
Abstract
Background:
Untreated overt hypo- and hyperthyroidism can lead to detrimental effects on muscle tissue and physical performance, but it is still unclear whether subclinical hypo- or hyperthyroidism has clinically relevant effects on muscle function and physical performance. The objective of this study was to determine associations of thyrotropin (TSH) with grip strength and physical performance.
Methods:
A sample of 6196 participants from the Study of Health in Pomerania and the Berlin Aging Study II was included in this cross-sectional analysis. Handgrip strength was measured with a hand-held dynamometer and physical performance was assessed with the timed up and go (TUG) test.
Results:
Serum TSH levels were significantly inversely associated with handgrip strength (β −0.11; [95% confidence interval, CI, −0.18 to −0.03]; p < 0.05) in multivariable linear regression. Individuals with high (β −1.06; [95% CI −1.86 to −0.26]; p < 0.05) or low (β −0.99; [95% CI −1.70 to −0.28]; p < 0.05) serum TSH levels had a significantly lower handgrip strength than individuals with serum TSH levels within the reference range. There was no association between TSH and the TUG time. Age showed a significant influence on the association of TSH with grip strength and TUG time.
Conclusions:
Even mild disturbances of thyroid function might lead to a relevant decline in grip strength, particularly in young and middle-aged subjects. Mild subclinical hypothyroidism might not be that unfavorable with regard to physical function in terms of handgrip strength at older age. Further studies are needed to clarify causal relationships.
Introduction
Thyroid hormones regulate important metabolic processes and, thus, thyroid dysfunction can lead to clinically relevant alterations in energy expenditure, body weight regulation, glucose metabolism, and lipid metabolism (1). The skeletal muscle is a major target of thyroid hormone signaling that is essential in regulating metabolic and contractile properties of muscle fibers. The binding of triiodothyronine to the thyroid hormone nuclear receptors in skeletal muscle is necessary for normal muscle development, homeostasis, and regeneration (2). Clinically, both hypothyroidism and hyperthyroidism can lead to a wide range of muscular symptoms such as muscle pain and muscle weakness up to severe effects including myopathy and muscle breakdown (3).
It is still under debate whether subclinical hypo- or hyperthyroidism leads to clinically relevant detrimental effects on muscle function and physical performance. In older people, subclinical hypothyroidism might even be advantageous toward better physical function, whereas subclinical hyperthyroidism was shown to be associated with poor physical performance (4 –6). Another study, however, has not reported such a difference (7). Sample sizes of some of the available studies on this topic have been small (6,7) or have been focused on much older populations (5,8), whereas the cohort of this study is covering an age range of 20–84 years.
In any case, an intact muscle function is essential to maintain independent performance of basic activities of daily living such as walking, bathing, dressing, climbing stairs, and general well functioning. This is especially important in an aging population wherein the age-associated loss of muscle mass and strength itself, sarcopenia, are increasingly recognized as an independent risk factor for frailty and disability (9,10). Against this background, the goal of this study was to investigate the association of thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) with muscle strength and physical function in a large combined cohort of two cross-sectional epidemiologic studies. A further goal was to examine the potential impact of age on the association of thyroid function with the parameters of muscle strength and physical function. Muscle strength was defined by grip strength and physical function by a timed up and go (TUG) test.
Materials and Methods
Study population
Altogether, 6196 participants from the Study of Health in Pomerania (SHIP) and the Berlin Aging Study II (BASE-II) were included in this cross-sectional analysis.
SHIP-TREND-0 is a population-based study conducted in the northeast of Germany between 2008 and 2012 (11). For SHIP-TREND-0, a random, age- and sex-stratified sample of 8826 eligible subjects was drawn from the population registry of which 4420 subjects aged 20–80 years participated (net response 50.1%). All participants gave informed written consent. SHIP-TREND-0 followed the recommendations of the Declaration of Helsinki and was approved by the ethics committee of the University of Greifswald. For the present analysis, we excluded 265 individuals due to missing data in any of the considered variables.
The BASE-II cohort was drawn as a convenience sample from the greater Berlin metropolitan area. Two thousand one hundred seventy-two participants (∼75% aged 60–84 years and ∼25% aged 20–35 years) were recruited for the medical part of the study (12). BASE-II is a prospective epidemiological study to investigate factors associated with “healthy” or “unhealthy” aging, which has been described previously in detail (13,14). The participants were recruited as a convenience sample in the residents of the greater metropolitan area of Berlin, Germany. All participants gave written informed consent and the BASE-II was approved by the ethics committee of the Charité—Universitätsmedizin Berlin (approval no. EA2/029/09) and registered with the clinical trial registry Deutsches Register Klinischer Studien (DRKS00009277). For this analysis, we excluded 69 individuals due to missing data in any of the considered variables.
Assessments
In BASE-II, information on smoking status was taken from the medical history recorded by a study physician. In SHIP, smoking status was assessed in a computer-assisted interview. Smoking status was categorized into three: current smokers, former smokers, and never smokers. Physical activity was assessed by interview and a questionnaire, and is reflected by a dichotomous variable discriminating between regularly physical active or not. Information on diabetes mellitus was taken from the medical history or by increased levels of glucose (≥11.1 mmol/L) or HbA1c (≥6.5%). Blood samples were taken as fasting blood samples and analyzed in a central certified laboratory using standardized protocols. Serum TSH, fT3, and fT4 levels were analyzed by electrochemiluminescence immunoassays (BASE-II: Cobas immunoassay systems; Roche diagnostics, Mannheim, Germany; SHIP-TREND-0: Dimension Vista® System Flex® reagent cartridge; Siemens Healthcare Diagnostics, Inc., Newark, DE). The analytical measuring range was 0.005–100 mIU/mL, 0.1–8.0 ng/dL, and 0.50–30.00 pg/mL for TSH, fT4, and fT3, respectively. TSH levels were categorized into three: TSH in the reference range, high TSH, and low TSH according to the established reference limits of 0.27 to 4.20 mU/L in BASE-II and 0.49 to 3.29 mIU/L in SHIP-TREND-0 (15). Subclinical hypothyroidism and subclinical hyperthyroidism were defined as TSH above, respectively, below the reference range with free thyroid hormones being in the reference range. Overt hypothyroidism was defined as TSH above the reference range combined with fT3 and fT4 below the reference range and overt hyperthyroidism was defined as TSH below the reference range combined with fT3 and fT4 above the reference range.
In both studies, body weight was measured in light clothes with a portable electronic scale to the nearest 0.1 kg and height was determined to the nearest 0.1 cm by using an electronic weighing and measuring station (seca 764, seca, Hamburg, Germany). Weight and height were used for calculating the body mass index (BMI) (weight [kg]/height2 [m]).
Muscle strength
Muscle strength was assessed by measuring handgrip strength. In BASE-II, handgrip strength was measured with a Smedley Dynamometer (Scandidact, Denmark). The subjects were instructed to perform a maximal isometric contraction and the test was performed three times for each hand and the highest value was chosen. In SHIP the same device was used, but the test was performed only once for each hand. Handgrip strength was measured in kilograms. The maximum handgrip strength was used in the regression models in the statistical analyses.
Physical performance
In both studies, SHIP and BASE-II, physical performance was assessed by using the TUG test (16). The time in seconds taken to stand up from a chair, walk a distance of 3 m, turn, walk back to the chair, and sit down again was measured for the participants (TUG time).
Statistical analyses
Characteristics of the study population are provided stratified by study site as median 25th and 75th percentile for continuous variables or as absolute numbers and percentages for categorical variables. In the pooled population of the BASE-II study and SHIP-TREND study associations of thyroid biomarkers with handgrip and TUG test was analyzed by linear regression models adjusted for age, sex, BMI, smoking status, and study site. Interactions of serum TSH levels with age were tested in these regression models. A p < 0.05 was considered as statistically significant. All analyses were carried out using Stata14.2 (Stata Corporation, College Station, TX).
Results
The median age of the 6196 participants was 59 years with a roughly balanced sex ratio of 3004 men to 3192 women. The BASE-II participants were older than the SHIP participants with a median age of 67 years compared with 53 years. BASE-II-participants also had a lower BMI and lower grip strength than SHIP. Furthermore, in SHIP, more individuals had type 2 diabetes mellitus than in BASE-II (12.4% vs. 7.9%). The median TUG time was lower in BASE-II participants than in SHIP participants. While the vast majority of the participants were euthyroid, ∼9% displayed subclinical hypo- or hyperthyroidism and ∼2% overt hypo- or hyperthyroidism. The median maximum grip strength was 35.0 kg and median TUG time 8.1 seconds. The characteristics of the study population are given in Table 1.
Characteristics of the Study Population
BASE-II, Berlin Aging Study II; fT3, free triiodothyronine; fT4, free thyroxine; SHIP, Study of Health in Pomerania; TSH, thyrotropin; TUG, timed up and go.
Association of thyroid biomarkers with handgrip strength
In the pooled population of BASE-II and SHIP-TREND, serum TSH levels over the full range were significantly inversely associated with handgrip strength in multivariable linear regression (Table 2). The association of TSH levels as a continuous variable with mean handgrip strength is shown in Figure 1. This association was also seen when restricting the analysis only to individuals with TSH levels in the reference range. Concretely, per one unit rise of TSH, a decline of 0.11 kg grip strength was observed. However, individuals with high or low serum TSH levels had a significantly lower handgrip strength than individuals with serum TSH levels within the reference range (mean grip strength 35.7 ± 0.35 and 35.6 ± 0.40 kg for low and high TSH, respectively, vs. 36.7 ± 0.91 kg for TSH in the reference range). Serum fT4 levels were inversely associated with grip strength, while there was no association between serum fT3 levels and grip strength (Table 2).

The association of serum TSH levels with mean handgrip strength. TSH, thyrotropin.
Association of Thyroid Biomarkers with Handgrip and Timed Up and Go
Linear regression adjusted for age, sex, body mass index, smoking status, and study.
In comparison with TSH in the reference range.
p < 0.05
CI, confidence interval.
Age was a significant modifying factor for the association between TSH and grip strength (p for interaction 0.007). As shown in Figure 2, TSH was significantly inversely associated with grip strength in younger participants up to an age of ∼60 years but not in older adults.

Effect modification of age on the association of TSH with grip strength.
Association of thyroid biomarkers with TUG test
Serum TSH levels, whether in the full range or in the reference range, were not significantly associated with TUG time in the entire cohort. The TUG time did not differ significantly between individuals with low or high serum TSH levels in comparison with individuals with serum TSH levels within the reference range. Whereas fT3 levels were inversely associated with TUG time, no significant association was found between serum fT4 levels and TUG time.
Age showed a significant influence on the association for TSH with TUG time (p for interaction 0.003). TSH was significantly positively associated with TUG time in younger participants, while in older participants the association was inverse (Fig. 3).
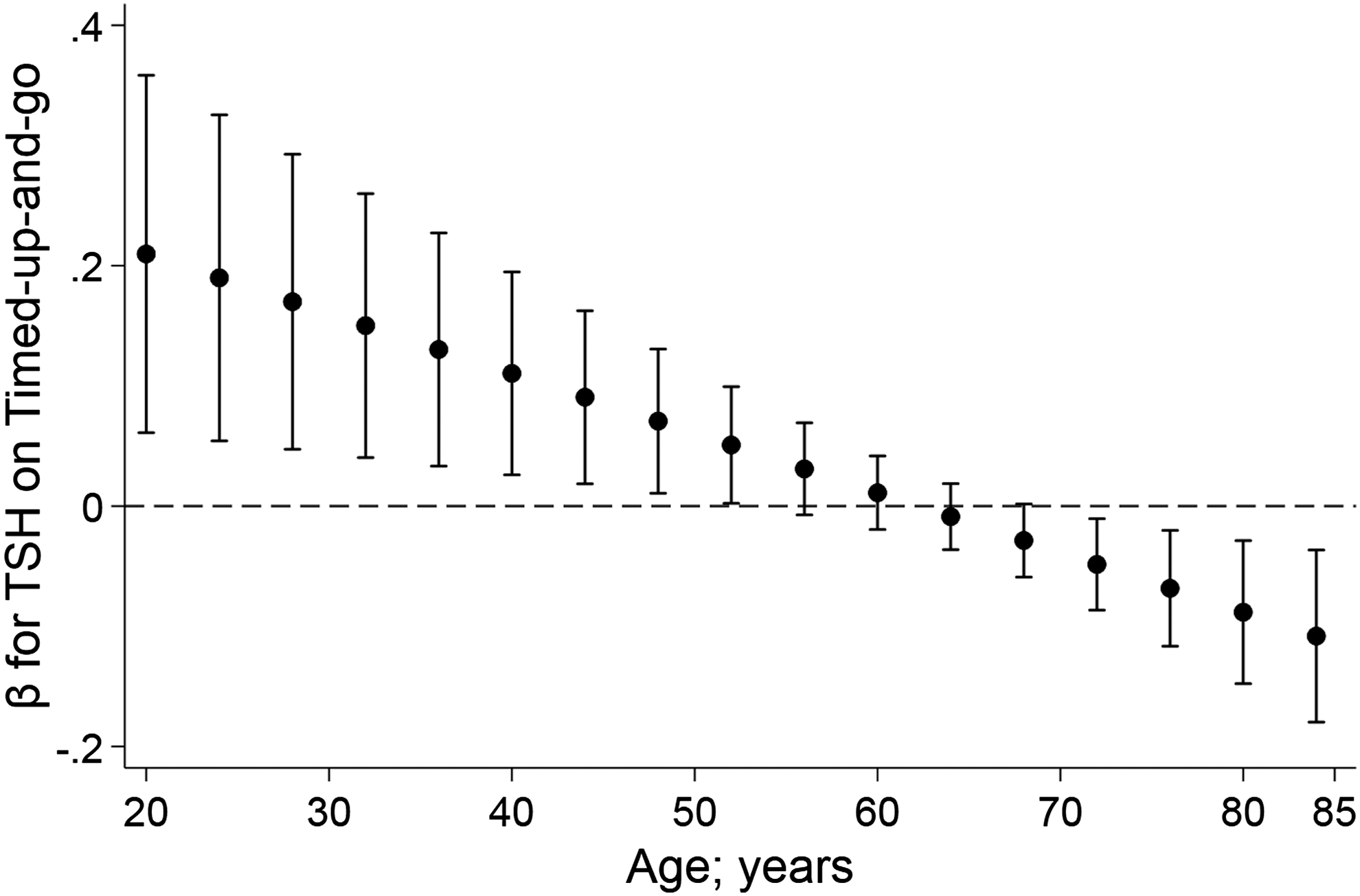
Effect modification of age on the association of TSH with TUG time. TUG, timed up and go.
The association of age with handgrip strength and TUG is shown in Figures 4 and 5.

Boxplots showing the distribution of grip strength stratified by age and study site.

Boxplots showing the distribution of TUG time stratified by age and study site.
Discussion
In data from two cross-sectional epidemiologic studies from Germany, we detected consistent associations of thyroid function assessed by serum levels of TSH levels with grip strength. While grip strength decreased over the TSH reference range, individuals with TSH values below or above the reference range had a significantly lower grip strength than individuals with serum TSH levels within the reference range, suggesting potential adverse effects of hypo- and hyperthyroidism on grip strength. Interestingly, while there was an inverse association of fT4 with grip strength, fT3 was not significantly associated with grip strength. Only fT3 but not TSH and fT4 was significantly associated with TUG time. Age significantly modified the associations of TSH with grip strength and TUG time.
Median values of grip strength (35.0 kg) and TUG time (8.1 seconds) of the study participants in our study were comparable with age-stratified values provided by other studies (17,18). To provide a clinical context, especially with regard to the observed effect modification by age, grip strength and physical performance of the majority of the study participants were also better than what could be expected in functionally impaired sarcopenic subjects for whom a grip strength <27 and 16 kg for men and women, respectively, and a TUG time >20 seconds are considered as cutoff values (19).
Thyroid function and muscle strength
There are some previous studies that have investigated possible associations between thyroid function and grip strength or, on a broader level, muscle strength in general (5 –7,20). It was already shown that hyperthyroidism may be associated with myopathy, which is responsive to treatment of hyperthyroidism, resulting in improved functional tests of hand and shoulder strength (21). Hypothyroid patients can be afflicted with neuromuscular complaints and clinical weakness as well (3). Erkol Inal et al., in contrast, found no significant differences between the handgrip strength of 51 subjects with primary hyperthyroidism compared with a group of 44 healthy controls (7). Van den Beld et al. examined 403 independently and ambulatory living older men aged 73 to 94 years and found that, independent of age and diseases such as hypertension, atherosclerotic diseases, congestive heart failure, chronic obstructive pulmonary disease, diabetes and arthrosis, high serum fT4 concentrations within the reference range were related to lower isometric grip strength (6). This is comparable with our results concerning fT4 and grip strength. Cross-sectional associations of subclinical thyroid disorders with physical and cognitive function were examined in 1219 participants of the Longitudinal Study of Amsterdam, also including the assessment of handgrip strength. There was a trend for lower mean handgrip strength in individuals with subclinical hyperthyroidism compared with euthyroid participants, but this difference did not reach statistical significance (p = 0.08) (20).
The comparison of the majority of the mentioned studies with our study is hampered since they focused either on much more severe cases of thyroid dysfunction or had lower sample sizes or studied older populations (3,5 –8,21). Irrespective of this, it is noncontroversial that thyroid hormones play an important role in maintaining an intact muscle metabolism and muscle function (22). Our data suggest that also nonsevere states of thyroid dysfunction, whether hypo- or hyperthyroid, and also subtle changes in thyroid function, possibly even occurring within the reference range of TSH, can lead to a decline in muscle function measured by grip strength. Although a decline of 0.11 kg grip strength per 1 mU/L increase of TSH might not seem much at first, this effect might well become more pronounced in case of prolonged states of untreated thyroid dysfunction.
Grip strength has not only been proven as a strong predictor of mortality (23) but it is also considered as a biomarker of aging and indicator of underlying aging processes (24). Moreover, grip strength is an essential diagnostic criterion of sarcopenia, the age-associated decline of muscle mass and function (25). This is especially important to consider in an aging population. Thyroid dysfunction is usually well treatable and has to be considered as a potential secondary and reversible cause of sarcopenia. However, our data suggest that hypothyroidism particularly affects grip strength in young to middle-aged individuals but not in older adults. Our results, therefore, encourage further preferentially longitudinal investigations into the relationship between thyroid function and grip strength.
Thyroid function and physical performance
To the best of our knowledge, no previous study associated thyroid biomarkers with physical performance exactly measured by the TUG test. Nonetheless, comparable markers of physical performance like walking speed were used by some studies. In the Health, Aging and Body Composition study, subjects with mild subclinical hypothyroidism showed higher walking speed than subjects in the euthyroid group. While a group of subjects with TSH levels between 6.45 and 7.45 mU/L showed the highest walking speed, TSH levels higher than this showed no association with a further increase in gait speed (4). Comparable with our study, Simonsick et al. found no association between TSH and gait speed in a sample of 602 older men and women aged 70–79 years. However, increasing fT4 levels were associated with worse reported walking ability as well as slower usual and rapid gait speed (8). In the study by de Jongh et al., participants with subclinical hypothyroidism did less frequently report more than one activity limitation than euthyroid subjects (20). Findings like these led to the argument that mildly downregulated thyroid function might be favorable for better function with aging and could be a sign of positive adaptation reflecting healthy aging. With regard to the inverse association of TSH with TUG time occurring in subjects beginning with an age of ∼70 years, our data support these results. Data of the InChianti study are also pointing in a similar direction as men with subclinical hyperthyroidism showed a poorer lower extremity function (assessed by the Summary Physical Performance Battery also including the 4-meter walking speed test) than healthy subjects (5). The association of an increase in fT3 levels with a lower TUG time could be interpreted as a positive effect of thyroid hormones on mobility but might also be only a short-term effect that in the long run might turn to the opposite in case of untreated hyperthyroidism. Moreover, it has to be considered that the ability to stand up and walk is determined by numerous determinants and other factors such as neuromuscular coordination, joint function or sensory perception might be far more decisive than thyroid function.
One of the limitations of our study is that not all of the many factors that potentially influence grip strength and physical performance could have been included in our analyses. The two study groups also have different age profiles and different profiles of morbidity (e.g., a higher prevalence of diabetes in SHIP), which potentially impacts muscle function and physical performance through different pathways. Moreover, although formally the same assessments, TUG and handgrip strength, were used in both studies, we cannot preclude subtle differences in the execution of these tests that might relate to the study site. For example, it is difficult to explain why the BASE-II participants, on average older than the SHIP participants, had a better TUG performance. Furthermore, TUG is part of the geriatric assessment and formally not intended to be used with younger cohorts, and thus our results have to be interpreted with caution. Another methodological limitation is the use of different laboratory assays in the measurement of TSH, fT3, and fT4. Although both were electrochemiluminescence immunoassays used in accredited laboratories, we cannot preclude a potential impact on the results. The strength of this study lies in its large sample size and the combination of two different cohorts spanning a large age range that is important since thyroid disease can occur all over the lifespan.
In summary, we found an association between thyroid function reflected by TSH levels and grip strength. Both, TSH levels below and above the reference range were associated with a lower handgrip strength, but a significant association was not observed in older participants. This is noteworthy since our data suggest that with increasing age mild hypothyroidism might gradually lose its clinical significance with regard to muscle function and physical performance. In older age, many other factors such as neurodegenerative diseases, nutritional deficiency, or polypharmacy, among others, might have an additional and even more substantial impact on muscle strength and physical functioning than mild thyroid dysfunction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Berlin Aging Study II was supported by the German Federal Ministry of Education and Research under Grant No. 16SV5536K. The Study of Health in Pomerania is part of the Community Medicine Research net of the University Medicine Greifswald, which is supported by the German Federal State of Mecklenburg-West Pomerania.