
Abstract
Background:
In this ongoing multicenter prospective cohort study on active surveillance (AS) in low-risk papillary thyroid microcarcinoma (PTMC), we aimed to compare the quality of life (QoL) of participants based on their choice of treatment, that is, AS or immediate surgery (OP).
Methods:
QoL of 203 participants who chose AS and 192 participants who underwent OP was evaluated using a thyroid-specific QoL questionnaire at diagnosis and during follow-up (median 8 months).
Results:
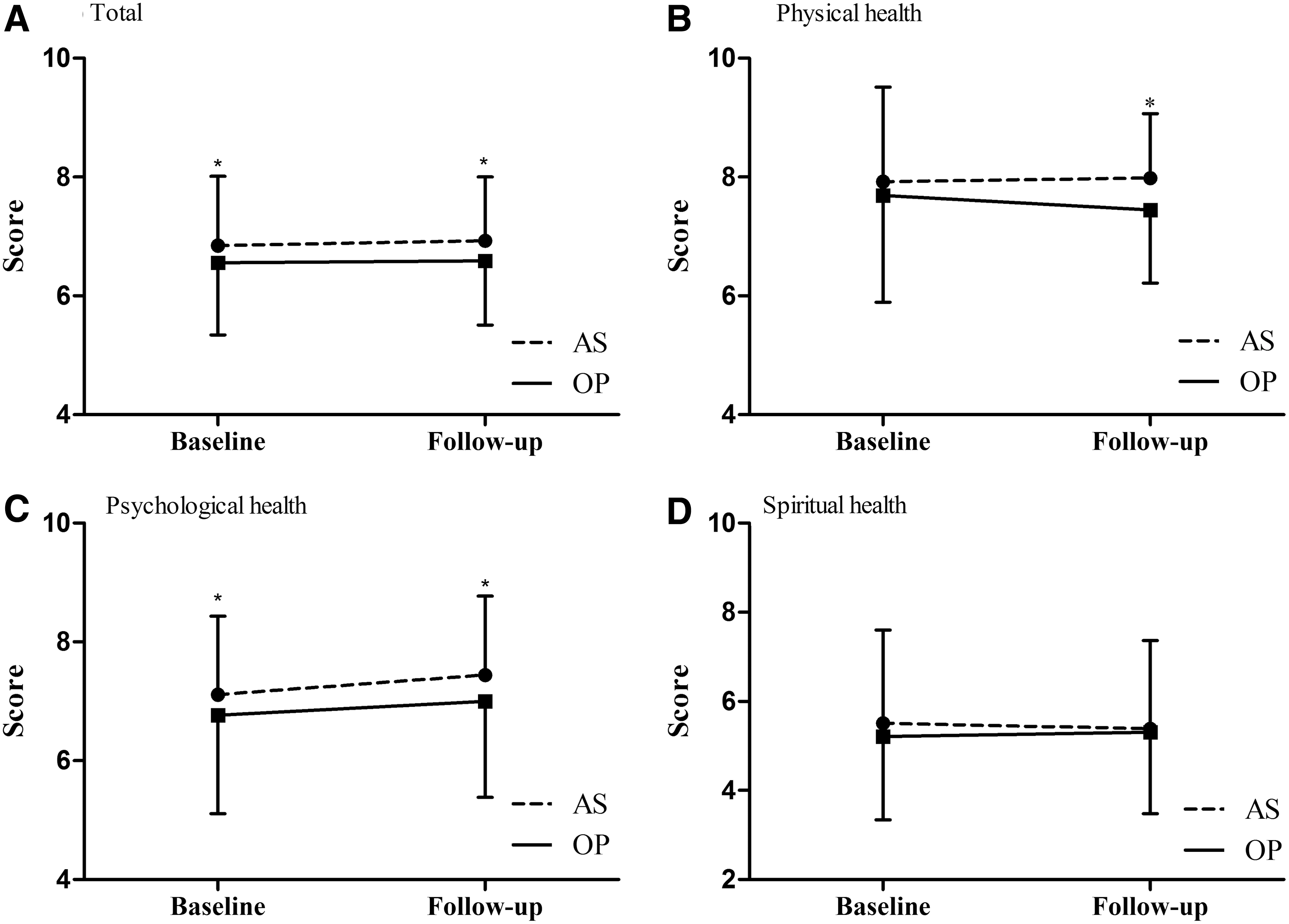
The mean ages of the participants in the AS and OP groups were 47.3 ± 11.7 and 45.6 ± 10.5 years (p = 0.138), respectively, and the mean tumor sizes were 5.7 ± 1.6 and 6.5 ± 2.1 mm (p = 0.065), respectively. At baseline, significantly better psychological health (7.1 ± 1.3 vs. 6.8 ± 1.6, p = 0.023) and overall health (6.8 ± 1.2 vs. 6.5 ± 1.3, p = 0.018) were observed in the AS group than in the OP group. During follow-up, significantly better physical (7.9 ± 1.1 vs. 7.4 ± 1.2, p < 0.001), psychological (7.4 ± 1.3 vs. 6.9 ± 1.6, p = 0.004), and overall health (6.9 ± 1.0 vs. 6.5 ± 1.1, p = 0.002) were observed in the AS group than in the OP group, whereas spiritual health was comparable between the two groups. Compared with the AS group, the OP group experienced more fatigue, changes in voice and appearance, less satisfaction, and low fear of recurrence. The self-assessed financial burden was similar at baseline and follow-up in both groups.
Conclusion:
The QoL of PTMC patients is different according to the type of treatment. Better psychological health at baseline and physical and psychological health at follow-up were observed in the AS group than in the OP group. However, studies with longer follow-up periods are needed.
Introduction
The incidence of thyroid cancer (TC), especially papillary thyroid microcarcinoma (PTMC), is on the rise (1,2). Since the recent introduction of the concept of active surveillance (AS) for management of PTMC, treatment options including AS are being considered (3,4). The concept of AS comprises thorough observation without surgery and intervention only in case of progression; this minimizes unnecessary surgeries and potential complications in the patient's quality of life (QoL) (5).
Recent studies support AS as a treatment option in PTMC patients. The Kuma Hospital group led by Miyauchi reported that during 10 years of observation of PTMC patients, 8% experienced an enlargement (>3 mm) of the lesion, 3.8% experienced lymph node metastases, and none had distant metastasis or disease-related mortality (6). Sugitani et al. at the Cancer Institute Hospital in Tokyo, Japan, reported that during 5 years of follow-up, 7% of patients experienced size enlargement, and none experienced extrathyroidal invasion or distant metastasis (7). Although medical costs vary among countries according to different insurance systems, AS was more cost-effective than surgery in Japan and the United States (8). Recent studies suggest that AS may be a treatment option for properly selected patients with low-risk PTMC.
QoL is one of the key considerations when deciding between AS and immediate surgery (OP) for PTMC. While some studies on prostate cancer, which pioneered the concept of AS, have reported that health-related QoL was comparable in patients who chose AS and OP (9 –11), others have concluded that AS resulted in worse QoL (12 –14). Patients choosing AS may experience fewer decrements in physical functions related to surgery, but end up with a poorer QoL due to anxiety regarding the future course of their disease, loneliness, and pressure from family members (12,13,15). However, research on QoL in PTMC is so far limited.
This study aimed at prospectively evaluating the QoL of low-risk PTMC patients opting for AS or OP at baseline and at follow-up. This study is a first step to (i) compare the effects of AS and OP on the QoL in PTMC patients and (ii) elucidating factors that affect choices related to treatment.
Materials and Methods
Study population
This study was part of the Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro), which is an ongoing study with continuing recruitment of participants. Diagnosis and enrollment criteria of the patients and the cohort protocol were described previously (16). Patients who were diagnosed with suspicion of papillary thyroid cancer (PTC) or as having PTC based on the results of fine needle aspiration (FNA) or core needle biopsy (CNB) were included. Patients with a maximal nodule diameter of >1 cm, suspected major organ involvement, lymph node/distant metastasis, poorly differentiated histology, or a variant with a poor prognosis were excluded. According to the Revised Korean Thyroid Association Management Guidelines in 2016 (17), thyroid nodules with high suspicious features and a diameter ≥5 mm are recommended to undergo FNA or CNB. However, FNA or CNB was occasionally performed for smaller lesions with suspicious features against the advice of physicians if patients desired to undergo the procedure.
A total of 732 patients with PTMC were enrolled in MAeSTro at 3 participating centers (Seoul National University Hospital [SNUH], Seoul National University Bundang Hospital [SNUBH, Seongnam city], and the National Cancer Center [NCC, Goyang city, Korea]) from June 2016 to March 2018. Among these, 687 patients agreed to complete the QoL questionnaire, and 395 patients who completed both baseline and follow-up questionnaires were included in the analyses of the present study. Clinical characteristics such as age; sex; maximal diameter of the tumor; and baseline serum thyrotropin (TSH), thyroglobulin (Tg), and anti-thyroglobulin antibody (TgAb) levels were similar between patients who were included in the analyses and those who were not. The median duration of the follow-up was 8.2 months.
The study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (1603-044-747), Seoul National University Bundang Hospital (B-1605-348-402), Seoul National University Boramae Medical Center (26-2017-18), and National Cancer Center (NCC2016-0183). Informed consent was obtained from all participants.
Assessment of QoL
To assess the thyroid-specific symptoms as well as the QoL in TC patients, a thyroid-specific QoL questionnaire was used, which was translated into Korean and validated (18 –20). Dow et al. (18) first reported the questionnaire in 1997, as a thyroid-specific QoL questionnaire that was developed to evaluate the impact of thyroid hormone on patients' perceived changes in QoL. Considering that TC patients often face unique QoL problems as compared with other types of cancer, assessing them by means of a disease-specific QoL questionnaire is important.
The questionnaire evaluates the physical, psychological, and spiritual dimensions, and scores the responses on a scale from 0 (worst) to 10 (best outcome). The QoL questionnaire consisted of 15, 30, and 7 items on the physical, psychological, and spiritual aspects, respectively. Overall health score is an average score of three dimensions. The responses to questions on QoL were obtained at the diagnosis before making a decision of AS or OP, and after 6–12 months of follow-up in both AS and OP groups (16). The interviews and questionnaires were administered by two trained clinical research coordinators.
Clinical data
Each participant had a comprehensive physical examination and was interviewed covering aspects of general health and the medical history as previously described (16). Anthropometric data were collected with the participants wearing light clothing without shoes or accessories. Height and weight were measured with the patient in an upright position using an electronic scale. Body mass index was calculated as weight (kg)/height2 (m2). Blood pressure and pulse rate were measured twice after five minutes of rest at the heart level in the seated position. Anthropometric data were obtained at diagnosis and at each follow-up to clarify the relationship between QoL scores and physical changes.
Laboratory data
Laboratory data were collected as previously reported (16). Serum TSH levels were measured at each visit using an immunoradiometric assay (DiaSorin SPA, Saluggia, Italy in SNUH; Cisbio International, Gif-sur-Yvette, France in SNUBH and NCC). Tg and TgAb levels were also measured using an immunoradiometric assay (RIA Tg-plus for Tg; anti-Tg for TgAb; BRAHMS GmbH, Hennigsdorf, Germany). The analytical sensitivity of the optimal curve was 0.08 ng/mL and 5.5 U/mL, and the functional assay sensitivity was 0.2 ng/mL and <20 U/mL for Tg and TgAb, respectively.
Statistical analysis
Categorical variables are presented as numbers and percentages, and continuous variables are expressed as the mean ± standard deviation for normal distribution, or medians with IQR for non-normal distribution. Pearson's chi-square test was used to compare categorical variables. Continuous variables were compared using Student's t test for normally distributed variables and the Mann–Whitney U test for non-normal distributions. Logistic regression analyses were used to assess the factors associated with the selection of AS over OP. Age and sex were adjusted in multivariate model. All p-values were two sided, and p < 0.05 was considered statistically significant and Benjamini–Hochberg correction (false discovery rate 0.05) was used in multiple statistical tests. All statistical analyses were performed using the SPSS software (version 22.0; IBM, IL).
Results
Clinical characteristics
Among the 395 participants who completed the QoL questionnaire at least 2 times, 192 patients (men: 49 [24.1%]) opted for AS while 203 (men: 36 [18.8%]) opted for OP. In the AS and OP groups, the mean ages (47.3 ± 11.7 and 45.6 ± 10.5 years, respectively) and tumor sizes (5.7 ± 1.6 and 6.5 ± 2.1 mm, respectively) were comparable (Table 1). Although patients who chose AS tended to have longer follow-up periods than those who underwent OP, there were no significant differences in TSH, Tg, and TgAb levels between the two groups at diagnosis.
Baseline Characteristics of Active Surveillance and Immediate Surgery Group
Continuous variables are expressed as mean ± standard deviation, or median [interquartile range], and categorical variables as numbers (percentages).
AS, active surveillance; BMI, body mass index; OP, immediate surgery; Tg, thyroglobulin; TgAb, anti-thyroglobulin antibody; TSH, thyrotropin.
In the AS group, there was a patient who changed from AS to OP because of disease progression with lymph node metastasis during the follow-up. In addition, four patients changed their decision from AS to OP because of other reasons, without disease progression. Three patients changed due to worry and anxiety for disease progression. One changed because she and her physician worried about a partly suspicious lymph node found during follow-up, which was, however, not definitive to confirm disease progression. The patient who had disease progression was a 28-year-old female with a tumor size of 7 mm; in this patient, lymph node metastasis was found at 17 months of follow-up. Four patients (two female, two male) who changed their mind during surveillance had a mean age of 50.3 ± 9.1 years, a mean tumor size of 6.1 ± 1.1 mm, and a follow-up duration of 10.8 ± 7.3 months before they underwent surgery. Patients were included in analyses as the AS group, and subgroup analyses were conducted to compare patients who continued AS and those who changed to OP without disease progression (Supplementary Table S1). Baseline and follow-up QoL scores were similar between the groups.
Among the OP group, 58 patients (30.2%) underwent total thyroidectomy, and 133 patients (69.3%) had a hemithyroidectomy. Central lymph node dissection was performed in 171 patients (89.1%), and a modified radial neck dissection was additionally performed in 4 patients (2.1%). Postoperative hypoparathyroidism and voice change occurred in 31 (16.2%) and 16 (8.3%) patients, respectively. Moreover, three patients (1.6%) experienced postoperative hematomas at the surgical site. There has been no evidence of recurrent disease after surgery until now.
Thyroid hormone replacement therapy at baseline was administered in only a small number of patients in both groups (four in the AS group, one in the OP group, p = 0.380). The median thyroxine (T4) dose of both groups was similar (50 μg daily, p = 0.179) and was maintained throughout the follow-up period. Thyroid hormone replacement therapy at follow-up was administered in 17 patients in the AS group and 118 patients in the OP group (80 μg daily in the AS group, 93 μg daily in the OP group, p = 0.230). Expectedly, the OP group required a significantly higher dose of T4 than the AS group at follow-up (0 μg in the AS group, 50 μg daily in the OP group, p < 0.01).
QoL at baseline and follow-up
At baseline, patients who chose AS had better psychological and overall health, particularly in terms of anxiety related to diagnosis, and feelings of isolation (Table 2 and Fig. 1). They considered themselves as more active in household chores, preparing meals, and leisure activities than patients who chose OP. However, depression, anxiety related to future tests, recurrences, metastases, and subjective impression of financial burden were not different between the groups. Also, there was no significant difference in the physical and spiritual health of participants in the groups.
QoL score changes in the AS and OP groups in (
Quality of Life Score Assessed by Questionnaire at Baseline and Follow-Up
QoL scores are ranged 0 to 10, and high score represents positive state. Student t test was done between AS and OP groups at baseline and follow-up. Continuous variables are expressed as mean ± standard deviation, or median [interquartile range]. Menstrual changes were evaluated only in women. Benjamini–Hochberg correction was done in each category—physical (15 items), psychological (30 items), and spiritual (7 items). Average scores were not corrected.
p-Value significant after Benjamini–Hochberg correction.
QoL, quality of life.
After a mean follow-up of 8.2 ± 4.6 months, patients who underwent AS experienced better physical health than those who chose OP, especially in aspects of fatigue, appetite change, aches or pain, voice changes, neck discomfort, and difficulties in swallowing. As for the psychological health, the responses indicated that patients in the AS group were healthier than those in the OP group in terms of their overall QoL, ability to cope with the disease, change in appearance and self-concept (the way participants see themselves), work efficiency, productivity, work quality, feelings of isolation, ability to drive, perform household chores, and leisure activities. However, fear of recurrence, metastasis, and the subjective impression of financial burden were similar in both groups. In the area of spiritual health, the average scores of the two groups were comparable, although patients in the AS group had more positive thinking than those in the OP group (Fig. 1B).
The percentage changes in the QoL scores during the follow-up were also evaluated (Supplementary Table S2). The percentage changes in QoL with respect to physical health showed a more severe deterioration in the OP group than in the AS group. In the area of psychological health, percentage change of QoL scores in the OP group worsened only in terms of memory and diagnosis-related anxiety. However, percentage change of QoL scores in other aspects of psychological health, such as coping with the disease, changes in appearance, self-concept, work efficiency, productivity, work quality, feelings of isolation, and daily activities was not different between the groups. The percentage change of QoL related to spiritual and overall health remained comparable between the groups.
Factors associated with the selection of AS over OP
To investigate the factors associated with treatment choices, a logistic regression analysis of the baseline characteristics was performed. Univariate analysis found that patients with a longer follow-up, better psychological and overall QoL, especially in terms of diagnosis-related anxiety, feelings of isolation, and an active life-style including performing household chores, preparing meals, and leisure activities tended to select AS over OP for treatment. A multivariate analysis found that diagnosis-related anxiety, feelings of isolation, and active lifestyle that included performing household chores, preparing meals, and leisure activities remained significant after adjusting for age and sex (Table 3).
Odds Ratios for Selection of Active Surveillance over Immediate Surgery
QoL scores are ranged from 0 to 10, and high score represents excellent, low score represents poor state. Logistic regression analysis was done for selection of AS, selection of OP as a reference. Age and sex were adjusted in multivariate model.
Discussion
In this multicenter prospective study with PTMC patients, those who chose AS over OP as a treatment option showed better baseline psychological health, while baseline physical and spiritual health scores were comparable between the two groups. After a mean follow-up period of 8 months, patients who chose AS showed better physical and psychological health than those in the OP group, especially with regard to the postoperative QoL. Fatigue, aches and pain, voice changes, discomfort in neck/swallowing, changes in appearance, and self-concept, which were comparable at baseline, became worse in the OP group at the follow-up visits. A recent cross-sectional QoL study by Jeon et al. also reported that patients with PTMC who underwent lobectomy experienced more health-related problems than those managed by AS (21). These findings add clinical evidence in terms of QoL on the previous studies showing the role of AS as a reasonable management option for patients with PTMC (6,7). But the deteriorated physical health in the OP group may be due to the short follow-up period (7 months), during which the patients were still experiencing the postoperative sequelae. In prostate cancer, the major reason for adapting the concept of AS was the significant deterioration in physical QoL caused by postsurgical events such as urinary and sexual dysfunction (22). However, thyroidectomy for PTMC is a less invasive surgery, and its impact on physical QoL is relatively small (23). Long-term prospective studies are needed to ensure that the patients recover from surgery and to assess whether their QoL is restored.
Psychological health was also better in the AS group than in the OP group. These parameters showed better results in the AS group both at baseline and at follow-up. Participants who felt less isolated and thought of themselves as more active tended to choose AS, and this difference in trend between the two groups remained unchanged during follow-up. Moreover, patients in the AS group felt less anxious about the diagnosis than those in the OP group, at baseline. Since the baseline QoL questionnaire was evaluated before the decision between AS and OP, this trend was evaluated again as odds ratios of selecting AS in the study, which showed that patients who (i) participated more actively in household chores and leisure activities, (ii) felt less isolated, and (iii) were less stressed about the diagnosis were more likely to choose AS over OP. These findings suggest that the baseline QoL status has some impact on the choice of the treatment modality. Similar trends were observed in patients with prostate cancer who chose AS. They had higher psychological health scores than the general population at baseline and follow-up, suggesting that men with better psychological health chose AS (24). It implicates that patient personality and psychological characteristics should be taken into account during the counseling process in choosing treatment options (25), since these traits impact their ability to cope with the psychological burden in the long term (26). In prostate cancer patients, it has been reported that the awareness of cancer and the uncertainty associated with it become intolerable for some patients, leading them to opt for OP to avoid stress and anxiety (27). Also, patients on AS who had a less neurotic personality and good physical health were often found to have a good psychological status during follow-up (28). Therefore, as each patient's situation is different, it is important for the physicians to communicate in depth with them to thoroughly assess their physical and psychological status at baseline before suggesting any treatment options.
In this study, anxiety related to diagnosis and the fear of recurrence/metastasis were comparable between the two groups at follow-up. The fear of disease progression particularly related to the fear of second cancer, recurrence, and metastasis was similar at diagnosis and follow-up. This suggests that patients who chose AS did not experience a greater fear of progression than patients in the OP group, which was one of the main concerns during the follow-up of patients in the AS group. Contrary to some studies in prostate cancer, which have suggested that patients undergoing AS experience greater fear of progression (12,13), most recent studies have reported that these patients do not experience increased anxiety or depression related to cancer progression (9 –11). Our results show that fear of cancer progression did not have a major influence during AS in PTMC patients, but this could have been due to the short follow-up duration.
The concern regarding the subjective impressions of financial burden was comparable between the groups at initial diagnosis and follow-up. This could be due to the fact that both surgery and ultrasonography are not very expensive in Korea, and, therefore, cost was not a major concern when selecting treatment options. In Korea, total thyroidectomy and thyroid sonography cost ∼5 million won (∼4599 US$) and 183,000 won (∼160 US$). While the national insurance program covers the majority of the expenses, patients pay ∼1.2–1.4 million won (∼1300 US$) for total thyroidectomy and 73,000 won (∼65 US$) for thyroid sonography. In Japan, in contrast, the total cost of OP is about four times higher than that of AS (8), while the cost for sonography is lower (∼30 US$). In the United States, an analysis of the cost-effectiveness showed that hemithyroidectomy could be more cost-effective than AS in patients with modest decrements in QoL (29). Therefore, the impact of cost on treatment choices should be considered individually for each country based on the different medical insurance structures.
The study has several strengths. First of all, this is the first prospective study to compare QoL in the AS and OP groups in parallel, which can help in identifying factors that influence the selection of treatment options. Second, being a multicenter study, it includes rural and urban areas, as well as secondary and tertiary hospitals. We believe the results are more reliable because they are less likely to be skewed by a single institution or the preferences of physicians. Third, the study had a unified protocol for AS and OP and followed the patients according to a previously published protocol (16), which is likely to have reduced information and confounding biases. Fourth, the QoL scores were evaluated using the thyroid QoL (18 –20), which was specifically developed for TC patients. Finally, there were a sufficient number of patients in both groups to make valid comparisons.
The study also has some limitations. The follow-up duration for the OP group was shorter than that for the AS group, which could influence their responses on QoL. Also, the duration might not have been sufficiently long to see differences in aspects of psychological and spiritual health. Studies with longer follow-up durations would be needed to see the long-term effects on the QoL in these patients. The results could also potentially be influenced by self-selection bias because the patients were not randomized due to ethical issues.
In conclusion, PTMC patients who chose AS had better physical and psychological QoL than those who had surgery during 8 months of follow-up period. These findings support the role of AS as a reasonable management option for patients with PTMC, although QoL deterioration in the OP group was mainly caused by postoperative changes and studies with longer follow-up periods are needed. Also, it would be important to give patients detailed and precise information about their treatment options, since accepting the disease at the time of diagnosis could influence their decision-making.
Footnotes
Acknowledgments
This study was supported by Seoul National University Hospital (research grant 25-2016-0010) and National Cancer Center (research grant 1810151-1).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2