
Abstract
Background:
Follicular-patterned thyroid nodules predominantly composed of macrofollicular structures without nuclear atypia are generally regarded as benign (i.e., hyperplastic nodules or follicular adenomas). In line with this concept, fine-needle aspiration cytology (FNAC) also assigns a benign connotation to the presence of macrofollicular structures, unless thyrocytes present papillary thyroid carcinoma (PTC)-related nuclear features that raise the possibility of a macrofollicular variant of PTC. However, cases showing macrofollicular architecture, capsular invasion, and no PTC features can also be observed.
Methods:
We describe the clinical, cytological, histological, and molecular genetic features of four cases of encapsulated follicular neoplasms that presented histologically with a predominant (>70%) macrofollicular architecture, but which also showed clear signs of capsular invasion, and thus were classified as macrofollicular variant of follicular thyroid carcinoma (MV-FTC).
Results:
Cytologically, macrofollicular structures were identified in all cases, leading to a benign FNAC diagnosis in three of the four cases. Due to increasing nodule size, thyroidectomy was performed in all cases. Histology showed focal and limited capsular invasion, without vascular invasion. Next-generation sequencing (custom 394 gene panel) of each tumor compared with matched normal DNA revealed a total of 7 somatic variants, including dual (likely biallelic) mutations in the DICER1 gene in 2 patients. The clinical outcome was excellent in all cases.
Conclusions:
Similar to the classical minimally invasive follicular thyroid carcinoma, MV-FTC appears to behave indolently. MV-FTC has a high rate of false-negative FNAC results, but MV-FTC is very rare (<0.05% of all thyroidectomies) and apparently has an indolent behavior. Further studies comprising larger series are necessary to better clarify the biology of this diagnostically challenging rare tumor.
Introduction
Thyroid carcinoma is the most frequent endocrine neoplasm, and its incidence has been increasing over past decades (1 –3). With an estimated 316,000 new cases in 2015, it represents about 2% of all cancers (3). The most common thyroid malignancy is papillary thyroid carcinoma (PTC), accounting for about 80% of all thyroid malignancies, followed by follicular thyroid carcinoma (FTC), which represents 10–15% of cases. Both cancers are considered well-differentiated thyroid carcinomas and have generally a relatively good prognosis.
The architecture of FTC resembles that of follicular adenoma, with follicular, trabecular, and solid areas that can be mixed in the same lesion. The follicular architecture is usually made up of small-sized follicles that have no PTC nuclear features and display hyperchromatic oval nuclei with granular chromatin and regular contours. Malignancy is defined by the presence of capsular and/or vascular invasion. As a dogma in thyroid pathology, the more colloid and macrofollicular structures a thyroid lesion contains (without atypical nuclei), the more likely it is benign. The most important prognostic marker for FTC is the extent of invasion.
In the current WHO classification of thyroid neoplasms, FTC is divided into three main pathological categories: (i) minimally invasive, when only capsular invasion is seen; (ii) encapsulated angioinvasive, when vascular invasion is found in the capsule (irrespective of the number of blood vessels involved); and (iii) widely (i.e., grossly) invasive, which is often admixed with poorly differentiated thyroid carcinoma (4). Cases with only capsular invasion show an excellent prognosis, with few adverse outcomes observed (5,6). The 2015 American Thyroid Association (ATA) guidelines recommend distinguishing FTC with capsular invasion alone, FTC with minimal vascular invasion (<4 blood vessels), and FTC with extensive vascular invasion (≥4 blood vessels) (7).
With the exception of oncocytic Hürthle cell carcinoma, which is now classified separately from FTC according to the WHO, a concept that is strongly supported by recent studies demonstrating an unique and distinct genomic landscape (8 –10), variants of FTC are uncommon to rare and include primarily the clear cell variant and the mixed medullary and follicular variant. Some FTC are described as having an insular, solid, trabecular, or macrofollicular component, but the clinical significance of these findings is uncertain; these are not currently considered specific FTC variants according to the WHO criteria (4).
The first description of the macrofollicular variant of follicular thyroid carcinoma (MV-FTC) was reported in 2009, with a second case described in 2013, both by our group (11,12). Since then, no other reports describing this entity have been published. This may not be attributed only to the rarity of MV-FTC but is probably also related to underdiagnosis due to insufficient knowledge of its existence, including lack of explicit recognition by the WHO classification. Herein, we present two additional cases of MV-FTC and describe the cytological, morphological, immunohistochemical, and molecular genetic features of all four known cases to better define this rare entity and to raise awareness among cytopathologists and clinicians about the diagnostic challenges of this very rare tumor.
Patients
Cases #1 and #2
These two cases have been reported previously (11,12). Both patients were female, 28 and 37 years old (Table 1). They were operated because their respective nodules increased in size. The nodules were made up of >70% of macrofollicles, with a mean surface area per follicular structure of 48,343 and 31,415 μm2, respectively, considering that normal follicular structures (i.e., normofollicles) have a mean surface area of 10,145 μm2 (11).
Clinicopathological Features of the Four Patients and Their Respective Thyroid Nodules Diagnosed as Macrofollicular Variant of Follicular Thyroid Carcinoma
F, female; FNAC, fine-needle aspiration cytology; IHC, immunohistochemistry; n.a., not available; PTC, papillary thyroid carcinoma; US, ultrasound.
Case #3
A 39-year-old female with an unremarkable personal and family history underwent two fine-needle aspiration cytology (FNAC) procedures with a 2-year interval because of a growing nodule in the left thyroid lobe. Both FNAC were benign according to The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) (13). She was admitted to surgery 12 months after the second fine-needle aspiration (FNA) because of persistent growth of the nodule that reached 3.7 cm in diameter (Table 1).
Case #4
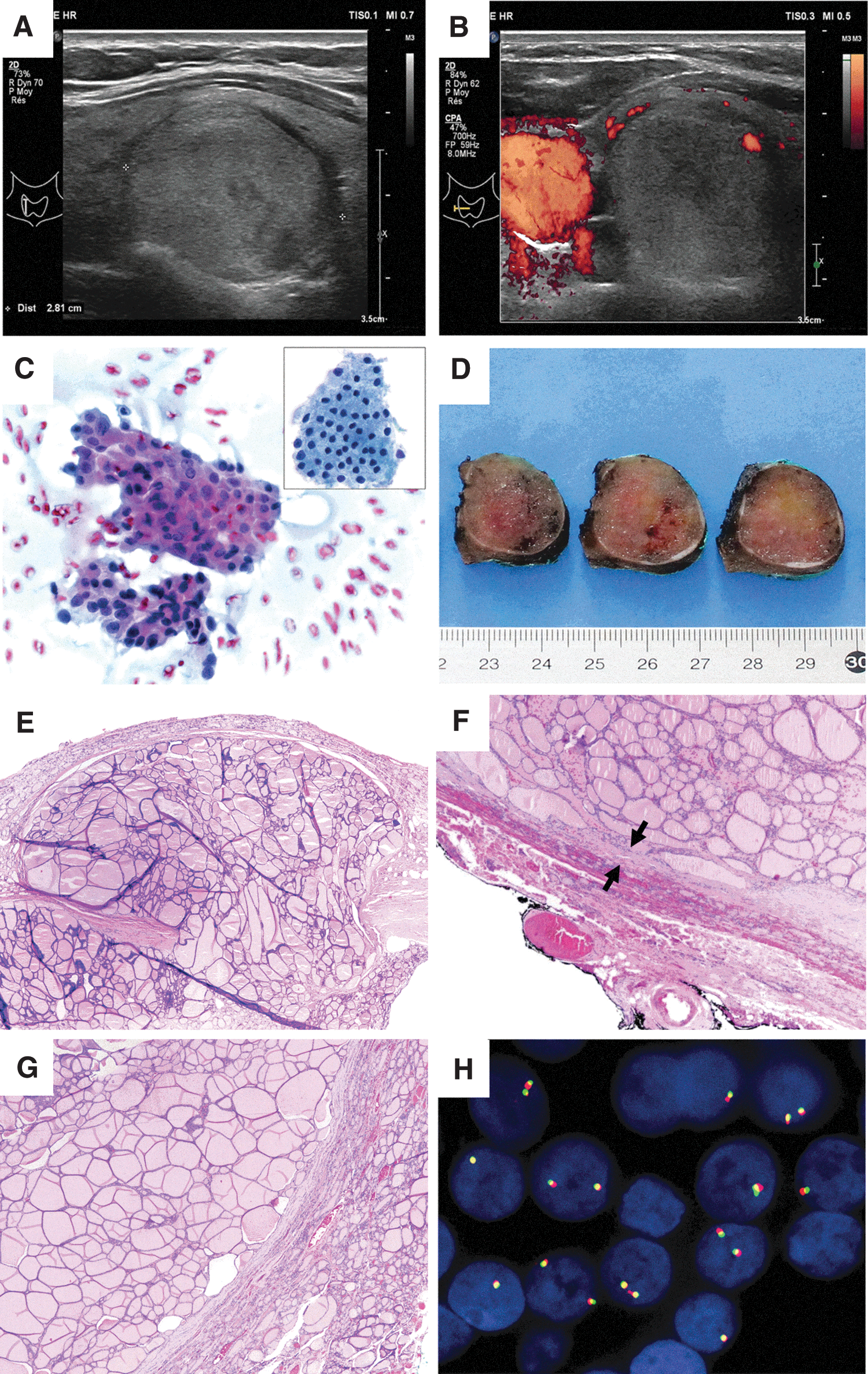
A 52-year-old female presented with a palpable lump on the right side of her neck. Ultrasound revealed a 2.8 cm nodule in the right thyroid lobe, for which an FNAC was performed and returned a benign result. The patient underwent right hemithyroidectomy and gross inspection showed a 3 cm colloidal nodule (Table 1).
Materials and Methods
Clinical and morphological examination
Cases #1 and #2 were diagnosed at ADMED Laboratories, Pathology section, Neuchatel; case #3 was diagnosed at the University Hospitals of Geneva, and case #4 was diagnosed at the University Hospital of Lausanne, Switzerland, by different pathologists of the respective institutions. The diagnosis was also reviewed and discussed by a team of expert thyroid pathologists (M.B., M.P., and C.D.V.). These four cases represent roughly <0.05% of all thyroidectomies in our institutions.
All tissues were formalin-fixed paraffin-embedded (FFPE) and stained with hematoxylin–eosin (H&E) for histopathological evaluation. According to the original histopathological reports and according to our hospitals' procedures for encapsulated thyroid nodules, the capsule and the entire nodule were thoroughly examined in all cases. The following clinical data were gathered for each case: family history, sex, age, tumor localization, symptoms, and lymph node or distant metastases present at imaging. Immunohistochemistry was performed on the Ventana BenchMark automat (Ventana Medical Systems, AZ) on 4 μm thick sections of a representative FFPE tissue block, using the following antibodies: Galectin 3 (clone 9C4, dilution 1:100, Novocastra; Leica Biosystems, Newcastle Upon Tyne, United Kingdom) and anti-Mesothelial Cell (clone HBME-1, dilution 1:100; Dako, Glostrup, Denmark).
Molecular genetic analyses
For each case, extensive molecular analyses were performed on a representative FFPE tissue block to search for genetic alterations, including the most frequent ones reported in thyroid carcinomas, that is, mutations in HRAS, KRAS, NRAS, and BRAF, as well as PAX8-PPARG and RET-PTC translocations.
Targeted next-generation sequencing was used for mutational analysis, performed in parallel on tumor and matched nontumor DNA extracted from FFPE tissue sections. The regions of interest (corresponding to areas with at least 80% tumor cells and to areas of normal thyroid tissue, respectively) were selected on an H&E-stained slide, enriched by manual scraping on corresponding toluidine blue-stained sections, and collected for DNA extraction (Maxwell 16 FFPE Plus LEV DNA Purification kit; Promega, Madison, WI).
Starting from 100 ng DNA, capture-based targeted high-throughput sequencing was performed with a KAPA HyperPlus library preparation kit (Roche, Pleasanton, CA), followed by hybridization capture using a custom design of xGen Lockdown Probes (Integrated DNA Technologies, Coralville, IA) covering the full coding sequences of 394 cancer-associated genes (Supplementary Table S1). Enriched libraries were sequenced on a NextSeq 550 instrument (Illumina, San Diego, CA).
Sequence analysis was based on established algorithms and pipelines according to the GATK (The Genome Analysis Toolkit) standards. Briefly, forward and reverse reads were aligned to the human genome (GATK repository, build 37 decoy) using BWA-MEM (v0.7.5a). BAM files were subjected to PCR duplicate removal (Picard GATK v4.0.9), followed by realignment around indels and base recalibration using GATK tools (v4.0.9). Single nucleotide variant (SNV) and indel variant calling was performed using samtools mpileup (v1.9-2) and VarScan (v2.4.3) as well as MuTect2 algorithm (GATK v4.0.9), comparing tumor versus matched normal samples. Raw variant calls were annotated for presence in the dbSNP and COSMIC databases, as well as the mutation effect on the gene transcript by SnpEff (v.4.3t). SNVs and indels were filtered based on coverage, quality, and variant allele frequency (threshold of 5%).
Furthermore, variants were filtered using their biological impact as well as a panel-specific list of known artifacts, collected during the validation phase of the panel. All retained alterations were confirmed by visual inspection with the IGV software. Effects on splicing were assessed using the “Human Splicing Finder—version 3.1” web tool. Copy number variation (CNV) analysis was performed starting from aligned sequencing data (BAM files) using FACETS package with default settings.
For gene translocation analysis, interphase fluorescence in situ hybridization (FISH) assays were performed on 4 μm thick sections using break-apart probes for RET and PPARG genes (ZytoLight SPEC RET Dual Color Break Apart Probe; ZytoVision, Bremerhaven, Germany, and Kreatech PPARG (3p25) Break FISH probe; Leica Biosystems, Nussloch, Germany), according to the standard protocols. These assays are able to detect RET and PPARG gene rearrangements, irrespective of their translocation partners.
Results
Histological examination
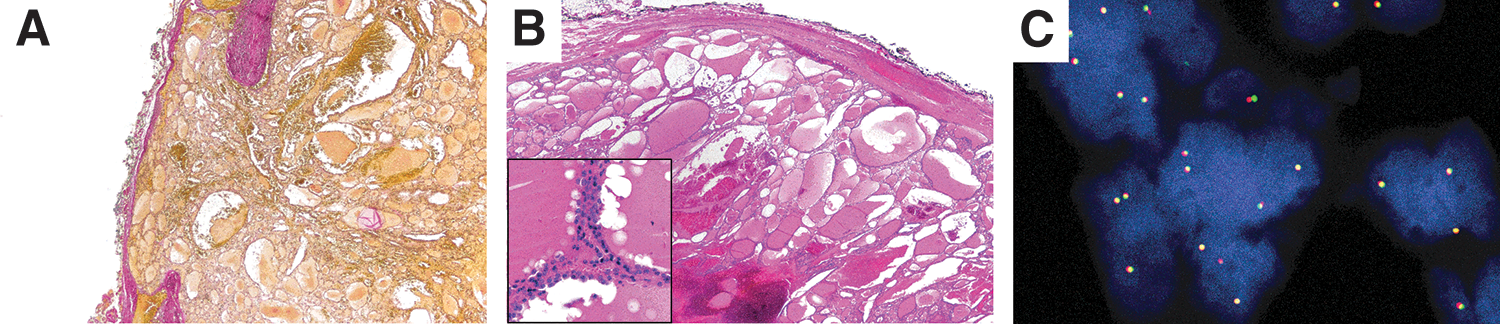
The most important pathological features are summarized in Table 1. On gross morphology, all nodules had a colloid appearance. This was compatible with the histological appearance of the specimens, which were found to be made up of >70% of macrofollicles. There were no areas of necrosis, oncocytic features, or nuclear features of PTC. Vascular invasion was not seen in any case, while capsular invasion was detected in all cases: two foci in case #1, four in case #2, one in case #3, and two in case #4 (Figs. 1 and 2). The initial diagnosis of MV-FTC was confirmed in all cases by the expert reviewers.
(
(
Molecular analysis
The four tumors and their matched normal samples were sequenced at a mean coverage of 1396 × (range 760–2106 × ) and 353 × (range 197–498 × ), reaching a proportion of targeted sequencing covered with more than 100 × of 99% and 94%, respectively. We observed in total seven somatic variants (Table 2), of which five nonsynonymous alterations and two affecting splice sites. All but one variant (a POLE missense mutation of unknown functional significance, detected at a low allele frequency of 5% in patient #3) were classified as probably pathogenic. Notably, two tumors (patient #1, patient #2) showed dual somatic mutations of the DICER1 gene (one missense variant in each patient with an additional splice site or frameshift variant) suggesting a double-hit event, although they were too far apart to assess whether they were in cis or in trans. No mutation was detected in the hotspot regions of HRAS, KRAS, NRAS, and BRAF.
Mutations Detected by Targeted Sequencing
ACGS class: based on the recommendations of the ACGS: class 3, variant of uncertain significance; class 4, likely.
ACGS, Association for Clinical Genomic Science.
CNV analysis revealed a stable chromosomal landscape in all cases, with very few and inconsistent copy number alterations (Table 3), namely some low-level copy gains and deletions, including a focal heterozygous loss of CDKN2A locus in patient #3.
Copy Number Variations Detected by Targeted Sequencing
CNV, copy number variation.
Break-apart FISH assays for RET and PPARG did not show any rearrangement nor any significant CNV of these loci.
Discussion
The clinical, pathological, and molecular genetic profiles of this well-documented yet unique case series of MV-FTC highlight several issues that concern not only this particular variant but also the diagnosis and management of thyroid carcinomas more generally.
The first issue is the role of FNAC in diagnosing macrofollicular-patterned thyroid neoplasms. FNAC is an excellent diagnostic test for classical PTC and most PTC variants, including the macrofollicular variant (14), since the diagnosis is based mainly on specific nuclear features including chromatin clearing, nuclear grooves, and pseudoinclusions associated with specific architectural features such as papillae. Conversely, FNAC is considered as a screening test for all follicular-patterned lesions, for which the diagnosis of malignancy relies on evidence of capsular or vascular invasion, aspects that cannot be assessed cytologically. Since FTC does not display nuclear atypia (in the sense of PTC), a suspicion for FTC can be raised only when there is a predominance of microfollicles, hence the difficulty in diagnosing FTC by FNAC. Indeed, follicular neoplasms predominantly composed of microfollicles (i.e., no more than 12 follicular cells composing the follicle section), including noninvasive follicular thyroid neoplasm with papillary-like nuclear features, require surgery to be classified correctly. A definitive distinction between these entities is not possible on cytological material.
Even more problematic is the cytological diagnosis of follicular neoplasms showing a macrofollicular pattern, which have been generally and traditionally considered to be benign (benign follicular nodules). However, it is worth noting that macrofollicular-patterned lesions may occasionally also include malignant neoplasms, such as in the macrofollicular variant of papillary thyroid carcinoma (MV-PTC). Therefore, the follow-up of patients with a benign FNAC diagnosis, according to the ATA guidelines, takes into account the presence or absence of suspicious ultrasonographic findings as well as the nodule's tendency to grow or remain stable, even though these features are not pathognomonic either. The current diagnostic approach for follicular-patterned lesions is highly effective for the diagnosis of benign lesions, with a negative predictive value of around 95–98%. In line with this approach, three of the four cases of MV-FTC were diagnosed as benign on FNAC; they were treated surgically due to their large and progressively increasing size. The single case cytologically diagnosed as suspicious for PTC presented pseudopapillary structures and slightly atypical nuclei (that were overinterpreted as worrisome), in addition to abundant colloidal material in the background (which is mostly a sign of colloidal and benign nodules); after expert revision, it was concluded that this FNAC specimen should have been diagnosed as benign.
The second issue concerns the true nature of capsular invasion. The example of MV-FTC poses the following question: can foci of apparent invasion at the level of the capsule be attributed to increased intratumoral pressure caused by macrofollicles filled with colloid, with secondary herniation of thyroid tissue through areas where the capsule is the thinnest or weakest (by a mechanism similar to that of pseudoinvasion in benign pseudodiverticulae of the colon), rather than by true neoplastic invasion? In our cases, we excluded an artifactual pseudoinvasion related to the FNA passes, because there was no inflammatory or fibrotic reaction that is usually seen in this context. In addition, surgeries for all cases were performed more than 3 weeks after FNAC, and therefore, any acute changes following FNAC (the so-called “worrisome histological alterations following fine-needle aspiration of the thyroid,” WHAFFT) present initially in the nodule should no longer be observed in the histological specimens (15 –17). Chronic changes related to FNA (fibrosclerotic stroma and lymphocytic infiltration) were also absent. Beyond excluding FNA as a cause of apparent capsular invasion, it is not possible to further address the open question of the mechanism of capsular invasion in MV-FTC.
The third issue concerns the accuracy of FNAC diagnosis and the possible differential diagnoses. Although the histological criteria for the diagnosis of FTC are well defined in the WHO classification of thyroid tumors, these criteria have been difficult to apply in practice and have even led to confusion, because the definition of true capsular and vascular invasion is still a matter of debate among expert pathologists (4,6,18,19). As a result, given the difficulty in precisely diagnosing FTC, it is not surprising that there is substantial intra- and interobserver variation in diagnosis. For this reason, before starting the present investigation, all the slides were reviewed by each participating expert thyroid pathologist (M.B., M.P., and C.D.V.) to confirm the presence of capsular invasion. Vascular invasion was never seen, and thus, all cases were diagnosed as minimally invasive according to the WHO classification (4). We also excluded the diagnosis of MV-PTC, because the nuclei in our cases did not show any nuclear feature suggestive of PTC. In case #1, the FNAC diagnosis of “suspicious for PTC” had been motivated by the presence of papillary structures and clear chromatin, but these features were not confirmed histologically, where only focal papillary hyperplasia without nuclear atypia was observed. It is noteworthy that some cases of MV-PTC can also be missed by FNAC, as these entities can present only with focal features of PTC (20,21).
Apart from the two cases previously described in the literature that correspond to case #1 and case #2 of the present series, we have not found any other reports or descriptions supporting the actual existence of MV-FTC. Our explanation is that pathologists must certainly have encountered cases such as the ones described in the present report, but probably have not reported them as such. For example, Sclabas et al. have stated that FTC may have a macrofollicular pattern, making the differentiation with adenomatoid nodules difficult (22). It is tempting to suggest that a subset of the so-called “benign metastasizing goiter” cases, already described in 1876, could potentially represent underdiagnosed MV-FTCs, in addition to MV-PTCs (23,24). In a Japanese study in 2008, the prevalence of “benign nodular goiter” showing metastasis to regional or distant organs was 0.17% (5 of 2978 cases) (24). Because MV-FTC is likely to yield a false-negative diagnosis on FNAC and possibly also on histopathology results, it is important to raise awareness of this entity among clinicians and pathologists alike. The existence of this variant can also contribute to justify the recommendation for ultrasound follow-up of nodules after an initial benign FNAC diagnosis (25).
Considering the molecular analyses, performed in parallel on the four tumors and matched normal tissues, we were quite surprised to find two patients (cases #1 and #2) with similar double somatic DICER1 alterations, which are likely biallelic in both cases. The c.5113G>A (p.Glu1705Lys) and c.5428G>C (p.Asp1810His) missense variants, each identified in one patient, are hotspot mutations affecting the RNase IIIb domain of the DICER1 gene and have previously been described in numerous DICER1-related tumors, typically arising postzygotically (26). As has been seen in nearly all DICER1-related tumors, these hotspot missense mutations are usually accompanied by loss-of-function pathogenic variants occurring on the other allele (i.e., in trans, resulting in biallelic alteration of DICER1). In our two patients, the above missense DICER1 variants were each coupled with a splice site or a frameshift variant, also proven to be somatic in origin by comparing tumor and normal tissue. Although we were unable to show that these variants occurred indeed in trans, it is reasonable to assume that this is the case. The involvement of DICER1 in differentiated thyroid cancer (DTC) was first demonstrated in four unrelated DICER1 syndrome pedigrees (27,28), and subsequent studies have identified germline DICER1 variants in familial DTC, not selected because of known DICER1 syndrome features in the family history (29). Nevertheless, studies of unselected series of both adult and pediatric DTC have identified biallelic somatic, rather than germline DICER1 mutations (30). By contrast, early-onset multinodular goiter appears to be strongly linked to pathogenic germline DICER1 variants (30 –32). The two lesions that harbored DICER1 mutations did not show any particular cytomorphological features, nor were they morphologically different from the other two tumors that did not show DICER1 alterations.
Mutations affecting the hotspot A113 splice site of the EIF1AX gene have been described as drivers in thyroid tumorigenesis and have been identified so far in a wide variety of follicular-derived thyroid lesions, including hyperplastic nodules (1.3%), follicular adenomas (7.4%), PTCs (2.3%), Hürthle cell carcinomas (33), and anaplastic thyroid carcinomas (25%, often coexisting with other mutations such as TP53 or TERT promoter alterations) (34,35), but not in FTCs.
In our series, we found a POLE missense mutation of unknown functional significance, detected at a low allele frequency of 5% in one case only. Interestingly, in a series of fatal nonanaplastic thyroid cancer, mutations in the POLE gene were seen in 4/57 (7%) patients, suggesting a potential role for this gene in tumor aggressiveness (36).
The last issue concerns the prognosis and biological significance of MV-FTC. In our cases, foci of capsular invasion were limited, and the clinical course of the patients suggests an indolent nature of these neoplasms. The present cases did not show vascular invasion and did not express Galectin-3 and HBME-1, which are considered general markers of thyroid malignancy. It is important to note that our present findings do not justify any deviation from current guidelines regarding the diagnosis and management of thyroid nodules in routine clinical practice. This is due to the extremely low number of cases described so far (four in total); the very low frequency of this entity (estimated to be <0.05% of all thyroidectomies); the apparent excellent evolution at follow-up; and the need for more studies with a larger number of cases and longer follow-up. The increasing use of molecular tests in cytology (currently mainly limited to the indeterminate diagnostic categories), which can assess a wide and expanding number of gene mutations, might be useful in the future to screen cases that have a benign cytology but are increasing in size. The new WHO classification has made an important distinction between FTCs that have only capsular invasion (minimally invasive) and FTCs that have limited vascular invasion (encapsulated FTC with angioinvasion) or extensive vascular invasion (widely invasive), affirming that minimally invasive FTCs have an excellent prognosis (4,5). More importance is thus given to vascular invasion, which, if present, is considered a sign of a worse prognosis. Further studies should examine whether different architectural features of FTC (not only macrofollicular changes but also clear cell, solid, trabecular, and other alterations) have an impact on prognosis.
In conclusion, we describe the clinical, cytological, histological, and molecular genetic features of a MV-FTC. This variant cannot be diagnosed or suspected by FNAC as it is predominantly composed of macrofollicles, and for this reason, it is likely to be classified in the benign diagnostic category. Similar to the classical minimally invasive FTC, the MV-FTC appears to behave indolently. Raising awareness of this entity among clinicians and pathologists alike is important and may lead to studies comprising larger series to better clarify the molecular alterations and the biology of this diagnostically challenging but rare tumor.
Footnotes
Acknowledgment
We are grateful to Prof. J. Rosai, Centro Diagnostico Italiano, Milan, Italy, for his review of the histology of case #1.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
G.P.S. is partly supported by a Leenaards Foundation Fellowship for Academic Promotion in Clinical Medicine. W.D.F. is funded by a Foundation grant from the Canadian Institutes of Health (Grant No. 2016).
Supplementary Material
Supplementary Table S1