
Abstract
Background:
Based on the new TNM classification, differentiated thyroid carcinomas with extrathyroidal extension (ETE) into the strap muscles are designated as T3b. The current study analyzed the clinical significance of this new stage in patients with papillary thyroid cancer (PTC).
Subjects and Methods:
This retrospective cohort study included 4045 eligible PTC patients. The patients were divided into four groups according to the extent of ETE: no ETE, ETE into perithyroidal tissue, T3b (ETE into the strap muscles), and ETE beyond the strap muscles. Differences in the clinical characteristics and prognosis of the four groups were assessed.
Results:
Of these 4045 patients, 2300 (56.9%) had no ETE, 1004 (24.8%) had ETE into perithyroidal tissue, 371 (9.2%) had ETE into the strap muscles, and 370 (9.1%) had ETE beyond the strap muscles. Tumor size, multifocality, lymph node metastasis (LNM), distant metastasis (DM), recurrence, and recurrence-free survival (RFS) between patients with ETE into perithyroidal tissue and patients without ETE did not show differences, but significant differences were observed between patients with T3b and patients without ETE, and only patients with ETE beyond the strap muscles had significantly worse overall survival (OS) than the other three groups. However, T3b did not independently predict worse RFS in univariable and multivariable analyses.
Conclusions:
T3b, distinguished from minimal ETE, may be related to larger tumor size, higher prevalence of multifocality, LNM, DM, recurrence, and worse RFS than no ETE, but it may not affect OS and may not independently predict recurrence in PTC patients.
Introduction
Extrathyroidal extension (ETE) of thyroid carcinoma, referring to the invasion of the primary tumor into adjacent tissues beyond the gland (1,2), is a well-established factor that is associated with adverse outcomes in patients with papillary thyroid carcinoma (PTC) (3 –5). The presence of ETE, a staging variable, plays a prominent role in almost all staging systems due to its importance in prognosis (6). On histology, ETE has been classified based on the extent of invasion; minimal ETE involves the perithyroidal soft tissue or sternothyroid muscles, whereas extensive ETE involves extension to the subcutaneous soft tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve (7).
The eighth edition of the American Joint Committee Cancer (AJCC) staging system for differentiated thyroid cancer uses the same definitions for the T, N, and M categories (8). However, minimal ETE was removed from the definition of pT3 disease because there was little evidence that it is an independent predictor of persistence/recurrence or survival (9,10). Instead, the T3 category has been divided into two subgroups: (i) T3a is defined as tumors greater than 4 cm limited to the thyroid, and (ii) T3b is defined as a tumor of any size demonstrating gross ETE invading only a strap muscle (Table 1). The new staging system distinguishes T3b from minimal ETE for the first time. However, the clinical significance of T3b has not been independently assessed and validated.
Comparison of American Joint Committee Cancer Seventh and Eighth Edition Classification System for Differentiated Thyroid Cancer
ETE, extrathyroidal extension.
Hence, the present study sought to investigate the clinicopathologic characteristics of patients with T3b, aiming to identify the clinical significance of this feature in PTC.
Subjects and Methods
Study population
The study population was identified from a retrospective database review of all patients undergoing surgery for thyroid cancer from December 2011 to December 2016 at our institution, and clinical information was retrospectively collected for each patient from the medical system, including the patients' baseline characteristics, intraoperative data, postoperative recovery, and pathological examination findings. The inclusion criteria were PTC patients who underwent total or hemithyroidectomy and neck dissection, including prophylactic central lymph node (LN) dissection, therapeutic central LN dissection, and/or therapeutic lateral LN dissection from 18 to 80 years of age and had complete clinical data and follow-up information. Individuals who were diagnosed with another confirmed pathological disease or with positive resection margins and those with incomplete medical records were excluded. Based on the inclusion and exclusion criteria, 4045 subjects were eligible for this retrospective analysis.
Based on our surgical and histopathologic findings, the patients were divided into four groups: no ETE, ETE into perithyroidal tissue, T3b (ETE into the strap muscles without extension beyond the strap muscles, i.e., sternohyoid, sternothyroid, thyrohyoid, or omohyoid muscles), and ETE beyond the strap muscles (i.e., subcutaneous soft tissue, larynx, trachea, esophagus, recurrent laryngeal nerve, or prevertebral fascia, or encasing the carotid artery or mediastinal vessels). Recurrent/persistent disease referred to any newly detected tumor or lymph node metastasis (LNM) after the initial operation and/or the appearance of metastatic lesions in the lungs, bones, and/or brain identified by imaging examination or abnormal thyroglobulin (Tg) levels or rising anti-Tg antibody levels in the absence of localizable disease for patients with total thyroidectomy, according to the criteria of the 2015 ATA guidelines (11). Recurrence-free survival (RFS) was defined as the time from the initial surgery to the latest follow-up or the first evidence of recurrence. Neck ultrasound examination and measurement of serum-free triiodothyronine, serum-free thyroxine, thyroid-stimulating hormone, Tg, and anti-Tg antibody concentrations are routinely performed 1, 3, 6, and 12 months after surgery during the first year and then at yearly intervals. The follow-up time of the study population was 12–63 months, and the median follow-up time was 32 months. The study protocol was approved by the Institutional Review Board of West China Hospital of Sichuan University, and patient approval or informed consent was required for review of the patients' medical records.
Surgical treatment
At our institution, we perform total or hemithyroidectomy for tumors measuring ≤10 mm according to the conditions of the contralateral lobe of the thyroid gland on ultrasound. Total thyroidectomy is generally performed for patients with tumors >10 mm in size. Prophylactic ipsilateral central LN dissection is routinely performed in PTC patients. The contralateral central LN is dissected when the pretracheal or prelaryngeal LN is involved in intraoperative frozen sections, and dissection of the lateral neck is performed only in patients with suspicious LN metastases on ultrasound or confirmed lateral neck nodal metastases based on preoperative fine-needle aspiration biopsy. Central LN dissection extends superiorly to the hyoid bone, inferiorly to the innominate vein, laterally to the carotid sheaths, and dorsally to the prevertebral fascia. Lateral LN dissection was performed using a modified radical operation that involved complete removal of level II through IV lateral cervical LNs. Level I and V dissection was not performed if there was no clinical evidence of metastases.
Statistical analysis
Statistical analysis was performed using SPSS software, version 20.0 (SPSS, Chicago, IL). Continuous variables are expressed as the means ± standard deviations or the medians, and differences were compared using Student's t-test, ANOVA, or the rank test. Categorical variables are presented as numbers, and differences were compared using the chi-square test or Fisher's exact chi-square test. A scatter diagram was used to analyze the tumor size among the four groups. Logistic and Cox regression analyses were used to quantify the intensity of the presence or absence of certain characteristics between the four groups. The risk estimates, including hazard ratios (HRs), odds ratios (ORs), and relative confidence intervals (CIs), were calculated. The Kaplan–Meier method and log-rank test were used to analyze time-dependent variables. A p-value <0.05 was considered indicative of statistical significance.
Results
Key clinical characteristics of patients according to ETE
The clinicopathologic characteristics of the 4045 patients with PTC included in the study population are reported in Table 2. Of these 4045 patients, 2300 (56.9%) had no ETE, 1004 (24.8%) had ETE into perithyroidal tissue, 371 (9.2%) had ETE into the strap muscles (T3b), and 370 (9.1%) had ETE beyond the strap muscles. The key clinical characteristics of mean tumor size, multifocality, LNM, and distant metastasis (DM) were compared among these four groups. The results are shown in Figure 1 and Tables 3 –5.
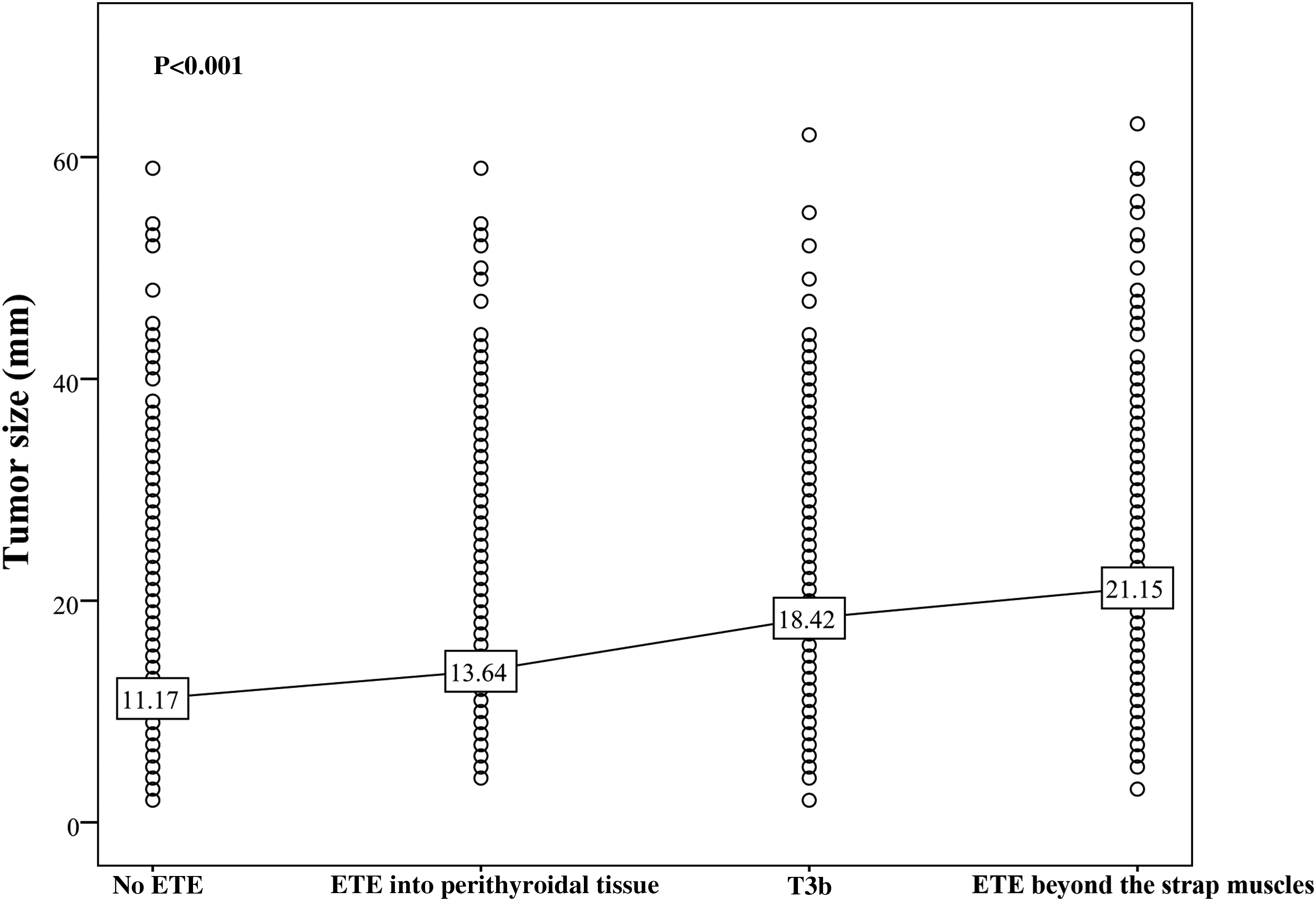
The average tumor size in the four groups according to the extent of ETE (p < 0.001). (ETE into perithyroidal tissue vs. no ETE, p = 0.112; T3b vs. no ETE, p = 0.009; ETE beyond the strap muscles vs. no ETE, p < 0.001.) ETE, extrathyroidal extension.
The Baseline Demographics and Tumor Characteristics of Patients with Papillary Thyroid Carcinomas
Statistically significant difference.
BMI, body mass index; C/LLND, central/lateral lymph node dissection; DM, distant metastasis; LNM, lymph node metastasis; RAI, radioiodine; SD, standard deviation; Tg, thyroglobulin; TT, total thyroidectomy.
Number and Portion of Multifocality According to Degree of Extrathyroidal Extension
Statistically significant difference.
Number and Portion of Lymph Node Metastasis According to Degree of Extrathyroidal Extension
Statistically significant difference.
Number and Portion of Distant Metastasis According to Degree of Extrathyroidal Extension
Statistically significant difference.
The average tumor size distributions based on the extent of ETE are presented in Figure 1. The mean tumor diameters were significantly different at 11.17 ± 8.11 mm in the group without ETE, 18.42 ± 10.61 mm in the group with T3b, and 21.15 ± 9.88 mm in the group with ETE beyond the strap muscles (T3b vs. no ETE, p = 0.009; ETE beyond the strap muscles vs. no ETE, p < 0.001). However, the mean tumor diameter of 13.64 ± 9.61 mm in the group with ETE into the perithyroidal tissue was similar to that in the group without ETE (p = 0.112).
Multifocality occurred in 27.2% of patients with PTC without ETE and in 27.3% of patients with ETE into perithyroidal tissue (p = 0.532; HR: 1.04). However, when comparing patients with T3b with those without ETE, the proportions of multifocality significantly differed at 33.4% and 27.1%, respectively (p = 0.033; HR: 1.64). In addition, significant differences were also observed between patients with ETE beyond the strap muscles and patients without ETE (36.2% vs. 27.1%; p < 0.001; HR: 1.82) (Table 3).
LNM was present in 50.9% of patients at the time of surgery. The prevalence of LNM (50.0%) in patients with ETE into perithyroidal tissue was similar to the frequency of LNM (45.2%) in patients without ETE (p = 0.179; HR: 1.12). However, individuals with T3b (65.2%) and those with PTC with ETE beyond the strap muscles (74.1%) were at a higher risk for LN involvement than those without ETE (p = 0.011; HR: 1.94 and p < 0.001; HR: 3.67) (Table 4).
DM was identified in 26 (0.64%) patients in our study population, all of whom presented with pulmonary metastasis. There were no significant differences between patients with ETE into perithyroidal soft tissue and patients without ETE (p = 0.450; HR: 0.88). However, the proportions of patients with DM significantly differed in the groups with T3b and ETE beyond the strap muscles compared with the group without ETE (p < 0.001; HR: 9.47 and p < 0.001; HR: 29.76) (Table 5).
Prognosis stratified by the degree of ETE
Recurrence (median duration, 32 months; interquartile range, 12–63 months) occurred in 22.5% of our patients. In 912 patients with primary PTC recurrence, 470 (20.4%) and 214 (21.3%) patients were included in the groups without ETE and ETE into perithyroidal tissue, respectively, and no significant differences were observed between the two groups (p = 0.243; HR: 1.15). However, the groups with T3b (25.9%) and ETE beyond the strap muscle (35.7%) exhibited a higher rate of recurrence than the group without ETE (p = 0.017; HR: 1.89 and p < 0.001; HR: 2.94) (Table 6). RFS curves between all four groups are shown in Figure 2. Similarly, differences in RFS between patients with ETE into perithyroidal tissue and patients without ETE did not reach significance (p = 0.054). RFS was significantly worse in patients with T3b and patients with ETE beyond the strap muscles than in patients without ETE (p = 0.002; p < 0.001), and significant differences were found between patients with T3b and those with ETE into perithyroidal tissue (p = 0.032).
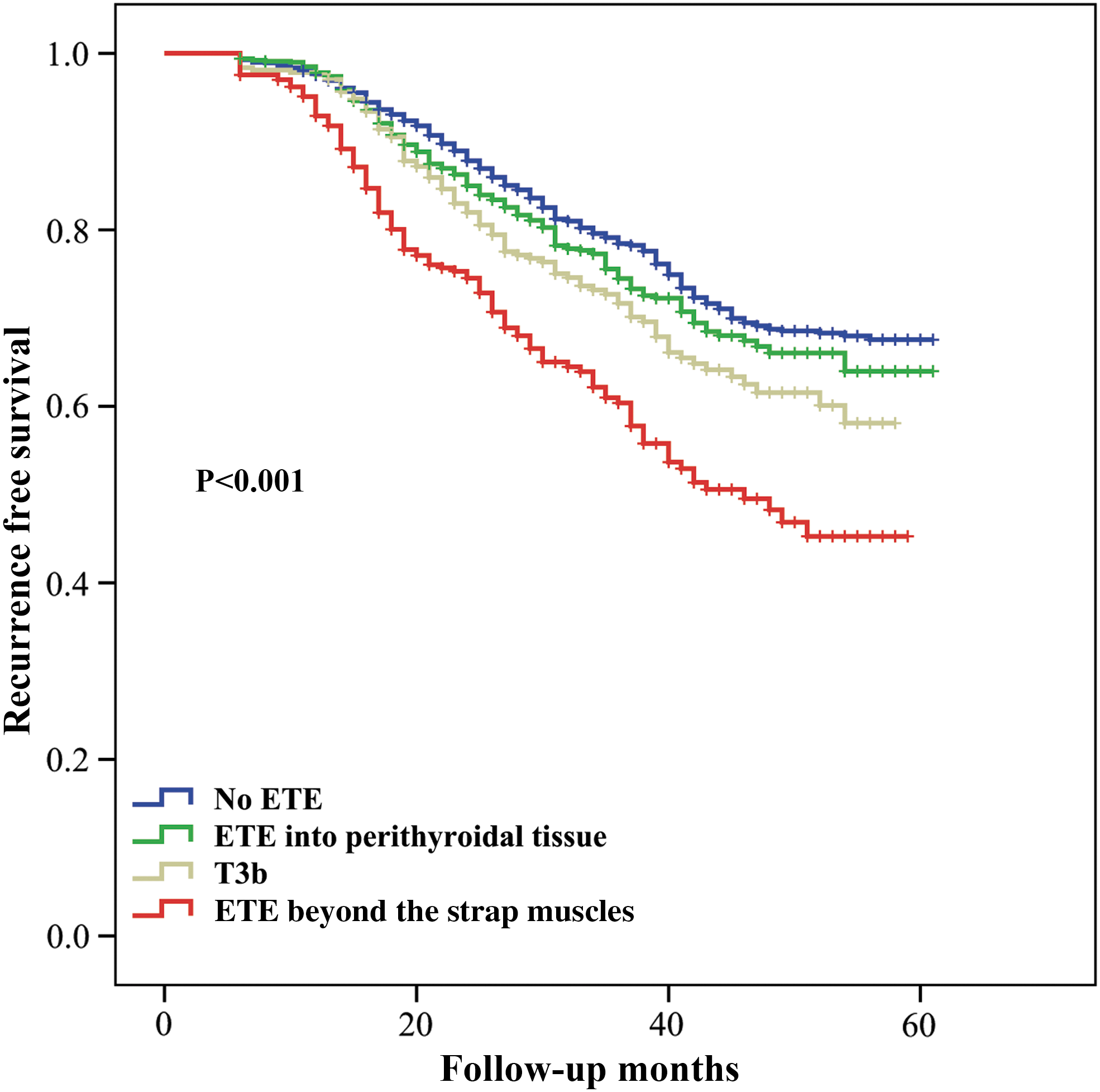
Kaplan–Meier survival curves for recurrence-free survival according to extent of ETE (p < 0.001). (ETE into perithyroidal tissue vs. no ETE, p = 0.054; T3b vs. no ETE, p = 0.002; ETE beyond the strap muscles vs. no ETE, p < 0.001; T3b vs. ETE into perithyroidal tissue, p = 0.032.) Color images are available online.
Number and Portion of Recurrence According to Degree of Extrathyroidal Extension
Statistically significant difference.
Cancer-specific deaths occurred in 0.22% of patients at the latest follow-up. No significant differences were observed in the group of patients with ETE into perithyroidal tissue (0.10%) and the group of patients with T3b (0.27%) (p = 0.433; HR: 0.81 and p = 0.104; HR: 1.28) compared with the group of patients without ETE (0.13%). However, the group of patients with ETE beyond the strap muscles (1.08%) exhibited a higher rate of cancer-related deaths than the group of patients without ETE (p = 0.012; HR: 3.76) (Table 7). Patients with ETE beyond the strap muscles had significantly worse overall survival (OS) than patients in the other three groups, which did not differ significantly from one another (p = 0.757, ETE into perithyroidal tissues vs. no ETE; p = 0.572, T3b vs. no ETE; p = 0.010, ETE beyond the strap muscles vs. no ETE) (Fig. 3).
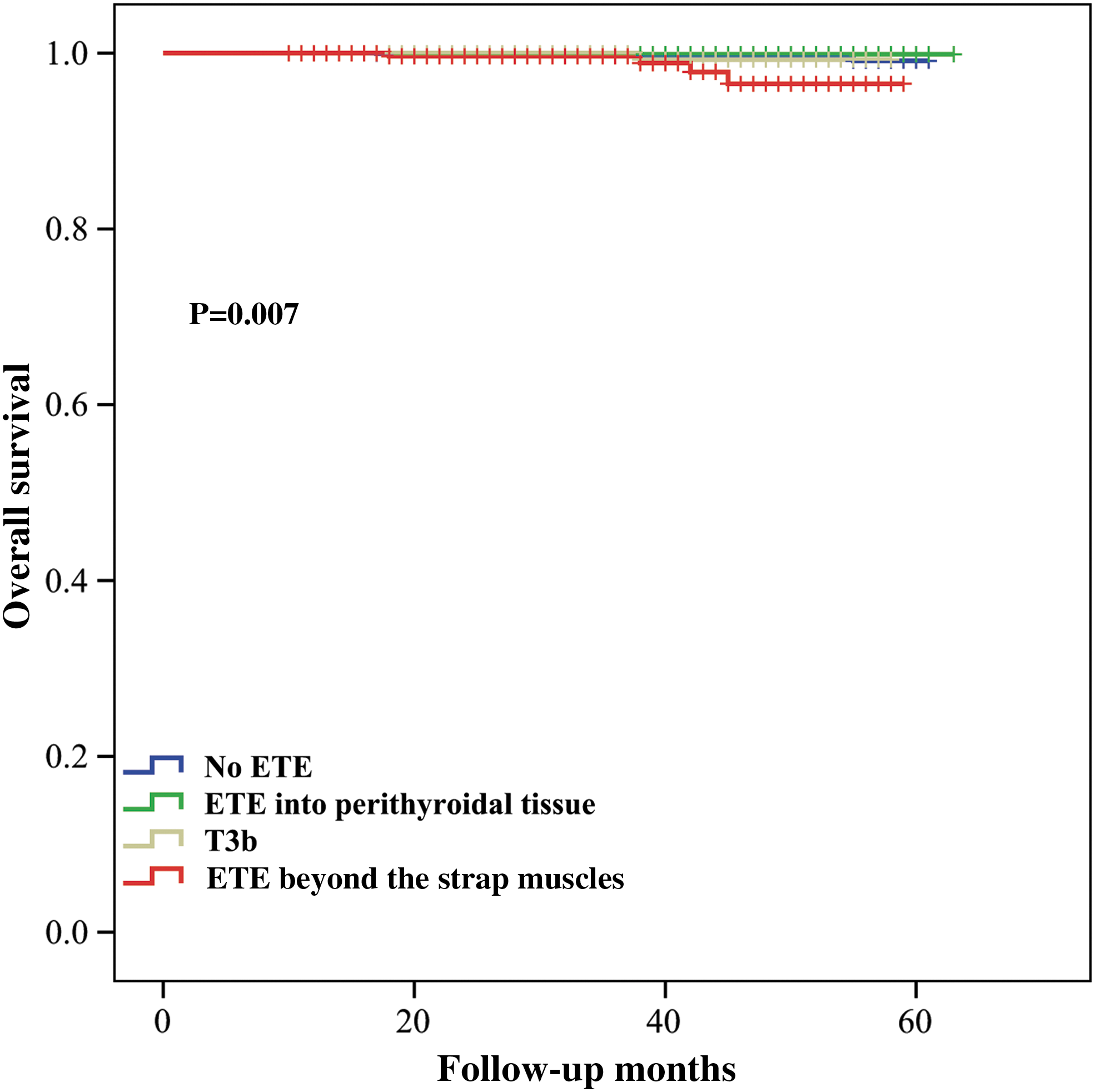
Kaplan–Meier survival curves for overall survival according to extent of ETE (p = 0.007). (ETE into perithyroidal tissue vs. no ETE, p = 0.757; T3b vs. no ETE, p = 0.572; ETE beyond the strap muscles vs. no ETE, p = 0.010.) Color images are available online.
Overall Survival According to Degree of Extrathyroidal Extension
Statistically significant difference.
The parameters associated with recurrence
On univariable analysis, the following seven factors significantly increased the risk of recurrence: age at diagnosis ≥55 years, male sex, body mass index >24 kg/m2, tumor dimensions >20 mm, multifocality, LNM, and radioiodine therapy (all p < 0.05). However, T3b was not associated with worse RFS (p = 0.107). The factors that continued to be independently related to recurrence were age at diagnosis ≥55 years (OR 1.313 [CI 1.129–1.676], p = 0.028), male sex (OR 1.798 [CI 1.406–2.300], p < 0.001), tumor dimensions >20 mm (OR 1.488 [CI 1.204–1.922], p = 0.012), and LNM (OR 2.110 [CI 1.771–3.228], p < 0.001) (Table 8).
Univariate and Multivariate Analysis of the Parameters That Could Be Associated with Recurrence
Statistically significant difference.
CI, confidence interval.
Discussion
PTC is the most common type of thyroid cancer and has an excellent prognosis, with a less than 10% cancer-related mortality rate (12). ETE is observed in 5–45% of patients with PTC and has been suggested to be associated with an increased risk of LN metastasis, local recurrence, and decreased survival rate (5,13,14). In the sixth and seventh editions of the AJCC TNM staging system (15,16), T3 disease included any tumor with minimal ETE (such as extension to the sternothyroid muscles or perithyroidal soft tissue). Several studies have attempted to clarify the impact of minimal ETE on the prognosis of PTC (17 –19). There is no strong evidence that minimal ETE predicts RFS, and most studies have suggested that ETE is not an independent predictor of mortality (9,10). For this reason, in the eighth edition of the AJCC TNM staging manual, ETE invading only the strap muscles replaced minimal ETE as a determinant of T3b disease, whereas tumors with only perithyroidal soft tissue invasion no longer impacted either the T stage or overall stage regardless of the patient's age. The negative impact of ETE invading major structures (T4 disease in the AJCC TNM staging system) on recurrence and mortality is widely accepted (13,20). However, to the best of our knowledge, a detailed analysis of the prognostic significance of T3b has not yet been performed.
In the studies by Amit et al. (21) and Park et al. (22), the investigators analyzed 2084 and 3174 patients with differentiated thyroid cancer over a long-term follow-up and demonstrated that T3b did not affect disease-specific mortality but provided information about long-term recurrence. In addition, they reported that patients with T3b shared the same recurrence rates with patients with ETE into perithyroidal tissues, and those with PTC with ETE into perithyroidal tissues had a significantly worse RFS than those with PTC without ETE. Few other studies to date have addressed the importance of distinguishing T3b from microscopic ETE, except for the abovementioned studies. Hence, we repeated this study at a different center and with a different patient population, comprehensively testing these parameters in patients with PTC.
We conducted a large-scale epidemiological study in the Chinese population, where the rate of T3b is 9.2%. A high proportion of T3b was found in our population compared with a cohort from the United States (3%) (21), but our findings are similar to data obtained in a Korean population that ranged from 8.2% to 12.5% (17,22,23). Based on these results, which are similar to the findings reported by Amit et al. (21) and Park et al. (22), our data show significant differences between T3b and no ETE in terms of recurrence and RFS. Only patients with ETE beyond the strap muscles had significantly worse cancer-specific death rates and OS, and T3b did not predict worse RFS in univariable and multivariable analyses in our study. Amit et al. and Park et al. explained that this finding might be because it is more difficult to clear disease with posterolateral ETE than with anterolateral ETE because of the location of the disease in relation to critical laryngotracheal structures. Contrary to the findings in the studies by Amit et al. and Park et al., but consistent with studies by Moon et al. (24) and Ito et al. (25), we found that RFS in patients with ETE into perithyroidal tissues was almost identical to that in patients without ETE. Moreover, patients with T3b presented higher recurrence rates that differed significantly from patients with ETE into perithyroidal tissues. Furthermore, our study investigated the relationship of key clinical features among four groups compared with patients without ETE. The results show that patients with ETE into perithyroidal tissues had similar tumor sizes, multifocality, LNM, and DM relative to those with no ETE. However, patients with T3b presented a larger tumor size and higher risks of multifocality, LNM, and DM than those in the no-ETE or ETE into perithyroidal tissue groups. Therefore, T3b appears to be associated with more aggressive clinical behavior than other forms of ETE.
For the sake of improved postoperative risk stratification, the T staging has been constantly changed and subdivided during the past decades. In terms of N staging, in the seventh edition of the AJCC Staging Manual, regional LNs were classified as N0 (no regional LN metastasis), N1a (metastasis to level VI, which includes the pretracheal, paratracheal, prelaryngeal, and Delphian LNs), or N1b (metastasis to unilateral, bilateral, or contralateral LNs at cervical LN levels I, II, III, IV, or V; or retropharyngeal LNs; or level VII superior mediastinal LNs). The major change in the N category is related to the upper mediastinal LNs (cervical level VII), which has been reassigned to the N1a (central neck) category in the eighth edition of the AJCC Staging Manual (26). In a previous study, our data revealed that metastatic LN invasion in the capsule or organ had significant prognostic value for predicting the risk of recurrence (27). However, the extent of metastatic extranodal invasion, such as no invasion, capsular invasion, and invasion of perithyroidal soft tissue, is not considered in the seventh or eighth edition of the AJCC Staging Manual. Thus, the definitions for regional LN categories may need to be divided into subgroups similar to thyroidal PTC lesions, except for N1a and N1b, to refine risk stratification in the future.
Inevitably, there are still several potential limitations to this study. First, the retrospective data collection in this study design is subject to well-known limitations and there is the possibility of type I error in certain indicators because the p-value is very close to 0.05. Second, our study analyzed data from a limited follow-up period (12–63 months; median, 32 months). Fortunately, the RFS and OS curves revealed significant differences due to the large group of patients, and we will follow these patients continually and determine the clinical significance of the aforementioned findings in the future. Third, multicenter validation to verify the findings is needed because single-center verification may not be sufficiently accurate. However, excluded patients with unclear records only account for 0.30% (N = 12) in our study population, and thus, there is a low risk of selection bias and the large sample size is a major strength of the present study.
In conclusion, T3b may be associated with a larger tumor size, a higher risk of multifocality, LNM, DM, recurrence, and worse RFS than absent ETE. However, T3b patients have almost identical cancer-specific death and OS rates compared with those without ETE, and T3b did not independently predict worse RFS in PTC patients.
Footnotes
Authors' Contributions
G.L. and R.L. performed research and wrote the first draft. All authors contributed to the design and interpretation of the study and to further drafts.
Author Disclosure Statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Funding Information
This study was supported by grants from the National Key R&D Program of China (2017YF0907504), the National Natural Science Foundation (81702646), the National Post-Doctor Research Project (2018M631086, 2019T120846), Sichuan Province Science and Technology Project of China (2014SZ0005, 2017SZ0139), Sichuan University for youth fund (2017SCU11016), Health and Family Planning Commission of Sichuan Province (17PJ398), Postdoctoral Sustentation Fund of Sichuan University (2017SCU12035), and Post-Doctor Research Project, West China Hospital, Sichuan University (2019HXBH043).