
Abstract
Background:
Prevention and treatment of iodine deficiency-related diseases remain an important public health challenge. Iodine deficiency can have severe health consequences, such as cretinism, goiter, or other thyroid disorders, and it has economic implications. Our aim was to give an overview of studies applying decision-analytic modeling to evaluate the effectiveness and/or cost-effectiveness of iodine deficiency-related prevention strategies or treatments related to thyroid disorders.
Methods:
We performed a systematic literature search in PubMed/MEDLINE (Medical Literature Analysis and Retrieval System Online), EMBASE (Excerpta Medica Database), Tuft's Cost-Effectiveness Analysis Registry, and National Health System Economic Evaluation Database (NHS EED) to identify studies published between 1985 and 2018 comparing different prevention or treatment strategies for iodine deficiency and thyroid disorders by applying a mathematical decision-analytic model. Studies were required to evaluate patient-relevant health outcomes (e.g., remaining life years, quality-adjusted life years [QALYs]).
Results:
Overall, we found 3950 studies. After removal of duplicates, abstract/title, and full-text screening, 17 studies were included. Eleven studies evaluated screening programs (mainly newborns and pregnant women), five studies focused on treatment approaches (Graves' disease, toxic thyroid adenoma), and one study was about primary prevention (consequences of iodine supplementation on offspring). Most of the studies were conducted within the U.S. health care context (n = 7). Seven studies were based on a Markov state-transition model, nine studies on a decision tree model, and in one study, an initial decision tree and a long-term Markov state-transition model were combined. The analytic time horizon ranged from 1 year to lifetime. QALYs were evaluated as health outcome measure in 15 of the included studies. In all studies, a cost-effectiveness analysis was performed. None of the models reported a formal model validation. In most cases, the authors of the modeling studies concluded that screening is potentially cost-effective or even cost-saving. The recommendations for treatment approaches were rather heterogeneous and depending on the specific research question, population, and setting.
Conclusions:
Overall, we predominantly identified decision-analytic modeling studies evaluating specific screening programs or treatment approaches; however, there was no model evaluating primary prevention programs on a population basis. Conclusions deriving from these studies, for example, that prevention is cost-saving, need to be carefully interpreted as they rely on many assumptions.
Introduction
Iodine deficiency is one of the world's leading causes of preventable brain disorders and intellectual disability. Thyroid disorders include a range of health conditions, such as goiter, thyroid nodules, hyperthyroidism, and hypothyroidism. These health conditions occur because the physiological function of the thyroid is affected. The iodine status is, at least in part, a key determinant for the pathogenesis of thyroid disorders (1 –3). About 28.5% of the world's population have insufficient iodine intake and are at risk of developing iodine deficiency disorders (IDDs) (4). Iodine deficiency is decreasing worldwide (4) because of the implementation of salt iodization programs. Although severe iodine deficiency has been eliminated from nearly all countries, individuals in many countries are still at risk of having mild-to-moderate iodine deficiency (4). This is due to the fact that the iodine intake is still not sufficient in many countries, posing a substantial public health problem (4,5). Recommendations and guidelines for iodine fortification and supplementation are published by WHO, UNICEF, and the Iodine Global Network (IGN) (1,6,7).
Iodine is essential for the synthesis of thyroid hormones, and therefore, for healthy brain development in the fetus. Iodine deficiency can therefore result in mental impairment, but IDD can be prevented by iodine fortification of food on a population basis. During pregnancy, additional iodine supplementation of pregnant women may be necessary to ensure adequate iodine supply to the fetus (2). Switzerland was the first country in Europe to implement a prevention program by starting an oral iodization program in 1922 on a voluntary basis. During the following decades, most countries in Europe started iodization programs on a voluntary or mandatory basis through the introduction of fortified table salt and iodine supplementation for pregnant women (4). For example, IDD prevention programs were introduced in Austria in 1963 and Germany in 1981 (1). IDD monitoring programs, assessing iodine intake and urinary iodine excretion in the population, are crucial for the evaluation of IDD prevention programs (8). Treatment strategies for disorders associated with insufficient iodine intake may vary and comprise, for example, hormone replacement therapy for hypothyroidism or total thyroidectomy for patients with large goiter (9).
Due to the variety of prevention and treatment programs available, it is essential for decision makers to thoroughly evaluate the benefits, harms, and cost-effectiveness of these strategies to derive evidence-based recommendations guiding public health decisions. Important outcome measures relevant to the individuals include survival measured in life years (LYs) and indices of health-related quality of life (QoL), such as quality-adjusted life years (QALYs). Additionally, considering limited health care resources, it becomes more important to take into account economic aspects and to assess the cost-effectiveness to compare them with other preventive and therapeutic interventions. Decision-analytic models are useful tools that are recommended to link evidence-based short-term clinical outcomes from clinical trials with long-term evidence on disease progression, patient preferences, and resource utilization to guide clinicians and health care policy decision-makers (10 –13). Decision-analytic models evaluate systematically a decision problem by including all available alternatives (e.g., therapeutic interventions) and all possible health consequences of the different options and analyze these options with regard to the outcome of interest (e.g., LYs, QALYs, or costs) (14,15).
To perform a systematic and quantitative assessment of the short- and long-term benefit–harm balance and cost-effectiveness of prevention programs for IDDs, decision-analytic modeling is needed to capture all possible health consequences of iodine deficiency and the comprehensive effect of a population-wide IDD prevention program on the population's life expectancy and QoL.
To the best of our knowledge, there is no systematic overview available on decision-analytic modeling studies evaluating the effectiveness or cost-effectiveness of prevention and treatment strategies for IDD and related thyroid disorders. The aim of this systematic review was to provide an overview of published decision-analytic models that evaluate the effectiveness or cost-effectiveness of prevention and treatment programs for thyroid disorders that can be related to iodine deficiency, such as hypothyroidism, but that might also have other causes. Furthermore, diseases might be caused by excessive iodine intake due to an IDD prevention program. Additionally, we aim to give critical insights for thyroid and clinical experts who are not familiar with decision-analytic modeling and cost-effectiveness analyses.
Materials and Methods
We performed a comprehensive systematic literature search in PubMed/MEDLINE (Medical Literature Analysis and Retrieval System Online), EMBASE (Excerpta Medica Database), Tuft's Cost-Effectiveness Analysis Registry, and NHS EED (National Health System Economic Evaluation Database) to identify published studies that applied decision-analytic models to evaluate prevention approaches of IDD as well as treatment strategies. To gain a broad overview of published decision-analytic models, potential consequences of iodine supplementation were also included in our review. For example, Graves' disease (GD) was included as “in regions of iodine deficiency, iodine supplementation precipitates Graves' hyperthyroidism” (16). As we were interested not only in IDDs themselves but also in how modeling techniques are applied to the disease course, consequences, and treatment, we also included diseases, such as hypothyroidism, when they did occur in iodine-sufficient regions or were not caused by iodine sufficiency. For example, autoimmune thyroiditis was included as it could be caused by excessive iodine intake (17) and therefore could be a potential harm of a prevention program. Studies related to thyroid cancer and individual diagnostic work-up (e.g., diagnostic work-up of thyroid nodules) were out of the scope of this study and were excluded. We included studies published between 1985 and May 2018 and did not go back further in time as we assumed that models older than that might be too old to reflect the current state of the art in medicine and research. The search was restricted to studies published in German or English. To be eligible, studies were required to compare different prevention or treatment strategies with a decision-analytic model and to evaluate patient-relevant health outcomes, such as remaining LYs or QALYs. QALYs are calculated by multiplying the LYs spent in a specific health state by the utility of the health state. Utilities are preference-based measures (i.e., quality-of-life indices) with values from zero (death) to one (perfect health) (18).
Commonly applied modeling techniques in medical decision-making and health economic evaluations are decision trees, state-transition models, discrete-event simulations, agent-based models, and dynamic transmission models (19). The optimal modeling technique depends on the particular decision problem or research question of interest (13,19).
A decision tree provides an overview of all important components of a decision problem as it depicts all possible pathways and consequences for all compared strategies (18). According to the ISPOR-SMDM guidelines for modeling, decision trees may be an appropriate model type for simple models addressing problems with a very short time horizons and very few outcomes (19). State-transition models are appropriate if the disease process can be represented as a series of health (or disease) states and transitions between these states (19). They are useful for longer time horizons as well as for the timing and recurrence of events (10,19,20). In state-transition models, individuals are in different health states and move in cycles between these states based on evidence-based transition probabilities derived from different published data from clinical trials, observational studies, clinical registries, or expert opinion (20). Discrete event simulation should be applied if the decision problem involves constrained resources (e.g., waiting lines) (21). Agent-based models are an extension of discrete event simulation and can be applied for more complex behavior and detailed representation of interactions between individuals or populations with the environment (21). Dynamic transition models should be applied to model the effect of disease transmission in open cohorts, for example, to assess the spread of an epidemic in acute infectious diseases (22).
All studies were screened by at least two independent reviewers (M.S. V.Q.R., I.S., M.S.), and a third person (U.R.) decided on inclusion if there was disagreement on methodological questions. For clinical and epidemiological questions, an expert from the EUthyroid consortium (
Results are combined and displayed in a comprehensive evidence table providing a systematic overview on the various study characteristics, such as target population, research question/objective, time horizon, health outcomes, analytic approach, perspective (e.g., payer perspective, societal perspective, and patient perspective), results, and the authors' conclusions. For transparency and comparability, we standardized the results of all modeling studies. In the first step, we adjusted all costs to Euros of the same year using purchasing power parity rates (24). In the second step, we converted these adjusted costs into 2017 Euros by applying the Consumer Price Index (25). Additionally, we provided a condensed descriptive summary of the results including interpretations to facilitate comprehension for the readers. Finally, we discussed the different modeling approaches applied to provide an introduction to the matter for thyroid and clinical experts. Our interpretations and presentations follow international guidelines for modeling and health technology assessment (12,13,15,19,20,22,26 –28). Details of the systematic search are provided in the Supplementary Data.
Results
Systematic search
Overall, 3950 studies were identified. After removal of duplicates and abstract/title screening, 48 studies were evaluated in the full-text screening. After full-text screening, 17 studies were included (Fig. 1). Studies excluded in full-text screening are listed in Supplementary Table S1 with exclusion reasons.
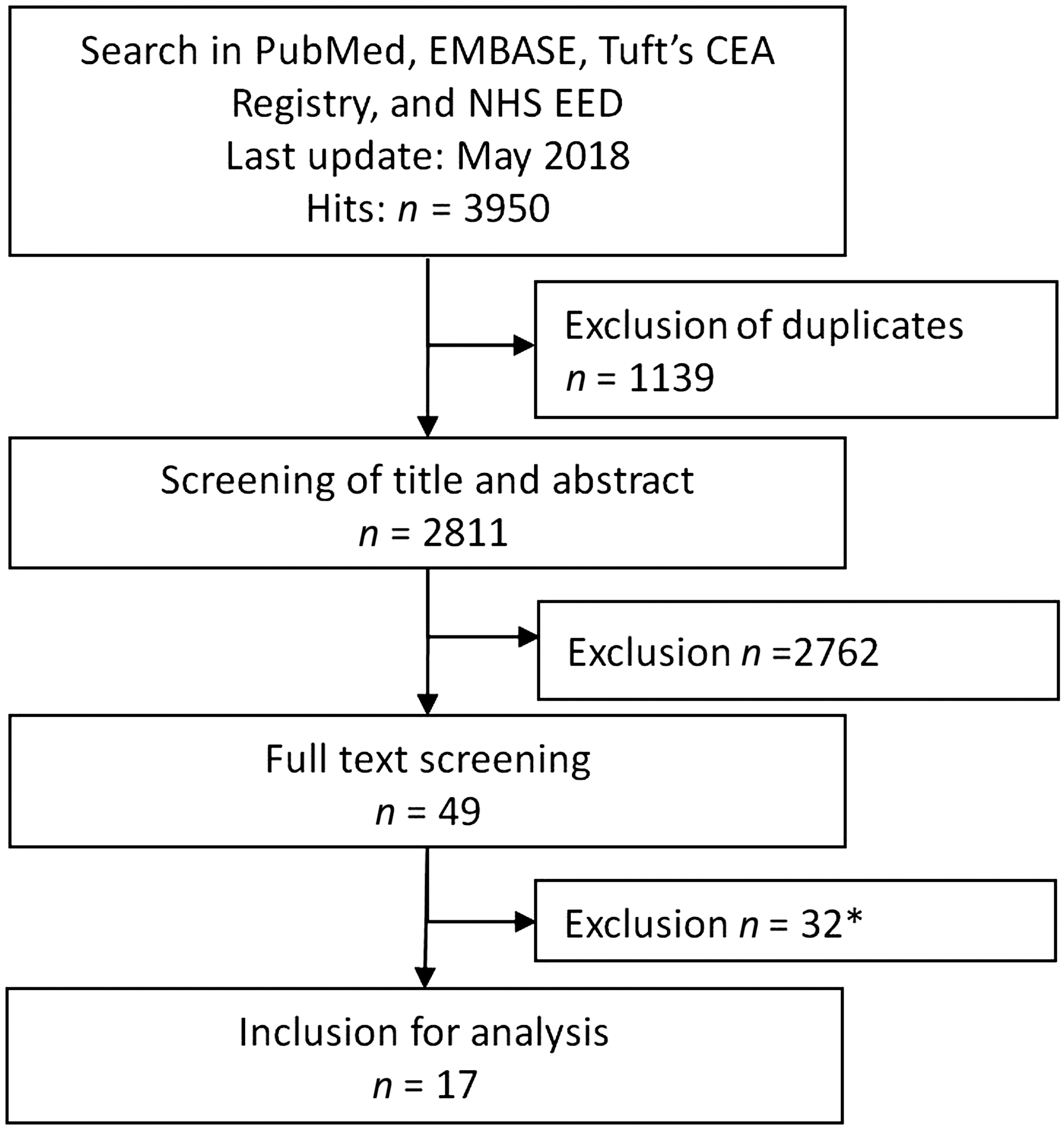
Flow diagram of the systematic search. Modified flow diagram recommended by PRISMA. *Thirty-two studies were excluded as they were no decision-analytic modeling studies, the model not described detailed enough, the content not related to treatment or prevention of iodine deficiency disorders or thyroid-related diseases, or the full-text was not accessible. EMBASE, Excerpta Medica Database; MEDLINE, Medical Literature Analysis and Retrieval System Online, PRISMA, preferred reporting items for systematic reviews and meta-analyses; PubMed; NHS EED, National Health System Economic Evaluation Database; Tufts CEA Registry, Tufts Cost-Effectiveness Registry.
General overview
Eleven studies evaluated screening programs, five studies evaluated treatment approaches, and one study evaluated a primary prevention strategy related to IDD. Most of the studies have been conducted in the health care context of the United States (n = 7); three evaluations are for the Iranian context, two for the French context, one for Italy, one for Spain, one for The Netherlands, one for the United Kingdom, and one jointly for England and Australia. Most of the studies did not mention if they were conducted in an iodine-deficient population. However, most of the studied populations are assumed to be iodine sufficient (e.g., United States, France, The Netherlands, Iran) (8). Only the population in the United Kingdom is mildly to moderate iodine deficient, and this was explicitly mentioned in the modeling analysis by Monahan et al. for the UK context (29). In nine studies, a decision tree analysis was applied and a Markov state-transition model was used in seven studies. In one study, a combination of an initial decision tree and a long-term Markov state-transition model was reported (30). Across studies, the analytic time horizon ranged from 1 year to lifetime. In 15 studies, QALYs were evaluated as outcome measure. None of the models reported a formal model validation. Table 1 provides a comprehensive overview of the included studies and their characteristics and features.
Comprehensive Overview of Evaluated Research Questions, Applied Methods, Results, and Conclusions
Only direct costs are included.
Authors call it: “government contribution to the healthcare sector.”
Authors call it “decision tree.” In our opinion, it could be a Markov state-transition model or a combination of both.
Authors call it: “Markov decision-tree model.”
Ab, antibody; AITD, autoimmune thyroid disease; ATDs, antithyroid drugs; ATM, antithyroid medication; BIOT, biotinidase deficiency; CAH, congenital adrenal hyperplasia; CEA, cost-effectiveness analysis; CH, congenital hypothyroidism; CL, cycle length; CUA, cost–utility analysis; DALY, disability-adjusted life year; DSA, deterministic sensitivity analysis; GAL, galactosemia; GD, Graves' disease; HCY, homocystinuria; MCAD, medium-chain acyl-CoA dehydrogenase; MSUD, maple syrup urine disease; NHS, National Health Service; PKU, phenylketonuria; PP, postpartum; PPT, postpartum thyroiditis; PSA, probabilistic sensitivity analysis; QALY, quality-adjusted life year; RAI, radioactive iodine; TPO, thyroid peroxidase; TSH, thyrotropin; TT, total thyroidectomy.
The next paragraphs present narrative study descriptions including short interpretations.
Primary prevention modeling
The study by Monahan et al. performed in the United Kingdom was the only one evaluating a primary prevention program (29). The authors applied a decision tree to assess the consequences of supplementation of iodine during pregnancy on the offspring, particularly regarding the IQ level. The authors concluded that iodine supplementation is cost-saving (dominant) in the UK context (29), meaning that the program provides health benefits in terms of IQ points gained and simultaneously saves net costs. The authors used a rather simple decision tree approach because the only outcome assessed was the IQ in the offspring (29).
Secondary prevention/screening modeling
Newborn screening
Four studies were on screening and prevention programs in newborns (31 –34). Different laboratory methods for screening were examined by two of the studies (31,32).
Shamshiri et al. aimed to recommend an optimal cutoff point for congenital hypothyroidism screening with the Guthrie thyrotropin (TSH) test (32). The health outcome evaluated was disability-adjusted life years (DALYs). DALYs take into account the years-of-life lost due to premature mortality and the years lost due to disability caused by the disease; it can be interpreted as “one lost year of ‘healthy’ life” (35,36). The authors concluded that increasing the cutoff of the Guthrie TSH test for congenital hypothyroidism determination not only decreases the recall rate and stress for the family but also decreases the DALYs gained and increases cost and care of patients with congenital hypothyroidism (32). The authors developed a rather simply structured decision tree including patients with false negative test results and a recall system for suspected cases. The outcomes included permanent mental retardation, transient retardation, and no retardation. Disabilities by other diseases or conditions were considered for the whole cohort in the model (32).
Hatam et al. evaluated different neonatal screening programs including congenital hypothyroidism screening (33,34). They published two articles using different perspectives for the economic analysis. The authors concluded that the screening programs are cost-saving (33,34). Hatam et al. also created a simple decision tree and estimated the lifelong costs of the screening programs including consequences for treatment (screened and unscreened patients) and the screening programs themselves (33,34). Additionally, infrastructure and family/patient expenses were considered. It remains unclear how the authors estimated the life expectancy of the newborns; they might have applied life expectancy from life tables and then multiplied the expected life expectancy by the utilities, which they derived for screened and unscreened patients (33,34).
Carroll and Downs also evaluated different screening programs (31). The screening programs consisted of a mixture of eight different screening tests. Life expectancies and respective decreases by morbidity were estimated from the national official data and cohort studies. The authors concluded that newborn screening is, in most cases, cost-saving. A decision tree was constructed including various health outcomes, such as developmental delay or early childhood death by Carroll and Downs (31).
Pregnancy screening
Five screening studies with pregnant women were included (30, 37 –40).
Bonds and Freedberg applied a decision tree model “that accounted for cases of PPT [postpartum thyroiditis] detected, medical outcomes of screening, and costs of screening and care” (40). Three different strategies were compared, and a PPT subtree was created that included outcomes such as GD and PPT and respective utilities (corrected for the duration of the different outcomes). Bonds and Freedberg found that screening could be cost-effective depending on the willingness to pay threshold (indicating how much the society is willing to pay for an incremental unit of health, e.g., one QALY gained through the introduction of the new health technology) and should therefore be considered for inclusion to routine screening (40). The study is a classic example for the application of a decision tree model as it evaluates a short-term disease (“PPT generally resolves within the first year of delivery, the analysis was limited to 1-year postpartum”) (40).
Thung et al. aimed to evaluate the cost-effectiveness of screening for subclinical hypothyroidism during pregnancy (38). They applied a decision tree model to evaluate the base-case analysis with the outcomes being the IQ of the offspring and associated QALYs. The authors concluded that “routine screening of thyroid function early in pregnancy is not only cost-effective but also actually saves money while improving offspring outcome.” However, the authors mentioned several assumptions, such as “baseline estimates are derived from an observational study that contained relatively few patients and had certain methods limitations” (38). Thung et al. also applied a decision tree model evaluating the cost-effectiveness of screening for subclinical hypothyroidism during pregnancy. All effects of the program had a short-term time horizon, except for lifelong costs of mental retardation; therefore, a decision tree was sufficient for the problem (38).
Dosiou et al. applied a Markov state-transition model to compare TSH screening with anti-TPO (thyroid peroxidase) antibody screening and not screening of pregnant women in terms of cost-effectiveness (37). In the base-case analysis, only the impact on health outcomes of the mother was included (IQ decrease of the offspring was included as decrement in her QoL). The authors found TSH screening to be cost-saving compared with no screening in the base-case analysis. Anti-TPO antibodies screening compared with TSH screening resulted in an incremental cost-effectiveness ratio (ICER) of €16,191 per QALY gained (37).
In their updated (new data from two randomized controlled trials [RCTs]) study, Dosiou et al. compared universal screening, screening only in high-risk groups, and no screening (39). The model in this study did not make assumptions about the treatment effect on outcomes that have not been assessed in RCTs. For example, improvement of IQ in the offspring was not considered in the model because there has not been evidence about the effect of screening on offspring IQ levels in RCTs. The authors concluded that risk-based screening was cost-effective compared with no screening (€5776/QALY); universal screening versus risk-based screening resulted in a slightly higher ICER (€6208/QALY) (39). Dosiou et al. (37) applied a Markov state-transition model. Different from the screening models discussed above, here, not only short-term screening and treatment were included, but, for example, annual follow-up visits were considered; additionally, compliance was considered and, for example, in case of noncompliance with treatment, women could also return to being compliant (37).
Donnay Candil et al. evaluated different screening strategies for thyroid disorders during pregnancy in Spain (30). They concluded that universal screening in the first trimester is prevailing in Spain compared with screening of high-risk women and reported an ICER of €389/QALY when compared with no screening. Donnay Candil et al. used a decision tree model for short-term outcomes during pregnancy time and 1 year after pregnancy (30). This was followed by a Markov state-transition model evaluating lifelong clinical and health economic outcomes.
Periodic screening in the general population
Two studies evaluated periodic screening in the general population (41,42).
Bona et al. applied a Markov state-transition model to compare screening versus no screening for subclinical hypothyroidism in older adults (41). Patients (starting age of 60 years) were seen annually by a general practitioner and screened. The authors concluded that screening could be beneficial but is also accompanied by high costs when introduced at a population level. However, the interpretation of the results is difficult as the authors did not report results of a full incremental approach (41). The authors did not describe that they considered the identification of hyperthyroidism through TSH screening and the consequences of these findings.
Danese et al. evaluated screening every 5 years for mild thyroid failure at a periodic health examination starting at the age of 35 years (42). Depending on the results of the screening, patients were either treated, underwent yearly follow-up visits, or were screened again after 5 years. The model comprised several health states, including cardiovascular events, myxedema, and overt hypothyroidism. The authors concluded, “The cost-effectiveness of screening for mild thyroid failure compares favorably with other generally accepted preventive medical practices.” (42).
Bona et al. and Danese et al. applied a Markov state-transition model with periodically recurring events (e.g., annual screening) (41,42). This is a classical scenario for a Markov state-transition when multiple repeated events are considered.
Treatment modeling
Five of the studies compared treatment strategies including antithyroid medication, radioiodine therapy, and total thyroidectomy for patients with GD (43 –45), and for patients with toxic thyroid adenomas (46,47). Three applied a Markov state-transition approach and two applied a decision tree approach.
Treatment for GD
In et al. compared costs and other outcomes of different “therapeutic strategies for Graves' disease in patients failing to become euthyroid after an 18-month course of ATM [antithyroid medication]” (43). They concluded that in the United States total thyroidectomy is a cost-effective therapeutic option (43). In et al. stated that they applied a decision tree model, although they analyzed a rather long time horizon (50 years, which was the remaining life expectancy of the patients) and included different pathways and consequences and used sophisticated elements to include several future treatments and events in the decision tree (e.g., change management in case the treatment was not successful, occurrence of cancer in year 20). But the fixed system of the decision tree forced them to assume, for example, that all cancer cases occur in year 20 (43).
Zanocco et al. concluded that “subtotal thyroidectomy can be a cost-effective treatment for GD [Graves' disease],” whereas total thyroidectomy was dominated (i.e., more expensive and less effective than subtotal thyroidectomy) (44).
It must be noted that the results of the study by In et al. and the study by Zanocco et al. are not comparable because the target population assessed by Zanocco et al. consisted of patients at initial diagnosis of GD, whereas In et al. evaluated the treatment after failure of initial ATM (43,44). The model of Zanocco et al. also compared different treatment strategies for patients with GD. In this Markov state-transition model, it is possible to incorporate repeated events and time-dependent probabilities, such as: “a second 1-year attempt involving ATD [antithyroid drugs] treatment for persistent hyperthyroidism” or “the decision model permitted RAI [radioactive iodine] to be administered up to 4 times […]” (44).
Donovan et al. compared different first-line therapies for GD in England and Australia. ATM was the cost-effective alternative to total thyroidectomy and RAI (45). The authors applied a Markov state-transition model to include rates of relapse and the occurrence of major complications as well as the impact of the second-line therapy.
Treatment for toxic thyroid adenoma
Vidal-Trecan et al. published two studies modeling therapy for toxic thyroid adenomas (46,47). In their first study, they applied a decision tree model to compare four different strategies for the treatment of toxic thyroid adenomas. Surgery was found to be the most effective and less costly strategy (46). The authors stated, “as thyroid toxic adenoma cannot be considered as a chronic disease, we designed a simple recursive tree” (46). Additionally, they did not apply a Markov state-transition model due to the lack of data for the time-dependent probabilities of radiation-induced hypothyroidism, although a Markov state-transition model might have been more powerful in considering long-term consequences (e.g., radiation-induced hypothyroidism or thyroid cancer) (46). Vidal-Trecan et al. advanced their model and applied it to the US context and applied a Markov state-transition model including long-term consequences and more detailed information, such as if-then rules for repeating RAI or the decision for surgery (47). For the US setting, surgery was found to be an effective strategy with reasonable costs in patients younger than 60 years (47). Due to the different setting (i.e., first study for the European setting, second for the United States), a comparison between these results is not straightforward; however, the authors state that the results of both analyses are consistent (47).
Discussion
To the best of our knowledge, this is the first comprehensive systematic review on decision-analytic modeling studies on the evaluation prevention approaches or treatment strategies for IDD and related thyroid disorders. We identified 17 studies revealing a broad range of areas. However, only one study was explicitly conducted for an iodine-deficient population. The remaining studies included populations that are assumed to be iodine sufficient.
We found in our review that in nine studies solely a decision tree approach was applied. While this rather simple approach may be sufficient for some research questions, for other more complex research questions, a Markov state-transition model would be the more appropriate option. Decision trees are recommended to be used for questions that have a short and fixed time horizon (19). However, for chronic diseases with longer time horizons, it is recommended to use more flexible modeling methods, such as Markov state-transition models, individual-level state-transition microsimulations, discrete event simulation, or dynamic transmission models (19). In many diseases, the disease progresses over a longer time horizon and model parameters for progression/regression, QoL, and resource utilization change over time, or events can occur repeatedly. In these cases, decision tree models are usually not sufficient to provide a valid representation of the disease process. For these situations, the ISPOR-SMDM Joint Task Force recommends applying state-transition models as appropriate option, particularly if the disease can be represented with transitions between health states (19,20). Model types can also be combined. For example, in the study of Donnay Candil et al., (30) the authors adequately applied an initial decision tree to represent short-term events during pregnancy followed by a Markov state-transition model to evaluate the long-term consequences including new cases of clinical hypothyroidism, which could occur in the future.
Another issue is the choice of the cohort simulation as closed or open (dynamic) cohort. A closed cohort includes patients at a certain (baseline) point in time and follows them over a specific time span or until all have died (as in a trial). An open cohort allows for the entry of new individuals into the assessed (dynamic) population. We did not find any modeling approaches considering open/dynamic cohort modeling approaches, in which the full effect of a prevention or screening strategy on the currently alive individuals and future generations was evaluated. Closed cohort models evaluating IDD prevention programs only consider the effect of the preventive intervention on the currently alive population. They cannot capture the full effect of an intervention on a population, including future generations, as they do not consider the effect on newborns (entering the cohort) leading to an under- or overestimation of benefits or harms.
A strength of comprehensive and flexibly programmed decision models is that they can be adapted to evaluate new decision problems and research questions or be transferred to other perspectives, regions, and populations (48). In our review, we identified only one model that was applied for two different health care contexts and one model using two different perspectives for the economic analysis. There are different obstacles for transferring decision-analytic models to other contexts or settings by independent modelers. Due to space limitations, the models are often not sufficiently described, which makes it nearly impossible for independent research groups to “rebuild” the model. However, models should be reported transparently and it is possible nowadays to provide technical documents in supplementary appendices or to make them accessible by other means (27).
There are still substantial research gaps in evidence-based prevention of IDDs and related thyroid disorders.
Although many of the modeling studies in the field of screening are in favor of screening for thyroid dysfunction during pregnancy, it is very important to note that among experts screening in pregnancy is a highly controversial issue and modeling studies rely on many assumptions. For example, effectiveness data in the study of Thung et al. were estimated based on observational data (38). The current guidelines of the American Thyroid Association state, “There is insufficient evidence to recommend for or against universal screening for abnormal TSH concentrations in early pregnancy.” (49).
Studies on screening for hypothyroidism in the general population should consider the full range of effects of screening. For example, the detection of hyperthyroidism when TSH is measured could be included in the benefit harm ratio of the screening.
Only one study evaluated a primary prevention program of IDDs; this study was targeted to the specific topic of pregnancy. Currently, no comprehensive decision-analytic models are available incorporating the magnitude of patient- and disease-specific variables to evaluate the health consequences of iodine deficiency and the long-term effectiveness and cost-effectiveness of a population-based IDD prevention program. For a comprehensive assessment of an IDD prevention program, not only benefits but also harms should be included in the analysis. Furthermore, a decision-analytic model evaluating the long-term effectiveness and cost-effectiveness of an IDD prevention program should consider different aspects for a comprehensive analysis. The consequences of iodine deficiency can affect individuals of different ages. Therefore, the target population of a decision-analytic model evaluating consequences of iodine deficiency and its prevention should represent all age groups. Additionally, such a model should adopt an open cohort option to consider and quantify the effect on pregnancy and newborns in addition to the effect on the current population. A further crucial issue that is not addressed in any of the modeling studies is the risk or harm associated with iodine supplementation in the general population. For example, iodine fortification can be associated with deteriorated thyroid function and can also lead to autoimmune thyroid diseases. This aspect should be considered in a decision-analytic benefit–harm analysis, even before focusing on cost-effectiveness. As all systematic reviews, our study has several limitations. Our review was restricted to studies published in German or English languages. Therefore, we might have missed several studies, particularly outside North America and Europe. Additionally, the search was limited to four literature databases. However, the searched databases cover a broad range of studies. Furthermore, we restricted our search to studies published between 1985 and 2018. A strong limitation is the subjective interpretation of the published studies, their methodological approaches and results. We aimed to minimize this subjectivity by using standardized procedures and predefined extraction and evidence reporting tables and open the reporting and discussion of the studies to a broad range of co-authors from different areas. Importantly, whereas there were several studies focusing on different thyroid disorders, only one study specifically focused on the impact of iodine deficiency and was conducted in the context of an iodine-deficient population. Therefore, the results of the modeling studies are rather restricted in their applicability to IDD. However, our focus was on the methodological modeling approaches to assess which types of modeling studies were applied until now to evaluate prevention and treatment strategies in the field of IDD and thyroid disorders.
In conclusion, our study aimed to assess available evidence on the long-term effectiveness and cost-effectiveness of prevention and treatment programs for IDDs and thyroid disorders evaluated by decision-analytic modeling studies. Overall, we identified mainly decision-analytic modeling studies evaluating specific screening programs or treatment approaches of thyroid disorders; there was no model evaluating prevention programs on a population basis on multiple IDD outcomes. Further research in this field is needed to better understand the long-term benefits, risks, and cost-effectiveness of prevention strategies for the disorders due to iodine deficiency.
Footnotes
Acknowledgments
This work was also integrated in a Master thesis at UMIT (Marie Schönhensch “Systematic overview and meta-analysis on iodine deficiency related diseases and prevention programs,” completed February 2017). Edited for English language: Marisa Schauerhamer.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by EUthyroid. The project has received funding from the European Union's Horizon 2020 research and innovation program under grant agreement number 634453. This work was financially supported through Erasmus Mundus Western Balkans (ERAWEB), a project funded by the European Commission.
Supplementary Material
Supplementary Data
Supplementary Table S1