
Abstract
Background:
Particulate matter (PM) air pollution is an environmental risk to public health. The prevalence of thyroid disease during pregnancy has increased rapidly in recent decades, but the available data on the relationships among air pollution, thyroid function, and birth outcomes in pregnant women, particularly in China, are scarce. We aimed to evaluate the association between maternal exposure to PM2.5 and its components and maternal and neonatal thyroid function and to investigate whether thyroid function acts as a mediator between air pollution and birth weight.
Methods:
In this prospective birth cohort study, the levels of maternal exposure to PM2.5 and its components during the first trimester were assessed in 433 pregnant women in Nanjing, China, enrolled during 2014–2015. We evaluated the levels of maternal exposure to PM2.5 and its six main constituents—organic matter (OM), black carbon (BC), sulfate (SO4 2−), nitrate (NO3 −), ammonium (NH4 +), and soil dust—using the V4.CH.02 product of the Dalhousie University Atmospheric Composition Analysis Group. The maternal serum-free thyroxine (fT4), thyrotropin (TSH), and thyroid peroxidase antibody (TPOAb) levels during the second trimester were measured through electrochemiluminescent microparticle immunoassays. The neonatal TSH levels were detected using an AutoDELFIA Neonatal TSH kit within 72 hours after birth, and the birth weight Z-score of each newborn was estimated.
Results:
Higher exposure to maternal PM2.5 and some components (BC and NH4 +) decreased the maternal fT4 level (p < 0.05), and the birth weight Z-score was decreased (p < 0.05) by higher exposure to maternal PM2.5 and some components (OM, BC, NO3 −, and NH4 +). A mediation analysis clarified that the maternal fT4 levels explained 15.9%, 18.4%, and 20.9% of the associations of maternal PM2.5, BC, and NH4 + exposure with the birth weight Z-score, respectively (p < 0.05). After additional sensitivity analyses including only nonpreterm participants (n = 418) and non-TPOAb-positive participants (n = 415), the models remained stable.
Conclusions:
Our results suggest an inverse association between maternal exposure to PM2.5 and its components and the maternal fT4 levels. Maternal fT4 might act as a mediator between exposure to PM2.5 and its components and birth weight.
Introduction
Air pollution with particulate matter (PM), particularly fine PM with an aerodynamic diameter of ≤2.5 μm (PM2.5), is a major environmental risk to global public health (1,2). The main components of PM2.5 include organic matter (OM), black carbon (BC), sulfate (SO4 2−), nitrate (NO3 −), ammonium (NH4 +), and soil dust (3). PM2.5 can enter the blood circulation and distribute to various organs (4 –6). Additionally, PM-adsorbed components can detach from PM deposited in the lungs, cross the epithelial layer, and enter the bloodstream (7,8), and the adsorbed components of PM can also pass through the placental barrier to the fetus from the mother's blood and possibly affect fetal growth and development (9 –13).
Fetal growth and development are closely related to thyroid function, which is essential for a normal pregnancy (14). The fetal thyroid gland begins to develop at ∼10 weeks of gestation and cannot synthesize sufficient thyroid hormones by itself (15), and as a result, the fetus is dependent on the placental transfer of maternal thyroid hormones during the first half of pregnancy (16). Therefore, even minor changes in maternal thyroid homeostasis might affect the fetus.
Thyroid function is regulated by the hypothalamic–pituitary–thyroid (HPT) axis, and its homeostasis is vulnerable to environmental disruptors. Serum-free thyroxine (fT4) and thyrotropin (TSH) are the most commonly used markers for evaluating thyroid homeostasis in human studies. However, the effect of PM2.5 exposure on maternal and neonatal thyroid function is unclear. In fact, few epidemiological studies have examined PM2.5 exposure and thyroid function during early life (17), although it has been demonstrated that associated OM and some metals can disrupt the thyroid system in pregnant women and neonates (18 –24). In addition, a recent study observed an inverse association between third-trimester exposure to PM2.5 and the cord blood fT4/free triiodothyronine (fT3) ratio in newborns (17).
Maternal thyroid dysfunction is associated with increased or decreased birth weight (25,26). A previous study found that maternal exposure to PM2.5 can interfere with normal fetal growth and thereby lead to altered birth outcomes, such as lower birth weight (27 –30), and lower birth weight is associated with the occurrence of diseases later in life (31 –33).
To the best of our knowledge, the relationships between PM2.5, thyroid function, and birth weight have not been analyzed, particularly with regard to the components of PM2.5. Therefore, we aimed to evaluate the association between maternal exposure to PM2.5 and its components and maternal and neonatal thyroid function and to investigate whether thyroid function acts as a mediator between ambient air pollution and birth weight.
Methods
Study design and participants
This study was initiated and maintained at the Nanjing Maternity and Child Care Center. Eligible study participants (n = 910) were recruited between 2014 and 2015 in Nanjing, China. We obtained signed informed consent from all participants and the study was approved by the Medical Ethics Committee of Nanjing Medical University. We obtained signed informed consent from all participants and the study was approved by the Medical Ethics Committee of Nanjing Medical University. The eligibility criteria included a maternal age of ≥18 years, no active smoking and drinking before and during pregnancy, and Nanjing residency with an intent to participate and deliver in Nanjing. A face-to-face questionnaire interview was conducted at the time of enrollment to collect demographic information, including age, education level, maternal weight and height before pregnancy, and passive smoking before and during pregnancy. Data on birth outcomes, such as gestational age and birth weight, were obtained from the individual birth records. The distribution of the geographic location of the participants is shown in Figure 1.
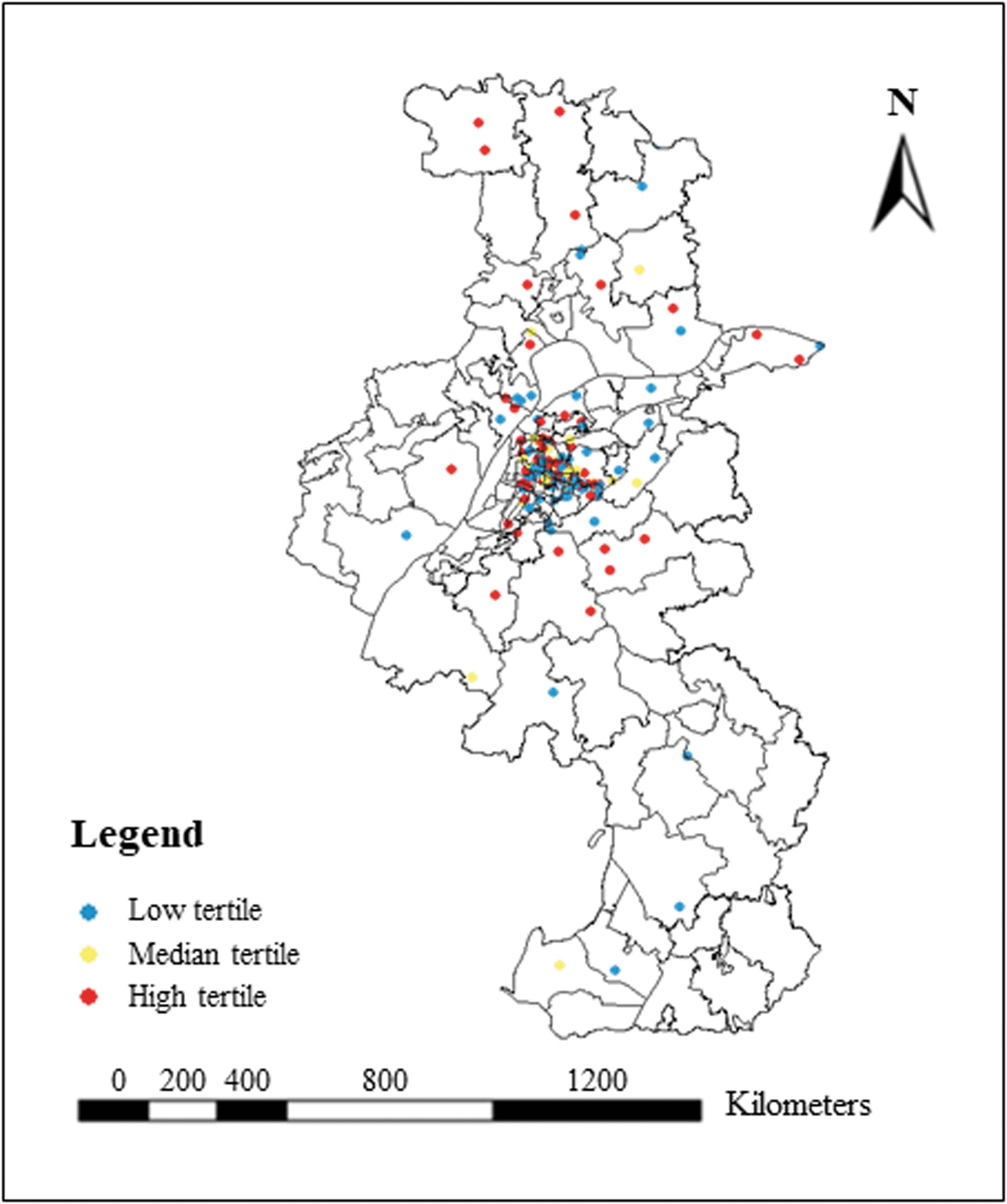
Distribution of the geographical location of the participants in Nanjing, China. Color images are available online.
Of the 910 enrolled eligible women, 72 were excluded due to lack of an accurate home address. Those who conceived with assistance (n = 27) were excluded, and the women who underwent definite treatment after a diagnosis of thyroid diseases before pregnancy (n = 10) were also excluded. Maternal serum samples were obtained from 466 of the remaining 801 women during the second trimester, and the maternal thyroid function during the second trimester was measured. The birth weights of the newborns of 443 of these 446 women were measured at the time of delivery, and their TSH levels were measured within 72 hours after birth. Thus, 443 mother–infant pairs were included in the final analysis (Supplementary Fig. S1).
Assessment of maternal exposure to PM2.5 and its components
The geocoded residential addresses of all 443 mothers were linked to the average modeled concentrations of PM2.5 and its constituents during the associated pregnancy trimesters. We evaluated the residential maternal exposure to PM2.5 and its six main constituents—OM, BC, SO4 2−, NO3 −, NH4 +, and soil dust—using the V4.CH.02 product of the Dalhousie University Atmospheric Composition Analysis Group (ACAG) (34) (Fig. 2). Briefly, this data set combines satellite retrievals and simulations of the aerosol optical depth from multiple sources (Multiangle Imaging Spectroradiometer [MISR], Moderate Resolution Imaging Spectroradiometer [MODIS] Dark Target, MODIS and Sea-Viewing Wide Field-of-View Sensor [SeaWiFS] Deep Blue, MODIS Multiangle Implementation of Atmospheric Correction [MAIAC], and Goddard Earth Observing System [GEOS]-Chem) with the geophysically based simulated relationship between the aerosol optical depth and the near-surface PM2.5 concentrations. GEOS-Chem simulation is used to partition PM2.5 mass into its composition. Ground-based observations from the recently expanded monitoring network over mainland China and Taiwan were then incorporated using monthly geographically weighted regressions at a 0.01° × 0.01° resolution from May 2014 to December 2016. The resulting annual mean PM2.5 concentrations were consistent with out-of-sample cross-validation observations (R2 = 0.78). The PM2.5 concentrations before this time period are based on the relative changes in ACAGs long-term product (34 –36).
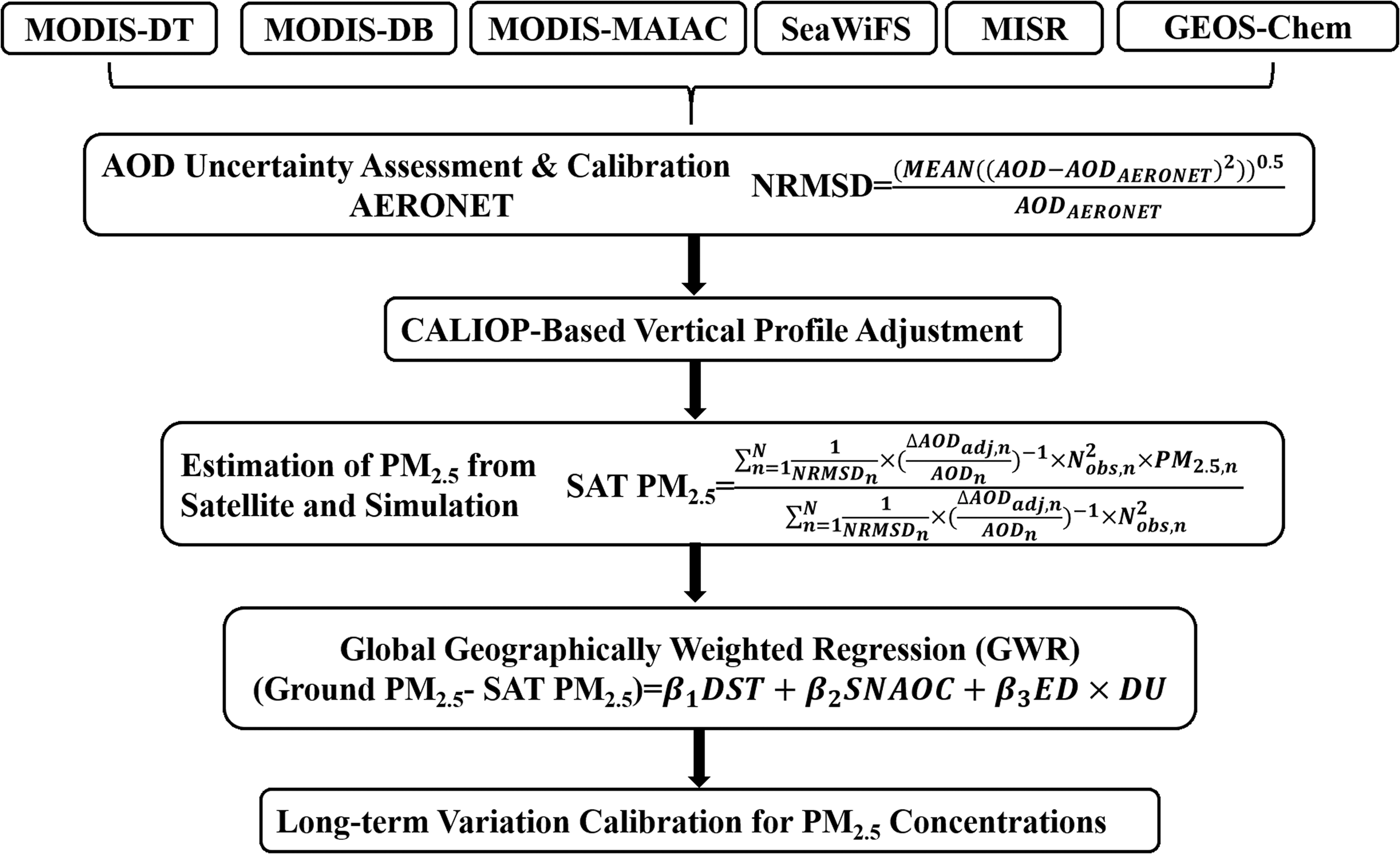
Flow diagram of the PM2.5 exposure assessment models. AOD, AOD, Aerosol Optical Depth; DB, Deep Blue; DST, disturbance index; DT, Dark Target; DU, inverse distance to the nearest urban land surface; ED, elevation difference; GEOS, Goddard Earth Observing System; MAIAC, Multiangle Implementation of Atmospheric Correction; MISR, Multiangle Imaging Spectroradiometer; MODIS, Moderate Resolution Imaging Spectroradiometer; NRMSD, normalized root mean square difference; PM, particulate matter; SeaWiFS, Sea-Viewing Wide Field-of-View Sensor; SNAOC, sum of sulfate, nitrate, ammonium, organic matter, and black carbon.
Assessment of maternal thyroid function
The maternal thyroid function during pregnancy was measured. In the first trimester (≤13 gestational weeks), the measurements of maternal thyroid function were performed at different community medical service centers. In the second trimester (14–27 weeks), the maternal thyroid function (fT4, TSH, and thyroid peroxidase antibody [TPOAb]) was measured at the Nanjing Maternity and Child Care Center.
Because thyroid function in the first trimester was assessed using different reagents and platforms at the different community medical service centers, we analyzed the thyroid hormone data from the second trimester. The maternal serum fT4, TSH, and TPOAb levels in the second trimester were measured through electrochemiluminescent microparticle immunoassays using the Architect system (Roche GmbH, Mannheim, Germany). The reference intervals in the second trimester are as follows (37): 0.39–5.22 mIU/L for TSH and 9.81–17.26 pmol/L for fT4. The normal clinical value of serum TPOAb is below 34 IU/mL.
Assessment of neonatal thyroid function
The neonatal TSH level, which serves as a marker of newborn thyroid hormone status, was measured within 72 hours after birth. Neonatal capillary blood samples were collected by heel pricking and spotted onto standardized filter paper. The neonatal TSH level was then measured using an AutoDELFIA Neonatal TSH kit (PerkinElmer, Inc.).
Statistical analyses
We estimated the birth weight of each newborn using the Z-score. According to the reference charts, the birth weight Z-score was determined by subtracting the mean and dividing by the standard deviation using the following formula:

where GA denotes the gestational age, XGA is the birth weight, and MGA and SDGA are the mean value and standard deviation at this GA according to the reference charts, respectively.
Analysis of variance F-tests were used to compare the levels of maternal exposure to PM2.5 based on the characteristics of the mothers and their infants.
Multiple linear regression models were used to examine the associations between (i) maternal exposure to PM2.5 levels and maternal and neonatal thyroid function, (ii) maternal exposure to PM2.5 levels and the neonatal birth weight Z-score, and (iii) maternal and neonatal thyroid function and the neonatal birth weight Z-score. Model 1 was unadjusted, and Model 2 was adjusted for the maternal age, education level, passive smoking, parity, sex of the baby, gestational age at delivery (if the neonatal TSH level was used as the outcome), and prepregnancy body mass index (BMI) based on the World Health Organization (WHO) classification (38). Independent variables were added to the model as continuous variables, and the exposures were categorized into low, medium, and high tertiles based on the exposure level and were used in the regression models with the first tertile as the reference. A mediation analysis was performed to explore the potential mediation of thyroid biomarkers that might underlie the relationship between maternal exposure to PM2.5 and the neonatal birth weight Z-score. In addition, the total effect was separated into a natural direct effect and a natural indirect effect through the mediation analysis (39), which was based on the assumption that all the relevant relationships, including the exposure and the outcome, the exposure and the mediator, and the mediator and the outcome, were causal and statistically significant.
All the analyses were performed using SAS 9.3 software (SAS Institute, Inc., Cary, NC). The level of significance was set to a two-sided p-value of ≤0.05.
Sensitivity analysis
Preterm delivery (gestational age < week 37) can affect birth weight (40). A previous study indicated that women positive for TPOAb during pregnancy have a higher risk of preterm delivery (41), which, as stated above, exerts an effect on birth weight. In a sensitivity analysis, we separately excluded the participants with preterm birth or those who were TPOAb-positive during pregnancy. We performed a linear regression analysis to examine the associations between first-trimester PM2.5 exposure and the neonatal birth weight Z-score after adjusting for the same confounders. We then repeated the mediation analysis to investigate whether this relationship was mediated by thyroid biomarkers in groups of women that did not include women with preterm birth or TPOAb positivity.
Results
In our study, the mean age of the participants was 29.5 years (range 20.0–41.0 years). Approximately half of the participants had a bachelor's degree or higher (n = 219; 50.6%), and 56.1% (n = 243) had a normal prepregnancy BMI (between 18.5 and 24.9 kg/m2). In addition, 51% (n = 221) and 49% (n = 212) of the newborns were boys and girls, respectively. Only 1% (n = 4) of the newborns were small for GA. The analysis of the levels of maternal exposure to PM2.5 did not show differences in any demographic characteristic, with the exception of passive smoking exposure and maternal education level, among the mothers and newborns. Participants who were subjected to passive smoking had higher levels of PM2.5 exposure (Table 1). Furthermore, we compared the characteristics of subjects who were included and excluded in the final analysis and found no statistical difference between them (Supplementary Table S1).
Characteristics of 433 Mothers and Their Infants, and Maternal Exposure to PM2.5
Statistically significant results (p < 0.05) are indicated in bold.
TPOAb negative: ≤34 IU/mL.
TPOAb positive: >34 IU/mL.
BMI, body mass index; PM, particulate matter; TPOAb, thyroid peroxidase antibody.
Table 2 shows the distributions of maternal exposure to PM2.5 and its components (OM, BC, SO4 2−, NH4 +, NO3 −, and soil dust), maternal and neonatal thyroid function, and birth weight. The levels of maternal exposure to PM2.5 ranged between 34.00 and 89.25 μg/m3. The maternal serum TSH and fT4 and neonatal TSH levels were detectable, and the means, percentiles, and ranges of these levels are provided in Table 2. The levels of fT4 were below the normal reference range in 17 individuals (3.9%) and above the normal reference range in 11 individuals (2.5%), and the levels of TSH were below the normal reference range in 8 individuals (1.8%) and above the normal reference range in 8 individuals (1.8%). Eighteen individuals (5.1%) were TPOAb positive, and there was no TPOAb data for 88 individuals. The maternal thyroid function status is shown in Supplementary Table S2. The follow-up characteristics of 41 individuals with abnormal gestational thyroid function are shown in Supplementary Table S3.
Distribution of Maternal Exposure to PM2.5 and Components, Maternal and Neonatal Thyroid Hormone Concentration, and Birth Weight
Among 433 subjects, the information for the maternal serum TPOAb concentration was missing in 83 subjects.
BC, black carbon; fT4, free thyroxine; NH4 +, ammonium; NO3 −, nitrate; OM, organic matter; SO4 2−, sulfate; TSH, thyrotropin.
Table 3 shows the associations between the levels of maternal exposure to PM2.5 and maternal and neonatal thyroid function. Higher levels of maternal exposure to PM2.5 were associated with decreased maternal fT4 levels and increased TPOAb concentrations after adjustment for potential confounders (maternal age, education, passive smoking, parity, gestational age, sex of the baby, and prepregnancy BMI) (p < 0.05). Consistent results were obtained from the comparisons of the high and low tertiles and the medium and low tertiles of maternal exposure to PM2.5 (p < 0.05). However, no statistically significant associations were observed between the levels of maternal exposure to PM2.5 and the neonatal TSH concentrations.
Associations Between Maternal Exposure to PM2.5 at the First Trimester and Maternal and Neonatal Thyroid Hormone Levels
Statistically significant results (p < 0.05) are indicated in bold.
Model 1: unadjusted model.
Model 2: adjusted for maternal age, education, passive smoking, parity, gestational age (for neonatal TSH level as outcomes), sex of the baby, and prepregnancy BMI categories (<18.5, 18.5–24.99, and ≥25 kg/m2).
CI, 95% confidence interval.
Table 4 shows the associations between maternal exposure to the components of PM2.5 and maternal and neonatal thyroid function. The levels of maternal exposure to BC and NH4 + were negatively associated with the maternal fT4 concentration, and the levels of maternal exposure to OC, BC, SO4 2−, and NO3 − were positively associated with the maternal TPOAb concentration after adjustment for confounders (p < 0.05). However, the levels of maternal exposure to PM2.5 components and neonatal TSH concentrations showed no statistically significant associations.
Associations Between Maternal Exposure to PM2.5 Components at the First Trimester and Maternal and Neonatal Thyroid Hormone Levels
Statistically significant results (p < 0.05) are indicated in bold.
Model 1: unadjusted model.
Model 2: adjusted for maternal age, education, passive smoking, parity, gestational age (for neonatal TSH level as outcomes), sex of the baby, and prepregnancy BMI categories (<18.5, 18.5–24.99, and ≥25 kg/m 2 ).
As shown in Table 5, the level of maternal exposure to PM2.5 was significantly inversely associated with the neonatal birth weight Z-score in a dose-related manner. Specifically, the birth weight Z-score of the newborns of mothers exposed to high PM2.5 levels was 0.23 (−0.47 to −0.01) lower than that of the newborns of mothers exposed to low PM2.5 levels, as demonstrated through linear multivariable-adjusted regression models adjusted for potential confounders. Additionally, the linear multivariable-adjusted regression models revealed a significant inverse association between maternal OM, BC, NH4 +, and NO3 − exposure and the birth weight Z-score (p < 0.05).
Associations Between Maternal Exposure to PM2.5 and Components at the First Trimester and Birth Weight Z-Score
Statistically significant results (p ≤ 0.05) are indicated in bold.
Model 1: unadjusted model.
Model 2: adjusted for maternal age, education, passive smoking, parity, gestational age, sex of the baby, and prepregnancy BMI categories (<18.5, 18.5–24.99, and ≥25 kg/m2).
Table 6 shows the associations between maternal thyroid function and the neonatal birth weight Z-score. No significant associations were found between the maternal TSH and TPOAb concentrations and the birth weight Z-score. Clearly, the maternal fT4 concentration was negatively associated with the birth weight Z-score (p < 0.05). The neonatal TSH concentrations were not significantly associated with the birth weight Z-score.
Associations Between Maternal and Neonatal Thyroid Hormone Levels and Birth Weight Z-Score
Statistically significant results (p < 0.05) are indicated in bold.
Model 1: unadjusted model.
Model 2: adjusted for maternal age, education, passive smoking, parity, gestational age, sex of the baby, and prepregnancy BMI categories (<18.5, 18.5–24.99, and ≥25 kg/m2).
The above steps completed our screening for mediation variables. First, our results show that maternal exposure to PM2.5 and some components (BC and NH4 +) are associated with a decreased maternal fT4 level. Second, we found that maternal exposure to PM2.5 and some components (OM, BC, NH4 +, and NO3 −) might decrease the birth weight Z-score. Third, we observed a negative association between the maternal fT4 level and the birth weight Z-score. Ultimately, we selected maternal fT4 as the mediator underlying the association between exposure to maternal PM2.5 and some components (BC and NH4 +) and the birth weight Z-score (Table 7). The mediation analysis clarified that the maternal fT4 level explained 15.9%, 18.4%, and 20.9% of the associations between maternal PM2.5, BC, and NH4 + exposure and the birth weight Z-score, respectively (all p < 0.05).
Natural Direct Effect and Natural Indirect Effect for Mediation of Maternal Exposure to PM2.5 and Components and Birth Weight Z-Score by Maternal Free Thyroxine Levels
Statistically significant results (p < 0.05) are indicated in bold.
Model 1: unadjusted model.
Model 2: adjusted for maternal age, education, passive smoking, parity, gestational age, sex of the baby, and prepregnancy BMI categories (<18.5, 18.5–24.99, and ≥25 kg/m2).
NDE, natural direct effect; NIE, natural indirect effect.
We did not include the maternal TSH and TPOAb levels in the mediation analyses because these variables did not meet the criteria for mediators.
Additional sensitivity analyses including only nonpreterm participants (n = 418) or non-TPOAb-positive participants (n = 415) did not alter the associations between first-trimester PM2.5 exposure and neonatal birth weight or the finding that fT4 was the main mediator after adjustment for the same confounders as in the main analysis (Supplementary Tables S4, S5, S6, S7).
Discussion
Thyroid homeostasis is closely related to the maternal and fetal physiological metabolism and is vulnerable to environmental disruptors. Abnormal maternal thyroid function is associated with a higher risk of perinatal complications, including premature delivery, low birth weight, placental abruption, preeclampsia, and neonatal death, and with a higher risk of detrimental effects on fetal neurodevelopment (42 –46). Our study constitutes the first exploration of the association between maternal exposure to PM2.5 and its components and thyroid function and of the factor through which thyroid function mediates the relationship between air pollution and birth weight in a birth cohort. We found evidence showing significant inverse associations between maternal exposure to PM2.5 and its components and the maternal fT4 level; moreover, the results show that maternal fT4 acts as a mediator between exposure to PM2.5 and its components and birth weight.
We assessed maternal ambient exposure to PM2.5 and its components. The mean prenatal PM2.5 exposure in our study was 60.82 μg/m3, which is approximately sixfold higher than the WHO air quality guideline (the exposure level is recommended to not exceed an annual mean of 10 μg/m3) (47). We compared the mean PM2.5 exposure in our study with that in other studies and found that it was at the same level or lower than that in the developing countries (48) and higher than that in the developed countries (17,49).
We found that higher maternal exposure to PM2.5 or PM2.5 components (BC and NH4 +) during the first trimester was associated with decreased maternal fT4 concentrations during the second trimester. This finding indicates that the first trimester of pregnancy is an important window of susceptibility to PM2.5 exposure. Only one previous study from Belgium focused on this topic, and the researchers who conducted the study demonstrated that prenatal exposure to PM2.5 leads to altered fetal fT4/fT3 levels but found no significant association between prenatal exposure to PM2.5 and maternal thyroid hormone levels among 431 participants. In our study, only TSH, a biomarker used for screening potential congenital hypothyroidism in newborns, was measured to assess the thyroid function of newborns, and we found no statistically significant difference between maternal PM2.5 exposure and neonatal TSH.
The method used in this study for the assessment of PM2.5 exposure is different from that used in the Belgian study (17). In addition, our exposure window was different. Specifically, we assessed maternal PM2.5 exposure during the first trimester, whereas the Belgian study assessed exposure during the third trimester. Furthermore, we obtained different ranges of exposure levels: the mean individual PM2.5 exposure levels in the Belgium study and our study were 16.0 and 60.82 μg/m3, respectively. This difference in exposure levels might lead to different effects on thyroid function.
Thyroid homeostasis is vulnerable to environmental disruptors. A previous study showed that air pollution from waste gas emissions, which originate mainly from industrial waste gas, is associated with thyroid cancer (50). No previous experiments have examined the effect of PM2.5 on the HPT axis. Thus, whether acute or long-term exposure to PM2.5 or its major components can influence the homeostasis of the HPT axis in susceptible individuals remains to be determined.
Evidence from our study suggests that PM2.5 exposure during pregnancy is negatively associated with child birth weight, which is consistent with the findings obtained in other studies (51,52). We also found that four components of PM2.5 (OM, BC, NH4 +, and NO3 −) might contribute to a lower birth weight. OM and BC are primary emissions from combustion processes, and NH4 + and NO3 − are inorganic aerosols generated in atmospheric chemical reactions (53). The mechanisms through which exposure to PM2.5 or its components leads to a lower birth weight remain unclear, although several mechanisms have been proposed (51). A previous study showed that thyroid hormone signaling is critical for regulating fetal growth and neural development (54). This finding is further supported by recent epidemiological studies in which maternal hyper- or hypothyroidism was found to be associated with fetal intrauterine growth retardation (26,55,56).
Previous studies found negative associations between maternal fT4 levels and birth weight (57,58), consistent with the results obtained in our study. Changes in maternal fT4 levels could affect the physiological metabolism, for example, lipid and protein degradation, of the mother and the fetus and thereby affect fetal growth and lead to changes in birth weight.
The mediation analysis showed that the maternal fT4 levels explained 15.9%, 18.4%, and 20.9% of the estimated effect of PM2.5, BC, and NH4 + exposure on the birth weight Z-score, respectively. Complex components adhere to the surfaces of PM2.5, and these components can accumulate in the maternal lungs and be transferred to the fetus (9,10,12,13), which supports our findings because these compounds potentially disturb maternal or fetal thyroid function and thereby affect fetal growth and development. At the public health level, the impact of our findings might be illustrated by previous studies showing that low birth weight is associated with health problems, such as perinatal mortality in the developing countries, childhood wheezing disorders, overweight or obesity, coronary heart disease, lowered intelligence in adolescence, all-cause mortality, chronic kidney disease, depressive disorders, and male reproductive dysfunction (31 –33).
In our study, the rate of maternal TPOAb positivity was 5.1% (18/350). Higher levels of maternal exposure to PM2.5 or some components (OM, BC, SO42−, and NO3 −) increased the TPOAb concentrations. The TPOAb levels are influenced by the immunomodulation that occurs during pregnancy (59,60), and experiments have confirmed that prenatal PM2.5 exposure adversely affects maternal immunity (61).
Finally, neither maternal nor neonatal TSH levels were found to be correlated with prenatal PM2.5 exposure.
The strengths of this study include, first, the use of a prospective birth cohort to evaluate the relationships between maternal PM2.5 exposure, thyroid function, and birth weight, particularly with a focus on a rarely investigated mediating factor: thyroid function. Second, we further explored the effects of major components of PM2.5 on thyroid function and low birth weight. Third, in our study, capillary blood samples were taken from the newborns, which might better reflect the thyroid function of newborns.
However, our study has limitations. First, we estimated PM2.5 exposure only based on the home address. The inclusion of individual assessments of PM2.5 exposure in the workplace would lead to more accurate results. Second, in this prospective cohort study, we studied the effects of PM2.5 during the first trimester on maternal thyroid function during the second trimester without assessing the long-term effects of prepregnancy PM2.5 exposure. Finally, iodine intake and the urinary iodine concentration, which might be related to the thyroid hormone levels, were not measured. Indeed, the findings emphasize the need for iodine measurements in other population studies.
In summary, we observed inverse associations between maternal exposure to PM2.5 and its components and the maternal fT4 levels. Maternal fT4 might act as a mediator between exposure to PM2.5 and its components and birth weight. Air pollution is a manageable and improvable environmental risk factor, and our results provide a theoretical basis for the future air pollution policy.
Footnotes
Acknowledgments
This work was supported by the National Key Research and Development Program of China (2017YFC0211605); the Qing Lan Project of Jiangsu Province, Six Talent Peaks Project of Jiangsu Province (JY-052); the Second Level of Training Object of Jiangsu Province “333” Project; and the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7