
Abstract
Background:
The most commonly reported symptom of hyperthyroidism is weight loss; successful treatment increases weight. Weight gain faced by patients with hyperthyroidism is widely considered a simple reaccumulation of premorbid weight, whereas many patients feel there is a significant weight “overshoot” attributable to the treatment. We aimed to establish if weight gain seen following treatment for hyperthyroidism represents replenishment of premorbid weight or “overshoot” beyond expected regain and, if there is excessive weight gain, whether this is associated with the applied treatment modality.
Methods:
We calculated the risk of becoming obese (body mass index [BMI] >30 kg/m2) following treatment for hyperthyroidism by comparing BMI of 1373 patients with overt hyperthyroidism seen in a secondary care setting with the age- and sex-matched background population (Health Survey for England, 2007–2009). Next, we investigated the effect of treatment with an antithyroid drug (ATD) alone in regard to ATD with radioactive iodine (131I) therapy. We modeled the longitudinal weight data in relation to the treatment pathway to thyroid function and the need for long-term thyroxine replacement.
Results:
During treatment of hyperthyroidism, men gained 8.0 kg (standard deviation ±7.5) and women 5.5 kg (±6.8). At discharge, there was a significantly increased risk of obesity in male (odds ratio = 1.7 [95% confidence interval 1.3–2.2], p < 0.001) and female (1.3, 1.2–1.5, p < 0.001) patients with hyperthyroidism compared with the background population. Treatment with 131I was associated with additional weight gain (0.6 kg, 0.4–0.8, p < 0.001), compared with ATD treatment alone. More weight gain was seen if serum thyrotropin (TSH) was markedly increased (TSH >10 mIU/L; 0.5 kg, 0.3–0.7, p < 0.001) or free thyroxine (fT4) was reduced (fT4 ≤ 10 pmol/L (0.8 ng/dL); 0.3 kg, 0.1–0.4, p < 0.001) during follow-up. Initiation of levothyroxine was associated with further weight gain (0.4 kg, 0.2–0.6, p < 0.001) and the predicted excess weight gain in 131I-induced hypothyroidism was 1.8 kg.
Conclusions:
Treatment for hyperthyroidism is associated with significant risks of becoming obese. 131I treatment and subsequent development of hypothyroidism were associated with small but significant amounts of excess weight gain compared with ATD alone. We advocate that the discussion over the weight “overshoot” risk forms part of the individualized treatment decision-making process.
Introduction
Hyperthyroidism, characterized by excess concentrations of circulating thyroid hormones, commonly presents with weight loss, often despite increased appetite and caloric intake (1). Weight regain may therefore be expected following normalization of thyroid function. However, it is not clear if this weight regain reflects the desirable replenishment of premorbid weight or an undesirable “overshoot” potentially contributing to increased risks of obesity. Since hyperthyroidism is a common condition, affecting 3% of women and 0.3% of men in the United Kingdom (2 –4), and is associated with increased morbidity and mortality (5,6), especially from cardiovascular causes, weight control in this group of patients is an important public health issue. At present, it is not clear whether treatment of hyperthyroidism is a risk factor for development of obesity; hence, no weight management interventions are routinely offered in clinical practice.
Three main modalities are used to treat hyperthyroidism—antithyroid drugs (ATDs), administration of radioactive iodine (131I), or thyroidectomy. While treatment with drugs is associated with higher recurrence rates, 131I and thyroidectomy most often result in hypothyroidism and the need for lifelong levothyroxine (LT4) replacement. Since no single treatment modality is obviously superior, guidelines recommend discussion of all therapeutic options between the patient and the clinician allowing final individualized shared decision-making (7,8). However, when treatment options are discussed, patients with hyperthyroidism frequently express concern that the administration of 131I will result in excessive weight gain, often determining that this is a less favored therapeutic option.
Several studies have indicated that the increased risk of mortality in hyperthyroidism is mitigated following induction of hypothyroidism with 131I and guidelines recommend that doses sufficient to induce hypothyroidism should be administered (8 –11). Some smaller studies (12) have proposed the initiation of LT4 replacement as an additional risk for becoming obese, a finding not confirmed by others (13). Importantly, higher body weight in patients treated with LT4 has been linked to reduced quality of life (14). There are no large studies that systematically assess the impact of the chosen treatment modality on weight changes in patients with hyperthyroidism.
We set out to determine whether treatment of hyperthyroidism is associated with increased risks of becoming obese in a large hospital cohort presenting with a first episode of overt hyperthyroidism to a single specialist clinic based on comparison with the age- and sex-matched English background population. We evaluated the extent of weight gain following treatment of hyperthyroidism and examined the influence of the treatment modality used (131I or ATDs), development of hypothyroidism, and biochemical control of hyperthyroidism, on the likelihood of weight gain.
Patients and Methods
We studied weight changes in patients registered in the Thyroid Clinic Database at the University Hospitals Birmingham NHS Foundation Trust. Data on all adult patients with newly diagnosed overt hyperthyroidism and treated with ATDs, administration of 131I, or a combination of both between 2000 and 2014 were extracted, allowing up to 36 months for follow-up (study period January 1, 2000, to June 30, 2017). Overt hyperthyroidism was defined as raised serum-free thyroxine (fT4) and/or free triiodothyronine (fT3) with undetectable serum thyrotropin (TSH). Further inclusion criteria encompassed a minimum duration of follow-up of 6 months and a minimum of four recorded weight measurements (with recording of clinic weights at presentation and discharge mandatory), a measurement of patients' height, and a confirmed successful outcome at discharge, which was defined as (i) normal serum TSH concentrations off any medication for at least 6 months following discontinuation of ATD or following 131I or (ii) start of LT4 replacement therapy for hypothyroidism. Patients treated with ATDs long term were excluded. From the cohort of 1604 eligible patients, we excluded those with transient hyperthyroidism due to thyroiditis (n = 30) and those with amiodarone-induced thyrotoxicosis (n = 22). In addition, we excluded patients with potentially unstable weight due to causes unrelated to hyperthyroidism: pregnancy or within 12 months postpartum (n = 123), or death during the study period (n = 56).
The final study cohort thus comprised 1373 patients, ages between 18 and 90 years. The project was approved and registered by the University Hospitals Birmingham NHS Foundation Trust (CARMS-11842).
Patients were categorized by simple clinical and immunological criteria into three diagnostic groups: Graves' disease, toxic nodular hyperthyroidism, and hyperthyroidism of indeterminate etiology. Graves' disease was defined as the presence of biochemical hyperthyroidism with at least two of the following characteristics: palpable diffuse goiter, significant titer (>1:100) of thyroid peroxidase, and/or presence of thyroid eye disease as previously described (1,11). In addition, 10% (139/1373) of patients had TSH-receptor antibodies (TRAb) measured following routine implementation of this assay (ELISA by Thermo Scientific B.R.A.H.M.S., Hennigsdorf, Germany) in April 2013 and TRAb titers >1 IU/L were considered indicative of Graves' disease. Toxic nodular hyperthyroidism was defined as hyperthyroidism in the presence of palpable nodular goiter. Patients who did not fulfill either of these criteria were categorized indeterminate, representing a mixed group with Graves' disease, toxic nodular hyperthyroidism, or both, the size of this group reflecting our policy of not performing routine radionuclide imaging in patients presenting with hyperthyroidism.
The following demographic factors were recorded at presentation: sex, age at diagnosis (divided into quartiles: 18–36 years, 37–47 years, 48–60 years, and 61–90 years), and height (m). Clinical data collected during initial examination comprised significant medical history, current drug therapy, and smoking status (current smoker/nonsmoker), as well as the presence, size, and type of goiter. Patients were requested to assess their weight change before presentation, categorized as weight loss, weight gain, or unchanged.
Weight (kg) was recorded at presentation and during each follow-up visit as part of our routine clinic protocol. Body mass index (BMI, kg/m2) was calculated and divided according to the International Classification (15) into underweight: <18.5 kg/m2; normal weight 18.5–25.0 kg/m2; overweight 25.1–30.0 kg/m2; and obese ≥30.1 kg/m2. The underweight and normal weight categories were combined and analyzed together due to the small number of underweight patients (44 at initial and 16 at discharge visit).
Laboratory measurements included serial concentrations of serum fT4 [reference range: 10–22 pmol/L (0.8–1.7 ng/dL)], TSH (0.30–4.50 mIU/L), and serum fT3 [3.5–6.5 pmol/L (0.23–0.42 ng/dL)] at presentation. The serum fT4 concentration at diagnosis (used as a marker of disease severity) was categorized into the following: 22.1–30.0, 30.1–40.0, 40.1–60.0, and ≥60.1 pmol/L (1.7–2.3, 2.3–3.1, 3.1–4.7, and ≥4.7 ng/dL). A fifth category was added to account for patients with triiodothyronine thyrotoxicosis [fT3 > 6.5 pmol/L (>0.42 ng/dL)] (n = 57), whose serum fT4 was within the reference range [≤22.0 pmol/L (≤1.7 ng/dL)]. Serum concentrations of fT4 during follow-up were categorized as follows: below normal [≤10.0 pmol/L (≤0.8 ng/dL)], normal [10.1–22.0 (0.8–1.7)], raised [22.1–30.0 (1.7–2.3)], high [30.1–40.0 (2.3–3.1)], and markedly high [≥40.1 (>3.1)]. Serial TSH concentrations were categorized as undetectable (≤0.10 mIU/L), low but detectable (0.11–0.30 mIU/L), normal (0.31–4.50), slightly raised (4.51–10.00), and markedly raised (≥10.01). Clinical measurements were censored at 36 months of follow-up irrespective of whether patients were discharged.
Treatment of hyperthyroidism
Patients were offered treatment with ATDs or with 131I according to local, national (16), and international (7) guidelines. Patients typically commenced a single dose of 20 mg carbimazole (CMZ) or twice-daily doses of 100 mg propylthiouracil (PTU). A dose titration regimen was used in all, with typical maintenance doses of 5–10 mg CMZ or 50–100 mg PTU daily. Patients were monitored every 6–8 weeks until control of hyperthyroidism and then every 3 months until discharge. Patients with Graves' disease who relapsed after a 12–18-month course of ATD were advised to undergo 131I therapy. Before 131I, patients received ATDs to control hyperthyroidism; ATD were stopped at least 1 week before 131I and not restarted sooner than 1 week after. Following 131I, patients were seen at 6–8-week intervals for a minimum of 6 months. They were discharged with no medication if thyroid function remained normal for at least 6 months (euthyroid outcome) or they were prescribed lifelong LT4 replacement once permanent hypothyroidism developed. Those remaining hyperthyroid six months after 131I were offered a second dose and if they declined, they were treated with ATD (11).
Background population
We compared patients' BMI (categorical and continuous) with background population data obtained from the Health Survey for England (HSE) (17). To account for the decreasing trend in the proportion of people with healthy BMI in England over the years, median years of presentation and discharge from the clinic were calculated, which were 2007 and 2009, respectively. We combined data from survey years 2007 to 2009, retrieving 22,726 records with valid BMI. To make data more comparable, we excluded survey participants younger than 18 years (n = 664) and older than 90 years (n = 53) and performed frequency matching (1:8) with no replacement based on sex and age categories defined for the patients. Altogether, data of 10,984 survey participants were used for comparison purposes. The methodology of HSE data collection is described elsewhere (18).
Statistical analyses
Demographic and clinical characteristics of the cohort are described using means and standard deviations (SDs) for continuous variables and counts and proportions for discrete variables. Statistical significance was set a priori at the 5% level.
Patients' and background population's BMI was compared as categorical and continuous measurements. Proportions were used to calculate odds ratios (ORs) as crude values and adjusted for smoking habit.
In longitudinal analysis of weight gain depending on treatment received, missing weight data were imputed as a mean of nearby points corrected for the time between the measurements. Missing self-reported weight change data before diagnosis were coded as a separate category. In cases of any other missing observations (smoking, goiter, and thyroid eye disease), an assumption of absence of the characteristics was made.
A generalized estimating equation linear model, which allowed for clustering within patients, was developed to investigate the relationship between weight and demographic and clinical measurements. Time-variant covariates entered into the model included duration of follow-up (months), serum fT4 and TSH concentration at each clinic visit, 131I treatment, and LT4 treatment. The model used an autoregressive working correlation matrix with robust standard errors. Our main variables of interest were those associated with treatment (131I with or without subsequent LT4 compared with ATDs only) and thyroid function control (serial fT4 and TSH). The remaining variables were treated as explanatory.
Due to the number of patients categorized as having hyperthyroidism of indeterminate etiology, the sensitivity of the findings was investigated by comparing model coefficients with and without those patients. A further sensitivity analysis was undertaken excluding patients with current oral or inhaled corticosteroid use (n = 26 patients) in view of well-documented effects of steroids on weight changes (19). The statistical analyses were performed in IBM SPSS Statistics (version 24).
Results
Characteristics of patient population
The baseline characteristics of 1373 patients in the cohort are presented in Table 1. Mean duration of follow-up was 23 (±8.6) months. Five hundred seventy-three patients received ATD only and 800 underwent treatment with 131I, which resulted in permanent hypothyroidism in 571 (78% of those undergoing 131I therapy).
Baseline Characteristics of 1373 Patients Presenting with Hyperthyroidism
Categorical data are presented as counts and proportions (%), and continuous data as means and SDs.
ATDs, antithyroid drugs; BMI, body mass index; fT4, free thyroxine; LT4, levothyroxine; SD, standard deviation.
Comparison of weight status in hyperthyroid cohort with the background population
The matched background population consisted of 10,984 participants surveyed between 2007 and 2009. The matching resulted in the same proportion of men to women (23% men and 77% women) and in similar age (49 [±16.4] vs. 48 [±16.4] years, respectively) of clinic patients compared with the background population. There was, however, a difference in smoking habits among men (32.7% male patients were smokers compared with 22.7% of the male background population, p < 0.001) but not among women (21.3% vs. 21.2%; p = 0.48).
At presentation, there were larger proportions of healthy/underweight male (46% vs. 30%, p < 0.001) and female patients (49% vs. 41%, p < 0.001) and smaller proportions of the obese compared with the background population (18% vs. 26%, p < 0.001 for men; 19% vs. 26%, p < 0.001 for women), likely reflecting the loss of weight before treatment for hyperthyroidism (Fig. 1, panel A).
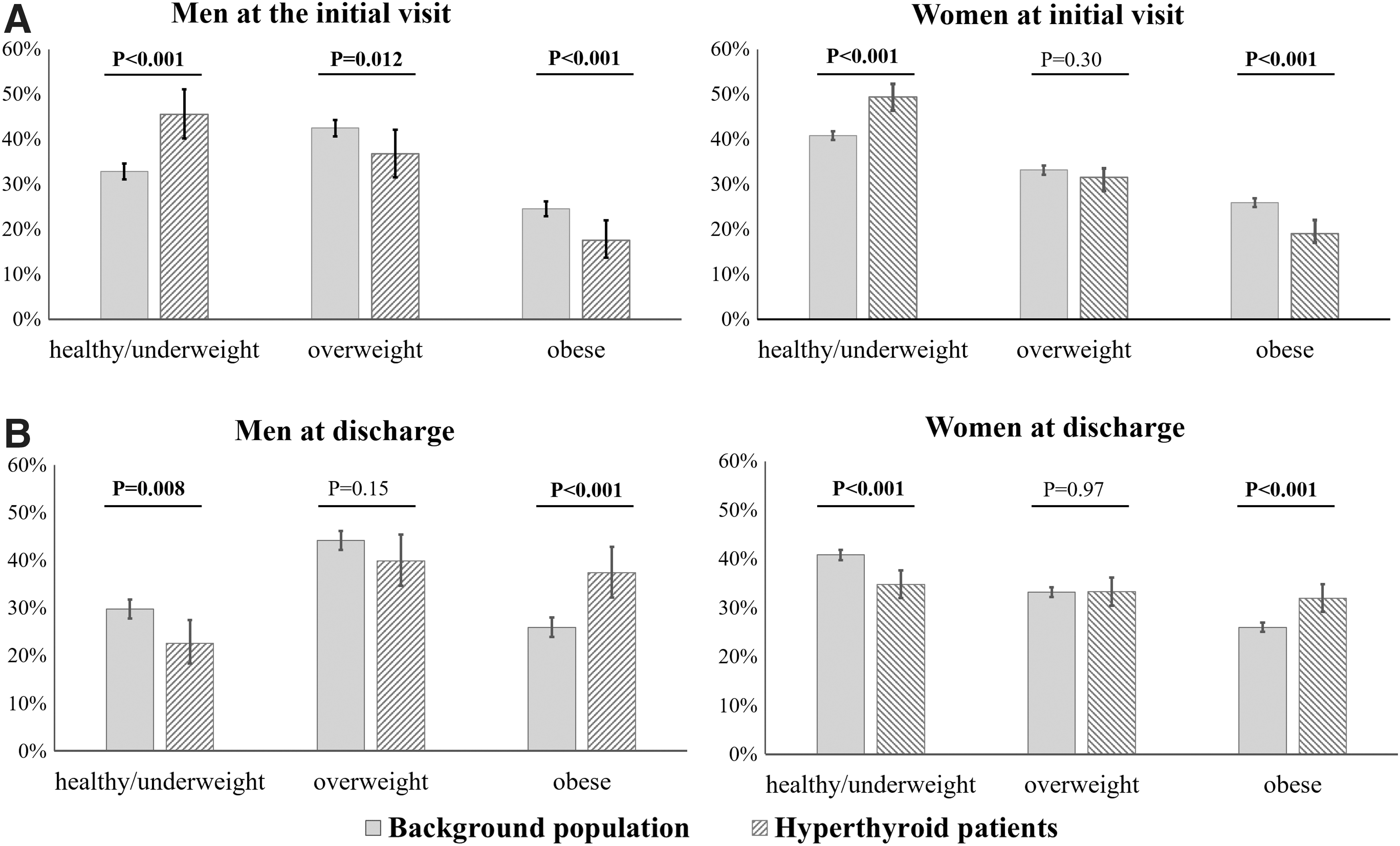
Body mass index in hyperthyroid patients compared with background population at time of initial visit (
At discharge, the proportions of obese male (37% vs. 26%, p < 0.001) and female (32% vs. 26%, p < 0.001) patients with hyperthyroidism were significantly higher compared with the control male and female population. The odds of becoming obese were increased for both male (1.7 [1.3–2.2], p < 0.001) and female patients (1.3 [1.2–1.5], p < 0.001). The OR estimates for obesity remained similar for both sexes after adjustment for smoking habits. The increases in proportions of obese patients were compensated by significantly less patients of both sexes with healthy/underweight BMI at the end of the treatment (23% vs. 30%, p < 0.001 for men and 35% vs. 41%, p < 0.001 for women) (Fig. 1, panel B). Patients' BMI expressed as continuous values at discharge was significantly higher compared with the background population (men: median 28.4 kg/m2 [interquartile range: 25.5–31.8] vs. 27.1 kg/m2 [24.5–31.2], p < 0.001; women: median 27.2 kg/m2 [23.8–31.2] vs. 26.1 kg/m2 [23.2–31.2], p < 0.001).
Weight changes during follow-up
The mean weight gain in the cohort of patients with hyperthyroidism was 6.0 (±7.1) kg. A weight increase of ≥5% was observed in 896 (65%) and of ≥10% in 526 (38%) patients, when comparing body weight at discharge and at presentation.
Men gained significantly more weight than women (Table 2) as did patients with Graves' disease compared with either those with toxic nodular hyperthyroidism or with indeterminate etiology. The extent of weight gained correlated with the severity of hyperthyroidism at presentation, and patients with Graves' disease had higher fT4 levels compared with those with toxic nodular disease (54.7 pmol/L, SD ±24.9 vs. 39.4 pmol/L, ±19.1). Patients who reported weight loss before diagnosis gained significantly more than the other groups; however, small amounts of weight gain were noted equally in those who reported weight gain or no weight change before treatment and in patients with no recorded weight changes. Cigarette smokers at presentation gained more at the end of treatment. Whether the final weight change was influenced by change in smoking habits is not clear as such data were not recorded during follow-up.
Mean Weight Change Comparing Initial and Discharge Weights (kg) and Mean Percentage Weight Change of Initial Body Weight (%)
CI, confidence interval.
Figure 2 illustrates the mean percentage weight change in all patients during follow-up. Weight gain was most pronounced during the first 6 months following presentation, when a mean increase of 5% of baseline weight was observed. Weight gain continued throughout the period of follow-up and reached a mean of 10% increase at 24 months after presentation, which continued until the end of study.
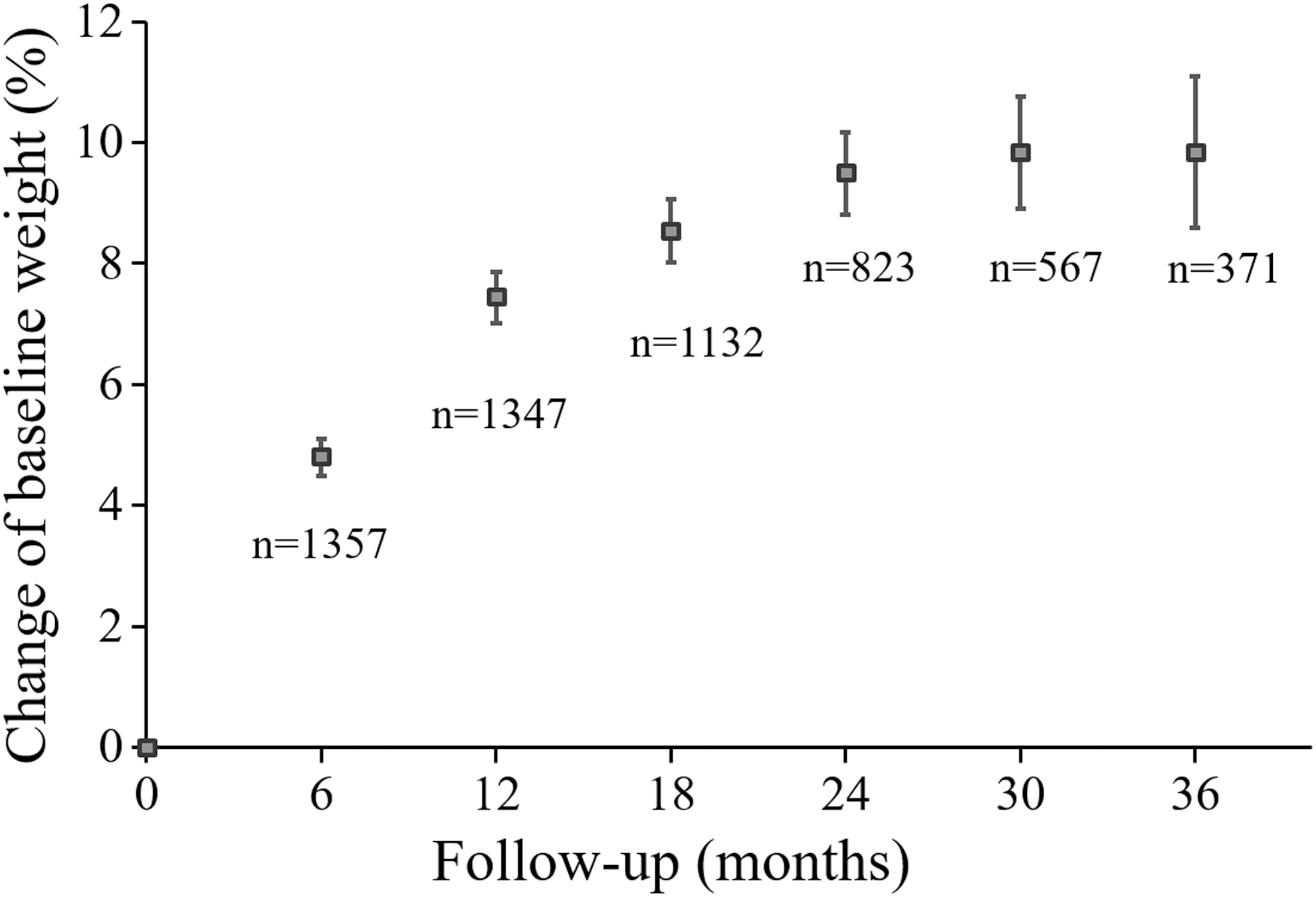
Mean percentage weight change in the study cohort during the follow-up in six-month intervals; whiskers represent 95% confidence intervals.
Weight changes in relation to treatment
Over the period of treatment and follow-up, patients undergoing medical therapy only (n = 573) gained on average 5.4 kg (±7.1), those remaining euthyroid following 131I (n = 229) gained 5.2 kg (±6.6), and patients who developed hypothyroidism following 131I (n = 571) gained 7.1 kg (±7.0). Those with 131I-induced hypothyroidism gained significantly more than those remaining euthyroid following131I (1.9 kg [95%CI = 0.6–3.3]) or those treated with ATD only (1.7 kg, 0.7–2.8). The difference in weight gain between ATD-only-treated patients and those euthyroid following 131I was statistically insignificant (0.2 kg, −1.2 to 1.5). Univariate analysis of weight gain within particular demographic and clinical categories is presented in Supplementary Table S1.
The multivariable longitudinal analysis demonstrated that 131I treatment was associated with a small but significant additional weight gain (0.6 kg, p < 0.001), compared with ATD alone (Table 3). Raised TSH levels (0.5 kg, p < 0.001) and low fT4 measurements (0.3 kg, p < 0.001) during follow-up were associated with significantly more weight gain compared with thyroid function within the reference range during follow-up. In addition to development of hypothyroidism (raised TSH concentrations and below normal fT4), the start of LT4 replacement was associated with an additional small but significant weight increase (0.4 kg, p < 0.001). On the contrary, uncontrolled and prolonged thyrotoxicosis, indicated by high serial concentrations of serum fT4 as well as undetectable or below normal serum TSH concentrations, was associated with less weight gain.
Multivariable Model Predicting the Weight Change Following Treatment for Hyperthyroidism
The model presents the variables of interest in bold; the coefficients indicate predicted weight change (kg); the reference category is underlined.
I, radioactive iodine; TSH, thyrotropin.
Based on our model, we predict that a typical patient, whose hyperthyroidism would be controlled with ATD pretreatment, who would undergo 131I therapy and become overtly hypothyroid (confirmed by fT4 ≤ 10.0 pmol/L [≤0.8 ng/dL] and TSH ≥10.01 mIU/L) requiring LT4 replacement would, therefore, weigh around 1.8 kg more than the same patient treated with ATDs only and not developing hypothyroidism. Figure 3 presents prediction of weight gain in a nonsmoking female patient with Graves' disease presenting with weight loss and fT4 between 30.1 and 40.0 pmol/L (2.3–3.1 ng/dL) treated with (i) ATDs alone, (ii) 131I, not developing hypothyroidism, or (iii) 131I, subsequently developing hypothyroidism requiring LT4 treatment.

Modeling of predicted weight gain in a nonsmoking female patient with Graves' disease presenting with weight loss and free thyroxine between 30.1 and 40.0 pmol/L (2.3–3.1 ng/dL) treated with (i) antithyroid drugs alone, (ii) 131I, not developing hypothyroidism, or (iii) 131I, subsequently developing hypothyroidism requiring levothyroxine treatment. 131I, radioactive iodine.
Sensitivity analysis excluding patients with indeterminate etiology
A sensitivity analysis was undertaken to test the model in patients with defined diagnoses of Graves' disease or toxic nodular hyperthyroidism and excluding those with hyperthyroidism of indeterminate etiology (characteristics of subcohort are presented in Supplementary Table S2). The analysis revealed similar findings and confirmed greater weight gain in patients treated with 131I compared with those receiving ATDs only (0.4 kg, p = 0.02). Serum TSH ≥10 mIU/L (0.5 kg, p < 0.001) and reduced fT4 (0.3 kg, p = 0.001) were associated with significantly greater weight gain. Following adjustment for weight changes associated with fluctuation in thyroid hormone concentrations, further additional weight gain was observed if 131I resulted in permanent hypothyroidism requiring treatment with LT4 (0.5 kg, p < 0.001). Raised serum fT4 concentrations during follow-up [−0.6 kg, −1.1, and −1.6 kg, p < 0.001 for fT4 22.1–30.0, 30.1–40.0, and >40 pmol/L (1.7–2.3, 2.3–3.1, >3.1 ng/dL), respectively] and below normal TSH concentrations (−0.8 kg, p < 0.001 for undetectable TSH and −0.4 kg, p = 0.001 for low but detectable TSH 0.1–0.3) were associated with significantly less weight gain. The full model data are presented in Supplementary Table S3.
Sensitivity analysis excluding patients using corticosteroids
Since patients with autoimmune thyroid disease are at increased risk of other autoimmune diseases (19) and therefore may require treatment with corticosteroids that may affect weight changes, we performed a further sensitivity analysis excluding those presently using oral or inhaled steroids. Twenty-six patients (1.8%) reported corticosteroid use and their baseline characteristics are displayed in Supplementary Table S4. Steroid users were more likely to be older than 60 years and to remain euthyroid following treatment with 131I. Patients on steroids were more likely to present with fT4 concentrations between 30.1 and 40.0 pmol/L (2.3–3.1 ng/dL), and were less likely to have well-defined Graves' disease. In view of these differences between steroid users and nonsteroid users, we conducted a further sensitivity analysis excluding patients taking steroids and the results are displayed in Supplementary Table S5. The values of the explanatory variables have not changed, confirming robustness of our model.
Discussion
Principal findings
Our large longitudinal study of patients treated for hyperthyroidism demonstrates significant weight gain following antithyroid treatment, especially during the initial 6 months of follow-up but continuing for more than 24 months. Weight loss at presentation—seen in two-thirds of patients before diagnosis—resulted in significant weight increase during the course of treatment. However, weight regain significantly overshot the comparator background population average weight, contributing to the increased risk of becoming obese.
We quantified the amount of weight change following treatment for hyperthyroidism defined as the difference between the weight measurements taken during the initial visit to our clinic and the time of discharge to community, which was 8 kg for men and 5.5 kg for women. In some patients, antithyroid treatment was commenced in the community and by the time of clinic measurements some regain may have occurred. While this may have affected our results, it is likely that our data underestimate the total weight gain following treatment for hyperthyroidism as the regain observed before the clinic visit was not captured. We confirmed more weight gain in men (20), in those with more severe hyperthyroidism (21,22), and in patients with Graves' disease (23). The observed excessive weight gain in patients with Graves' disease compared with toxic nodular hyperthyroidism may be, in part, related to a larger amount of weight loss before presentation as a consequence of more severe hyperthyroidism. However it is possible that appetite controlling signals are affected differently depending on the etiology of hyperthyroidism and further studies are required to explore these hypotheses.
Weight gain and BMI increase have been linked with increased risk of development of parameters of the metabolic syndrome, including hypertension, hypercholesterolemia, and type 2 diabetes mellitus (24 –26). However, there are no clear data relating to the exact impact of a 1.1–1.3 U difference in BMI as we observed when comparing our patients with the background population, and the follow-up period in our study was not long enough to detect significant increases in development of these long-term consequences. However, since patients with hyperthyroidism are at increased risk of cardiovascular morbidity and mortality, further studies are required specifically assessing the risk of development of the metabolic syndrome in patients treated for hyperthyroidism.
Our longitudinal model established time-varying changes in serum concentrations of thyroid hormones as significant factors influencing total weight change at the end of the study. TSH concentrations outside the reference range were significantly associated with weight alterations. In particular, TSH levels above and fT4 below normal were associated with more weight gain. The extent of TSH abnormality correlated with the amount of observed weight change. Importantly, we demonstrated that the control of thyroid function during follow-up significantly influenced the total amount of weight change. Prolonged periods of increased serum fT4 and/or of reduced TSH concentrations resulted in less weight gain at 36 months of follow-up. Our findings are consistent with the strong correlation between alterations in thyroid hormone concentrations and changes in body weight found in children treated for Graves' disease (27). A large population study of healthy adults also showed that even small changes in thyroid function within the reference range may affect the BMI (28).
We demonstrate that there was an overall modest (0.6 kg) but significant increase in weight gain in those treated with 131I when compared with medical therapy alone. Additional significant increases were noted with development of hypothyroidism, indicated by reduced serum fT4 and raised TSH concentrations during follow-up, followed by LT4 replacement resulting in a further estimated amount of 1.2 kg weight gain. Similar findings were found in the subcohort of those with a defined etiology of hyperthyroidism.
Results in relation to other studies
Only a few smaller studies have compared the effect of different treatment modalities on weight gain. After 1 year of follow-up in 65 patients undergoing one of the three treatment modalities for hyperthyroidism, Pears et al. (29) found the highest increase in weight (7.4 kg) in patients receiving 131I, which was 2 kg more than those treated with ATDs and 1.1 kg higher than those treated with thyroidectomy. In univariate analysis, Dale et al. (23) reported no difference in weight gain comparing ATDs with 131I (5.2 vs. 4.8 kg), but patients treated with thyroidectomy gained significantly more (10.3 kg, p = 0.007). These results were not confirmed in multivariable analyses, most likely due insufficient power (n = 13 patients undergoing thyroidectomy). In our study, analyzing a much larger cohort, we were able to find a small but significant increase in weight gain in those treated with 131I in comparison with medical treatment.
Body weight is maintained by a fine-tuned balance between energy consumption and energy intake. Thyroid hormones have been reported to affect both. They influence thermogenesis (30) and formation of brown adipose tissue (31), as well as affecting resting energy expenditure by involuntary motor activity (32). Correlations between overfeeding/starvation and altered thyroid hormone production have also been reported (33). In addition, the relationship between hormones regulating appetite and the thyroid is well established (34,35). All interplaying factors may be affected during and following the treatment for hyperthyroidism, although the exact mechanisms and specific effects of different antithyroid treatments remain elusive.
Strengths and weaknesses of the study
Our study is the first longitudinal systematic analysis of a large cohort followed up for a long period of time allowing the long-term weight gain. Detailed and complex statistical analyses included not only baseline factors but also time-varying effects of thyroid function, which significantly affect the weight gain and so far have not been accounted for. Our approach of matched comparison to a randomly selected background population allowed us, for the first time, to associate the treatment for hyperthyroidism with the increased risk of becoming obese.
Nonetheless, our study is not free of shortcomings. First, our analysis is limited to two of three treatment modalities for hyperthyroidism; those undergoing thyroidectomy were not included in the study. A further limitation of our study is the proportion of patients in whom the etiology of hyperthyroidism was indeterminate. This is, in part, due to the lack of earlier testing for TRAb, which would allow for better identification of Graves' disease. However, our sensitivity analysis, including only patients with well-defined underlying diagnoses, lends further support to the validity of our data.
It would have been useful to study premorbid weight in relation to weight following completion of treatment. Due to the insidious nature of the condition and the prospective nature of the data collection, this was not obtainable. We did, however, collect data on self-reported weight changes compared with premorbid weights, as indicated in the Tables and Results sections. It is likely that these data are subjective and bias prone, which could, at least partially, explain the mean weight gain of 3.2 kg in those reporting no premorbid weight change.
Due to the nature of treatment for hyperthyroidism, blinded randomized clinical trials, considered the golden standard of clinical research, are not feasible. Hence, we used a nonrandomized observational design, in which causation has to be interpreted with caution.
Conclusions
Weight gain following treatment for hyperthyroidism with 131I or a 12- to 18-month course of ATDs is associated with increased risks of becoming obese. 131I treatment was associated with a small but significant increase in weight compared with ATD alone. An additional increase was observed following induction of hypothyroidism, which is commonly associated with 131I. Importantly, we observed significant effects of control of thyroid function on weight changes during follow-up. We postulate that discussion of the risk of excess weight gain should be undertaken and advocate weight management support approaches for patients with hyperthyroidism.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5