
Abstract
Background:
Severe pretibial myxedema (PTM) can be difficult to manage, highlighting the need to investigate newer therapies. Rituximab (RTX) and intravenous immunoglobulin (IVIg) have been tried in Graves' orbitopathy. Since PTM and orbitopathy share a similar underlying pathophysiology, this study aimed to explore these therapies for progressive PTM.
Methods:
The electronic database was screened for PTM patients evaluated at the Mayo Clinic, Rochester, from 2002 to 2016, and three patients who received IVIg and five who received RTX are reported. PTM pattern was classified as non-pitting edema, plaque and induration, nodular/nummular, and elephantiasis. PTM was confirmed by biopsy in six patients.
Results:
The patients' median age was 53.8 years, 75% were female, and all but one patient were either active or former smokers. All patients were euthyroid and had progressed despite various therapies prior to starting these agents. Six patients had a plaque and induration pattern, and two had a nodular pattern with elephantiasis. After therapy, six (75%) patients had PTM stability or improvement both subjectively and objectively (80% with RTX and 66% with IVIg). The three patients (one in the IVIg group and two in the RTX group) who had subjective improvement had a plaque pattern. One patient with elephantiasis had a transient response to IVIg and another had stability after RTX. Thyrotropin receptor antibody values and orbitopathy also improved in patients who demonstrated PTM improvement. No serious adverse events were reported, but one patient each had transient hypertension and injection-site thrombophlebitis after IVIg.
Conclusions:
Immunomodulation therapy was followed by PTM improvement or stability in most patients, with a slightly better response after RTX compared to IVIg. A validated response assessment instrument and larger series of patients are required to determine if the underlying disease process could be curtailed with these agents.
Introduction
Graves' dermopathy is a rare extrathyroidal manifestation of Graves' disease (1). It occurs most often in association with Graves' orbitopathy (GO) (2,3), though rarely it can be the first manifestation of the Graves' disease triad (4 –7). Graves' dermopathy typically localizes in the pretibial region. Hence, it is also known as pretibial myxedema (PTM). It can also involve the knees, elbows, neck, and other areas exposed to repeated pressure or trauma (3,8 –11). Orbital and pretibial fibroblasts express the thyrotropin (TSH) receptor (TSH-R) and insulin-line growth factor 1 receptor, and become targeted by TSH-R sensitized T cells and/or TSH-R antibodies (TRAb), leading to the inflammatory and infiltrative cascade of GO and PTM (12,13). The pathogenesis of PTM is characterized by fibroblast proliferation and glycosaminoglycan accumulation causing non-pitting edema, which leads to compression of dermal lymphatics and can progress to significant lymphedema (1). Almost all patients with these extrathyroidal manifestations of Graves' disease demonstrate high TRAb values, thought to explain the increased severity of their autoimmune phenomena (14,15).
As the spectrum of the PTM progresses from mild to severe forms such as elephantiasis, the likelihood of response to therapy decreases substantially (2,3). Standard PTM management includes minimizing risk factors (smoking, obesity), use of topical steroids (fluocinolone, triamcinolone), use of intra-lesional triamcinolone, compression bandages, and massage therapy for lymphedema. These therapies might help in mild cases but are not consistently successful in halting the progression of PTM. This highlights the need for investigating other management options, especially those that can potentially modify the underlying disease process. Two therapies deemed theoretically to have a high likelihood of response are intravenous immunoglobulin (IVIg) and rituximab (RTX).
Most of the available data for these agents comes from their use in GO. Because PTM and GO share a similar underlying pathophysiology, this study aimed to explore the role of these therapies in patients with progressive PTM. RTX is a humanized chimeric anti-CD20 monoclonal antibody that depletes both B lymphocytes in the intermediate stages of maturation and short-lived plasma cells. Since B lymphocytes act as antigen-presenting cells to T lymphocytes, it can be postulated that depleting them blocks the release of cytokines from T lymphocytes that would further mediate the cascade involved in the extrathyroidal manifestations of Graves' disease. IVIg depletes T lymphocytes (16) and has also been shown to contain antibodies against cross-reacting idiotypes. Use of these agents in GO and PTM patients opens up the avenue of immunomodulation as a management option. However, results thus far have been mixed (17 –19). Herein, the authors' experience with systemic immunomodulatory therapies with RTX and IVIg is described for severe PTM that had been unresponsive to standard therapy.
Methods
Case detection
After obtaining Mayo Clinic Institutional Review Board approval, the patient database was screened for all patients with PTM evaluated at the Mayo Clinic, Rochester, from January 1, 2002, through June 30, 2016, by searching for the terms “Graves' dermopathy,” “thyroid dermopathy,” and “pretibial myxedema.” All included patients had appropriate research authorization. In this 14-year period, 109 patients with PTM were evaluated, of whom eight had progressive disease (defined as either enlargement of lesions or worsening of associated symptoms, such as pain, burning, decreased mobility) despite standard therapy, and were treated with either IVIg or RTX. After case identification, PTM patterns were classified into one of four categories: non-pitting edema, plaque and induration, nodular/nummular, and elephantiasis.
Therapy regimen
Patients 1–3 were treated with monthly IVIg infusions, with a total dose of 2 g/kg split over three consecutive days for four to seven months. Of the five patients treated with RTX (patients 4–8), patients 4, 5, and 6 received 1 g infusions two weeks apart (rheumatoid arthritis [RA] protocol) and patients 7 and 8 received 375 mg/m2 infusions weekly for four weeks (lymphoma protocol).
Monitoring and potential confounding variables
The patients were evaluated approximately every three months to assess clinical response. Additionally, the patients' own opinion was sought for a subjective response, and the clinical response was compared to photographs taken prior to treatment. The duration of follow-up ranged from three months to one year after initiation of therapy. Clinical response was assessed as a subjective change in pain, tightness, numbness, joint mobility, ambulation, and functionality or an objective change in surface area involved, disease pattern, erythema, and circumference of the involved extremity. Categories for response were divided into objective and subjective “improvement,” “stability,” and “worsening.” Subjective (patient-reported) or objective (physician-reported) improvement and stability were considered as a positive response given patients' progressive disease up to that point, while subjective or objective worsening was considered as a negative response to therapy. Factors taken into account that could potentially influence the response to therapy were patient age, duration of PTM before therapy, previous or concurrent use of other therapies, pattern of PTM, extent of skin involvement, regimen of immunomodulation therapy, TRAb value, presence of GO or acropachy, and smoking status.
Evaluation of thyroid function and autoantibodies
Serum free thyroxine, total triiodothyronine, and TSH were measured directly by radio-immunometric assays developed by Roche Diagnostics (Indianapolis, IN). TRAb and TSH-binding inhibitor immunoglobulin (TBII) were measured by a third-generation competition-based assay. In some patients, this test was reported as percentage TBII (older assay; reference range <16%), while in others it was reported as IU/L (newer assay; reference range 0–1.75 IU/L). Thyroid-stimulating immunoglobulin (TSI) via bioassay (reference range ≤1.3) was also measured in two patients.
Statistical analysis
In this descriptive study, categorical variables are expressed as percentages. Continuous variables are expressed as median and range, as this is a small sample and the variables were not normally distributed.
Results
Baseline characteristics
The patients' median age at the start of therapy was 53.8 years, the majority were female (6/8), and all but one patient were either active or former smokers. All patients had hyperthyroidism in the past, but were clinically and biochemically euthyroid on levothyroxine replacement at the initiation of RTX and IVIg. They had elevated TRAb titers or a positive TSI index, and a history of active GO, and all had progressive PTM despite various combinations of prior therapies (topical steroids, intra-lesional steroids, oral steroids, pentoxifylline, and local physical therapy).
Distribution of the lesions
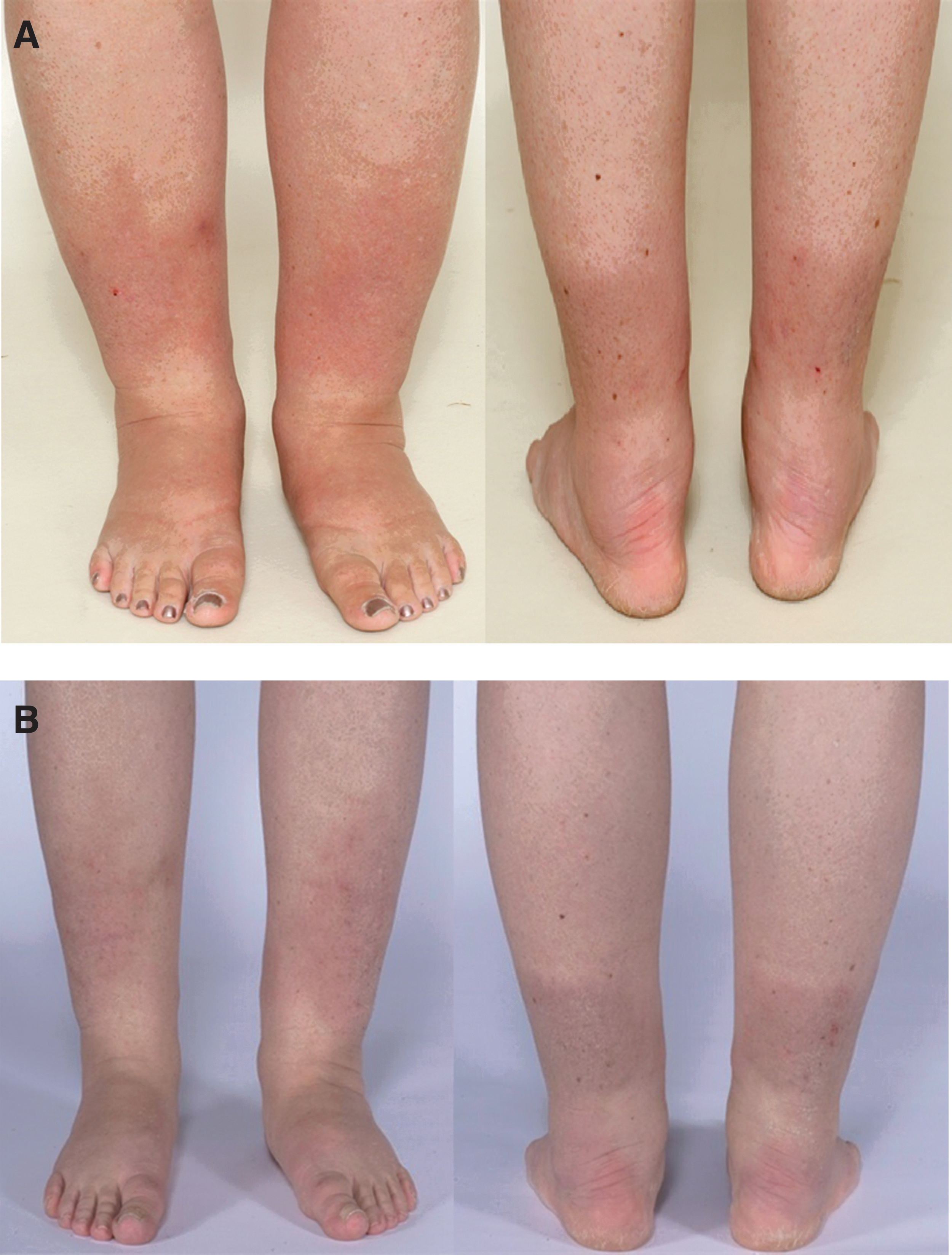
In addition to pretibial lesions, two patients also had involvement of the dorsum of the feet. One patient had plaque-like induration of the calf and thigh and non-pitting edema and thickening of the toes, almost appearing like elephantiasis of the toes (Fig. 1). Two patients presented with elephantiasis and nodular/nummular lesions, one of whom had the most extensive involvement (Fig. 2). All patients were evaluated by an endocrinologist and a dermatologist; six had confirmation of PTM by skin biopsy, shown for one of the patients in Figure 3A and B (compared to biopsy of normal skin; Fig. 3C). Other baseline characteristics are listed in Table 1.

Pretibial myxedema (PTM) before rituximab in patient 6 with plaque and induration of dorsum of bilateral feet along with non-pitting edema and thickening of the toes.

PTM before rituximab in patient 8 involving bilateral feet and legs with nummular/nodular and polypoid lesions along with elephantiasis.

(
Baseline Characteristics of Pretibial Myxedema Patients Prior to Therapy with Intravenous Immunoglobulin and Rituximab
Data are presented as median (range) or n (%).
PTM, pretibial myxedema.
Dermopathy response
Given the small numbers, patients whose disease stabilized or improved with RTX or IVIg were combined in the positive response group. As shown in Table 2, overall consistent subjective improvement occurred in three patients, two of whom also had an objective improvement. Subjective as well as objective stability occurred in three patients, while subjective as well as objective worsening occurred in two patients, although one of them had initial improvement. Among the three patients treated with IVIg, only one demonstrated subjective and objective improvement starting three months after the first infusion. A second patient demonstrated stability, and the third patient had eventual worsening after initial improvement following each infusion. Among the five patients treated with RTX, subjective improvement occurred in two patients, one of whom also had objective improvement after three months (Fig. 4A and B) and almost complete resolution of PTM after nine months (images were not available). There was subjective as well as objective stability in two other patients, and subjective as well as objective worsening in the fifth patient.
(
Pretibial Myxedema Response to Therapy Classified as Subjective (Patient-Reported) and Objective (Clinician-Documented) Improvement, Stability, and Worsening
Data are presented as n (%).
Initial improvement in one patient.
The response to therapy was also evaluated according to the pattern of PTM. Unfortunately, the pattern of disease was not able to predict the subjective response, and there was significant variability in terms of the improvement described by patients (Table 3). The three patients (one in the IVIg group and two in the RTX group) who had subjective improvement had a plaque pattern of PTM. Of note, one patient had almost complete resolution of erythema and plaque at the nine-month follow-up after the first RTX dose. However, one patient who had worsening of PTM despite RTX therapy (RA protocol) also had the plaque pattern with pretibial and toe involvement. One of the patients with elephantiasis initially had a transient response to IVIg, but then swelling recurred, and he was classified as “worsening” (the patient also became hypothyroid concomitantly, which might have influence the degree of edema). The other patient with elephantiasis and most severe polypoid PTM pattern was treated with RTX, and his disease stabilized despite disease progression prior to therapy. Objective response was described by physicians in terms of changes in surface area involved, erythema, degree of edema, and circumference, and is detailed in Table 3. Objective improvement or stability was seen in all the patients who reported some degree of subjective improvement.
Response to Therapy in Individual Patients
TRAb, thyrotropin receptor antibodies; TSI, thyroid stimulating immunoglobulin; GO, Graves’ orbitopathy; IVIg, intravenous immunoglobulin; RA, rheumatoid arthritis.
Change in thyroid function and autoantibodies
All patients were euthyroid at the start of therapy, and all but one remained so. This patient had elephantiasis and became significantly hypothyroid (TSH = 50 mIU/L) at the end of 5 cycles of IVIg. All the patients had a high TRAb titer or TSI index prior to initiating IVIg or RTX. In all those with subjective or objective improvement, antibody values (TRAb or TSI) also improved in that time period (Table 3). Among the three patients who had stability of PTM, the antibody values did not change in two patients but decreased in one patient. Among the two patients who had worsening of PTM, the antibody value did not change in the patient treated with RTX. However, TSI decreased slightly in the case that worsened after initial improvement with IVIg.
Response in other extrathyroidal manifestations
GO was present in all patients, and four had already undergone orbital decompression for moderate to severe GO. Their eye disease was inactive at the time of IVIg or RTX initiation and did not worsen or reactivate. GO improved in both patients who had subjective and objective improvement in PTM, and it actually resolved completely in the patient treated with IVIg. Acropachy was present in three patients, and this did not change after therapy.
Safety and tolerance of therapy
None of the patients reported any serious adverse events. In the IVIg group, one patient experienced transient hypertension that resolved spontaneously and another experienced injection-site thrombophlebitis that resolved as well. These adverse events were mild or Common Terminology Criteria for Adverse Events grade 1. None of the patients treated with RTX experienced any adverse events from the therapy.
Discussion
In the present study, eight patients with severe PTM are described who received immunomodulatory therapy. The patients were euthyroid but had elevated TRAb or TSI values and clinical manifestations of GO. Most importantly, all had progression of PTM despite various combinations of therapies. A composite of 75% patients had either improvement or stability of PTM while on immunotherapy. In the RTX group, this proportion was higher at 80% compared to the IVIg group at 66% (Table 2). Objective improvement or stability was demonstrated in all patients who reported some degree of subjective improvement.
IVIg has antigen-specific T-cell suppressive effect (16), and this immunomodulatory action has been used to treat several hematologic, rheumatologic, neurologic, and dermatologic conditions effectively (20). IVIg has also been shown to be equally effective and better tolerated than standard regimen oral prednisolone for active GO in a randomized study (21). However, its use for PTM has been minimally explored and yielded mixed results, with one case series showing marked improvement and even resolution of dermopathy (18), while another case with elephantiasis demonstrated no clinical benefit (22). In the present series, three patients received IVIg, with one each demonstrating improvement (subjective as well as objective), stability, and worsening. It is noteworthy that this latter patient did have initial improvement shortly after IVIg administration. The B-cell depleting effect of RTX has showed mixed results in GO (17,19,23), with a significant response in some studies (19,23), but not in one of two RCTs (17). To the authors' knowledge, RTX has not been reported for therapy of PTM. In the five patients treated with RTX in this series, improvement was noted in two patients (with one patient demonstrating resolution of PTM), in two patients the disease stabilized, and in one case it continued to worsen after therapy.
This study also aimed to evaluate whether a specific PTM pattern responded better to RTX or IVIg, but this aim was limited by the small number of patients in this study. In this series, the three patients demonstrating consistent subjective improvement had a plaque pattern of PTM. However, of the two patients who had worsening of PTM, one also had a plaque pattern, but it was more severe with some nodules, and the patient was also an active smoker. The two patients with severe elephantiasic PTM did not improve. The one treated with RTX demonstrated stabilization of PTM, while the one treated with IVIg had transient improvement immediately following each infusion but eventually worsened as he became hypothyroid. The study that reported IVIg use for PTM did not identify IVIg as inducing hypothyroidism (18). In that study, the only patient with severe elephantiasic PTM did respond after six cycles of IVIg (18), while another case report did not identify any improvement after six cycles of IVIg in the elephantiasic form (22). These data suggest that the response to IVIg for severe elephantiasic PTM is unpredictable, though the small numbers preclude a strong conclusion.
Time to subjective improvement in PTM after therapy initiation varied, but in general was within a few weeks. In the IVIg group, the earliest response was a transient one immediately after an infusion. Yet, consistent responses were seen three months after the first infusion. In the literature, the study that reported the use of IVIg in PTM (18) showed improvement occurring a few weeks after therapy initiation. In the RTX group, the earliest response was noted one month after the first infusion. The duration of disease prior to starting therapy is also likely to play a role. In clinical practice, investigational therapies such as IVIg and RTX are considered when patients have not responded to standard medical and local therapies. However, based on the use of RTX for GO (17,19), it could be postulated that the response might be better when instituted earlier in the course of the extrathyroidal manifestations of Graves' disease. The limited duration of benefit in most patients suggests the need for repeated infusions. The patient with elephantiasis and polypoid pattern continued to demonstrate improvement at six months and then the disease stabilized, suggesting requirement for either repeat RTX dose or another agent. Even though GO and PTM share a common pathogenesis, the phases of active inflammation followed by a chronic inactivity in the former has not been described in the latter. If that same disease paradigm applies to PTM, then theoretically immunomodulatory agents would have the most benefit when used in the active inflammatory phase, which would translate to an indication to use them earlier in the course of PTM. In the present patients, it was not possible to demonstrate a clear relationship between the duration of PTM before initiation of IVIg or RTX and response to therapy.
PTM is an autoimmune disorder mediated by the interaction between TRAb and/or TSH-R sensitized T-cells and the TSH-R on dermal fibroblasts (12,13). There is clear evidence of antibody values influencing the prognosis of GO (24), but the evidence is not that convincing for PTM. All patients in this study had high TRAb or TSI values prior to RTX and IVIg administration, and these decreased in all those who had subjective or objective improvement in PTM. An improvement in TRAb titers has also been shown in the cases that demonstrated PTM regression with IVIg (18). Unfortunately, the change in TRAb in GO patients treated with RTX was not impacted by the use of this immunomodulatory agent. Hence, these changes might be just a reflection of the underlying disease activity and not a therapeutic response (17,19). This should not preclude the use of TRAb for monitoring PTM where it might have a prognostic role, possibly independent of therapy.
Since the natural course of PTM is unpredictable, with spontaneous improvement occurring in up to 50% of cases especially when mild (1 –3), it is imperative to contrast that possibility with the potential adverse events associated with any new therapy. In our series, two patients experienced mild/grade 1 adverse events after IVIg, both of which resolved with conservative measures. RTX was well tolerated without any adverse events.
This case series does have a number of limitations. The small sample size limits the generalizability of the findings. A control group was did not enlisted due to the rarity of the disorder and the difficulty in finding patients with progressive disease of similar severity that were observed. The follow-up was of limited duration in some patients. Thus, it was not possible to assess the long-term impact of therapy. This is also a highly selected patient population with concern for referral bias to a tertiary care center. Finally, a standardized instrument for outcome assessment of PTM is lacking, but this is not limited to the patients in this study. In usual clinical practice, assessment of PTM does not incorporate well-defined clinical scoring criteria as opposed to GO. Some studies have used ultrasound in addition to clinical evaluation to assess response better, which might be a useful consideration. Using biopsy to assess response might be counterproductive, given the possibility of worsening of dermopathy from repeated local trauma. A combination of objective measurements (such as volume displacement and photographs) and functional assessments might provide a more comprehensive understanding of therapeutic efficacy.
To conclude, this study illustrates the clinical experience with RTX and IVIg as exploratory immunomodulatory therapies for severe PTM refractory to usual care. Following either therapy, most patients experienced either stabilization or improvement of PTM. A milder plaque pattern was associated with a better response. Overall, more patients treated with RTX had improvement or stability of PTM compared to IVIg. However, the small sample size and lack of a control group limit the ability to distinguish between therapy response and natural history of PTM. A validated response assessment instrument and a larger series of patients along with a control group are required to determine whether the disease process could be curtailed with these therapies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.