
Abstract
Background:
The lymphocyte-to-monocyte ratio (LMR), which reflects the tumor-infiltrating immune cell status and host immunity, has been reported as a prognostic marker in various cancers. The aim of the present study was to evaluate the role of the LMR as a prognostic marker in predicting the survival of patients with anaplastic thyroid carcinoma (ATC).
Methods:
This study retrospectively included 35 ATC patients with available complete blood cell count data. The primary outcome was the overall survival (OS) of patients with ATC.
Results:
There were no significant differences between the LMR of the baseline and that of the follow-up complete blood cell count data (p = 0.53). The patients were divided into two groups based on their baseline LMR: a low LMR group (<4; n = 23, 66%) and a high LMR group (≥4; n = 12, 34%). The proportion of cervical lymph node metastasis in the low LMR group was significantly higher than that in the high LMR group (p = 0.021). The OS curves were significantly different based on the LMR values, and the median OS of the low and high LMR groups were 3.0 and 9.5 months, respectively (p = 0.004). In multivariate analysis, a low LMR was also an independent risk factor for all-cause mortality in patients with ATC (hazard ratio = 2.55 [confidence interval 1.08–6.00], p = 0.032) after adjusting for sex, tumor size, and distant metastasis.
Conclusions:
A low LMR is associated with poor survival in patients with ATC. The LMR could be a simple and stable prognostic biomarker reflecting host immunity in patients with ATC. Further studies are needed to confirm the prognostic role of the LMR in ATC.
Introduction
The host immune system plays an important role in the suppression and progression of malignancies (1,2). Therefore, previous studies have reported the lymphocyte-to-monocyte ratio (LMR) as a simple prognostic marker reflecting the status of the host immune system in various solid tumors, such as lung, pancreas, colon, and breast cancers as well as hematologic malignancies (3 –8). Tumor-infiltrating lymphocytes (TILs) have humoral and cellular antitumor effects (9 –11). Conversely, tumor-associated macrophages (TAMs), which are derived from circulating monocytes, can accelerate tumor progression via the production of growth factors and cytokines that play a role in angiogenesis and anti-immune reaction (2,6,12,13). The LMR, which is calculated from the peripheral blood lymphocyte and monocyte count, may reflect the tumor-infiltrating immune cell status and act as an indirect indicator of host immunity.
The thyroid gland is highly immunogenic, and some immunologic characteristics are known to be associated with the prognosis of thyroid cancer (2). In a previous study, the coexistence of lymphocytic thyroiditis was significantly associated with favorable outcomes in papillary thyroid cancer (14). Furthermore, increased TAM infiltration is reportedly associated with poor survival of patients with anaplastic thyroid carcinoma (ATC), the most fatal form of thyroid cancer (15 –19). These studies suggest the important role of the immune system in the progression of thyroid cancer. However, the clinical implications of the LMR in thyroid cancer are not clearly elucidated (20). It was hypothesized that a low LMR may be associated with poor survival of patients with ATC because increased TAM infiltration is known as a poor prognostic marker for ATC.
The present study evaluated the role of the LMR as a prognostic marker for predicting the overall survival (OS) of patients with ATC.
Methods
Subjects
Between January 2000 and May 2018, a total of 87 patients were histologically confirmed to have ATC at the Asan Medical Center, Seoul, Republic of Korea. The present retrospective study included patients with ATC who were >20 years of age with available baseline and follow-up complete blood cell count (CBC) data. The exclusion criteria were as follows: ATC from recurrent differentiated thyroid carcinoma, unavailable baseline and follow-up CBC data, double primary cancer, and very unstable status at diagnosis. Thirty-five patients were included in the present study. The patients were divided into two groups based on their treatment: palliative and multimodal treatment (MMT) groups. MMT was defined as surgery with postoperative radiation and/or chemotherapy (21 –23). Figure 1 shows a study flow chart. The study protocol was approved by the Institutional Review Board of the Asan Medical Center.
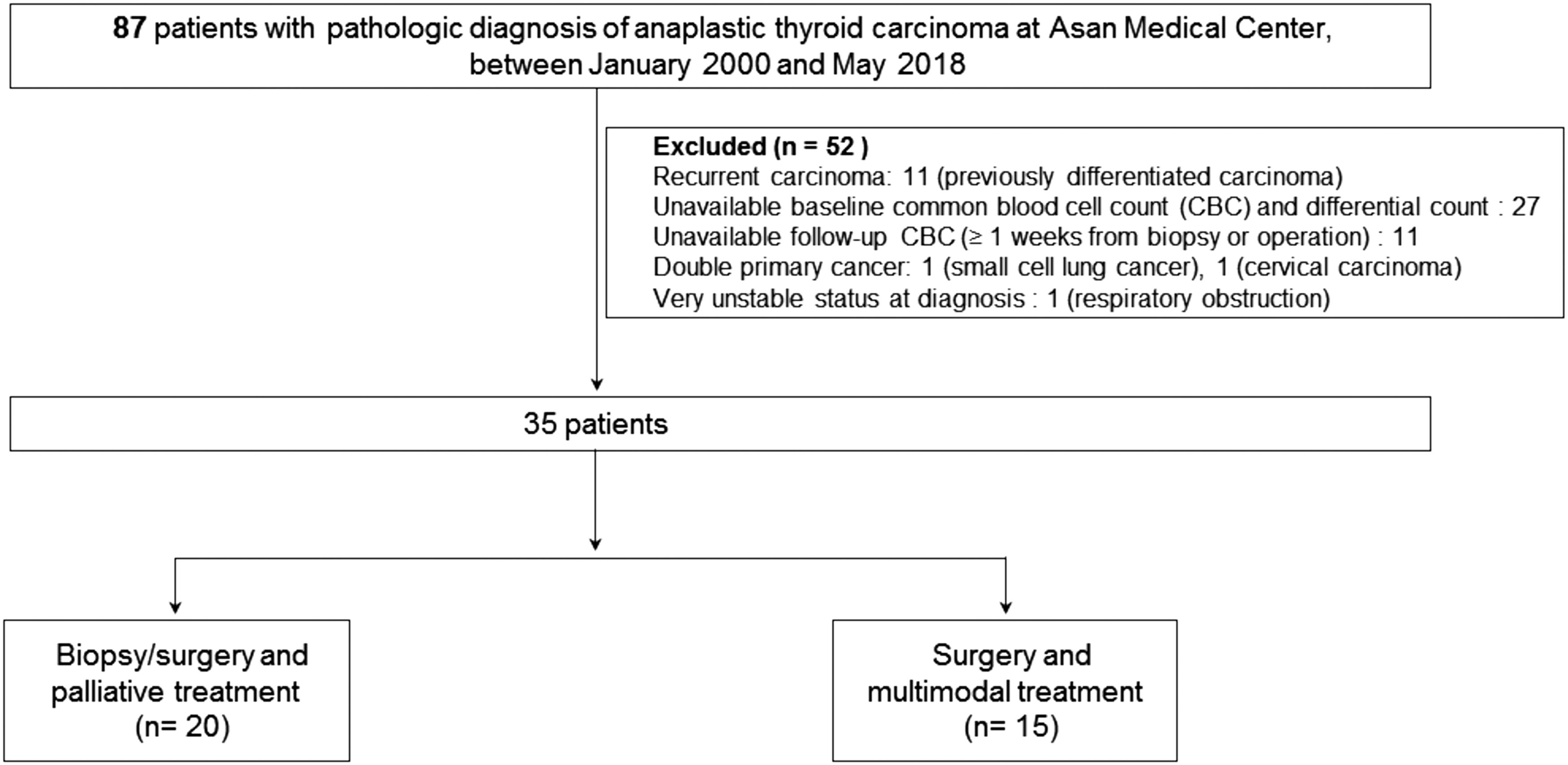
Study flow chart.
Definitions
The eighth edition of the American Joint Committee on Cancer tumor-node-metastasis (TNM) staging system was used to determine the TNM stage (24,25). In seven (20%) patients who underwent biopsy alone, the tumor size was defined as the greatest dimension measured using ultrasonography (US), and the presence of lymph node (LN) metastasis was estimated by using US or computed tomography. Baseline CBC data were obtained when the patients were in a stable condition before undergoing surgery or biopsy for ATC. The follow-up CBC was obtained at least seven days after surgery or biopsy for ATC. The LMR was calculated from the CBC as the absolute lymphocyte count divided by the absolute monocyte count. The primary outcome was OS, which was calculated as the date of diagnosis to the date of death from any cause.
Statistical analysis
R v3.4.4 (R Foundation for Statistical Computing, Vienna, Austria) was used to conduct all statistical analyses. Continuous and categorical variables are presented as the median with interquartile range (IQR) and numbers (percentages), respectively. A paired t-test was used to compare the baseline and follow-up CBCs. To evaluate the optimal cutoff levels for the LMR, receiver operating characteristic (ROC) analysis was performed evaluating the area under the curve (AUC) value and confidence interval (CI). The characteristics of the two groups were compared using the chi-square test for categorical variables and Wilcoxon's rank-sum test for continuous variables. The OS curves were plotted using the Kaplan–Meier method, and the log-rank test was used to determine their significance. A Cox proportional hazards model was used to evaluate the prognostic values of the LMR, age, size, sex, LN metastasis, and distant metastasis on the OS of patients with ATC. Statistical significance was considered if p < 0.05.
Results
Baseline characteristics of patients with ATC
Table 1 shows the baseline characteristics of the 35 patients with ATC. The median age at the time of diagnosis was 68 years (IQR 60.5–75.0 years), and 68.6% of patients were female. The median tumor size was 4.5 cm (IQR 3.7–6.5 cm). Based on the eighth edition of the TNM staging system, 83% of patients had T4 tumors or cervical LN metastasis. Approximately half of the patients (n = 16; 46%) also had distant metastasis. The numbers of patients with stage IVA, IVB, and IVC disease were 1 (2.9%), 18 (51.4%), and 16 (45.7%), respectively. Of the 35 patients with ATC, 20 (57.1%) received palliative treatment after diagnosis by surgery or biopsy, and 15 (42.9%) received MMT (Fig. 1). The median survival was 4.3 months (IQR 2.1–8.9 months).
Baseline Characteristics of Patients with ATC
Continuous variables are presented as median (interquartile range). Categorical variables are presented as number (percentage).
ATC, anaplastic thyroid carcinoma; TNM, tumor-node-metastasis stage according to the eighth TNM staging system; LMR, lymphocyte-to-monocyte ratio.
Optimal cutoff value of the LMR
The baseline LMR and follow-up LMR values were compared to evaluate whether the LMR may serve as a stable marker indicating host immunity. The median baseline LMR was 2.9 (IQR 2.2–4.4), and the median interval between the day of baseline CBC collection and the day of surgery/biopsy was 16 days (IQR 8–26 days). The median follow-up LMR was 3.8 (IQR 1.7–5.9), and the median interval between the day of follow-up CBC collection and the day of surgery/biopsy was 29 days (IQR 16–51.5 days). Results of the paired t-test showed no significant differences between the baseline and follow-up LMRs (p = 0.53). Therefore, the baseline LMR value was regarded as a possible prognostic marker indicating host immunity for patients with ATC. By ROC analysis, the optimal cutoff level for the LMR was 4.22 for OS, and the AUC value was 0.84 (sensitivity 0.8; specificity 1.0). With this result, the patients with ATC were subclassified into two groups: the low LMR group with a LMR <4 (n = 23; 66%), and the high LMR group with a LMR ≥4 (n = 12; 34%). When the clinicopathologic parameters were compared between the two groups, there was significantly more cervical LN metastasis in the low LMR group compared to the high LMR group (p = 0.021). The baseline lymphocyte counts of the low LMR group were significantly lower than those of the high LMR group (p = 0.023), and the baseline monocyte counts of the low LMR group were significantly higher than those of the high LMR group (p < 0.001; Table 2).
Clinicopathologic Parameters Based on LMR
Continuous variables are presented as median (interquartile range). Categorical variables are presented as number (percentage).
OS based on the LMR
All-cause mortality and OS of patients with ATC based on the LMR were evaluated. The OS curves differed significantly based on the LMR value (p = 0.004). The median OS of the low LMR group was 3.0 months, and that of high LMR group was 9.5 months (Fig. 2). In univariate analysis, a low LMR, male sex, large tumor size (>4 cm), and the presence of distant metastases were associated with all-cause mortality. In multivariate analysis, a low LMR was an independent risk factor for all-cause mortality in patients with ATC (hazard ratio = 2.55 [CI 1.08–6.00], p = 0.032; Table 3).
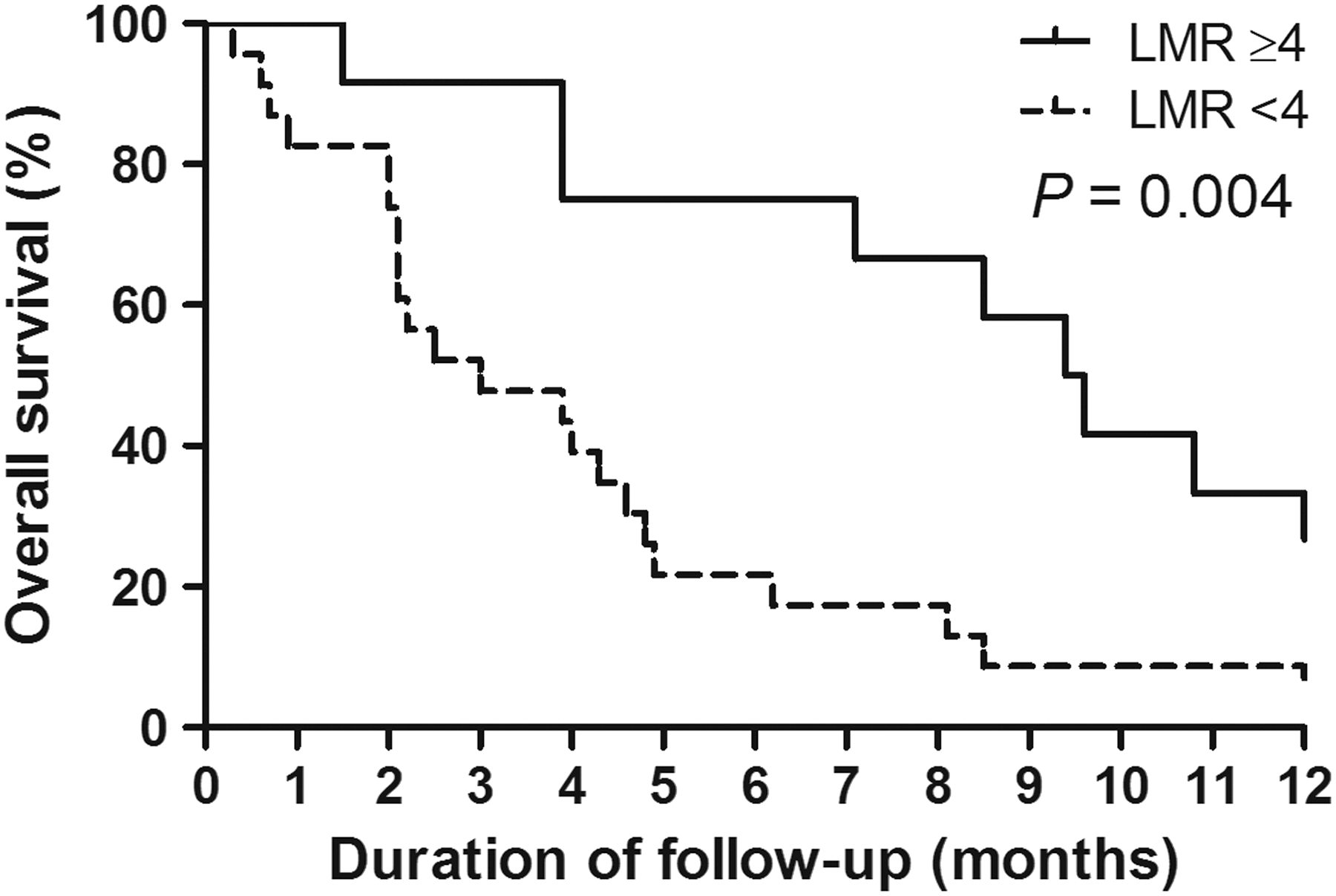
Overall survival (OS) based on the lymphocyte-to-monocyte ratio (LMR) in patients with anaplastic thyroid carcinoma. The solid line represents the OS rate of the high LMR group (≥4; n = 12; 34%), while the dotted line represents the OS rate of the low LMR group (<4; n = 23; 66%). A significant difference was found in the OS between the two groups (p = 0.004).
Cox Proportional Hazards Model of All-Cause Mortality in Patients with ATC
HR, hazard ratio; CI, confidence interval.
Discussion
The present study evaluated the role of the LMR as a prognostic marker for ATC. The LMR values between the baseline and follow-up CBCs were not significantly different. These findings suggested that the LMR is a stable marker indicating host immunity. When the patients were classified into two groups based on their LMRs, the OS of the low LMR group was significantly lower than that of the high LMR group. A low LMR was an independent risk factor for all-cause mortality in patients with ATC after adjusting for sex, tumor size, and distant metastasis.
The host immune function is important in the destruction or growth of cancer cells; it can destroy tumor cells, but may also facilitate tumor growth by establishing a tumor-favorable microenvironment (1,6). Lymphocytes and TILs play an important role in antitumor effects (26 –29). Absolute lymphopenia produces an insufficient immune response against a tumor (4). In contrast to the function of lymphocytes, increased monocytes are associated with poor prognosis in hematologic and solid tumors (6,30,31), as are increased TAMs derived from monocytes (12,32,33). In previous studies, the total ATC tumor volume consisted of 50% TAMs, and an increased number of TAMs was associated with poor OS in ATC (18,19,34). Because a low LMR with a high absolute monocyte count may reflect the increased infiltration of TAMs into tumors, the present results are consistent with previous studies that suggested the prognostic role of TAMs in ATCs. The present findings indicate that the LMR can be a simple prognostic biomarker reflecting the host immune function and TAM infiltration in ATC. However, further prospective pathologic analysis evaluating real TAM infiltration in association with the LMR is needed to validate the findings.
Immunotherapy based on cancer immunoediting has been recognized as an area of treatment for advanced or chemotherapy-resistant cancers. In advanced differentiated thyroid carcinomas or ATC, the possibility of immunotherapy has also emerged as a new treatment. However, the exact mechanism is not clearly elucidated (2,35). The present findings support the important role of TAMs in the progression of ATC, and suggest that immunologic therapies modulating the function of TAMs may be helpful in the treatment of ATC. One study reported that colony-stimulating factor 1 (CSF1)/CSF1 receptor (CSF1R) signaling plays an important role in the function of TAMs, and the depletion of CSF1 reduced TAM infiltration and induced more differentiated and smaller PTCs (36,37).
The present study has some limitations that must be considered. First, ATC accounts for <2–3% of all thyroid cancers (17), and the total number of subjects included in the study is small. Thus, this study has the nature of a pilot study that requires validation. Second, the possibility of selection bias should be considered because this was a single-center retrospective study. Third, baseline and follow-up CBCs were not regularly performed. Because CBCs can be easily performed but can also change in response to other situations such as infection and nutrition, CBCs should be cautiously interpreted. Finally, this study is limited due to its retrospective nature. Moreover, the available tissue specimens were insufficient to perform additional immunohistochemical staining. Therefore, the presence and proportion of TAM infiltration in ATC between the low and high LMR groups were not evaluated in this study. Fluorescence-activated cell sorting analyses evaluating T-cell subtypes could not be evaluated. Despite these limitations, the results of the present study are important because to the best of the authors' knowledge, this is the first study to evaluate the association between the LMR and OS of patients with ATC.
In summary, a low LMR is associated with poor survival in patients with ATC. This study results suggest a role for the LMR as a simple and readily available prognostic biomarker reflecting the host immune function for predicting the OS of patients with ATC. Further studies are needed to clarify the relationship between the LMR and TAM infiltration in ATC.
Footnotes
Acknowledgments
This study was supported by the National Research Foundation (NRF) of Korea Research Grants (NRF-2017R1D1A1B03028231 and NRF-2018R1D1A1A02085395).
Author Disclosure Statement
No competing financial interests exist.