
Abstract
Background:
Thyroid eye disease (TED) develops in around 25% of those with Graves' disease (GD). Patients with TED may present late to ophthalmologists, when debilitating orbital inflammatory changes have already occurred. The reasons for this are multifactorial, but poor knowledge of TED in GD patients may be contributory. This study aimed to assess the knowledge of TED in those with established TED, GD without orbitopathy, and control subjects.
Methods:
A validated, anonymized questionnaire, with 20 knowledge-based questions, was prospectively completed by 100 GD patients, 100 TED patients, and 100 age- and sex-matched controls (with no history of thyroid disease or TED) in two tertiary referral thyroid and orbital diseases clinics. Demographic data and details of highest educational level, disease duration, and follow-up were gained. Residence postcode was used to determine Index of Multiple Deprivation (2015) quintile. Knowledge score was established for each of the study groups of interest. Statistical analysis was undertaken with Kruskal–Wallis test, chi-square test, and multivariable logistic regression.
Results:
There was no significant difference in median knowledge scores (out of 20) between GD (13.71, range 9–18) and TED (14.25, range 9–18) patients. However, both groups had significantly higher scores than controls (11.53, range 4–16; p < 0.001). Multivariable analysis determined no particular independent factor associated with lower knowledge score. There were a number of important areas in which patient knowledge of TED was poor. While almost all (99% TED, 89% GD) knew that TED involved orbital tissue inflammation, a large proportion (60% TED, 50% GD) were unaware that TED may develop in the absence of hyperthyroidism or did not know that cigarette smoking is associated with more severe TED (21%TED, 33% GD).
Conclusions:
TED patients had equivalent levels of TED knowledge compared to GD patients without orbitopathy. While subjects in both disease groups had greater knowledge than controls, each had significant misconceptions regarding aspects of TED diagnosis, management, and treatment. These findings should guide the future provision of patient information for TED, with educational materials being targeted to address existing gaps in knowledge.
Introduction
Previous studies have demonstrated that increased patient knowledge of a disease results in earlier presentation to health services, better insight into that condition, reduced anxiety, and increased compliance with treatment (1). This is especially important in thyroid eye disease (TED), an inflammatory condition of the orbital tissues that occurs in around 25% of those with the autoimmune disorder Graves' disease (GD) (2). GD develops before or at the same time as TED in around 80% of cases (3), and of those with GD who do develop TED, around 70% will develop orbital manifestations within 12 months of their GD diagnosis (4).
However, evidence also exists that patients present late with TED, with a mean time from development of ocular symptoms to TED diagnosis of nine months (5). This represents a lost opportunity for early intervention (e.g., with early immunosuppression or targeted smoking cessation) with the possible prevention or reduction of the subsequent physically and psychosocially debilitating effects of TED.
While it might be expected that a proportion of patients with GD will search the Internet for information about ocular problems related to autoimmune thyroid disease, it has been demonstrated that online information regarding TED is of poor readability. This means that patients may not be able to understand fully the potential morbidity associated with TED or the available strategies to reduce the impact of early symptoms, such as the use of topical lubricants, as well as those to prevent development of severe TED, including smoking cessation (6).
To the authors' knowledge, no study to date has objectively assessed the level of knowledge of TED in either patients with TED or those with GD who are at risk of subsequently developing TED. This study aimed to assess and compare TED knowledge between GD patients (with and without ocular or orbital manifestations) and controls in order to identify any misconceptions about TED and to determine factors that may predict poorer understanding of TED.
Methods
The study model was based on previous research assessing patient knowledge of glaucoma by Danesh-Meyer et al. (1). Recruitment sites for the study were the Thyroid Clinic of the University Hospital Birmingham (Birmingham, United Kingdom; TED and GD subjects) and the Orbital Diseases Clinic of the Birmingham and Midland Eye Centre (Birmingham, United Kingdom; TED subjects only). The study followed the principles of the Declaration of Helsinki and was approved by the research and development departments of both hospital trust recruitment sites.
Study subjects were recruited into three groups: those with established TED, those with GD but no manifestations of ocular or orbital disease, and age- and sex-matched controls. Patients were eligible for inclusion in the GD group if they had this diagnosis made by a consultant endocrinologist on the basis of abnormal thyroid function tests (overt hyper- or hypothyroidism) either at the time of recruitment or previously, as well as raised concentrations of thyrotropin receptor (TSH-R) antibodies. Overt hyperthyroidism was defined as undetectable serum TSH concentrations with raised serum free thyroxine (fT4) and/or free triiodothyronine concentrations. Overt hypothyroidism was defined as raised serum TSH concentrations with reduced serum fT4 concentrations. Subjects were eligible to be included in the TED group if they had the above criteria for GD, in addition to a diagnosis of TED made by a consultant ophthalmologist, for six months or more on the basis of signs of orbitopathy (e.g., proptosis, periocular swelling, and strabismus/ocular movement restriction). The control group was recruited randomly from patients, family members, and friends attending non-thyroid and non-orbit outpatient clinics at the University Hospital Birmingham. Exclusion criteria for control subjects included a personal or family history of thyroid dysfunction or TED.
An anonymized questionnaire was developed for GD, TED, and control subjects (Supplementary Data S1), the first section of which sought demographic information (age, sex, and ethnic origin), level of educational attainment (no qualifications, secondary school education, vocational qualifications, university degree, or higher degree), and first language spoken at home. Residence postcode was used to determine an Index of Multiple Deprivation (IMD) 2015 score using the GeoConvert Web site (
The second section of the questionnaire (Supplementary Data S2) comprised 20 true/false format questions. These questions were written and discussed at a focus group of two endocrinologists and two ophthalmologists, with the aim being to explore patient knowledge of TED diagnosis, disease-modifying factors, and treatment. Feedback on the questions was requested from members of the British-based TED charity, Thyroid Eye Disease Charitable Trust (TEDct), to ensure that the questions were of sufficient quality and importance. The questionnaire was piloted on 10 TED patients prior to the commencement of the full study. Following this validation period, the questionnaire was personally administered to and completed by all study subjects while they were in the outpatient clinic environment, ensuring that it was not possible for participants to search for the correct answers to questions while completing the questionnaire.
Statistical analysis was undertaken for non-normally distributed data using the Mann–Whitney test (two groups) and Kruskal–Wallis test (three or more groups) for continuous data and the chi-square test for categorical data. Multivariable logistic regression was undertaken to determine if differences in knowledge scores were associated with any independent variable. Analyses were undertaken using GraphPad Prism v5.0 (GraphPad Software, La Jolla, CA) and IBM SPSS Statistics for Windows v18 (IBM Corp., Chicago, IL). A p-value of <0.05 was considered statistically significant.
Results
The study was undertaken over a 12-month period, with 300 consecutive subjects recruited. There were 100 TED, 100 GD, and 100 control subjects in each study group. The groups were well matched for age and sex.
The overall TED knowledge scores for each of the study groups are shown in Figure 1. The median knowledge scores were 14.25/20 (range 9–18) in the TED group, 13.71/20 (range 9–18) in the GD group, and 11.53/20 (range 4–16) in the control group. There was no significant difference between the scores in the TED group and GD group, but both of these groups scored significantly higher than the controls (p < 0.001). The proportion of correct answers for each of the groups was significantly different for some but not all of the 20 questions (Table 1).
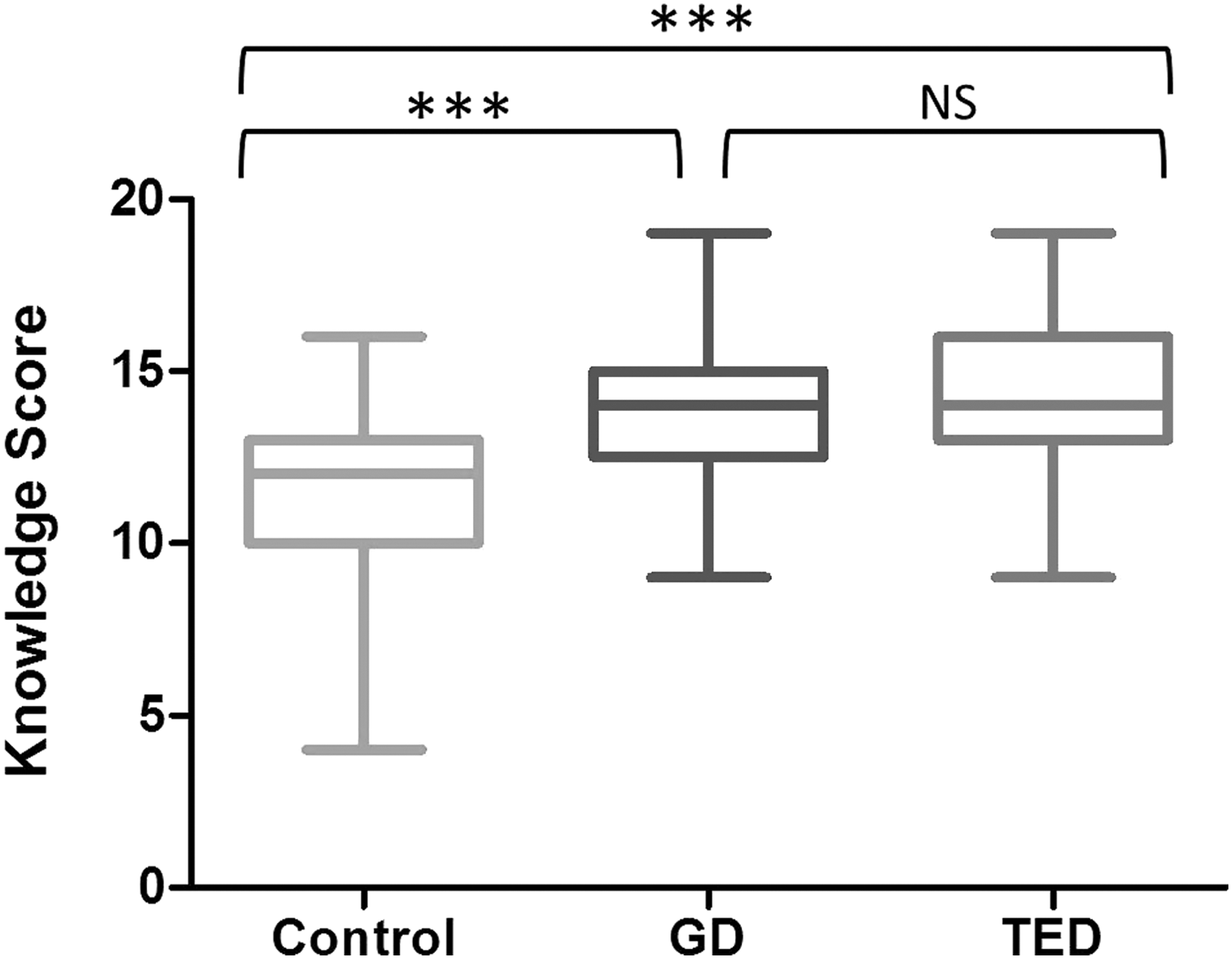
Median knowledge scores of 13.71/20 for Graves' disease (GD; range 9–18) and 14.25/20 for thyroid eye disease (TED; range 9–18) subjects were not significantly different. However, both GD and TED subjects had higher knowledge scores than controls (11.53/20; range 4–16). Kruskal–Wallis test (with Dunn's post-test) ***p < 0.001. NS, not significant.
Median Scores for Each of the 20 Questions for Control, Graves' Disease (GD), and Thyroid Eye Disease (TED) Participants
Correct answers against which patient responses were marked, as determined by Pubmed literature review for each of the questions, are presented at the end of each question (T, true; F, false). Statistical analysis was performed with the chi-square test. For each question, the level of statistical significance of the difference in knowledge score varied (*GD significantly different from control, †TED significantly different from control, §TED significantly different from GD), but in each case was p < 0.05. Univariate analyses determined no significant difference in knowledge scores in GD and TED subjects according to age, sex, race/ethnicity, level of educational attainment, first language, or Index of Multiple Deprivation 2015 quintile. Likewise, there was no significant difference in knowledge score by duration of GD or TED, period over which seen in thyroid or orbit clinic, or whether patients had undergone medical or surgical treatment for TED. Multivariable analyses determined no factor to be independently associated with a higher or lower TED knowledge score.
Univariate analyses determined no significant difference in TED knowledge scores according to age, sex, race/ethnicity, level of highest educational attainment, first language, or IMD 2015 score. Similarly, there was no significant difference in TED knowledge scores in relation to disease duration following diagnosis of GD or TED, the duration of follow-up in the thyroid or orbit clinic, whether patients had ever been seen and assessed by an ophthalmologist, whether patients had received steroids or orbital radiotherapy for TED, or whether they had undergone emergency or rehabilitative surgery for TED. Furthermore, multivariable analysis determined that there was no factor independently associated with higher or lower TED knowledge score in any of the study groups.
Discussion
To the authors' knowledge, this is the first study to evaluate the level of TED knowledge in GD patients with and without orbitopathy. While GD and TED patients scored significantly higher than controls from a statistical point of view, the actual practical difference in knowledge scores (two to three points higher than the controls) for GD and TED patients is likely to be insignificant. Indeed, TED patients only scored significantly higher than controls in 13/20 (65%) questions, while GD patients scored higher than controls in 8/20 (40%) questions.
It is perhaps surprising that those with a longer duration of GD or TED, or TED that had required steroid treatment, orbital radiotherapy, or surgical intervention, did not score more highly. Similarly, those with a shorter duration of GD or TED may have been anticipated to score more highly, as they may have been expected to have sought out relevant information more recently or had more recent contact with their endocrinologist or ophthalmologist. However, this did not prove to be the case. This may also indicate that recent attempts by endocrinologists and ophthalmologists to educate those with GD and TED were unsuccessful.
In univariate analysis, no significant difference was observed in knowledge scores by age, sex, race/ethnicity, highest educational attainment, first language, IMD 2015 score, or duration of follow-up in the thyroid or orbit clinic. Likewise, no factor was found to be independently associated with higher or lower TED knowledge scores on multivariable analyses.
Studies evaluating patient knowledge of other diseases have noted that higher educational level and socioeconomic status are associated with earlier presentation to medical services, increased knowledge of disease, and better compliance with treatment regimens (1). Other studies have shown higher knowledge scores for diseases such as glaucoma and diabetic retinopathy in those whose first language is English (1,7,8), mainly as the questionnaires in these studies were written in English. Such an association was not found in this study. Studies assessing conditions such as uveitis have also determined patient knowledge of their own condition to be poor (9).
Significant misconceptions were identified in key areas that may impact upon drivers for worse TED in GD patients, such as the importance of good thyroid function control and the crucial role of smoking in TED. While both GD and TED patients scored significantly higher than controls in terms of demographic aspects of TED (e.g., questions 4 and 7), only 50% of GD and 40% of TED patients knew that TED does not necessarily only occur in those with hyperthyroidism (question 1). This might result in euthyroid or hypothyroid GD patients becoming complacent in having a perception that they are less likely to develop TED, even if experiencing ocular symptoms. Likewise, while GD and TED subjects scored relatively highly regarding TED pathogenesis (e.g., questions 8, 12, 16, 17, and 20), only 67% of GD and 79% of TED patients knew about the association between smoking and more severe TED. Furthermore, knowledge of the surgical management of TED appeared poor, with GD and TED subjects overestimating the effectiveness of thyroidectomy in treating TED (question 9), overestimating the tendency of radioiodine to worsen TED (question 15), and demonstrating poor knowledge regarding the role of orbital radiotherapy and orbital decompression (questions 18 and 19) in the management of some TED patients. It is also important to note that around two-thirds of GD and TED subjects perceived that psychological stress made TED worse (question 5). While no published literature currently exists regarding an association between stress and TED, the weighting that the GD and TED patient groups gave to this area suggests that it may be an interesting avenue for further research.
Those with TED are known to have delay to presentation from their initial experience of ocular symptoms, with recent Europe-wide data determining that the median period is nine months (although with a range of 0–552 months) (5). Similarly, in a multicenter British audit, the mean time from initial symptoms of TED to diagnosis was >27 months, and from first visit to any doctor with ocular symptoms to TED diagnosis was more than nine months (10). The reasons for this are multifactorial, but may include the patient themselves not presenting sufficiently early, as initial symptoms of grittiness and soreness may be perceived as being due to an allergy or conjunctivitis. Nevertheless, this duration is shorter than in earlier studies from 15 years ago when the median time from symptoms to diagnosis was 16 months (range 0–720 months) (11). This is important, as studies have shown that treatments may be more efficacious when a diagnosis of TED is made earlier (12). In addition, delay to diagnosis may result in increased time to intervention, with the possibility of developing morbidity, including loss of vision, diplopia, and disfigurement, but also loss of work, income (13), reduced quality of life, social status, as well as negative psychosocial consequences (14).
The objectives of the Amsterdam Declaration for people with TED in general were to minimize the morbidity associated with TED, improve patients' experience and quality of life, and prevent the development of TED in people at high risk (15). There has been an increasing recognition of the importance of early diagnosis of TED, with agencies such as the UK Thyroid Eye Disease Amsterdam Declaration Implementation Group advocating that GD patients be issued with early warning cards to prompt them to seek urgent assessment if ocular symptoms develop (16). Clinical assessment tools, such as Diagnosis of Graves' Orbitopathy (17), to aid endocrinologists in making an earlier diagnosis of TED in GD patients have also been devised. However, if patients do not adequately understand their medical condition, these may be of lesser utility. Patient and public involvement in TED has been attempted (18), and in the United Kingdom, there are support agencies such as TEDct and the British Thyroid Foundation. There are also numerous Web sites with patient information for people with TED. However, studies indicate that the actual readability of the information on these Web sites is poor and therefore may not be understood by GD and TED patients (6).
Endocrinologists and ophthalmologists need to have an understanding of the level of knowledge their patients with GD, with and without ocular manifestations, have about TED. In the former group of patients, good understanding may result in medical advice being sought in good time. In the latter, patient knowledge and understanding may result in better motivation to make necessary life-style modifications, adhere to treatment regimens, and have an awareness of the available treatment modalities. Endocrinologists and ophthalmologists also need to know which areas of TED knowledge may be deficient so that these can be effectively targeted and emphasized during the usually short clinic attendances that may be afforded in busy outpatient clinics. Despite time and resource limitations, physicians still have responsibility for ensuring that patients are appropriately counseled regarding important aspects of GD with and without orbitopathy.
The answers given by GD and TED patients in this study demonstrate a number of misconceptions that endocrinologists and ophthalmologists need to be aware of and try to overcome. The findings indicate the need to tailor educational efforts and materials to deficient areas and to focus on important aspects of TED knowledge with the aim of dispelling misconceptions.
It is recommended that endocrinologists and ophthalmologists undertake similar surveys of the knowledge of their own GD and TED patients to gauge patient knowledge more accurately as a surrogate of local performance in GD and TED patient education and information retention. It is acknowledged that it is not possible to guarantee the wider applicability of the results of this survey to other national and international specialist clinics. However, the city in which the study was undertaken is a very culturally and ethnically diverse region of the United Kingdom, and the respondent population was large and truly represents an unbiased regional cross-section. There are also more holistic means of assessing patient knowledge beyond true/false format questionnaires (e.g., structured interviews), but the data do demonstrate real-world responses of GD and TED patients to extremely pertinent questions regarding their presentation, assessment, and treatment.
In summary, this is the first study to evaluate the level of TED knowledge in GD patients with and without orbitopathy, and to provide a comparison with the knowledge levels of the public in general. GD and TED knowledge scores were significantly higher than controls from a statistical point of view, but not necessarily from a practical point of view. Significant misconceptions and knowledge gaps in important areas were observed. These data should be used to inform future decisions about the provision of patient information for those with GD and TED and will facilitate the tailoring of educational materials to these patients.
Footnotes
Acknowledgments
We would like to thank committee members of the TEDct for their feedback on the content of the knowledge questionnaire. We would also like to thank Mr. Alastair Denniston, Consultant Ophthalmologist, for reviewing the questionnaire, and Miss Faye Mellington, Consultant Oculoplastic Surgeon, for her permission to distribute questionnaires to patients with TED in the orbital diseases clinic at Birmingham and Midland Eye Centre.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data S1
Supplementary Data S2