
Abstract
Background:
Tumor volume (TV) of papillary thyroid carcinoma (PTC) increases exponentially during active surveillance, and the growth rate differs for each patient. TV doubling time (TVDT) is considered a strong dynamic marker for the prediction of the growth rate and progression of the tumor.
Methods:
This cohort study analyzed 273 PTC patients who underwent active surveillance for more than one year rather than immediate thyroid surgery. TVDT was calculated in each patient, and patients were divided into two groups: rapid-growing (TVDT <5 years) and stable (TVDT ≥5 years). Clinical and initial ultrasonography (US) features between the two groups were compared.
Results:
The median patient age was 51.1 years (interquartile range [IQR] 42.2–61.0 years), and 76% of the patients were women. The initial TV of PTC was 62.1 mm3 (IQR 28.1–122.8 mm3). During a median of 42 months (IQR 29–61 months) of active surveillance, 10.3% of the patients had a TVDT of less than two years, 5.1% had a TVDT between two and three years, 6.2% had a TVDT between three and four years, 6.6% had a TVDT between four and five years, and 71.8% had a TVDT of five years or more. Patients in the rapid-growing group (77 patients; 28.2%) were significantly younger (p = 0.004) than those in the stable group (196 patients; 71.8%). Being younger than 50 years of age was significantly associated with rapid tumor growth of PTC (odds ratio = 2.31 [confidence interval 1.30–4.31], p = 0.004) in multivariate analysis. In ultrasound findings, macrocalcification was independently associated with rapid tumor growing of PTCs (odds ratio = 4.98 [confidence interval 2.19–11.69], p < 0.001).
Conclusions:
TVDT is a good indicator for presenting the growing velocity of PTCs during active surveillance. Younger age and macrocalcification in the initial US were associated with rapid-growing PTCs. Determination of TVDT during the early phase of active surveillance may be helpful for the prediction of rapidly progressing PTCs and deciding whether to adopt an early surgical approach.
Introduction
Active surveillance is an alternative treatment option to immediate thyroid surgery for patients with low-risk papillary thyroid carcinoma (PTC) (1). Some PTCs may progress during active surveillance (2 –6). Therefore, it is essential to identify PTC patients who are likely to progress or to be stable for a long time in the early phase of active surveillance. However, biological or molecular predictive markers do not exist yet.
Currently, there is no gold standard for the decision for surgical intervention during active surveillance of PTCs. Tumor volume (TV) doubling time (TVDT) is considered a strong dynamic marker for the prediction of the growth rate and progression of solid tumors, including PTC (7 –10). In a lung cancer screening program, TVDT has been proposed as a tool to mitigate overdiagnosis (10). One recent study suggested that the exponential growth of PTC during active surveillance and the growth rate may differ between patients (6). Knowing the growth rate of a tumor in individual patients will be helpful for decisions about early surgical intervention and the follow-up intensity of active surveillance in PTC patients.
Ultrasonography (US) features may predict the biological behavior of thyroid cancer (11). Previous studies have suggested the possibility that biological changes may lead to a phenotypic change in neck US and that US findings may be associated with poor prognosis (12,13). Considering that US features may reflect the natural properties of thyroid nodules, they may be associated with the growth of PTC during active surveillance.
Currently, no study has evaluated the clinical implications of TVDT during active surveillance of PTCs. The aims of this study were to evaluate the growth velocity of TV by determining TVDT in each patient and to elucidate the clinical and the US features associated with rapid tumor growth during active surveillance of PTCs.
Methods
Patients and study design
The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Republic of Korea. This cohort study included 273 patients in active surveillance for more than one year after cytopathologically being diagnosed with PTC between 2002 and 2016, as previously reported (4,14). Patients with lateral cervical lymph node (LN) metastasis or any evidence of macroscopic invasion into the perithyroidal soft tissue, the trachea, or the recurrent laryngeal nerve on the initial US were excluded from the study. Patients with distant metastasis or those diagnosed with an aggressive variant of PTC on fine-needle aspiration cytology (FNAC) or core-needle biopsy (CNB) were also excluded.
Neck US examination and diagnosis of PTC
Thyroid gland and neck area images were evaluated, as previously reported (4,14). Briefly, the scanning protocol included both transverse and longitudinal real-time imaging of thyroid nodules. Neck US examinations and US-guided FNAC or CNB were performed by radiologists under the supervision of two experienced radiologists (J.H.L. and J.H.B. with 13 and 21 years of experience, respectively) and retrospectively reviewed by three experienced radiologists (H.S.O., W.G.K., and J.H.B.). Three authors discussed the findings to reach agreements on different reviews between radiologists (15). PTC was diagnosed using US-guided FNAC or CNB according to previous recommendations (16,17). A cytopathologic diagnosis was made by experienced pathologists in thyroid cytopathology. FNAC diagnoses were classified into six categories according to the Bethesda System (18), and CNB specimens were evaluated on the basis of criteria proposed by the Korean endocrine pathology thyroid CNB study group (19,20). Hashimoto's thyroiditis was defined as serum antithyroid peroxidase antibody levels >60 IU/mL, with diffuse parenchymal heterogeneity on US.
Evaluation of US findings and calculation of TV
US findings, including maximum tumor diameter, volume, location, internal content, echogenicity of solid portion, shape, margin, calcifications, and subcapsular location of the tumor, were evaluated according to previous reports (1,17,21,22). Kappa values for the intra- and inter-observer agreements of each US feature ranged from 0.61 to 0.99 (Supplementary Table S1), as previously reported (12). All nodules were evaluated with both transverse and longitudinal planes for three-dimensional evaluation and TV measurement. The maximum diameter of PTC was measured using US; in patients with multifocal PTCs, the dimensions of the largest PTC lesion were used for the assessment. TV was calculated using the following equation: TV (mm3) = length (mm) × width (mm) × thickness (mm) × π/6 (23). Tumor location was classified into upper-pole location of the right or left thyroid gland versus others. The internal content of a nodule was categorized according to the ratio of the cystic to the solid portion within a nodule such as solid (≤10% cystic) and predominantly solid (>10% and ≤50% cystic) (17). Decreased echogenicity of the nodule—compared to that of the thyroid parenchyma—was defined as hypoechogenic echogenicity. A marked hypoechogenic pattern was defined as a decrease in echogenicity compared to that of the strap muscle (17). The nodule shape was categorized as follows: ovoid to round, irregular, and taller than wide. Margins were classified as well-defined smooth, ill defined, and spiculated. Calcifications were categorized as microcalcification (calcification foci ≤1 mm), macrocalcification (calcification foci >1 mm), rim calcification (curvilinear or eggshell calcification), calcified spot (single-course calcification without visualization of the surrounding tumor), or none. When the nodule had mixed types of calcification (i.e., macrocalcification or rim calcification intermingled with microcalcification), the nodule was considered to have macrocalcification or rim calcification (24). When a nodule abutted to the thyroid capsule without any intervening thyroid parenchyma, it was identified as a subcapsular location (17).
TVDT
TVDT was determined with the calculator suggested by Kuma hospital (25). All available TVs, or at least three between the initial and last US, were used in each patient for the calculation of TVDT. Figure 1 shows an example TVDT calculation. The values for the three diameters of the thyroid nodule in all available US were entered, and TVDT was automatically calculated and presented as day, month, and year. In the analysis, TVDT is presented as TVDT <2, 2–3, 3–4, 4–5, and ≥5 years, and patients with a TV decrease were classified into the TVDT ≥5 years group. Patients were classified into two groups according to TVDT: the rapid-growing group (TVDT <5 years) and the stable group (TVDT ≥5 years).

Representative image of tumor volume doubling time calculation with the Kuma Hospital calculator. Three diameters and examination date of the patient in every ultrasonography have been entered. (
Follow-up protocol for active surveillance
The management and follow-up protocols for PTC patients during active surveillance have been previously described (4). Briefly, patients were regularly followed up with physical examination and neck US performed every 6–12 months. All patients were evaluated for both central and lateral cervical LNs by neck US. When suspicious LNs were found, FNAC of LNs with thyroglobulin levels in the washout of the needle was performed. Thyroid surgery was generally recommended when the primary tumor size was >1 cm or increased by >3 mm, TV increased by >50% from the baseline, new metastatic LNs or distant metastasis was found, or when tumor growth was toward adjacent structures, including the recurrent laryngeal nerve, trachea, and esophagus.
Statistical analysis
Statistical analysis was performed with R v3.4.0 (R Foundation for Statistical Computing, Vienna, Austria;
Results
Characteristics of PTC patients under active surveillance
This study evaluated 273 PTC patients whose median age at diagnosis was 51.1 years (IQR 42.2–61.0 years), and 115 (42.1%) patients were <50 years of age (Table 1). The age distribution of the study subjects was: six (2.2%) patients in their 20s, 38 (13.9%) patients in their 30s, 71 (26.0%) patients in their 40s, 82 (30.0%) patients in their 50s, 44 (16.1%) patients in their 60s, and 32 (11.7%) patients >70 years of age. Among the patients, 75.8% were female. The initial maximum diameter and volume of PTC on the US were 5.8 mm (IQR 4.4–7.3 mm) and 62.1 mm3 (IQR 28.1–122.8 mm3), respectively. During a median of 42 months (IQR 28.6–60.8 months) of active surveillance, 59 (21.6%) patients had a significant volume increase ≥50%, and 12 (4.4%) patients had significant maximal diameter increase ≥3 mm. During the follow-up periods, 52 (19.0%) patients underwent delayed thyroid surgery.
Characteristics of Study Participants
Continuous variables are presented as medians (interquartile range). Categorical variables are presented as frequencies (percentages).
US, ultrasonography.
TVDT and clinical features associated with tumor growth
Table 2 shows the clinical features of PTC patients according to TVDT. Among 273 PTC patients, 10.3% had a TVDT of less than two years, 5.1% had a TVDT between two and three years, 6.2% had a TVDT between three and four years, 6.6% had a TVDT between four and five years, and 71.8% had a TVDT of five years or more. The patients’ age was different as a function of different TVDT (p = 0.037). TVDT was not different according to sex, initial maximal diameter, and initial volume on US. A maximal diameter increase ≥3 mm was only found in patients with a TVDT of less than two years (nine patients) and between two and three years (three patients). About 90% of patients with a TV increase ≥50% had a TVDT of less than five years. However, 6/196 (3.1%) patients with a long TVDT (≥5 years) had a TV increase ≥50% during follow-up. There were more volume increases and maximal diameter increases in those patients with a shorter TVDT than in those with a longer TVDT (p for trend <0.001 and p for trend <0.001, respectively).
TVDT and Clinical Features Associated with Tumor Growth
Continuous variables were described as medians (interquartile range). Categorical variables were presented as frequencies (percentages).
TVDT, tumor volume doubling time.
Rapid-growing and stable group according to TVDT
Among study participants, 77 (28.2%) patients were classified in the rapid-growing group (TVDT <5 years; Table 3). Patients in the rapid-growing group were significantly younger than those in the stable group (p = 0.004). There was no significant difference in sex, initial maximal diameter, or initial TV between the two groups. Figure 2 shows the changes of logarithmically transformed actual TV in each patient during active surveillance. The TV in the rapid-growing group increased over time (Fig. 2A; p = 0.008), while the TV in the stable group remained steady (Fig. 2B; p < 0.001).
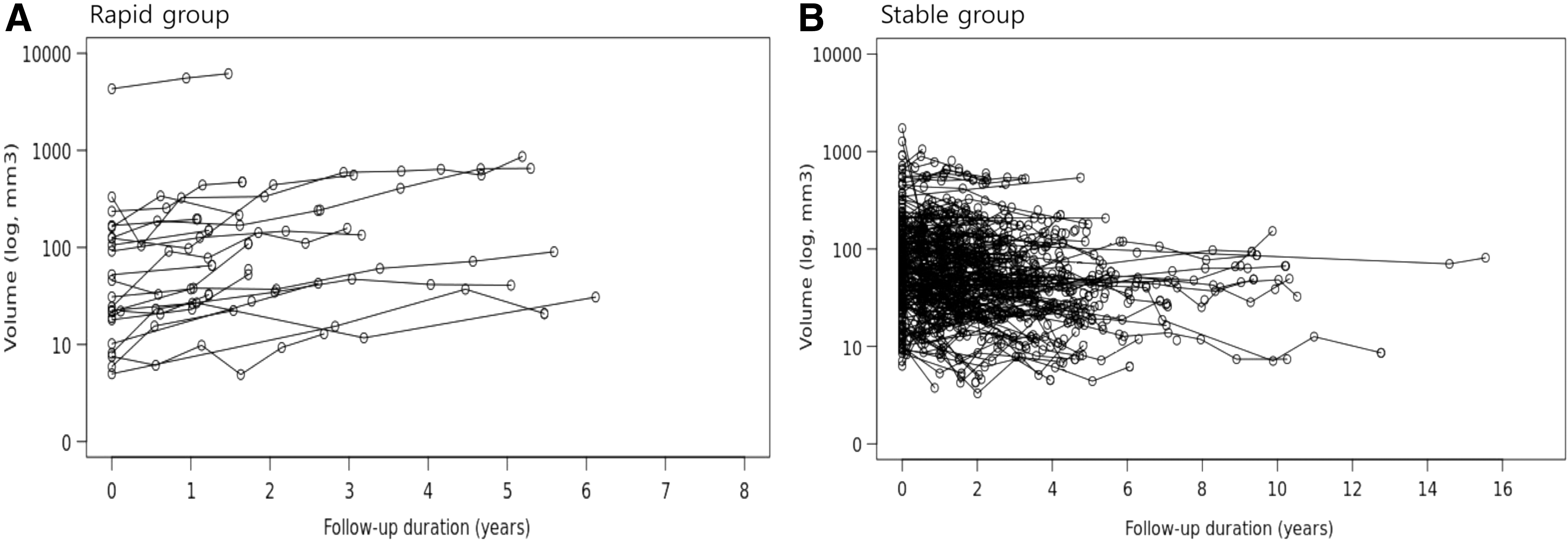
Changes in tumor volume with time. (
Clinical and Sonographic Characteristics of PTC Patients According to TVDT
Continuous variables are presented as medians (interquartile range), and categorical variables were presented as frequencies (percentages). Statistically significant values are shown in bold.
PTC, papillary thyroid carcinoma.
The US features of PTCs at the initial US were compared between the two groups. The calcification pattern was significantly different between the two groups (p = 0.001). Macrocalcification was more frequently found in the rapid-growing group (23.4%) than in the stable group (8.2%). Calcified spot and rim calcifications were found in only one patient (1.3%) in the rapid-growing group. No significant difference was found in the location, internal content, echogenicity, shape, margin, or subcapsular location of the tumor on US between the two groups.
Clinical and US features associated with a shorter TVDT of less than five years
The clinical and initial US features associated with shorter a TVDT of less than five years during active surveillance were evaluated (Table 4). In multivariate analysis, age <50 years was significantly associated with a shorter TVDT of less than five years in PTC (odds ratio [OR] = 2.31 [confidence interval (CI) 1.30–4.31], p = 0.004). Among sonographic findings, macrocalcification was independently associated with shorter a TVDT of less than five years in PTC (OR = 4.98 [CI 2.19–11.69], p < 0.001).
Clinical and Sonographic Features Associated with a Shorter TVDT of Less Than Five Years
Statistically significant values are shown in bold.
The values were adjusted for patient's age, sex, presence of Hashimoto's thyroiditis, and ultrasonography features of location, internal content, echogenicity, shape, margin, calcification pattern, and subcapsular location of the tumor.
OR, odds ratio; CI, confidence interval.
Clinicopathologic characteristics of patients who underwent delayed thyroid surgery
During active surveillance, 53 (19.4%) PTC patients underwent delayed thyroid surgery (Supplementary Table S2). The median time to surgery from diagnosis was 28.6 months (IQR 21.7–40.2 months). Among them, 32 (60.3%) patients were classified in the rapid-growing group. On the final pathology report, LN metastasis was found in 17 (32.1%) patients, and lateral cervical LN metastasis was found in two patients who were classified in the rapid-growing group. No patient showed recurrences, distant metastasis, or cancer-specific death after the initial thyroid surgery during a median follow-up period of 14.0 months (IQR 4.8–24.3 months).
Discussion
The present study determined that TVDT is a good indicator representing the velocity of tumor growth during active surveillance of PTCs. During active surveillance, 28.2% of patients had a TVDT of less than five years, and these patients may be classified as being at high risk for tumor progression. Determination of TVDT in active surveillance is advantageous because it reflects the time-dependent growth rate of PTCs. This approach of TVDT is not consistent with the current definition of significant increase of maximal diameter and relative TV increase (2,4,6). However, all patients with a maximal tumor size increase ≥3 mm had a TVDT of less than three years, and 89.8% of patients with a volume increase ≥50% had a TVDT of less than five years. TVDT can be calculated in the early phase of active surveillance (within two or three years), and it can be a helpful for the prediction of rapidly progressing PTCs and deciding whether to adopt an early surgical approach.
Previous studies have suggested that tumors in humans grow exponentially, and TV reflects the tumor growth in a more sensitive manner than a unidimensional increase in size (7,27). It was previously reported that changes in TV predicted tumor progression more sensitively in the earlier stage of active surveillance than changes in the maximum diameter, and a recent study suggested the presence of an exponential growth of PTC during active surveillance (4,6). This indicates that PTC may eventually grow in a time-dependent manner, although the growth rate may vary for each patient. Therefore, clinical indicators reflecting the growth velocity of PTCs may be useful for patients in active surveillance programs.
TVDT is an accurate dynamic indicator that predicts the growth rate of the tumor, and it can be conveniently calculated by acquiring serial neck US of the thyroid neoplasms (7,20,28). TVDT has been recommended as a strong biomarker for the prediction of tumor progression and response to therapy in many cancers (7 –10). In lung cancer, a previous study suggested that the TVDT of a lung nodule can help to mitigate overdiagnosis in lung cancer screening programs (10). This suggested that a nodule displays its own tumor growth rate in a given patient, and TVDT may indicate the need for a change in the management plan of cancer patients. TVDT can be calculated by three or four serial neck US during active surveillance. Moreover, TVDT will help to predict which patients are likely to progress rapidly or to be stable for a long time, and this approach will also minimize medical expenses by risk-adapted strategies for follow-up of PTC patients during active surveillance.
Neck US is currently the mainstay technique for detecting and evaluating thyroid nodules. Many guidelines have emphasized the role of ultrasound in the evaluation and management of thyroid disease (1,17,29,30). Certain US features such as the taller-than-wide shape, spiculated margins, and microcalcification of thyroid nodules are believed to predict malignant tumors (1,17). Previous studies have suggested the possibility that biological changes may lead to a phenotypic change in US and that US findings may be associated with poor prognosis of the tumor (12,13). It is possible that macrocalcification seen on US may be related to the growth of PTC during active surveillance. A previous Japanese study reported that PTCs with weak calcification patterns (microcalcification) tend to grow faster than those with strong calcification patterns (macrocalcification and rim calcification) (24). However, the present findings suggest that macrocalcification, rather than microcalcification, is associated with tumor growth during active surveillance. This difference is mainly due to the different definition of tumor progression and classification of calcification between the two studies. The present study adopted a more sensitive index of tumor growth using three-dimensional volumetric changes of PTCs. It also included relatively younger patients with PTC for active surveillance compared to the previous study. It is possible that microcalcification would eventually evolve to macrocalcification in PTCs. Calcification in cancer cells is a process of dystrophic calcification, and this process is evident in areas of dying tissue (31). This suggests that calcification in thyroid neoplasms might represent a biologically active tissue that can regenerate or necrosis. Therefore, rapidly growing tumors could have more calcifications. Further research focusing on US findings, particularly calcification patterns, is needed to predict the nature of PTC.
Several studies have demonstrated that age is associated with tumor growth during active surveillance (3,32,33). A recent Japanese study evaluated the progression of PTC during active surveillance by dividing patients in age decades and found that the progression rate was much higher in younger patients than in older patients (32). These results are consistent with the present findings, showing that young age is associated with a shorter TVDT of less than five years, even though this difference was not substantial. Therefore, active surveillance in younger patients should be more rigorously applied.
There are some limitations to this study. This was a single-center study, and a relatively small number of patients were included. There is a possibility of selection bias in this study. TVDT was evaluated retrospectively in this study, and there is a potential limitation of defining US characteristics because US is a dynamic examination. The follow-up duration of active surveillance was relatively short to reflect the natural course of PTCs during active surveillance. Further studies with long-term follow-up periods are required to validate the clinical impact of TVDT determined in the initial two to three years for prediction of prognosis of PTCs during active surveillance.
In conclusion, TVDT is a good indicator for the prediction of the growing velocity of PTCs during active surveillance. Younger age and macrocalcification in the initial US were associated with rapid-growing PTCs. Determination of TVDT during the early phase of active surveillance may be helpful for the prediction of rapidly progressing PTCs and prompt an early decision for a surgical approach.
Footnotes
Acknowledgments
This study was supported by the National Research Foundation (NRF) of Korea Research Grant (NRF-2018R1D1A1A02085365).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2