
Abstract
Background:
Thyroid hormone is essential for optimal fetal brain development. Evidence suggests that both low and high maternal thyroid hormone availability may have adverse effects on child neurodevelopmental outcomes, but the effect on behavioral problems remains unclear. We studied the association of maternal thyrotropin (TSH) and free thyroxine (fT4) concentrations during the first 18 weeks of pregnancy with child attention-deficit hyperactivity disorder (ADHD).
Methods:
A total of 7669 mother–child pairs with data on maternal thyroid function and child ADHD were selected from three prospective population-based birth cohorts: INfancia y Medio Ambiente (INMA; N = 1073, Spain), Generation R (N = 3812, The Netherlands), and Avon Longitudinal Study of Parents and Children (ALSPAC; N = 2784, United Kingdom). Exclusion criteria were multiple pregnancy, fertility treatment, usage of medication affecting the thyroid, and pre-existing thyroid disease. We used logistic regression models to study the association of maternal thyroid function with the primary outcome, ADHD, assessed via the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria by parents and/or teachers at a median child age of 4.5 to 7.6 years, and with the secondary outcome, an ADHD symptom score above the 90th percentile. Effect modification by gestational age and sex was tested with interaction terms and stratified analyses.
Results:
Overall, 233 (3%) children met the criteria for ADHD. When analyzed continuously, neither fT4 nor TSH was associated with a higher risk of ADHD (odds ratio [OR] 1.1, 95% confidence interval [CI 1.0–1.3], p = 0.060 and OR 0.9 [CI 0.9–1.1], p = 0.385, respectively) or with high symptom scores. When investigating effect modification by gestational age, a higher fT4 was associated with symptoms above the 90th percentile but only in the first trimester (for fT4 per 1 SD: OR 1.2 [CI 1.0–1.4], p = 0.027). However, these differential effects by gestational age were not consistent. No significant effect modification by sex was observed.
Conclusions:
We found no clear evidence of an association between maternal thyroid function and child ADHD.
Introduction
Thyroid hormone regulates important brain developmental processes including early neuronal proliferation and migration (1). Until mid-gestation, fetal thyroid hormone availability largely depends on the supply of maternal thyroid hormone via the placenta (2). Relatively mild deficits in thyroid hormone availability have been associated with adverse child neurodevelopmental outcomes, such as lower IQ, lower psychomotor development scores, and lower gray matter and cortex volume (3 –5). Evidence from mainly animal studies also suggests that high–normal thyroid hormone availability may have similar adverse effects on neurodevelopmental outcomes (5 –11). However, whether mild changes in thyroid hormone concentrations also play a role in the etiology of child behavioral problems is less well established.
Attention-deficit hyperactivity disorder (ADHD) is a “persistent pattern of inattention and/or hyperactivity–impulsivity that is more frequently displayed than is typically observed in individuals at a comparable level of development” (12) and occurs in ∼5.9–7.1% of children and adolescents (13). The exact cause of ADHD is unknown, but susceptibility is thought to depend on genetic predisposition, environmental factors, and their interactions (14,15).
There is some indication that high thyroid hormone availability may increase the risk of ADHD. Patients with resistance to thyroid hormone beta (RTHβ), in which a defective thyroid hormone receptor beta (TRβ) results in lifelong exposure to a high thyroid hormone concentration in tissues that predominantly express thyroid hormone receptor alpha (TRα) such as the brain, have a higher risk of ADHD (16). Furthermore, individuals with ADHD have a delay in cortical maturation, reduced neuronal activity, and brain volume (17 –19) compared with healthy controls; some of the same abnormalities are also seen in the offspring of mothers with gestational thyroid dysfunction (5,20 –22). However, further studies are required to clarify whether too low and/or too high thyroid hormone availability in pregnancy is consistently associated with the development of ADHD.
So far, evidence from epidemiological studies is inconsistent with regard to an association of maternal thyroid function with child ADHD (23 –31). Some studies indicated that the effects of maternal thyroid function on ADHD may be more prominent in girls (23,31), but further studies are needed to replicate and further clarify sex-specific effects. In addition, it would be relevant to investigate whether there are differential effects by gestational age, as the relatively late start of levothyroxine therapy in women with subclinical hypothyroidism or hypothyroxinemia in two randomized control trials has been suggested to be a reason for the negative findings for those trials (32,33). We therefore combined data from three prospective birth cohorts to study the association between free thyroxine (fT4) and thyrotropin (TSH) in early pregnancy and the risk of ADHD, as well as the effect modification by child sex and gestational age.
Materials and Methods
Study design and populations
We used data from three population-based birth cohort studies: INfancia y Medio Ambiente (INMA; Spain, subcohorts of Valencia, Sabadell, and Gipuzkoa), Generation R (The Netherlands), and the Avon Longitudinal Study of Parents and Children (ALSPAC, United Kingdom). Information on the designs of the three cohort studies can be found elsewhere (34 –37); the ALSPAC study website contains details of all the data that are available through a searchable data dictionary and variable search tool (38). Briefly, all three cohorts were designed to understand the role of environmental exposures and/or genetic characteristics for child growth, development, and health from fetal life until (young) adulthood.
The INMA Project is a network of seven birth cohorts in Spain with different recruitment periods. Pregnant women included in the Valencia (N = 855), Sabadell (N = 657), and Gipuzkoa (N = 638) cohorts enrolled from November 2003 until June 2005, July 2004 until July 2006, and April 2006 until January 2008, respectively. In Generation R, 9778 mothers with a delivery date from April 2002 until January 2006 were enrolled in the study. In ALSPAC, pregnant women resident in Avon, United Kingdom, with expected dates of delivery between April 1991 and December 1992 were invited to take part in the study. The initial number of pregnancies enrolled was 14,541, of which 13,998 children were alive at the first year of age.
For the current study, mother–child pairs were eligible if they had a thyroid measurement in the first half of pregnancy (≤18 weeks) and had data on an assessment of ADHD symptoms during childhood. Exclusion criteria were multiple pregnancy, fertility treatment, usage of medication affecting thyroid function during pregnancy, and pre-existing thyroid disease.
Ethical approval was obtained before recruitment and during the follow-up waves of data collection from a number of bodies: the Ethical Committee of the Municipal Institute of Medical Investigation, the Ethical Committees of the hospitals involved in the study (INMA; reference numbers G03/176, 2005/2106/I, and 2009/3432/I), the Medical Ethical Committee of the Erasmus Medical Center (Generation R; reference numbers: MEC 198.782.2001.31, MEC-2007-413), the ALSPAC Ethics and Law Committee, and the Local Research Ethics Committees [ALSPAC; reference numbers available at (39)]; approval by parents or guardians of the children was given by a signed informed consent form.
Maternal thyroid function
The procedures and methodologies by which maternal thyroid function was measured differed among cohorts.
In INMA, serum samples were collected at a mean (±standard deviation [SD]) gestational age of 13.1 ± 1.3 weeks and stored at −80°C after collection. fT4 and TSH were measured using a solid-phase, time-resolved sandwich fluoroimmunoassay (AutoDEL-FIA; PerkinElmer Life and Analytical Sciences, Wallac Oy, Turku, Finland) and a lanthanide metal europium (Eu) label. Thyroid peroxidase antibodies (TPOAbs) were not measured.
In Generation R, serum samples were collected at a mean ± SD age of 13.4 ± 1.9 weeks, centrifuged, and stored at −80°C after collection. fT4 and TSH were measured using the Vitros ECI immunodiagnostic (Ortho Clinical Diagnostics, Rochester, NY). Maternal TPOAbs were measured using the Phadia 250 immunoassay (Phadia AB, Uppsala, Sweden), and a TPO titer ≥60 IU/mL was considered as positive.
In ALSPAC, serum samples were collected at a mean ± SD age of 11.0 ± 3.2 weeks and stored at −20°C. fT4, TSH, and TPOAb measurements were performed using Abbott Architect i2000. A TPO titer ≥6 IU/mL was considered as positive. Additional information about the serum measurements is provided in the Supplementary Data.
ADHD symptoms
In INMA, ADHD symptoms were assessed by teachers at a median age of 4.5 years (interquartile range [IQR] 4.4–5.7 years) using the ADHD criteria of Diagnostic and Statistical Manual of Mental Disorders, fourth edition (ADHD-DSM-IV) list (12). The DSM criteria are a valid tool for diagnosing ADHD, already at a preschool age (40). The DSM-IV consists of questions on nine inattention symptoms and nine hyperactivity–impulsivity symptoms on a 4-point Likert scale (never or rarely, sometimes, often, or very often), designed to score ADHD symptoms present in the last six months before the assessment. A symptom was defined as present if the question was answered with “often” or “very often.” The total symptom score consisted of the sum of all the inattention and hyperactivity–impulsivity symptoms. Based on the symptom criteria of the DSM-IV, an ADHD diagnosis was given when the child had at least six inattention and/or six hyperactivity–impulsivity symptoms.
In Generation R, parents assessed their child's behavior in the last two months at a median age of 6.0 years (IQR 5.9–6.2 years) using the Child Behavior Checklist 1½–5 (CBCL/1½–5) (41). From this 99-item questionnaire, the sum score of six questions on a 3-point Likert scale (not true, somewhat or sometimes true, very true or often true) made up the total ADHD symptom score. In addition, the computer-assisted Diagnostic Interview Schedule for Children–Young Child version (42), which is a DSM-IV based interview, was administered by research assistants at a median age of 6.6 years (IQR 6.3–7.1 years) to the parents or caregivers of a selected group of children. This subgroup consisted of a random selection of negative controls and children with a high probability of a psychiatric disorder, e.g., children who scored in the top 15th percentile of the CBCL1½–5 total problem score and/or in the top 2% of the syndrome scale scores. Algorithms provided by the developers of this tool were used to derive a DSM-IV diagnosis based on the symptom criteria of the DSM-IV. More information on the procedures and assessment is described elsewhere (43). In our study, the reference group consisted of children who were not identified as having ADHD and children who did not have data on the Diagnostic Interview Schedule–Young Child version, but did have data on ADHD symptoms as assessed with the CBCL/1½–5 (e.g., mostly children with a low probability of a psychiatric disorder).
In ALSPAC, the Development and Well-Being Assessment (DAWBA) was used to evaluate child psychological disorders at a median age of 7.6 years (IQR 7.6–7.7 years) (44). This validated tool consists of questions based on the diagnostic criteria described in the International Classification of Diseases, Tenth Edition (ICD-10) or the DSM-IV. A semi-structured interview was administered to parents relating to inattention and hyperactivity symptoms present in the six months before the assessment. Teachers in the geographically defined study area were also requested to fill out the DAWBA questionnaire on all children with a birth date between April 1991 and December 1992. The completion rate by teachers was 37% for ALSPAC children (45). Clinical raters reviewed all available ratings on ADHD symptoms and assigned an ADHD diagnosis using the DSM-IV criteria as if in clinical settings.
Covariates
During pregnancy, questionnaires were used to collect information on maternal age, parity (zero, one, and two or more), prepregnancy body mass index, smoking during pregnancy (never, smoked in the beginning or until pregnancy confirmed, continued smoking), ethnicity/country of birth (cohort-specific categories), and maternal educational level (low, middle, and high). Gestational age at blood sampling was defined using ultrasound and/or last menstrual period. Information on sex of the child was obtained from community midwives, obstetricians, hospital registries, clinical records, or questionnaires. Age at ADHD assessment was obtained during the study visit.
Statistical analyses
Owing to the differences in assays, the absolute values of TSH and fT4 across the cohorts cannot be compared. We therefore calculated cohort-specific SD scores with a mean of 0 and a SD of 1 using logarithmically transformed values of fT4 and TSH based on TPOAb-negative women when possible. Values outside the mean ± 4 SD range were considered as outliers and excluded from further analyses.
We assessed the association of maternal TSH and fT4 SD scores within the mean ± 4 SD range with child ADHD by performing multivariable logistic regression models using pooled data. We used the same model to study the association with our secondary outcome, an ADHD symptom score above the 90th percentile, which was generated in each cohort separately. This extra harmonized cutoff was chosen a priori to increase statistical power owing to the low prevalence of children meeting the criteria of ADHD and has been used previously to define children at risk (46,47). Negative binomial regression models were used to assess the association of fT4 and TSH with total ADHD symptom scores on a continuous scale per cohort. We could not analyze these associations using pooled data since the symptom scores did not share a common metric between cohorts and therefore were not comparable.
We tested for nonlinearity by adding a quadratic term to our models and we assessed multicollinearity between covariates by the variance inflation factor. All cohort-specific models were adjusted for all the mentioned covariates. However, in the pooled analyses, we could not adjust for child age at ADHD ascertainment, maternal ethnicity/country of birth, and cohort simultaneously. The categories or the range of these variables did not overlap, i.e., they were cohort-specific, and adjusting for several of these variables at the same time causes multicollinearity. Therefore, in the pooled analyses, we chose to adjust for maternal ethnicity/country of birth because it is known that there are ethnic differences in maternal thyroid parameters during pregnancy (48 –50), and race/ethnicity is intertwined with social economic status, which has been associated with behavioral problems (51) and ADHD (13,52). We investigated whether adjusting for cohort instead of ethnicity/country of birth yielded different results. Because the results were similar, we chose to show the results based on the ethnicity/country of birth adjustment. We decided to present standard logistic regression models after comparison with multilevel models using the Akaike information criterion.
We performed several sensitivity analyses. First, we tested for heterogeneity between cohorts using the Cochran Q test and the I2 statistic [Supplementary Fig. S1; Ref. (53)]. Second, we also compared the effect estimates before and after excluding TPOAb-positive women in mother–child pairs, of which TPOAb status was known, e.g., Generation R and ALSPAC, since TPOAb positivity was associated with a higher risk of ADHD irrespective of maternal TSH (54). Third, we tested for possible effect modification by sex and/or gestational age at blood sampling by adding product terms into the models. To identify potential relevant effect modifiers, we screened for interaction terms with a p-value of <0.15 and subsequently performed stratified analyses to verify and quantify any relevant differences. For gestational age, analyses were stratified by tertiles based on pooled data (<11.8, ≥11.8 to ≤13.5, and >13.5 weeks).
The percentage of missing covariate data ranged from 0% to 15.6% (Table 1). Before pooling the cohort data, missing values in these covariates were imputed using chained equations, generating 25 data sets. Additionally, to alleviate the potential bias that arises when only the population with available data on maternal thyroid function and child ADHD symptoms is included, we applied inverse probability weighting (55). Briefly, we used data on characteristics available for all participants at recruitment to predict the probability of participation in the study, and an inverse of those probabilities as weights in the analyses so that results would be representative for the initial populations of the cohorts. Statistical analyses were performed in STATA (version 15.0; Stata Corporation, College Station, TX).
Distribution of Maternal and Child Characteristics
p-Value for differences was calculated using the chi-square test for categorical variables, one-way ANOVA for continuous normal-distributed variables, and Kruskal–Wallis test for continuous non-normal distributed variables.
Values do not take into account missing data (0%, 0.2%, and 0% for gestational age; 0.3%, 3.2%, and 2.5% for maternal education; 0.1%, 0%, and 2.9% for maternal ethnicity/country of birth; 0.2%, 0%, and 2.9% for parity; 1.4%, 9.0%, and 1.7% for smoking; 0%, 15.6%, and 8.8% for prepregnancy BMI; 0.1%, 0%, and 0% for child sex in INMA, Generation R, and ALSPAC, respectively).
ADHD, attention-deficit hyperactivity disorder; ALSPAC, Avon Longitudinal Study of Parents and Children; ANOVA, analysis of variance; BMI, body mass index; fT4, free thyroxine; INMA, INfancia y Medio Ambiente; IQR, interquartile range; NA, not available; SD, standard deviation; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Results
After exclusions, data for a total of 7669 mother–child pairs were available for analyses (Fig. 1). An overview of the characteristics of the study population is given in Table 1. The prevalence of ADHD was 5.3% (n = 57) in INMA, 3.2% (n = 121) in Generation R, and 2.0% (n = 55) in ALSPAC. Compared with the study population, women who were not included in the analysis had a lower education level, were less often native or Caucasian, and were younger in all three cohorts (Supplementary Table S1). There were similar differences in characteristics when comparing mothers whose children had an ADHD symptom score and those whose children did not undergo an ADHD assessment (Supplementary Table S2). No clinically relevant differences were found in TSH and fT4 concentrations between these two groups.
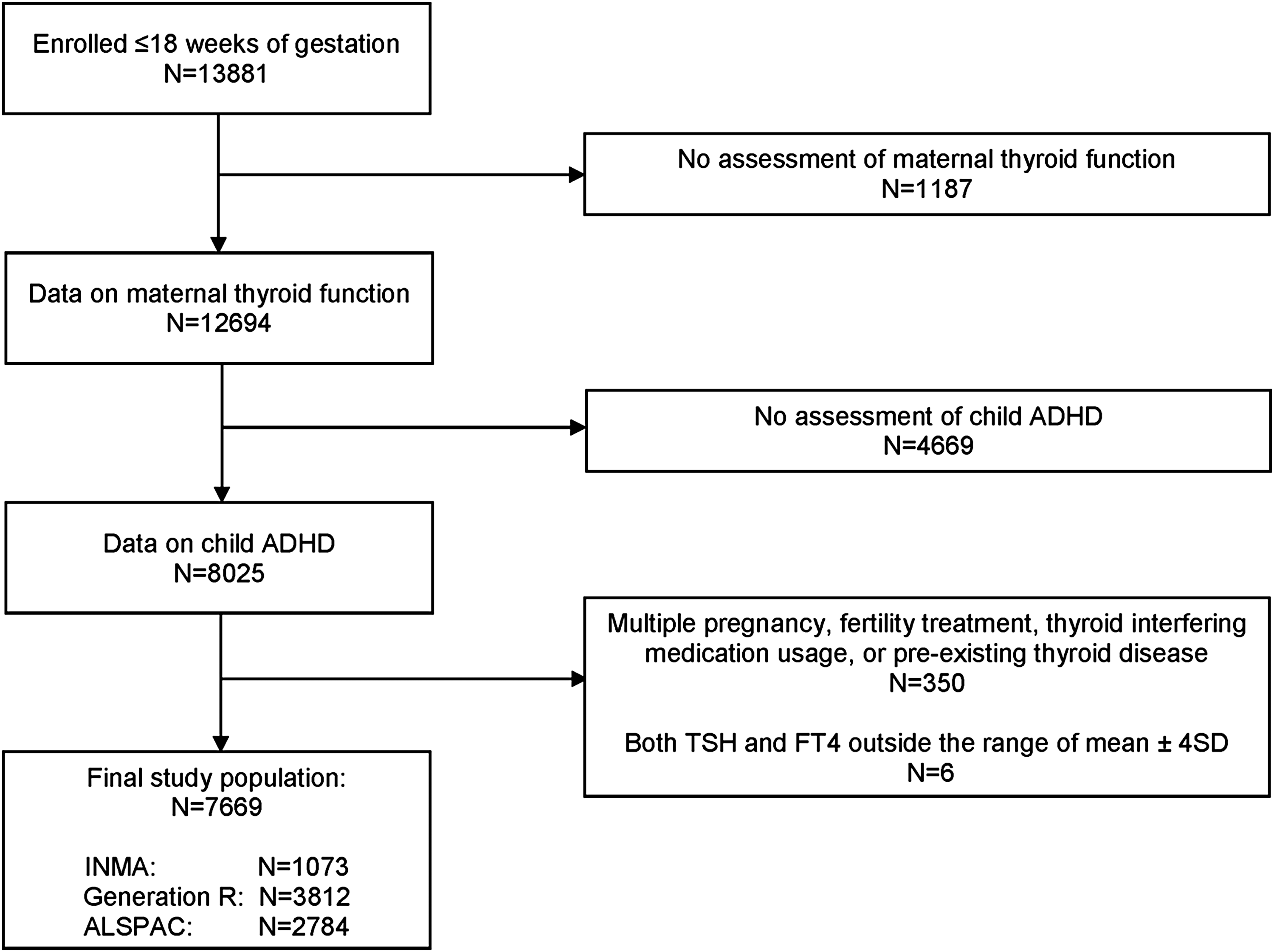
Flowchart of the selection of the study population. ADHD, attention-deficit hyperactivity disorder; ALSPAC, Avon Longitudinal Study of Parents and Children; fT4, free thyroxine; INMA, INfancia y Medio Ambiente; SD, standard deviation; TSH, thyrotropin.
Attention-deficit hyperactivity disorder
fT4 was not associated with ADHD (odds ratio [OR] 1.1, 95% confidence interval [CI 1.0–1.3], p = 0.060; Table 2 and Supplementary Fig. S1). The effect estimate remained similar after excluding TPOAb-positive women. There was no effect modification by gestational age (p for interaction term = 0.581). While there was no indication of significant effect modification by child's sex (p for interaction term = 0.144), we did observe a significant association in girls only (OR 1.3 [CI 1.0–1.7], p = 0.042; for boys: OR 1.1 [CI 0.9–1.3], p = 0.352). The association in girls became stronger after excluding TPOAb-positive women from mother–child pairs, of which TPOAb status was known (from OR 1.2 [CI 0.9–1.7], p = 0.187 to OR 1.5 [CI 1.1–2.1], p = 0.020), while the effect estimate remained similar in boys.
Association of Maternal Free Thyroxine and Thyrotropin Concentrations During Pregnancy with Child Attention-Deficit Hyperactivity Disorder and with an Attention-Deficit Hyperactivity Disorder Symptom Score ≥90th Percentile
Reported ORs and CIs are increase in odds per SD of log-transformed fT4 or TSH. Analyses were performed using logistic regression and adjusted for gestational age at blood sampling, maternal education, maternal ethnicity/country of birth, age, parity, smoking during pregnancy, prepregnancy body mass index, and child sex. Cohort-specific estimates were also adjusted for child age at ADHD ascertainment and subcohort in INMA.
n = children with ADHD, N = children without ADHD.
n = children with a symptom score ≥90th percentile, N = children with a symptom score <90th percentile.
A quadratic term (TSH SD score2) was added to the model, indicating a nonlinear association.
CI, 95% confidence interval; OR, odds ratio.
TSH was not associated with ADHD (OR 0.9 [CI 0.8–1.1], p = 0.385; Table 2 and Supplementary Fig. S1) and the effect estimate remained similar after excluding TPOAb-positive women. There was no effect modification by gestational age (p for interaction term = 0.757; Table 3) or child sex (p for interaction term = 0.474).
Pooled Association of Maternal Free Thyroxine and Thyrotropin Concentrations During Pregnancy with Child Attention-Deficit Hyperactivity Disorder and with an Attention-Deficit Hyperactivity Disorder Symptom Score Above the 90th Percentile, Stratified by Tertile of Gestation
Reported ORs and CIs are increase in odds per SD of log-transformed fT4 or TSH. Analyses were performed using logistic regression and adjusted for gestational age at blood sampling, maternal education, maternal ethnicity/country of birth, age, parity, smoking during pregnancy, prepregnancy body mass index, and child sex.
A quadratic term (fT4 SD score2) was added to the model, indicating a nonlinear association.
ADHD symptom score above the 90th percentile
There was no association of fT4 with an ADHD symptom score above the 90th percentile (OR 1.0 [CI 0.9–1.1], p = 0.554; Table 2 and Supplementary Fig. S1) and no indication of effect modification by child's sex. We did identify a possible effect modification by gestational age for the association of fT4 with symptoms above the 90th percentile (p for interaction term = 0.013); a higher fT4 was associated with a significant 1.2-fold higher risk of ADHD symptoms above the 90th percentile in the early-pregnancy fT4 measurements ([CI 1.0–1.4], p = 0.027; <11.8 weeks), while a higher fT4 was associated with a lower risk in mother–child pairs with relatively late-pregnancy fT4 measurements (OR 0.9 [CI 0.7–1.0], p = 0.045; Table 3). The effect estimates remained similar after excluding TPOAb-positive women.
There was no association of TSH with an ADHD symptom score above the 90th percentile (OR 0.9 [CI 0.9–1.0], p = 0.073; Table 2 and Supplementary Fig. S1) and no indication of effect modification by child's sex. We identified a possible effect modification by gestational age for the association of TSH with symptom scores above the 90th percentile (p for interaction term = 0.082). Stratified analyses by tertile of gestational age showed that a higher TSH was associated with a significant 0.8-fold lower risk of ADHD symptoms above the 90th percentile in the relatively early-pregnancy TSH measurements ([CI 0.7–0.9], p = 0.006; Table 3; <11.8 weeks). The effect estimates remained similar after excluding TPOAb-positive women.
ADHD symptoms on a continuous scale
No associations were identified between fT4 or TSH across the full range and the total ADHD symptom score as investigated in each cohort separately (Supplementary Tables S3 and S4).
Discussion
We did not identify an association between fT4 and TSH and ADHD in the overall study population. There was inconsistent evidence that the associations investigated were different depending on gestational age.
While both low and high–normal maternal fT4 concentrations have been associated with adverse outcomes related to fetal brain development (3 –11), the role of thyroid hormone in the development of ADHD is unknown. Exposure to high thyroid hormone concentrations might contribute to the etiology of this disorder, since individuals with generalized resistance to thyroid hormone were shown to be more prone to meet the criteria for ADHD than subjects without this condition (16). Fetuses without the mutation but born to a mother with RTHβ have reduced sensitivity to thyroid hormone compared with fetuses born to mothers without RTHβ (56). The reduced sensitivity to thyroid hormone was explained by increased deiodinase 3 (D3) expression in the anterior pituitary. Other studies have also shown that untreated hyperthyroidism during pregnancy may lead to persistent changes in the thyroid function of the child (57,58).
In addition, children born to mothers with RTHβ were found to have lower birth weight (59). Lower birth weight and small size for gestational age, which has been already shown to be associated with a higher fT4 concentration in pregnancy in Generation R and INMA (60,61), could be on the causal pathway to ADHD symptomatology (62).
Thus far, the results of studies on the association between maternal thyroid function and child ADHD are inconsistent. While one study reported a positive association between fT4 and ADHD symptoms (26), other studies either report no association (23,24,28,30) or a negative association (27,29,31). Likewise for TSH, studies show a positive association between TSH and attention problems or ADHD symptoms (23 –25), no association (26 –29,31), or a possible protective effect of a higher TSH concentration (30).
There may be different explanations as to why some studies found an association between fT4 or TSH and ADHD, while others did not. First of all, although fT4 and TSH reflect thyroid status, TSH is a more sensitive indicator of thyroid autoimmunity, which is associated with ADHD (54). Second, the inconsistent study results may also be explained by several methodological points. ADHD symptoms were assessed differently between studies, with some earlier studies using tools that did not include an extensive set of items as the DSM-IV uses to classify ADHD. In addition, ADHD was defined differently across studies—by medical diagnosis (26,31), symptoms on a continuous scale (24,27,30), or by ADHD or inattention symptom cutoffs (23,25,28,29)—hence the comparability between studies is limited. The latter studies did not use a symptom score above the 90th percentile, as used in our study. Third, iodine status may also explain part of the heterogeneity between studies (63). Results in a small study population showed that ADHD prevalence was higher in an iodine-deficient area than in an iodine-sufficient area (64).
The importance of maternal thyroid hormone for the fetal brain changes throughout pregnancy. Before the fetal thyroid is functionally mature at 18–20 weeks of gestation, the fetus depends on thyroid hormone from the mother (1). During the second half of pregnancy, the maternal thyroid remains an important source, but to a lesser extent as considerable amounts of thyroid hormone are produced by the fetus itself (2).
We investigated whether the effect of maternal thyroid hormone on ADHD (symptoms) differed by gestational age. The proportion of mother–child pairs was not equally distributed across the different groups of gestational age; in roughly the first 12 weeks of gestation, two thirds of the mother–child pairs were from the ALSPAC cohort. Stratified analyses showed that the association of higher fT4 with a higher risk of symptom score above the 90th percentile was prominent in roughly the first 12 weeks of gestation, but not thereafter. Given these findings and the physiological interrelation between fT4 and TSH, we could also observe that a higher TSH was associated with a lower risk of symptom scores above the 90th percentile only in the first trimester. However, there was no significant interaction with gestational age in the association of fT4 or TSH with ADHD. From our analyses, we therefore have no strong evidence for differential effects by gestational age.
Interestingly, in the current study, a higher maternal fT4 concentration during pregnancy was associated with a higher risk of ADHD in girls only. Differential effects of thyroid hormone on brain-development-related outcomes by sex have been reported previously (23,31), and it is well known that ADHD is more often diagnosed in males. While it remains unclear why this association may be sex-specific, it is known that child sex modifies the thyroidal response to human chorionic gonadotropin (hCG); women pregnant with a female fetus have a higher thyroidal response to high hCG concentrations, resulting in lower TSH and higher fT4, than those with a male fetus (65). However, our results have to be interpreted with caution as no significant interaction with sex was found. Further studies are needed to replicate if there are sex-specific effects of thyroid hormone on brain development.
Observational studies showed that both low and high maternal thyroid function are associated with lower child IQ and lower gray matter volume (3,5,25). Randomized trials thus far failed to show a benefit of levothyroxine treatment in pregnant women with subclinical hypothyroidism or hypothyroxinemia on child IQ (32,33), but these trials have been limited by a suboptimal timing and dose of treatment (66). Behavioral problems such as ADHD could also be considered an outcome that may reflect suboptimal fetal brain development during pregnancy. Our study shows no association between maternal thyroid function and child ADHD. However, owing to the observational design of this study, we cannot make statements on what the potential effects of this treatment on behavior problems in children would be.
We were able to combine data from three large cohorts, enabling us to investigate associations between thyroid function and ADHD in a large number of mother–child pairs. All three cohorts used the DSM, internationally applied, diagnostic criteria, which are the most used clinically for diagnosing psychiatric disorders. Using individual-participant data instead of aggregate data facilitated the use of consistent inclusion and exclusion criteria and standardized statistical analyses across cohort studies. Combining individual participant data into a meta-analysis offers further advantages over individual studies. Irrespective of a replication of findings as found in individual studies, findings from meta-analyses enrich our knowledge on the theory tested and increase confidence in generalization.
In our study, ADHD occurred in only 3% of children, which may have been a low proportion in which to detect an association. This prevalence was lower than that reported in children and adolescents in a systematic review (13). The prevalence of ADHD in Generation R was lower than previously reported due to a different sample size, and we did not report a weighted prevalence to represent the full sample with CBCL1½–5 data (43). Prevalence estimates are known to vary widely by individual studies. Part of this variability may be explained by the diagnostic criteria used to define ADHD, the method used to assess ADHD symptoms, the incorporation of functional impairments as part of the definition of ADHD, and possibly also by social economic status of the population (13).
In our study, mother–child pairs with a lower social economic status (e.g., lower maternal educational level and less often native or Caucasian) were more likely to be lost to follow-up. We accounted for potential differential loss to follow-up by applying inverse probability weighting. To increase statistical power, we used the highest 10% of ADHD symptoms as a secondary outcome. It should be noted that this extra cutoff was arbitrarily chosen and has not been validated.
A limitation of this study is that ADHD symptoms were assessed at different ages using different methods, including inconsistency in the type of assessor used by the different cohorts, which may have contributed to heterogeneity in results. The heterogeneity by the latter was shown by a recent study showing that maternal thyroid function was associated with teacher-rated ADHD symptoms, but not with parental ratings (29). Due to low-to-moderate agreement between teacher and parental observations, multi-informant assessment has been recommended to understand the behavior of a child in different settings (67,68); this was most closely adhered to in ALSPAC. We did not have the opportunity to rescore the data that were collected of a sample of children using the three methods. In addition, we had no data on clinical diagnosis of ADHD by a physician, which may have caused outcome misclassification.
In conclusion, the results of the current study do not show an association between maternal thyroid function and ADHD in the overall study population. As the etiology of ADHD as well as the potential role of thyroid hormone availability remains poorly understood, further studies are warranted.
Footnotes
Acknowledgments
We would like to thank the participants of all cohorts for their generous collaboration; Professor Scott Nelson, University of Glasgow, United Kingdom, for the ALSPAC thyroid measurements, which were funded by the Chief Scientist Office, Scotland (ETM 97/0357/130024782); Ane M. Castilla of the Public Health Laboratory of Bilbao, Spain, for the thyroid measurements in INMA, and Professor Dr. Yolanda de Rijke, Department of Clinical Chemistry, Erasmus MC, University Medical Center, the Netherlands, for design and measurements of the thyroid measurements in Generation R.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
EUthyroid Project: European Union's Horizon 2020 research and innovation programme under grant agreement No. 634453.
INMA, Spain: This study was funded by grants from EU (FP7-ENV-2011 cod 282957, HEALTH.2010.2.4.5–1, and 733206) and Spain: Instituto de Salud Carlos III (Red INMA G03/176; CB06/02/0041; FIS-FEDER: PI041436, PI05/1079, PI06/0867, PI081151, FIS-PI09/00090, PI11/01007, PI11/02591, PI11/02038, PI13/1944, PI13/2032, PI14/00891, PI14/01687, PI16/1288, and PI17/00663; Miguel Servet-FEDER CP11/00178, CP15/00025, and CPII16/00051; and Miguel Servet-FSE MS13/00054, MSII16/00051, and CPII18/00018), Generalitat Valenciana: FISABIO (UGP 15–230, UGP-15-244, and UGP-15-249), Alicia Koplowitz Foundation 2017, Generalitat de Catalunya-CIRIT 1999SGR 00241, Fundació La marató de TV3 (090430), Department of Health of the Basque Government (2005111093 and 2009111069), and the Provincial Government of Gipuzkoa (DFG06/004 and DFG08/001).
Generation R, The Netherlands: The Generation R Study is conducted by the Erasmus Medical Center in close collaboration with the Faculty of Social Sciences of the Erasmus University Rotterdam, the Municipal Health Service Rotterdam area, Rotterdam, and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR-MDC), Rotterdam. The Generation R Study is supported by the Erasmus Medical Center, Rotterdam, the Erasmus University Rotterdam, the Netherlands Organization for Health Research and Development (ZonMw), the Netherlands Organization for Scientific Research (NWO), and the Ministry of Health, Welfare and Sport. A grant from the Sophia Children's Hospital Research Funds supports the neurodevelopmental work on thyroid. R.P.P. is supported by a clinical fellowship from ZonMw, project number 90700412. H.T. is supported by a VICI grant with personal grant number 016.VICI.170.200.
ALSPAC, United Kingdom: We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which include interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists, and nurses. The UK Medical Research Council and Wellcome (Grant ref: 102215/2/13/2) and the University of Bristol currently provide core support for ALSPAC. Data collection is funded from a wide range of sources, which are detailed on the ALSPAC website. The publication is the work of the authors and Mònica Guxens will serve as guarantor for the contents of this article.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Figure S1