are regarded as a natural consequence of getting older (4,27). Our study identified large proportions of patients with undiagnosed overt and subclinical hypothyroidism. Thus, it is recommended to conduct a pilot project for systematic screening of adult population in Jordan and to assess whether this screening program is cost-effective or not. It is well established that treating overt hypothyroidism has a significant impact on metabolic and cardiac parameters, among others. Although the topic remains controversial, some support also treating patients with subclinical hypothyroidism (28). For example, results from a recently published crossover clinical trial showed strong evidence to support treatment of patients with repeated TSH levels above 4.5 mU/L (29).
Our study has some limitations. We could not conduct chart reviews for most of the patients or chart review forms were incomplete. Most patients are not registered with any specific general practitioner and prefer seeking care from endocrinologists. This limitation was partially solved by asking patients to bring/report recent TSH readings and their present medications. Lack of registration of residents in certain areas with their local general practitioners did not allow us to recruit directly via the records of general practitioners. Another limitation is the smaller number of male participants. Females were more willing to participate in the study, a finding that is consistent with other community-based epidemiological studies (30). In addition, a population-based study using a door-to-door approach is a new approach in Jordan. More systematic promotion for epidemiological and clinical research within the community in Jordan is also recommended.
In conclusion, the results of this study reveal that the prevalence of thyroid dysfunction among the adult population in Jordan is very high compared with international statistics, particularly the rates of undiagnosed cases. Given that treatment is known to be effective, there is a need for screening for adult hypothyroidism in Jordan, although more research on the most cost-effective approach and the target groups needs to be undertaken. Lastly, there is a need for national recommendations for the management (diagnosis, treatment, and follow-up) of patients with hypothyroidism and hyperthyroidism in Jordan.
Footnotes
Acknowledgments
This research was supported by National Research Fund Office, Ministry of Higher Education. We thank the Technical Affairs Department at the National Research Fund Office, which provided insight and expertise that greatly assisted the research. We also thank Mutah University and the Ministry of Health, Jordan, for the administrative support. We thank Dr. Enid Hennessy and Dr. Victoria Hill for their comments that greatly improved the article. We also thank the reviewers for their comments and valuable suggestions.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2