
Abstract
Background:
Radioiodine scanning may help risk stratify patients with differentiated thyroid carcinoma (DTC) during initial and subsequent restaging. To maximize the information obtained from radioiodine scanning, image quality and interpretation should be optimized. However, not all radioiodine scans are performed equally. This illustrated article reviews seven techniques that may significantly improve the information obtained from a radioiodine scan in patients with DTC, which in turn may alter management such as showing regional or distant metastases that were otherwise unknown and/or help classify whether a metastasis is radioiodine avid.
Summary:
The first of the techniques is spot imaging of anatomical areas of interest using a gamma camera with a parallel-hole collimator. Spot images typically provide superior spatial resolution and enhanced lesion detection compared with whole-body scans using the same equipment. The second technique is spot imaging of the thyroid bed and neck with a pin-hole collimator, further improving spatial resolution. Two other techniques, delayed image acquisition and longer acquisition time, may clarify the nature of indeterminate foci of uptake or areas with negative initial findings. Delayed image acquisition may increase tumor-to-background ratio and thus improves lesion detectability. Longer acquisition times also increase contrast resolution between lesions and background activity, again increasing the detectability of malignant lesions. The fifth technique, adjustment of image brightness/contrast on film or on the computer screen, may reveal previously unobserved subtle differences in counts. The sixth technique, focus-specific history, comprises additional patient information that is specific to a focus of radioiodine uptake and elicited by the nuclear medicine physician or technologist. The goal is to help determine if the focus represents a metastasis or an artifact, which in turn decreases false positives and increases specificity. The seventh technique, single-photon emission computed tomography/computed tomography, improves contrast resolution and helps localize foci of uptake to anatomical structures.
Conclusions:
Technique is important to maximize information obtained from radioiodine scans in patients with DTC. With the greater usage and understanding of these seven techniques, physicians will significantly improve the information obtained from a radioiodine scan in patients with DTC, which in turn may alter management and potentially outcomes.
Introduction
Radioiodine scanning is a valuable, although controversial, diagnostic tool for imaging differentiated thyroid cancer (DTC), and other publications have discussed the related controversies in detail (1 –4). Those who argue that radioiodine scans have little to no value infrequently discuss the techniques used to acquire their scans. This illustrated article reviews seven techniques that may significantly improve the information obtained from a radioiodine scan in patients with DTC (Table 1), and this information may show findings that may alter management such as showing regional or distant metastases that were otherwise unknown, and/or help classify whether a known metastasis of DTC is radioiodine avid. Of note, none of these techniques is original to this author, but all the techniques apply to most or all of the following types of radioiodine scans: (i) staging scans performed after the patient's initial surgery but before the first 131I therapy; (ii) post-therapy scans performed 3–7 days after 131I therapy; (iii) baseline scans or follow-up surveillance scans performed 6–18 months after the initial 131I therapy; and (iv) restaging scans performed when DTC recurrence or progression is suspected. Generally, these techniques pertain to both 123I and 131I imaging. A glossary of key terminology appears in Table 2. More in-depth discussions of the techniques are available in the Supplementary Data and previous publications (5,6).
Seven Imaging Techniques Used in the Evaluation of Patients with Differentiated Thyroid Cancer
SPECT, single-photon emission computed tomography.
Glossary
Technique 1: Spot Images
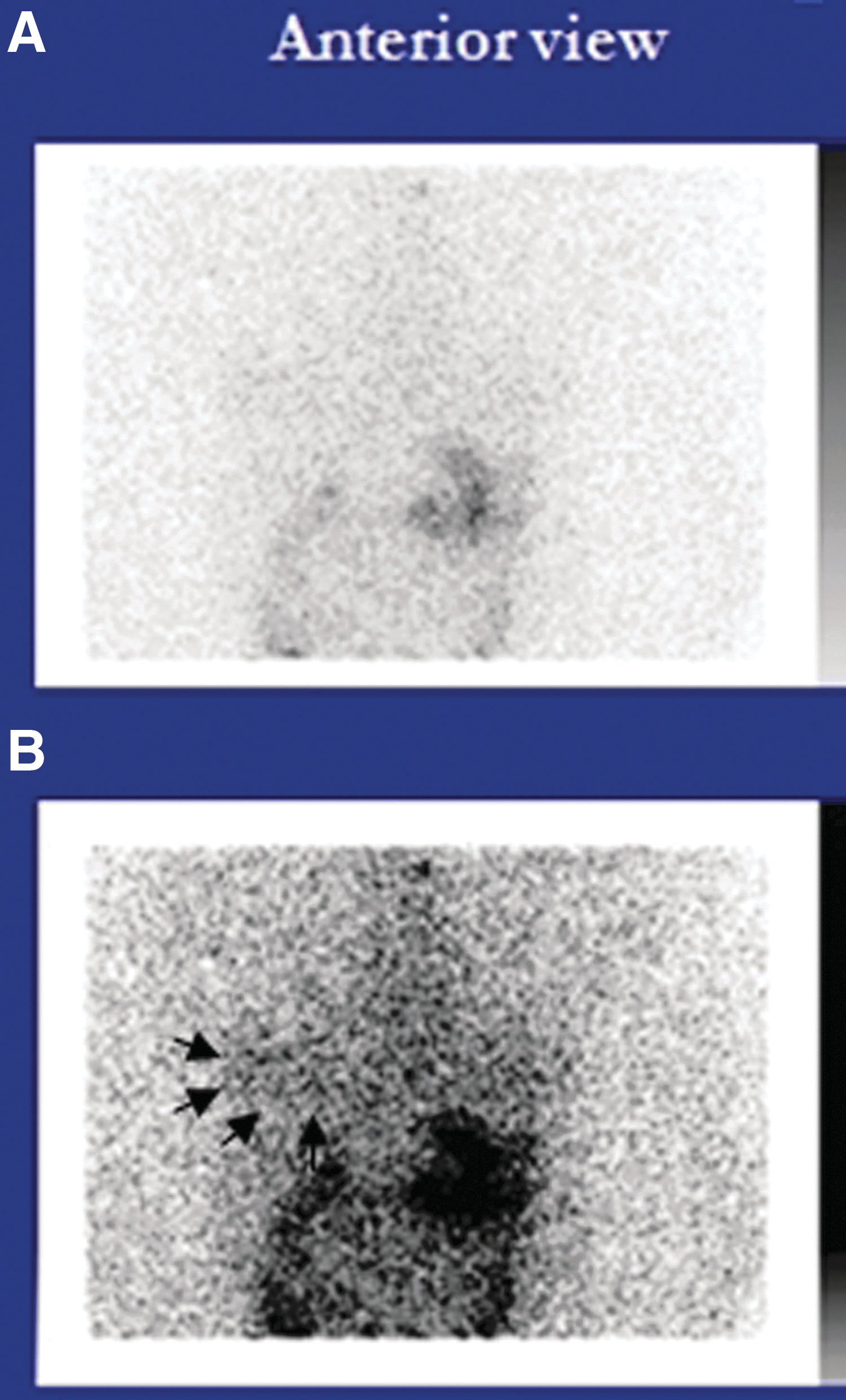
Figure 1 demonstrates the superiority of a “spot” camera image of the thyroid bed versus a whole-body scan (WBS) of the same area.
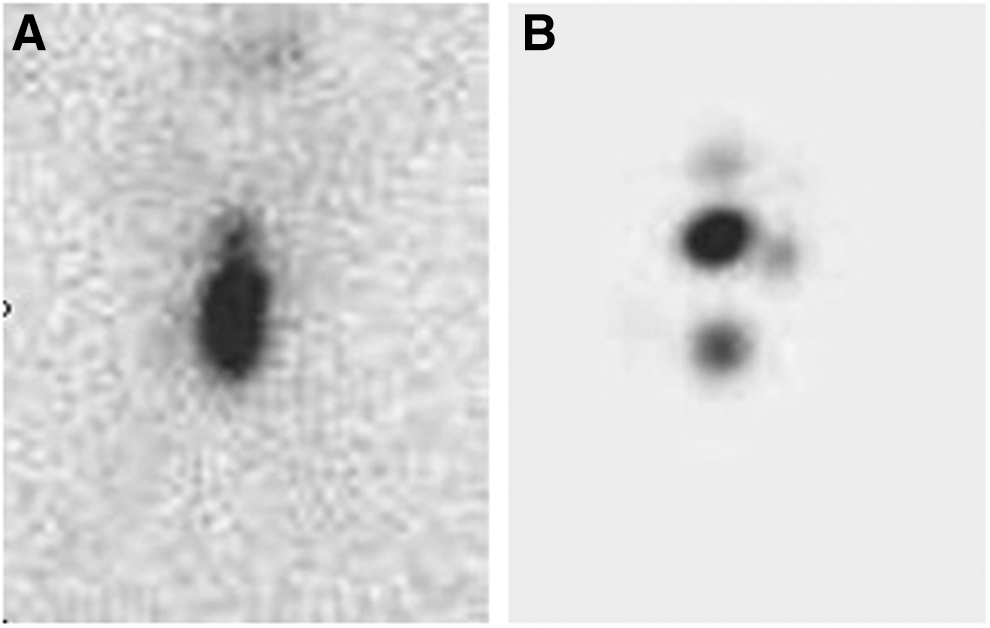
Whole-body image versus a “spot” image. (
A standard radioiodine imaging technique in DTC is WBS (5). A WBS is typically performed with a single-headed or dual-headed camera (Fig. 2) with a parallel-hole collimator (see Supplementary Fig. S1 in the Technique 1: Spot Images section of the Supplementary Data). The dual-headed gamma camera has one camera head above and the other camera head below the patient. To obtain a WBS, the table moves the patient or the two camera heads move simultaneously and continuously from the patient's head typically down to the patient's mid-thighs or the lower half of the lower extremities. The continuous sweeping and imaging of a WBS circumvents repeatedly repositioning the camera to obtain images of the whole body, thereby significantly reducing work for the technologist. This continuous imaging also eliminates the additional time associated with acquisition of multiple spot images (i.e., the time waiting for camera repositioning for each sequential view).

Typical dual-headed gamma camera. (Reproduced with permission from Keystone Press, Inc.)
For a “spot” image, the same camera typically using the same collimator or even a collimator with superior resolution is positioned over the area to be imaged. The camera remains stationary throughout the entire image acquisition. When stationary, the camera is frequently closer to the patient, which enhances spatial resolution. Additionally, when the camera is moving or the table is moving the patient, the camera–computer software must integrate all the counts being accumulated into a single whole-body images, and the software must account for the motion of the camera head or the patient. Although this software has improved significantly over the years, Kulkarni et al. (7) have shown that spot images have superior spatial resolution relative to whole-body images. A more technical discussion is available in Supplementary Figure S2 in the Technique 1: Spot Images section of the Supplementary Data.
Thus, to obtain superior thyroid bed and neck images, the Society of Nuclear Medicine guidelines recommend obtaining a spot view of areas of interest (8).
Technique 2: “Pin-hole” Collimator Spot Images
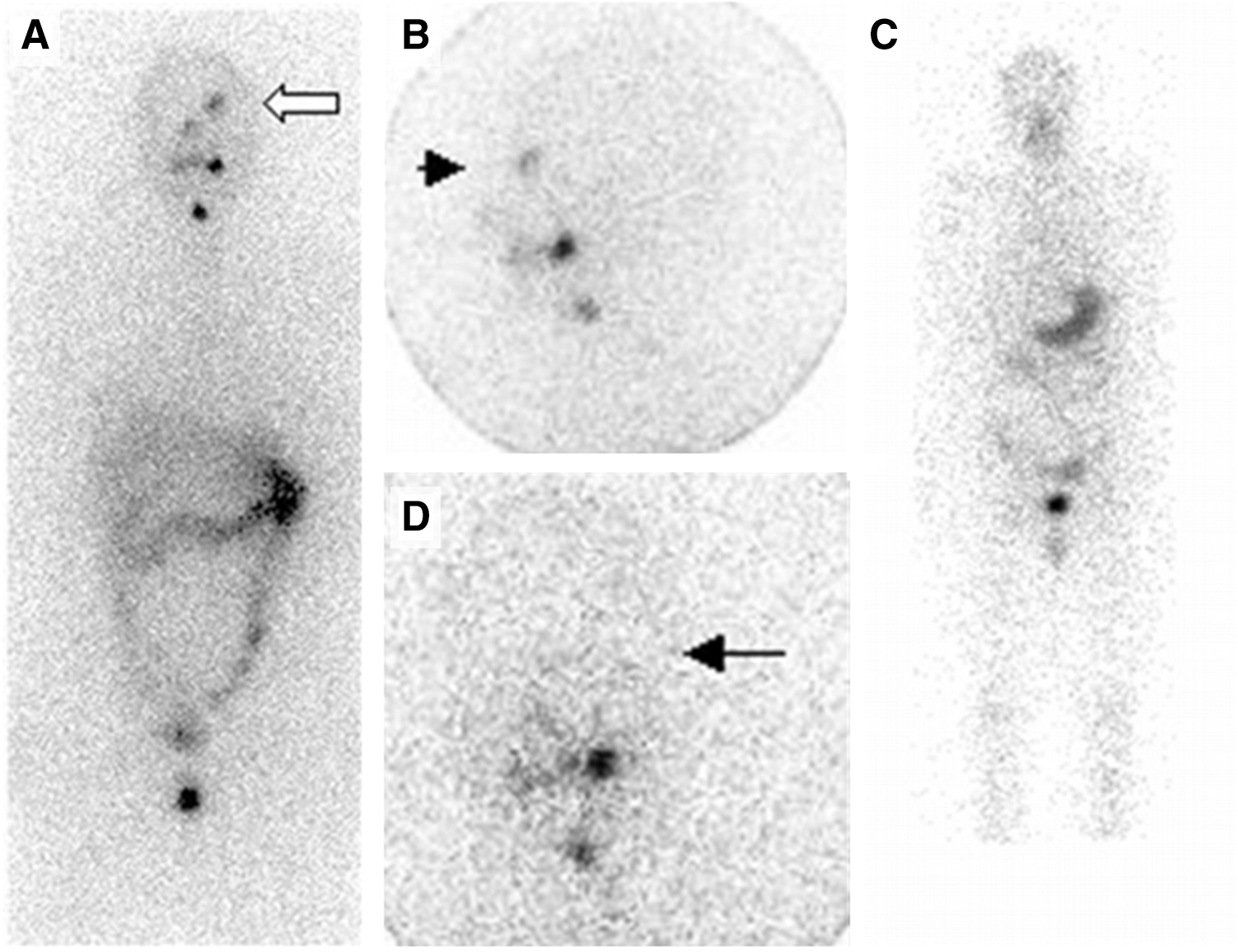
Figure 3A demonstrates a WBS, and Figure 3B is an image of the thyroid bed obtained using a pin-hole collimator immediately after the WBS. Figure 4 shows a camera using a pin-hole collimator, which is funnel shaped and offers even higher resolution of the thyroid bed and neck than images obtained with a parallel-hole collimator. Figure 5A and B shows the same images from Figure 1A and B along with the image obtained subsequently using the pin-hole collimator in the same patient (Fig. 1C).
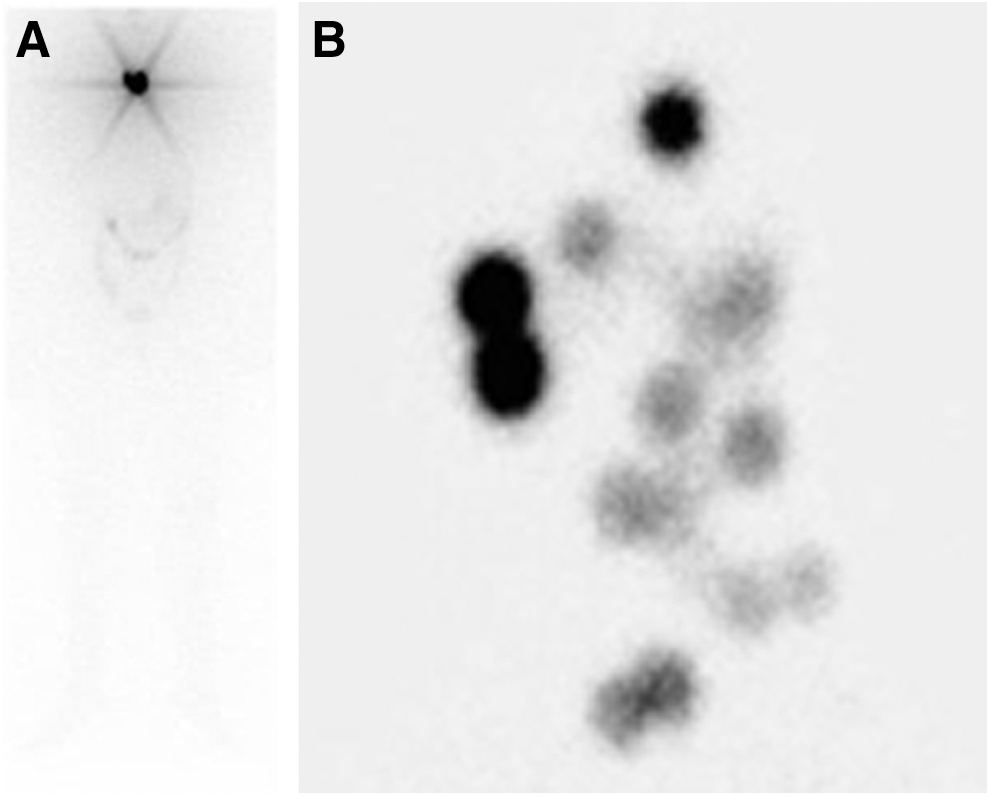
Whole-body image versus a “pin-hole collimator” image. (

Single-headed gamma camera with pin-hole collimator. (Reproduced with permission from Keystone Press, Inc.)
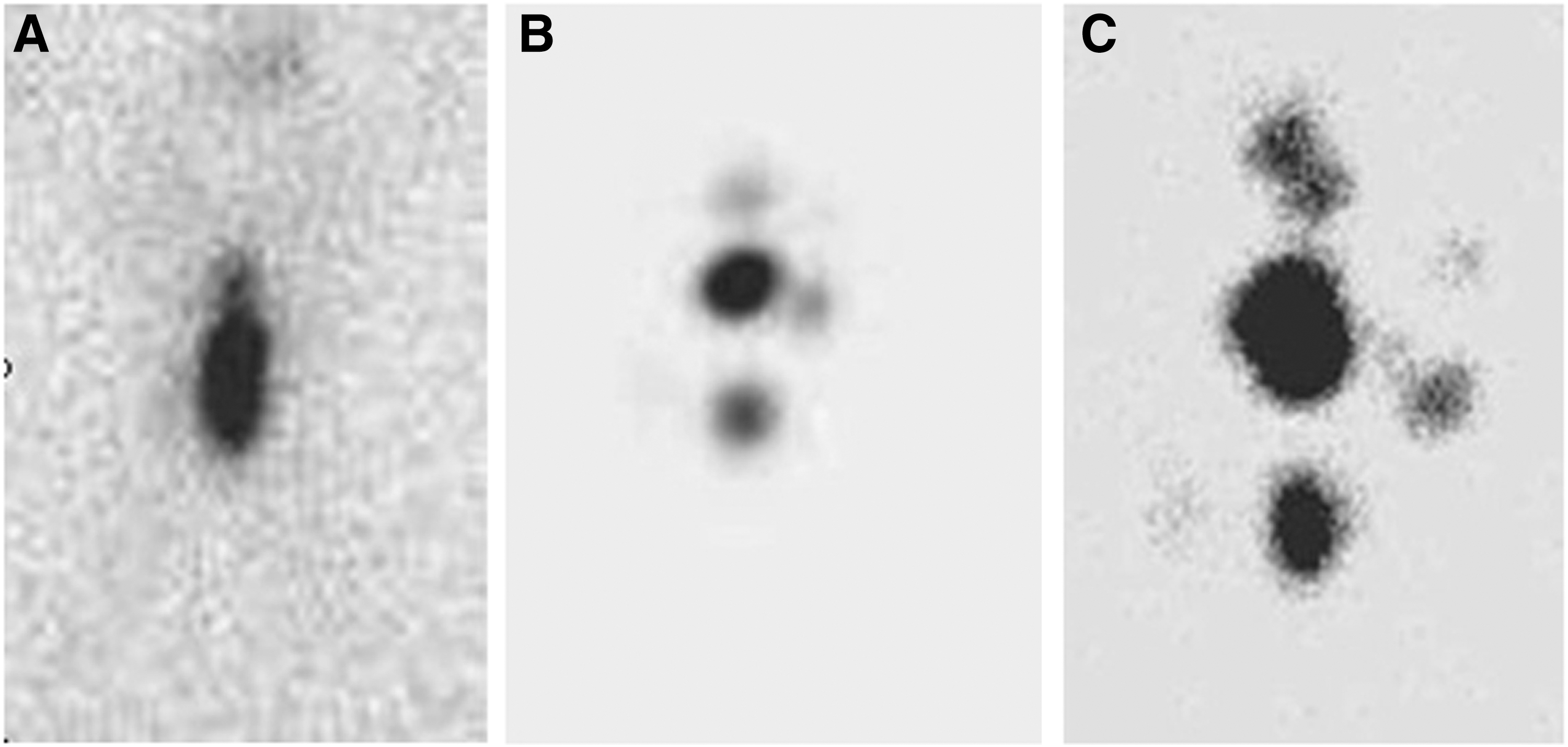
Comparison of the three types of images: whole body versus “spot” parallel-hole collimator versus “pin-hole” collimator. The first two images (
The pin-hole collimator has a single hole with side walls that are much thicker than those of a multi-hole parallel-hole collimator. Thus, the imaging characteristics of a pin-hole collimator differ distinctly from those of a parallel-hole collimator. Typically, images using a pin-hole collimator result in superior spatial resolution, and depending on the distance of the surface of the pin-hole collimator from the area of interest, the images may be magnified. One important advantage of a pin-hole collimator image is that it does not result in a “star artifact” that is frequently seen not only in a whole-body image but also in a “spot” image using a parallel-hole collimator. A discussion of a “star” artifact and other aspect of a pin-hole collimator are beyond the scope of this text. However, a more technical discussion is available in Supplementary Figures S3–S5 in the Technique 2: “Pin-hole” Collimator Spot Images section of the Supplementary Data, and further reading on pin-hole collimators are available (9 –11).
In regard to the utility of better determining the number and location of radioiodine-avid foci within the thyroid bed or neck, pin-hole collimator images allow at least two distinct advantages that may alter management. First, radioiodine uptake localized to the central or lateral compartment rather than the thyroid bed may prompt re-evaluation of the neck with ultrasound or further evaluation with single-photon emission computed tomography/computed tomography (SPECT/CT). Of note, SPECT/CT images are typically superior to pin-hole collimator images in localizing the radioiodine uptake to normal thyroid remnant tissue versus a lymph node or other structures. However, and despite the spatial resolution of newer SPECT/CT cameras improving, images obtained with a pin-hole collimator may still offer higher spatial resolution.
Second, when the number of foci identified on a pin-hole collimator spot image exceeds the “expected” number of foci that finding raises the possibility that the additional foci represent local metastases. That observation in turn may change the subsequent management, for example, by opting for additional surgery. The “expected” number of foci of uptake for a given surgeon was evaluated by Kulkarni et al. (12) at the MedStar Washington Hospital Center. They evaluated the spectrum of how many foci of uptake were visualized on radioiodine pin-hole collimator images after four high-volume surgeons performed a near-total or total thyroidectomy in patients with a low likelihood of locoregional disease. The number of foci visualized was classified as the “expected” number of foci for the surgeon. This is discussed in more detail in Supplementary Table S1 in the Technique 2: “Pin-hole” Collimator Spot Images section of the Supplementary Data.
In summary, performing radioiodine scans with additional pin-hole collimator images of the thyroid bed and neck could identify additional useful information that may alter management.
Technique 3: Delayed Imaging
Figure 6 demonstrates the superiority of acquiring “delayed” images. This term means repeating imaging after a longer time interval from administration of the radioiodine to the initiation of the image acquisition. Delayed imaging usually results in further clearance of both tumor radioactivity and background radioactivity. However, typically, radioactivity clears more rapidly from the “background tissue” than from the radioiodine-avid malignant thyroid tissue. When the background radioactivity clears faster than in the tumor, the ratio of tumor-to-background radioactivity increases. In turn, the contrast between the tumor and background increases, and the tumor may be visualized for the first time or an equivocal area of abnormal uptake may become clearly visualized. This phenomenon is akin to stargazing in the night sky; one will observe more stars in the countryside, where skies appear blacker, than in the city where light “pollution” dominates the skies. Similar to distinguishing the stars in the countryside, delayed imaging of DTC tumors generally offers better contrast resolution and can be valuable in detecting additional lesions. For further discussion of contrast versus spatial resolution, see Supplementary Fig. S6 in the Technique 3: Delayed Imaging section of the Supplementary Data. This technique of delaying acquisition of images from the time of administration of the radioiodine is especially important in demonstrating radioiodine-avid metastatic disease that might have otherwise been assumed to be radioiodine non-avid and hence potentially radioiodine refractory metastatic DTC (13).
Value of delayed acquisition. (
Technique 4: Longer Imaging Acquisition Time
Longer acquisition time simply means that the length of the time to acquire the image is longer, and like delayed images, this technique improves contrast resolution. Visually, the results are similar to those shown in Figure 6, and this is a result of improved counting statistics, which is beyond the scope of this text. However, a more technical discussion is presented in Supplementary Table S2 and Supplementary Figure S7 in the Technique 4: Longer Acquisition Time section of the Supplementary Data. As for delayed imaging, longer acquisition times potentially allow one to clarify an indeterminate focus of radioiodine uptake or visualizing an abnormal area of radioiodine uptake not previously seen, and both may alter management significantly, and potentially outcomes. Examples of altered management from these various techniques are listed in Table 3.
Examples of Enhanced-Imaging Techniques Altering Management
See Figures 1, 3, and 5, or the sections entitled “Spot Images” and “‘Pinhole Collimator’ Spot Images.”
FNA, fine needle aspiration; TSH, thyrotropin.
Technique 5: Adjusting Brightness, Contrast, or Both
All radioiodine images, whether on film or computer screen, can be adjusted for brightness/contrast. These two terms are used together in this article because the mechanism for the adjustment of brightness/contrast can vary significantly depending on the specifications used to produce those images and the display station used. Adjustments of brightness/contrast may help the interpreter identify subtle differences in counts that otherwise may have been missed. An example is shown in Figure 7. However, the interpreter and anyone else reviewing the scans must be cautious in interpreting images adjusted for brightness/contrast. A faint area of activity that is not clinically significant could be adjusted to be made to appear to have significant and even marked uptake. Nevertheless, this technique can significantly aid the interpreter.
Value of adjusting brightness, contrast, or both. (
Technique 6: Focus-Specific History
Planar radioiodine scans have poor specificity, so that focal areas of uptake on such images may frequently be false positive for DTC metastases. Shapiro et al. (14) published an excellent article on the wide spectrum of etiologies of false-positive radioiodine scans, which also has been updated (15).
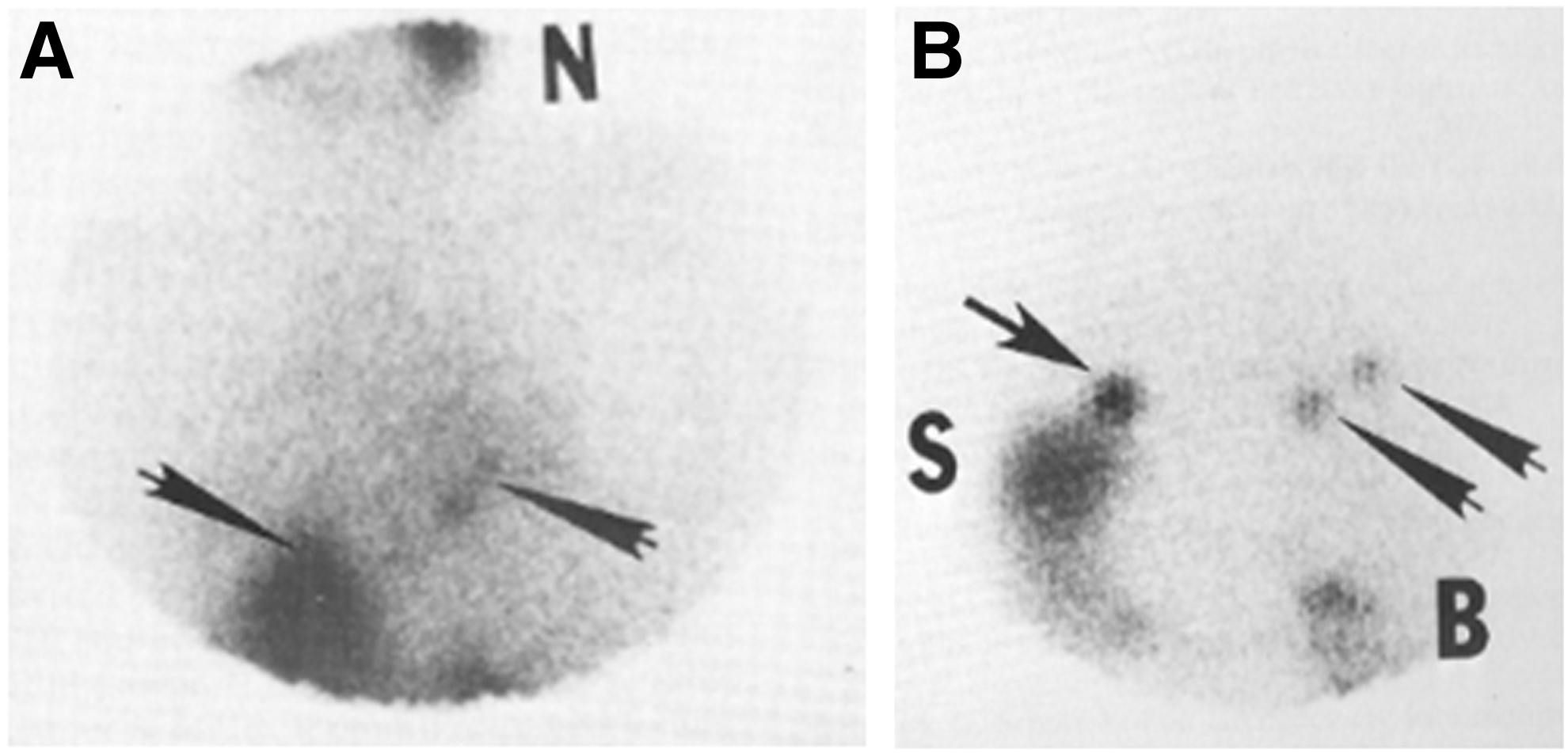
A focus-specific history consists of additional patient history obtained after the review of the initial routine images by the nuclear medicine physician or technologist and addresses a suspicious focal area of radioiodine uptake. The goal is to help determine whether an indeterminate focus of radioiodine uptake represents either a metastasis or an artifact. Frequently, after eliciting the focus-specific history, the physician obtains additional spot images to verify the suspected etiology of the focus. An excellent example of the value of a focus-specific history is shown in Figure 8. Although SPECT/CT imaging is one of the major advances in nuclear medicine to significantly improve the specificity of radioiodine scans and reduce the false-positive rate, obtaining “focus-specific” history remains an important technique for the interpreter of radioiodine scans.
Utility of a focus-specific history. (
Technique 7: SPECT/CT
One of the most valuable techniques, if not the most valuable technique, for imaging radioiodine uptake in patients with DTC is SPECT/CT, which provides three-dimensional tomographic images instead of two-dimensional planar images. Compared with planar scintigraphy, this modality improves contrast resolution and helps localize focal areas of radioiodine uptake to anatomical structures (Fig. 9). As a result, SPECT/CT significantly reduces false-positive radioiodine scans. Although it is beyond the scope of this article to discuss in depth how SPECT/CT is performed and the various factors affecting the quality of SPECT/CT imaging itself, the literature is summarized below and in Table 4 showing that SPECT/CT clearly enhances radioiodine image quality, thereby altering disease management and, potentially, patient outcomes. Examples of altered management are again noted in Table 3.
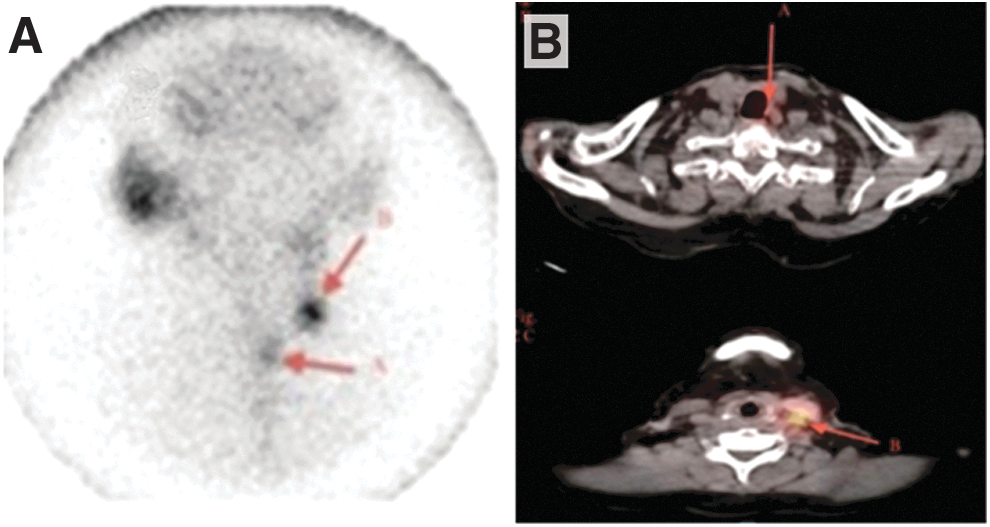
Value of SPECT/CT. (
Literature Supporting the Utility of Pre-therapy Single-Photon Emission Computed Tomography/Computed Tomography Radioiodine Scans in Patients with Differentiated Thyroid Cancer
Utility of Planar and SPECT Radioiodine Imaging
Several articles have demonstrated the utility of pre-131I therapy staging scans with planar imaging (2,16). For example, using 123I with imaging 24 hours after administration in 122 patients, Chen et al. (16) reported that pre-therapy radioiodine staging planar scans without SPECT provided additional critical information in 25% of cases. When patients had >3% uptake in the area of midline lymph nodes, the pre-therapy planar scan provided additional information in 50% of cases. Van Nostrand et al. (2) also evaluated pre-therapy planar staging scans performed with 123I and imaging 24 hours after radioiodine administration. Patients who had suspicious lymph nodes on physical examination or ultrasound, lymph nodes histologically positive for metastases, or any findings raising the possibility of distant metastases were excluded. In 29% of the 355 patients, pre-therapy radioiodine staging scans provided additional information that may have altered management with the objective of improving outcomes.
Multiple articles have reported the utility of SPECT radioiodine imaging (17 –32) changing management in 20–88% of patients (Table 4), and further reading is available (33,34). Again, examples of altered management are noted in Table 3. In short, the literature supports the utility of planar and SPECT radioiodine scans in altering management in a large proportion of patients with DTC.
The future
The future holds significant promise of further improving radioiodine imaging techniques for patients with DTC. Manufacturers are continually upgrading SPECT/CT cameras. Multiple organizations are evaluating and pursuing regulatory approval of the positron emission tomography radioisotope, 124I (35), and multiple pharmaceutical firms and facilities are evaluating agents that upregulate sodium–iodide symporter gene expression and function (36). These efforts hold significant promise to improve further the quality of radioiodine imaging.
Summary
In summary, planar and SPECT radioiodine scans have significant value postoperatively, after therapy with radioiodine, and in the follow-up in assessing patients with DTC. To maximize the information obtained from these images for these patients, technique is important, and not all radioiodine scans are performed equally. With the greater usage and understanding of these seven techniques, physicians will significantly improve the information obtained from a radioiodine scan in patients with DTC, which in turn may alter management and potentially outcomes.
Footnotes
Acknowledgments
I would like to thank Robert Marlowe, an independent medical editor, for critically reviewing, copy-editing, and formatting this article, and Sanofi Genzyme for supporting Mr. Marlowe's efforts, as well as reimbursing fees associated with publication of this article. However, I initiated this article and had sole responsibility and control regarding its content and regarding all decisions pertaining to its submission. I received no remuneration for writing this article.
Author Disclosure Statement
D.V.N. is a speaker and consultant to Jubilant Draximage.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2