
Abstract
Background:
Inactivation of DNA mismatch repair (MMR) and the resulting microsatellite instability (MSI) are frequently observed in endometrial, stomach, and colorectal cancers, as well as more rarely in other solid tumor types. The prevalence of MSI in thyroid cancer has not been explored in depth, although recent studies utilizing data from large cancer sequencing efforts such as The Cancer Genome Atlas indicate that MSI is absent or at least very rare in the most common and most well studied histologic subtype, papillary thyroid carcinoma. This study aimed to determine the prevalence of MSI in thyroid cancer by using a large series comprising all major histological subtypes.
Methods:
A total of 485 thyroid cancer patients were screened for MSI/MMR deficiency, including all major histologic subtypes (195 papillary thyroid carcinoma, 156 follicular thyroid carcinoma [FTC], 50 anaplastic thyroid carcinoma, 65 medullary thyroid carcinoma, and 17 poorly differentiated thyroid carcinomas) by using a combination of polymerase chain reaction–based detection, immunohistochemistry, and next-generation sequencing.
Results:
A total of four tumors were MSI-high and had loss of MMR protein expression, all of which were from FTC patients. Whole-exome sequencing was performed on two MSI-high FTCs and revealed a hemizygous loss of function mutation in MSH2 in one tumor.
Conclusions:
Based on these data, it is estimated that the overall prevalence of MSI in FTC is 2.5%, and MSI is either entirely absent or rare in other histology subtypes of thyroid carcinoma. These findings highlight the importance of testing for MSI in FTC.
Introduction
Thyroid cancer is the eighth most common malignancy in the United States, with an estimated 53,990 new cases in 2018 (1). Carcinomas arising from the follicular cells of the thyroid are the most common and include papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC), which account for approximately 70–80% and 10–15% of cases, respectively. Less common histologic subtypes include medullary thyroid cancer (MTC), which makes up 5–10% of cases and develops from parafollicular cells, anaplastic thyroid cancer (ATC), a rare and more aggressive undifferentiated subtype present in approximately 1% of cases, and poorly differentiated thyroid cancer (PDTC), which is also rare but distinct from ATC (2).
Microsatellite instability (MSI) is an accumulation of insertion or deletion mutations in repetitive DNA sequences due to underlying defects in DNA mismatch repair (MMR) (3). Tumors with MSI have a greatly increased overall mutational burden in addition to changes in microsatellite lengths (4). Importantly, due to this increased mutation load, dynamic mutational profiles, and continued renewal of tumor neoantigens, tumors that show MSI tumors respond well to anti programmed death-ligand 1 (PD-L1) immunotherapy, which has substantially improved patient outcomes in several cancers (5 –8).
Defining MSI status by utilizing polymerase chain reaction (PCR) and capillary electrophoresis was standardized in 1997 with the Bethesda panel of five selected microsatellites: the mononucleotide repeats BAT25 and BAT26, and the dinucleotide repeats D17S250, D2S123, and D5S346 (9). Tumors must show instability in at least two of the five markers to be classified as MSI-high (MSI-H), whereas those that show instability for a single locus are considered MSI-low, and those with no instability are microsatellite stable (MSS) (10). More recently, it has become more common to detect MSI using next-generation sequencing (NGS) approaches (11). Several informatics tools are available to detect MSI status using targeted, whole-exome, and whole-genome sequencing data, including the authors' own MonoSeq variant caller and MANTIS tool (12,13). MSI status can also be inferred through immunohistochemistry (IHC)-mediated detection of expression of the MMR proteins MLH1, PMS2, MSH2, and MSH6 because MSI is caused by underlying defects in DNA MMR. Paired loss of expression of either MLH1 and PMS2 or MSH2 and MSH6 is typically observed in MSI-H tumors (4).
While MSI is widely reported in colorectal, endometrial, and stomach cancers, the prevalence of MSI in thyroid cancer appears to be low, but a large detailed study is missing (14,15). Previous investigations of MSI in thyroid cancer have almost exclusively been performed on PTC cases, neglecting less common histologic subtypes, and have reported disparate and conflicting results (Table 1). In this study, a comprehensive effort was undertaken to assess the prevalence of MSI in a large series of malignant thyroid tumors comprising all major histologic subtypes.
Summary of Published Investigations of Microsatellite Instability in Thyroid Cancer
Study did not distinguish between MSI-H and MSI-L.
Histology not specified.
ATC, anaplastic thyroid carcinoma; CE, capillary electrophoresis; DTC, differentiated thyroid carcinoma; FTA, follicular thyroid adenoma; FTC, follicular thyroid carcinoma; IHC, immunohistochemistry; MSI-H, microsatellite instability high; MSI-L, microsatellite instability low; MTC, medullary thyroid carcinoma; PAGE, polyacrylamide gel electrophoresis; PCR, polymerase chain reaction; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma.
Methods
Patients
An initial sample set of 301 patients were recruited from a multidisciplinary thyroid tumor clinic at The Ohio State University Wexner Medical Center (OSUWMC), and all cases were histologically confirmed as either PTC, FTC, MTC, or ATC. All patients provided written informed consent, completed a questionnaire that included demographic, medical, and family history information, and donated a blood sample. Relevant clinicopathologic data for cases were extracted from the electronic medical records. All patients provided written informed consent, and the experimental protocols were approved by the Institutional Review Board at The Ohio State University. These samples were assessed for MSI using PCR-based detection and IHC of a tissue microarray (TMA).
A validation set of 188 tumor samples from 184 advanced thyroid carcinoma patients, defined as progressive recurrent and/or with distant metastases, were analyzed by targeted NGS at M.D. Anderson Cancer Center as part of patient care for planning additional therapies. Tumors with matched normal tissue or paired blood were analyzed, allowing for germline sequence variants to be excluded in the analysis. All patients provided written informed consent, and the experimental protocols and data sharing were approved by the Institutional Review Board at M.D. Anderson Cancer Center. These samples were assessed for MSI using NGS-based detection programs on targeted sequencing NGS data.
DNA extraction
The DNA samples from primary thyroid tumor tissue were snap frozen in liquid nitrogen after biopsy, digested with proteinase K, and extracted using phenol-chloroform methods. Twenty MTC cases were prepared using the same methods. For six ATC cases, formalin-fixed paraffin-embedded (FFPE) samples were deparaffinized using xylene, and DNA was extracted with phenol-chloroform methods. Thirty FTC samples were deparaffinized using xylene and extracted using the QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany). In the case of samples where adjacent normal thyroid tissue was unavailable, blood or mouthwash DNA was used. In the three cases that lacked adjacent normal thyroid tissue, skeletal muscle tissue was used for two cases and lymph node tissue for one.
PCR-based MSI testing
Marker-specific PCR primers for amplification of five microsatellites were used, with a fluorescein amidite (FAM) M13 universal forward primer, as previously described (16). Capillary electrophoresis was performed with an ABI PRISM® 3730 DNA Analyzer (Thermo Fischer Scientific, Waltham, MA) to detect strand-slippage mutations indicative of MSI. Malignant samples were compared with their germline DNA, a negative experimental control, and three MSI-H colorectal cancer control samples.
Whole-exome sequencing
Libraries were prepared using the KAPA Hyper Prep Kit (Roche, Basel, Switzerland) and were enriched using the xGEN® Exome Research Panel v1.0 (Integrated DNA Technologies, Coralville, IA). Sequencing was performed on a HiSeq4000 (Illumina, Inc., San Diego, CA) at The Genomics Services Laboratory at Nationwide Children's Hospital (Columbus, OH). Sequencing reads were aligned to hg19 using bwa v0.7.14 (17). Deduplication was performed using Picard v2.3.0 (18). Quality recalibration and local realignment around indels was performed with Picard and GATK v3.5 (19). Somatic single-nucleotide variations (SNVs), somatic indels, and germline SNVs were called using VarScan2 v2.3.9 (20).
TMA preparation
Thyroid resection specimens from 110 patients who were diagnosed with FTC were selected for the TMA. Hematoxylin and eosin slides of resection specimens were reviewed to select FFPE tissue blocks. All specimens included in this study contained a tumor surface area of >1 cm2 and had multiple available tumor blocks. TMAs were performed using duplicate 1 mm diameter cores. IHC of MLH1, PMS2, MSH2, and MSH6 was evaluated for all specimens with control reactivity of selected normal thyroid tissue. MMR protein expression was considered intact if convincing nuclear staining was present in >1% of tumor cells. IHC was repeated on whole tissue sections from nine cases that showed weak or absent staining in the presence of inadequate available internal controls on TMA slides.
Targeted sequencing
Sequencing libraries were prepared using the Oncomine v1 Assay, which amplifies 2530 target regions in 143 genes, and sequenced on an Ion Torrent platform. In brief, 20 ng of DNA extracted from FFPE or fine-needle aspirate tumor samples and matched normal controls was utilized per assay. Library preparation and subsequent analytical steps were completed, as previously described (21,22). Microsatellites contained in the Oncomine panel were identified and examined for strand-slippage mutations using MonoSeq, as previously described (23). MSI was determined for each microsatellite in each sample by comparing the percentages of reads containing strand-slippage mutations between paired tumor and normal DNAs.
Results
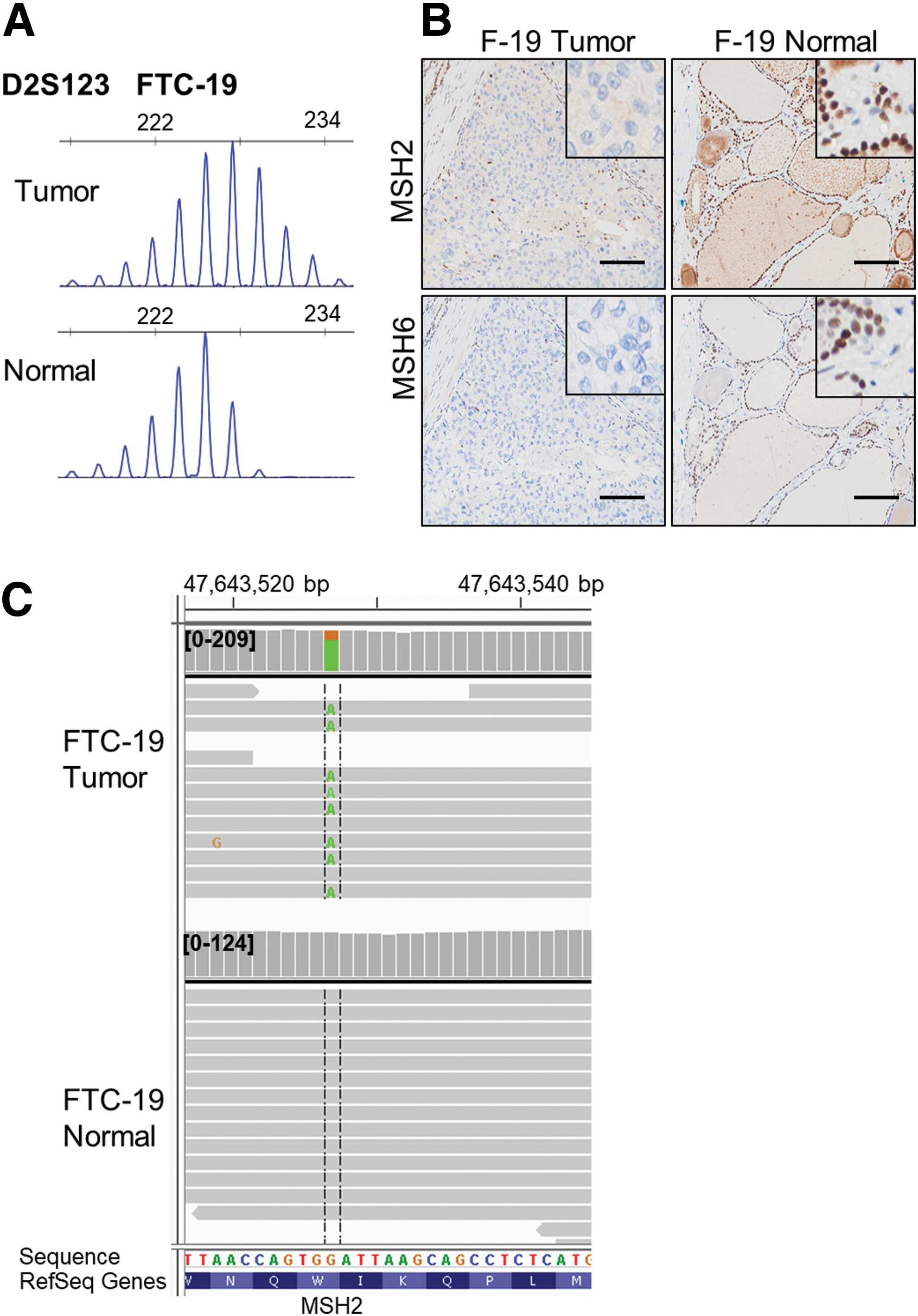
A set of 191 thyroid cancer tumor samples from 122 PTC, 35 FTC, 20 MTC, and 14 ATC patients was screened for MSI using PCR followed by capillary electrophoresis of four microsatellites from the Bethesda panel used for MSI detection (BAT25, BAT26, D17S250, and D2S123). Two out of 35 FTC samples showed clear instability at multiple microsatellites (Fig. 1A, Supplementary Fig. S1, and Supplementary Table S1). None of the PTC, MTC, or ATC tumor samples displayed MSI, although two ATC samples had single base pair insertions or deletion mutations for BAT26 (Supplementary Table S1). Loss of MMR protein expression was validated in the two MSI-H FTC cases by IHC. Tumor FTC-19 showed loss of expression of MSH2 and MSH6, while the staining of FTC-34 for MLH1 and PMS2 was equivocal (Fig. 1B and Supplementary Fig. S2).
(
To investigate underlying mutations in MMR genes and to validate MSI in these cases orthogonally, whole-exome sequencing was performed. FTC-34 was confirmed to be MSI-H by both the MANTIS tool and MSISensor (24), whereas FTC-19 was not sequenced to adequate depth for evaluation with these tools (Supplementary Table S2). In FTC-19, a nonsense mutation was detected in MSH2 (NM_000251:c.1035G>A, p.W345*) with a variant allele fraction (VAF) of 0.76, which is indicative of loss of heterozygosity. As the corresponding adjacent normal tissue did not harbor the MSH2 mutation, Lynch syndrome can be ruled out (Fig. 1C). In the other MSI-H case, FTC-34 did not have any loss-of-function mutations in the MMR genes, and it is speculated that MSI is a result of epigenetic silencing of MLH1.
To determine the overall frequency of MSI in FTC, an additional 110 FTC tumor samples from a different cohort of patients were assembled into a TMA, and IHC microscopy for the four MMR proteins was performed. Two of 110 cases were MMR deficient, with both lacking expression of MSH2 and MSH6 (Supplementary Fig. S3 and Supplementary Table S3).
Finally, as a validation of these experiments, the study sought to use available targeted NGS data from an additional 188 thyroid carcinomas (74 PTC, 45 MTC, 37 ATC, 18 PDTC, 11 FTC, and 3 Hürthle cell carcinomas) to determine MSI status in these tumors using the MonoSeq variant caller. Since previous studies using MonoSeq to investigate MSI status relied on data generated from Illumina sequencers (12,23) and the thyroid carcinoma NGS data were generated using an Ion Torrent platform, first the accuracy of MonoSeq to determine MSI status of samples sequenced with an Ion Torrent correctly was examined. MonoSeq was used to determine the MSI likelihood scores for each of 19 colorectal cancers of known MSI status (9 MSI-H and 10 MSS), and there was a clear separation of the two groups (Supplementary Fig. S4A). Therefore, MonoSeq was applied to the thyroid carcinoma samples, and 10 outliers were identified that were the most likely to be MSI-H (3 PTC, 3 FTC, 2 ATC, 1 PDTC, and 1 MTC; Supplementary Fig. S4B). Five of these cases had available paired tumor and normal DNA, and PCR-based MSI detection was performed using the five Bethesda panel microsatellites. None of these cases showed MSI for any of the assessed markers (Supplementary Table S4), making it unlikely that any of the samples in this cohort were MSI-H.
Discussion
This study found that 2.5% (4/156) of FTC cases displayed MSI. MSI was not detected in the 327 thyroid cancers of other histologies. The MSI-H FTC cases were evaluated for expression of MMR proteins using IHC, and three were deficient in MSH2/MSH6, while the remaining case showed equivocal expression of MLH1/PMS2 (Supplementary Figs. S2 and S3). Additionally, one of these cases harbored a somatic hemizygous loss-of-function mutation in MSH2 (Fig. 1).
Previous investigations of MSI in thyroid cancer have produced controversial results (Table 1). One study reported MSI is present in >80% of cases (25), whereas others have reported it to be entirely absent (26 –29). It is speculated that the elevated MSI rates in many of the early investigations can be attributed to frequent false-positives from the use of polyacrylamide gels for determination of microsatellite lengths, which can confound accurate determination of MSI status. In a report where the more accurate method of measuring microsatellite lengths using capillary electrophoresis was employed, MSI was found to be completely absent in thyroid cancer (26). More recently, investigations have used NGS data to determine the rate of MSI. Those that were limited to PTC showed a complete absence (14,30), whereas a report by Le et al. including other thyroid cancer histologies showed approximately 2% of cases were MSI-H (5). The present study highlights the importance of examining molecular phenotypes in uncommon subtypes of cancers that are not represented well in large data sets.
It is not unexpected that MSI was found in FTC but not in PTC, since the genetic events that are typically found in these two histologic subtypes are distinct (31,32). The most commonly mutated gene in PTC is BRAF, which is mutated in about 45% of tumors, but BRAF mutations are almost never seen in FTC patients (33 –38). In addition, FTCs often display aneuploidy, which is rare in PTCs, and have a higher mutational burden compared to PTCs (38,39). Although both FTC and PTC patients typically have favorable prognoses (40), a small subset of patients display widely invasive disease, and for these patients, the five-year survival rate drops to 38% (41).
In cancer types that show high rates of MSI, such as endometrial and colorectal cancer, MMR deficiency is widely regarded as an early event in carcinogenesis (42 –48). In contrast, whole-exome sequencing data in this study from FTC-19 showed that the somatic, hemizygous loss of function mutation in MSH2 had a VAF of 0.76, which is consistent with a subclonal mutation that occurred late in tumor development (a fully clonal hemizygous mutation would have a VAF of 1). Further supporting the concept that MMR inactivation is a late event and does not contribute to carcinogenesis are two independent reports of Lynch syndrome patients who presented with thyroid carcinomas that were not MSI-H (49,50). Additionally, in the study by Le et al., who reported ∼2% of thyroid carcinomas were MSI-H, all of the MSI-H thyroid cancers were late stage (5). It was previously reported that MSI is absent in diagnostic samples of acute myeloid leukemia (AML) (23). However, MSI has been found in smaller, subclonal populations of AML, indicating it can occur as a late event in cancer evolution (51).
Tumor MSI status has become more clinically relevant because of the remarkable response of patients with MSI-H cancers to treatment with programmed cell death protein 1/PD-L1 immune checkpoint inhibitors such as nivolumab and pembrolizumab. In one report, an FTC patient who presented with MSI-H disease and a somatic frameshift mutation in MSH2 was treated with pembrolizumab and had an ongoing partial response (52).
In conclusion, the present results indicate that at least a small percentage of FTC patients have MSI/MMR defects. This suggests that in some instances, clinical MSI testing and potential use of checkpoint inhibitor therapy should not be overlooked for FTC patients.
Footnotes
Acknowledgments
The authors would like to acknowledge: the patients who consented to provide material for this study; Jan Lockman and Barbara Fersch for administrative help; the OSUCCC Genomics Shared Resource and the Plant Microbe Genomics Facility for sequencing assistance; the OSUCCC Human Cancer Genetics Sample Bank for sample processing and storage; and the Ohio Supercomputer Center for computational resources. This work was supported by the Leukemia Clinical Research Foundation, the Pelotonia fellowship program, and the National Cancer Institute Grants P01CA124570 and P50CA168505.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4