
Abstract
Background:
The objective of this study was to evaluate the overall survival (OS) of radioiodine (131I) treatments alone or combined with non-131I treatments in patients with bone metastases (BM) of differentiated thyroid cancer (DTC).
Methods:
This was a retrospective study of patients who were evaluated between 2001 and 2018 at MedStar Washington Hospital Center and who had DTC, BM, and at least one 131I treatment after the diagnosis of BM. The OS was analyzed by Kaplan–Meier survival curves and was compared by log-rank test between two groups: patients who received 131I treatments alone and those who received treatments combining 131I with non-131I treatments (CombTx). Non-131I treatments include surgery, radiofrequency ablation, cryotherapy, arterial embolization, external beam radiation, Cyberknife, systemic targeted therapy, and anti-resorptive medication.
Results:
A total of 77 patients met the above criteria and were followed up to 41 years. Thirty percent (23/77) of patients received 131I treatment alone, and 70% (54/77) received CombTx. For 131I treatment alone, the median survival was 3.9 years, and the 1-, 2-, 3-, 5-, and 10-year OS rates were 86%, 81%, 61%, 35%, and 23%, respectively. For CombTx, the median survival was 7.7 years, and the 1-, 2-, 3-, 5-, and 10-year OS rates were 96%, 92%, 86%, 69%, and 30%, respectively. Patients who had undergone initial 131I therapy within six months post thyroidectomy demonstrated a better median survival after BM diagnosis than those whose initial 131I therapy was six months or more after thyroidectomy (6.5 vs. 0.5 years; p < 0.001). Patients who received external beam radiation therapy demonstrated a better median survival than those who did not (7.8 vs. 4.4 years; p = 0.016). Patients who received denosumab demonstrated a better median survival than those who did not (7.7 vs. 5.2 years; p = 0.03). Patients who were <55 years of age at the initial diagnosis of DTC or at the initial diagnosis of BM had a better median OS than those diagnosed at ≥55 years of age (both p = 0.01). In the multivariate analysis, only age at initial diagnosis of DTC and initial 131I therapy within six months post thyroidectomy, and multiple 131I treatments were independent prognostic factors.
Conclusions:
In patients with DTC with BM, 131I treatment in combination with one or more non-131I direct and systemic treatments was associated with a significant increase in OS compared with those patients who were treated by 131I treatment alone.
Introduction
Radioiodine (131I) treatment of 131I-avid bone metastases (BM) secondary to differentiated thyroid cancer (DTC) has been previously reviewed (1) and was found to be associated with improved survival (2 –11). For these patients, the 2015 American Thyroid Association (ATA) Guidelines recommend that 131I “should be employed” (12). In regard to using additional non-131I localized or systemic treatments, the ATA guidelines recommend that BM localized treatment such as surgery or external beam radiation therapy and systemic bone localized treatment “should also be considered” (12).
Multiple other authors have evaluated one or more non-131I localized or systemic treatments in patients with BM secondary to DTC (4,6,13 –23). Although all of these reports are valuable, each of the reports either (i) had a low number of patients (24), (ii) showed no difference in outcomes with the use of non-131I localized treatments (24,25), (iii) evaluated only single non-131I localized treatments without differentiating whether the patients also received 131I treatment (5,14,22,26 –29), (iv) did not report results specific to DTC (24), and/or (v) did not use overall survival (OS) as the endpoint (25). In addition, few studies report the outcomes of non-131I localized treatments used in conjunction with dosimetrically guided 131I treatment for BM (14,24).
The objective of this study was to evaluate the difference in OS of 131I treatments alone compared to combined therapy with non-131I treatments in patients with BM secondary to DTC.
Methods
This was a retrospective study of patients who were evaluated between 2001 and 2018 at MedStar Washington Hospital Center and had (i) DTC, including papillary, follicular variant of papillary, follicular, Hürthle cell, tall-cell, columnar-cell, diffuse sclerosing, and hobnail variants; (ii) BM, and (iii) at least one 131I treatment after the diagnosis of BM. BM were diagnosed by diagnostic or post-therapy radioiodine whole-body scan, computed tomography, magnetic resonance imaging, bone scintigraphy, 18F-fluorodeoxyglucose positron emission tomography, pathological fracture, and/or biopsy. 131I treatment after diagnosis of BM included empiric treatment and dosimetrically guided treatment. 131I blood/whole-body dosimetry was performed on five consecutive days after a low-iodine diet, adequate thyrotropin stimulation, and administration of 2 mCi 131I. The procedure for 131I blood/whole-body dosimetry has been previously described (30). Patients were excluded if the patient had non-DTC histology (i.e., poorly differentiated, medullary, or anaplastic) and suboptimal follow-up records. Patients were categorized into two groups: (i) patients who received 131I treatments alone and (ii) those who received 131I therapy combined with non-131I treatments. Non-131I treatments include surgery, radiofrequency ablation, cryotherapy, arterial embolization, external beam radiation, Cyberknife, systemic targeted therapy, and anti-resorptive medication. The patient demographics and clinical data, including treatment modalities, were collected from patient medical records and are shown in Table 1. For the purposes of this study, patients were categorized into those who received 131I therapy within six months post thyroidectomy or six months or later after post thyroidectomy. These 131I therapies were not further differentiated as remnant ablation, adjuvant therapy, or treatment of known metastatic disease (12,31). It was not possible to assess the data for outcomes based on individual remnant ablation, adjuvant treatment, or treatment of distant metastasis. However, it was possible to assess the timing of the initial 131I therapy post thyroidectomy, number of therapies, and cumulative 131I activity.
Patient Demographics of 77 Patients in the Total Cohort
The three patients who did not have total/completion thyroidectomy had an initial pathology report of low-risk disease or benign thyroid disease.
I, radioiodine; BM, bone metastasis; DTC, differentiated thyroid cancer.
Statistical analysis
The primary endpoint was all-cause mortality. OS was defined as the period of time from initial diagnosis of BM to death.
Continuous variables were compared using Student's t-test. Comparisons between each group according to the categorical variables were performed using the chi-square test or Fisher's exact test (two sided). Kaplan–Meier survival analysis determined the OS and was compared by log-rank test. The relationship between OS and the prognostic factors was assessed by Cox proportional hazards regression model. In multivariate analysis, the prognostic factors that were significantly associated with OS were included in univariate analysis. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics for Windows v17.0 (SPSS Inc., Chicago, IL).
The study was approved by the Institutional Review Board at MedStar Health.
Results
A total of 77 DTC patients who had 131I treatment for BM met the above criteria. The demographics are shown in Table 1. Fifty-two percent (40/77) of patients died. After BM diagnosis, the median OS was 6.4 years ([confidence interval (CI) 4.3–8.4 years]; Fig. 1). The 1-, 2-, 3-, 5-, and 10-year OS rates were 93%, 89%, 80%, 61%, and 27%, respectively.
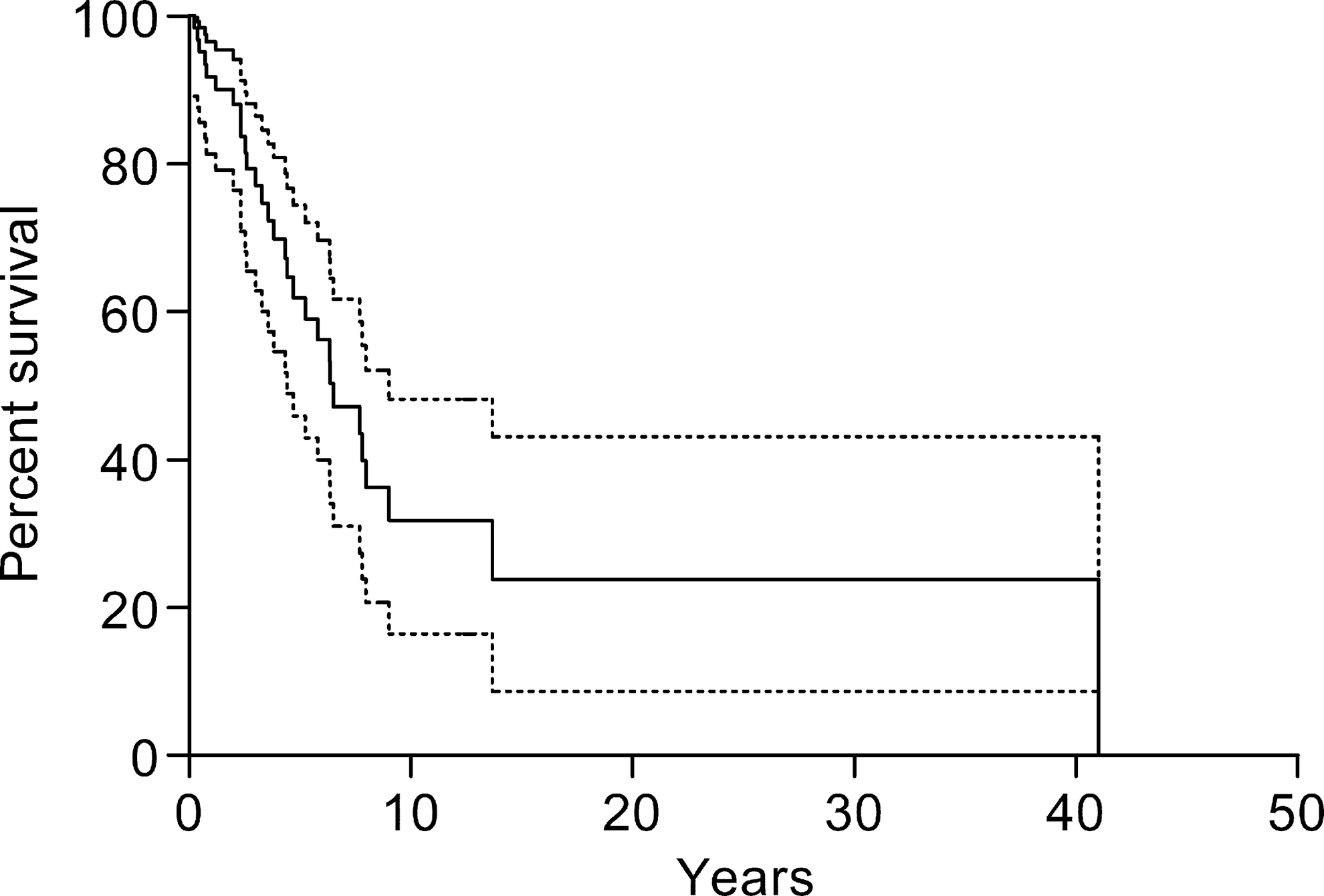
Overall survival (OS) in the total cohort of 77 patients who received radioactive iodine (131I) treatment for bone metastasis secondary to differentiated thyroid cancer (DTC). The median OS was 6.4 years [confidence interval (CI) 4.3–8.4 years]. Dotted lines indicate upper and lower confidence intervals.
Comparison of 131I alone versus 131I combination treatment
Thirty percent (23/77) of patients received 131I treatment alone for DTC BM, and 70% (54/77) received 131I combination treatment. In those patients treated with 131I-alone, the median survival was 3.9 years [CI 2.0–5.8 years], whereas in those patients who were treated with 131I combination treatment, the median OS was 7.7 years ([CI 5.4–9.9 years]; p = 0.03; Fig. 2). For 131I-alone, the 1-, 2-, 3-, 5-, and 10-year OS rates were 86%, 81%, 61%, 35%, and 23%, respectively. For 131I combination treatment, the 1-, 2-, 3-, 5-, and 10-year OS rates were 96%, 92%, 86%, 69%, and 30%, respectively.

Comparison of 131I treatment alone versus 131I treatment in combination with non-131I treatment for bone metastasis secondary to DTC.
Comparison of individual non-131I treatments in the overall cohort
In the total cohort of 77 patients, those who received external beam radiation therapy demonstrated a better median survival than those who did not (7.8 vs. 4.4 years; p = 0.016), and patients who received denosumab demonstrated a better median survival than those who did not (7.7 vs. 5.2 years; p = 0.03). Patients who received surgical procedures (7.8 vs. 5.9 years; p = 0.147) or bisphosphonates (7.8 vs. 6.0 years; p = 0.31) for BM seemed to have slightly improved survival, but this was not statistically significant. Patients who received arterial embolization, radiofrequency ablation cryotherapy, Cyberknife, or systemic targeted therapy did not show significant improvements in OS, this may be due to the very low patient numbers for comparison.
Comparison of individual non-131I treatments in the 131I combination treatment group
In the 131I combination treatment group of 54 patients treated, the median OS rate between patients who received surgery for BM showed no significant improvement in median OS compared to patients who did not receive surgical therapy. Out of the 24 surgeries, 15 were cranial or vertebral surgeries, and another five included fracture stabilization surgeries. No significant improvement in median OS was seen for all other non-131I treatment modalities, including external beam radiation therapy, radiofrequency ablation, cryotherapy, arterial embolization, Cyberknife, systemic targeted therapy, bisphosphonates, and denosumab. Of note, patients who did not receive a particular non-131I treatment may have received other non-131I treatment modalities.
Comparison of single versus multiple 131I treatments
The OS rate in patients who received more than one 131I treatment (median 9.4 years [CI 6.9–11.9 years]) was significantly greater than the OS in those patients who only received a single 131I treatment (median 4.3 years [CI 3.3–5.3 years]; p = 0.001). Likewise, greater cumulative 131I activities administered for BM was associated with better survival (hazard ratio = 0.998 [CI 0.997–0.999]; p = 0.028). However, radioiodine avidity of the BM as indicated on a recent diagnostic or post-therapy radioiodine scan was not associated with better survival compared to non-avid BM (median survival 7.8 vs. 6.0 years; p = 0.65). One possible reason for this lack of better survival in radioiodine-avid BM after 131I treatment could be the similar percentage of patients with other distant metastases: 65% (24/34) of radioiodine-avid patients versus 73% (8/11) of non-avid patients had other distant metastases (p = 0.73).
Prognostic factors
The univariate analysis and multivariate analysis for these prognostic factors are shown in Table 2. In the univariate analysis of the overall cohort, five factors were identified to be associated with survival: age at DTC diagnosis, age at BM diagnosis, initial 131I therapy within six months post thyroidectomy, multiple 131I treatments, and cumulative 131I activity.
Prognostic Factors of Overall Survival in 77 DTC Patients with BM Treated with 131I Adjusted for non-131I Treatment Status
Surgery included surgical excision of metastasis, stabilization, reconstruction, vertebroplasty and kyphoplasty, laminectomy and corpectomy, and hemiarthroplasty.
Systemic targeted therapy included vemurafenib, sunitinib, pazopanib, sorafenib, and lenvatinib.
Increasing age at initial thyroid cancer diagnosis and at initial BM diagnosis was significantly associated with reduced survival. When stratified, younger patients (age <55 years) at initial DTC diagnosis had a better median OS (9.4 years [CI 5.2–13.7 years]) than those aged ≥55 years (5.5 years [CI 3.9–7.0 years]; p = 0.01). Similarly, younger patients (age <55 years) at BM diagnosis had a better median OS (9.9 years [CI 8.4–11.5 years]) than those aged ≥55 years (5.2 years [CI 3.9–6.6 years]; p = 0.014). Age ≥45 years in comparison to <45 years did not show a significant effect on OS at initial DTC diagnosis (5.8 vs. 9.4 years; p = 0.126) and at initial BM diagnosis (5.5 vs. 9.4 years; p = 0.130). Although there is a trend of better survival in patients aged <45 years, a significant statistical difference could not be shown due to the low number of patients in each group.
Patients who had undergone initial 131I therapy within six months post thyroidectomy (including remnant ablation, adjuvant therapy, and metastasis treatment) demonstrated a better median survival after BM diagnosis than those who received initial 131I therapy six months or more after thyroidectomy (6.5 vs. 0.5 years; p < 0.001). Patients who had multiple 131I treatments for BM and higher cumulative 131I treatment activity for BM had better OS, as discussed previously. However, the following factors did not show a significant difference in OS (p > 0.05): sex, surgical extent (thyroidectomy vs. lobectomy), histology (papillary vs. follicular), presence of other metastasis or tumor, synchronous DTC + BM diagnosis (synchronous vs. metachronous), having BM signs/symptoms, and number of BM sites at initial diagnosis (single vs. multiple). In the multivariate analysis of the overall cohort, the only independent prognostic factors were age (<55 years) at initial DTC diagnosis, initial 131I therapy within six months post thyroidectomy, and multiple 131I treatment.
Discussion
The data shown here support the use of the combination of 131I treatment and non-131I localized and systemic treatments compared to 131I treatment alone to improve the OS of patients with BM secondary to DTC. In addition, the study helps to address some of the limitations of the previous studies. Specifically, the study (i) evaluated non-131I localized or systemic treatments in combination with 131I treatment, as well as in conjunction with dosimetrically-guided 131I treatment activities; (ii) reports results specific to DTC; and (iii) used OS as the endpoint.
The cohort of DTC patients with BM treated with 131I combination treatment (82% received dosimetrically guided activities) had better survival than those treated with 131I alone. Furthermore, a greater number of and higher cumulative activities of 131I treatments were independent prognostic factors for better survival. This result is supported by a study by Jentzen et al. (32) in which 124I lesional dosimetry was performed in a total of 61 bone lesions in 10 patients who received dosimetrically guided activities of 131I. They found that high lesional absorbed dose was associated with high response rates. Several studies have found that a combination of 131I treatment with surgery (22,26,27), arterial embolization (28), cementoplasty, cryoablation, radiofrequency ablation (29), and anti-resorptive medication (5) were associated with better outcomes, survival, or less skeletal-related events. However, no study has compared each modality to dosimetric 131I. Studies by Pittas et al. (14) and Wu et al. (24) included patients with BM treated with and without dosimetric 131I. No comparison was made with combination therapy by Pittas et al. (14). However, in comparing surgery versus no surgery for DTC BM, Wu et al. (24) reported a better five-year survival rate (80% vs. 71%).
The present study also found that initial 131I therapy within six months post thyroidectomy seemed to be associated with better OS in DTC patient with BM. However, there may be other reasons for this association apart from the effect of the initial 131I therapy itself, for example: (i) the inclusion of low-risk DTC patients who did not receive 131I within six months post thyroidectomy and who may have been followed less frequently and less closely until they presented, despite their low risk, with BM; or (ii) patients with advanced disease or poor prognosis may have received other treatment modalities (e.g., focal radiation therapy, radiofrequency ablation, surgery) prior to the initial 131I therapy, thereby delaying the initial 131I therapy for six months or more.
The study presented here evaluated the prognostic variables affecting survival and found that younger age (<55 years) was the only independent prognostic factor associated with better survival in patients treated with 131I for BM. Many of the previous studies compared age groups stratified at 45 years, which is in accordance to the seventh American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) staging. The current study adopted the age cutoff of 55 years based on the more recent updated eighth AJCC TNM staging. Previous studies such as those by Petrich et al. (6) and Choi et al. (33) described a distinct advantage for patients treated with 131I, particularly if they were younger (<45 years) (2,6,23,34). The few studies that did not detect an OS difference between age groups (<45 years vs. ≥45 years) may have been limited by an insufficient number of patients to detect a difference (15). A possible reason for OS difference between age groups is that older patients may have more advanced (e.g., multiple metastases) or dedifferentiated disease, and hence these patients are less likely to have improved survival from 131I treatment alone. In addition, although it was found that external beam radiation therapy may also be favorable for survival, this was not significant in the multivariate analysis (p = 0.06). Several other studies have found that post-thyroidectomy 131I therapy (including remnant ablation, adjuvant therapy, and metastasis treatment) (33), extent of BM (6,7,35,36), presence of other metastasis (7), serum stimulated thyroglobulin level at the initial 131I therapy (33), presence of skeletal-related events (33), bone surgical treatment (7,22), and therapy with zoledronic acid (5) are associated with outcome, prognosis, and survival. However, these factors were not found to be significant in this study. Two possible reasons are that (i) this study consists of a select group of patients from a tertiary medical center where DTC patients are referred for dosimetrically guided 131I therapy, which may represent more difficult cases of BM; and (ii) patients who received other non-131I treatment modalities may have more symptomatic or widespread disease than those who did not receive these additional treatment modalities.
This study has multiple limitations. First, it was a retrospective study with a small number of patients because many patients were not regularly followed up at the authors' tertiary referral hospital. Second, each patient was managed individually, and as a result, there were many confounding factors that could not be controlled. One major confounding factor is the variability of one or more non-131I localized or systemic treatments that were used along with the 131I treatment. In addition, these non-131I treatments were not standardized but were individualized. Another limitation is that the possibility cannot be excluded that better survival was not causally related to more non-131I treatments, but rather that the improved survival allowed more non-131I treatments. Patients considered too frail for various therapies (e.g., surgery or external beam radiation) may be selected for repeated 131I treatments thereby introducing a potential bias. Finally, although the data support improved OS with additional localized or systemic non-131I treatments, the study could not specifically evaluate which specific patients with BM should receive non-131I localized or systemic treatment or which specific non-131I localized or systemic treatment should be used. However, despite these limitations, this study presents data that help support the use of non-131I localized or systemic treatments in combination with 131I treatment to improve OS.
With the combination of localized therapy with 131I therapy to improve OS of patients with multiple BM secondary to DTC, rethinking some of the management approaches in selected patients may be warranted. For example, a frequent conventional management approach in a patient with multiple BM from DTC without any other evidence of distant metastases is to consider administration of 131I treatment first. If the patient has a BM with significant pain or an impending fracture, then additional localized treatment may be considered for palliation. However, in rethinking the management approach, perhaps localized treatment should be combined with and administered first before 131I treatment, with the objective of improving OS and not just palliation. This may be especially important when the BM that is to be targeted by localized therapy shows markedly increased 131I uptake. Specifically, if the patient has four 131I-avid BM and one of those metastases has markedly increased 131I uptake, perhaps the metastasis with the markedly increased 131I uptake should be treated first with localized therapy (e.g., surgery, external beam radiation, radiofrequency ablation, etc.). Subsequently, the other three BM may be treated with 131I. This unconventional management approach would achieve the following: after the localized ablation of the markedly increased 131I uptake in the index BM, the residence time of the 131I in the patient's whole body and blood should now be faster (i.e., faster clearance time). This, in turn, should increase the dosimetrically guided maximal tolerated 131I therapeutic activity that could be administered. If an increased 131I therapeutic activity is administered, the remaining three radioiodine-avid BM should receive increased absorbed doses.
In contrast to the above, if the patient has four 131I-avid BM, and one of those metastases has no apparent 131I uptake on a diagnostic radioiodine scan, perhaps that patient should be treated first with 131I and then subsequently treated with localized non-131I modalities such as external beam radiation. Frequently, BM that are negative on a diagnostic radioiodine scan may be positive on a post-therapy scan (37). Thus, if the metastases are positive on the post-therapy scan, the administration of the 131I before external beam radiation may help to deliver an increased absorbed dose to the metastasis than if the external beam radiation had been administered first. Based on the data supporting improved OS from the combination of localized therapy with systemic 131I therapy, reconsideration and discussion of conventional management approaches are warranted.
Although further prospective studies are recommended to evaluate this group of patients, it is recognized that such prospective studies will be very difficult to perform because there are so many confounding factors that will be difficult to control in this group. A partial list of these variables is shown in Table 3. Although management approaches are certainly sought that make treatment decisions simple and efficient for patients and physicians, this is not the case for patients who have BM secondary to DTC. In the interim, individualization of the management of these patients is recommended, with consideration of not only the many factors listed in Table 3 but also physician/facility capabilities and patient desires.
List of Confounding Factors of Studies on Treatment of BM Secondary to DTC
In patients with BM secondary to DTC, combining localized or systemic non-131I treatments with 131I treatments improved OS relative to 131I treatments alone, and OS may be an additional objective of non-131I localized or systemic treatments. Of course, further studies are needed to refine how to select which patients and which non-131I localized or systemic treatments with 131I treatment are likely to achieve improved OS. However, until further data are available, each patient should be individually managed.
Footnotes
Acknowledgments
This manuscript was underwritten by charitable donations from patients.
Author Disclosure Statement
D.V.N. is a speaker and advisor for Jubilant DraxImage. No competing financial interests exist for the remaining authors.