
Abstract
Background:
Remarkable achievements have been made for over two decades by implementing a universal salt iodization policy in China. However, changes in the standards and manufacturing of iodized salt have made it necessary to regularly monitor iodine intake and thyroid function in the population. Therefore, we aimed to evaluate iodine nutritional status using thyroid function and urinary iodine levels in pregnant women via a national survey.
Methods:
Participants included pregnant women enrolled in the 2015 Chinese Adults Chronic Diseases and Nutrition Surveillance (CACDNS). Urinary iodine concentration (UIC) was measured using arsenic and cerium catalysis spectrophotometry. Plasma levels of thyrotropin (TSH), fT4 (free thyroxine), thyroid peroxidase antibodies (TPO-Ab), and thyroglobulin antibodies (TG-Ab) were determined using an automated chemiluminescence immunoassay analyzer.
Results:
UIC was analyzed in a total of 6173 urinary samples collected from pregnant women residing in 31 provinces of China. The median urinary iodine concentration was 146 μg/L. Pregnant women with UIC >250 μg/L had higher TSH levels than those with UIC 120–149 and 150–249 μg/L. After excluding women with positive TPO-Ab and TG-Ab, a total 2097 plasma samples collected from pregnant women during three periods were analyzed for TSH and fT4. The frequency of normal thyroid function in this study was >85%. The most common type of abnormal thyroid function, subclinical hypothyroidism, was similar to the 2010–2012 China Nutrition and Health Surveillance (CNHS), but its prevalence decreased to 6.8% compared with that in the 2010–2012 CNHS. Compared with pregnant women who had UIC <250 μg/L, the prevalence of subclinical hypothyroidism was significantly increased in those with UIC >250 μg/L. Even with UIC levels 120–149 μg/L, the iodine status of Chinese pregnant women in the 2015 CACDNS is acceptable.
Conclusions:
The iodine status of pregnant women is generally adequate, but urinary iodine levels are close to the cutoff for suitable iodine status (150 μg/L). With noniodized salt widely available, continued improvement in monitoring of iodine nutritional status and thyroid function is important in this population.
Introduction
Iodine is an essential trace element, and the synthesis of thyroid hormones, thyroxine and triiodothyronine, requires iodine. Consequently, inadequate intake of iodine can lead to iodine deficiency disorders (IDD) and clinical or subclinical hypothyroidism; these conditions can result in developmental delays and other health problems. Especially during pregnancy and lactation, insufficient iodine intake can irreversibly induce cognitive and motor deficits in fetuses and infants (1 –4).
According to the lower limit of appropriate iodine nutritional status for pregnant women (median urinary iodine concentration [mUIC] <150 μg/L) recommended by international organizations such as the World Health Organization (WHO), the United Nations Children's Fund (UNICEF), and the Iodine Global Network (IGN) (5), pregnant women in two-thirds of Chinese provinces had poor iodine nutritional status (6) in the 2014 surveillance for IDD. In addition, the most recent standard of iodized salt has been changed from one national concentration to three concentrations: 30, 25, and 20 mg/kg (7). Therefore, it is important to investigate the iodine nutritional status of pregnant women. As the physiological function of iodine is mainly for the synthesis of thyroid hormones, it is helpful to include thyroid function in the evaluation of iodine nutritional status.
The first China Nutrition and Health Surveillance (CNHS) was carried out in 1959, and this has subsequently been conducted every 10 years since 1982. However, there was no monitoring of iodine status in pregnant women in the CNHS until 2015. We evaluated the thyroid function of pregnant women using data of the 2010–2012 CNHS and found that the rate of normal thyroid function in this cohort was only 78.1%. However, the sample size was small because of the limited amount of available serum; in addition, UIC values were missing; therefore, there is only limited information for the 2010–2012 CNHS. For the first time, assessment of the iodine status in pregnant women was included in the 2015 Chinese Adults Chronic Diseases and Nutrition Surveillance (CACDNS).
Despite impressive progress in the elimination of IDD over the past two decades, changes in the standards and manufacturing of iodized salt, together with the belief among some people that iodized salt may be harmful, have made it necessary to regularly monitor iodine intake and thyroid function among most pregnant women, a particularly vulnerable population. The 2015 CACDNS made this possible via collection of a nationally representative sample of urine, plasma, and household salt samples from pregnant women. Therefore, the goal of the present study was to evaluate the iodine nutritional status of pregnant women by determining thyroid function and urinary iodine levels. These data provide useful information for determining new salt standards in China and monitoring policies in the future.
Methods
Study design and data collection
The 2015 CACDNS is a national, representative, and cross-sectional study on nutrition and chronic diseases in the general population of China. Participants were recruited using a stratified multistage cluster sampling design. The CACDNS covers all 31 provinces, autonomous regions, and municipalities throughout China (except Taiwan, Hong Kong, and Macao) directly under the central government, including 302 monitoring points. Each monitoring point in the 2015 CACDNS included 30 pregnant women chosen from maternal and child health care institutions.
First, an appointment was made with pregnant women to collect basic information and determine who was eligible to participate in the intensive field survey. Pregnant women were told to bring samples of the salt they used at home when attending the field survey. Second, intensive field investigations were conducted at maternal and child health care institutions, which included collection of fasting blood, urine, and salt samples. Plasma samples that had been stored at −70°C were available from a subset of these women (n = 2329).
The mean age ± standard deviation (SD) and stage of pregnancy that corresponded with these samples are listed in Table 1. Stages of pregnancy were defined according to trimester, as follows: trimester 1 (T1): 0–12 weeks; trimester 2 (T2): 13–27 weeks; trimester 3 (T3): 28–40 weeks. All procedures involving human participants were approved by the Ethics Committee of the Chinese Center for Disease Control and Prevention (CDC; 201519-A). Informed written consent was obtained from all participants.
Basic Information of Pregnant Women
The enrolled pregnant women covered all the 31 provinces in China, and 253 monitoring points.
SD, standard deviation.
Determination of thyroid function-related indexes
We determined levels of thyrotropin (TSH), free thyroxine (fT4; Siemens ADVIA Centaur XP), thyroid peroxidase antibodies (TPO-Ab), and thyroglobulin antibodies (TG-Ab; e601; Roche) using an automated chemiluminescence immunoassay analyzer. TSH and fT4 were categorized according to gestation period (T1–T3). The normal reference ranges (95% confidence interval [CI]) used for TSH (in mIU/L) and fT4 (in pmol/L) according to trimester (T1, T2, and T3) (8) were as follows: 0.13–3.93, 0.26–3.50, and 0.42–3.85 mIU/L for TSH and 12.0–23.34, 11.2–21.46, and 9.8–18.2 pmol/L for fT4, respectively. Data of participants with elevated thyroid function status according to these values are summarized in Table 2. TPO-Ab was considered positive with values >34 IU/mL, and TG-Ab with values >115 IU/mL.
Thyroid Function in Relation to Plasma Levels of Thyrotropin and Free Thyroxine
Normal range for TSH (mIU/L) (8): 0.13–3.93 (T1), 0.26–3.50 (T2), and 0.42–3.85 (T3).
Normal range for fT4 (pmol/L) (8): 12.0–23.34 (T1), 11.2–21.46 (T2), and 9.8–18.2 (T3).
fT4, free thyroxine; T1, trimester 1; T2, trimester 2; T3, trimester 3; TSH, thyrotropin.
Urinary iodine and iodine salt
Laboratories at the provincial level were approved after passing the examination of the National Iodine Reference Laboratory, China CDC. UIC was measured using arsenic and cerium catalysis spectrophotometry (WS/WS 107-2006). Data of participants with elevated iodine nutritional status according to UIC are summarized in Table 3. To monitor iodized salt intake among pregnant women, normal iodized salt and seaweed iodized salt were determined using a direct titration method (GB/T 13025.7-2012) and oxidation–reduction titration (GB/T 13025.7-2012). Iodized salt was defined as salt with a concentration of iodine ≥5 mg/kg.
Iodine Nutrition Status During Pregnancy in Relation to Median Urinary Iodine
WHO/UNICEF/ICCIDD international organization formulate it.
ICCIDD, International Council for Control of Iodine Deficiency Disorders; UNICEF, United Nations Children's Fund; MUI, median urinary iodine; WHO, World Health Organization.
Statistical analyses
Data are expressed as mean ± SD. Detected levels of TSH and fT4 did not conform to a normal distribution; therefore, these data are expressed as median with 2.5th and 97.5th percentiles, and variables were assessed using Kruskal–Wallis one-way analysis of variance. Pairwise comparisons were performed using the Mann–Whitney rank-sum test. The prevalence of abnormal thyroid function and normal prevalence are expressed as percent with 95% CI. The chi-square test was used to detect statistically significant differences between rates of normal and abnormal thyroid function. All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Irvine, CA). A p-value <0.05 was considered statistically significant.
Results
Levels of urinary iodine and iodine salt
A total of 6173 urine samples and 2329 plasma samples from pregnant women participating in the 2015 CACDNS were collected and analyzed. Urinary iodine was detected in all urine samples; the results are listed in Table 4. The mUIC of the 6173 pregnant women in the study was 146 μg/L, and more than half (52%) of pregnant women in 15 provinces had an mUIC <150 μg/L. The mUIC was >500 μg/L in 2.27% of pregnant women. Moreover, the proportion of monitoring points with an mUIC <150 μg/L was 57% (145/253). Iodized salt was detected in each of the 5216 salt samples. The results are listed in Table 5. The iodized salt coverage rate (i.e., with an iodine concentration ≥5 mg/kg) and household coverage rate of qualified iodized salt (i.e., an iodine concentration of 18–50 mg/kg) were 95.9% and 89.99%, respectively. The urine iodine and salt iodine concentrations did not conform to a normal distribution. The Spearman correlation coefficient between UIC and salt iodine content was 0.08667 (p = 0.0023).
Urine Iodine Level Distribution of Pregnant Women
mUIC, median urinary iodine concentration; UI, urinary iodine.
Iodine Salt Monitoring of Pregnant Women
Before 2012, iodized salt concentration ranged from 20 to 50 mg/kg. Implementation of new iodized salt concentration after March 15, 2012, and having three iodized salt concentrations, namely 20 (14 –26), 25 (18–33), and 30 (21–39) mg/kg. However, all provinces chose iodized salt concentrations of more than or equal to 25 mg/kg. It is stipulated that iodized salt produced before March 2012 can be sold until March 2015. The 2015 CACDNS was carried out in January 2015. Therefore, the iodized salt concentration between 18 and 50 mg/kg was considered to be qualified iodized salt.
Qualified IS coverage rate: the number of qualified iodized salt (18–50 mg/kg) divided by the number of all salt.
CACDNS, Chinese Adults Chronic Diseases and Nutrition Surveillance; IS, iodized salt; ISC, IS concentration.
Rates of normal and abnormal thyroid function
The rate of normal thyroid function in 2329 analyzed plasma samples was 84.4%, with significant differences among the three trimesters (p < 0.0001) (Table 6). The rate of normal thyroid function in trimester T1, T2, and T3 was 89.2%, 86.7%, and 77.9%, respectively.
The Prevalence for Different Types of Abnormal Thyroid Function and Normal Prevalence (%, 95% Confidence Interval)
HTOX, hypothyroxinemia; Hyper T, hyperthyroidism; Hypo T, hypothyroidism.
The prevalence of TPO-Ab-positive and TG-Ab-positive samples was 7.78% and 5.28%, respectively. After excluding the TPO-Ab-positive and TG-Ab-positive samples, the proportion of normal thyroid function increased from 84.4% to 85.4% in the 2015 survey (Table 7). The proportion of pregnant women in the first trimester with normal thyroid function was 90.9%. Results for abnormal thyroid function in the 2097 analyzed plasma samples are listed in Table 7. There were significant differences in the incidence of subclinical hypothyroidism among pregnant women according to trimester (p = 0.0026); the prevalence of subclinical hypothyroidism was 6.8%, which was higher among women in T2 and T3. In addition, the prevalence of clinical hyperthyroidism in T3 was significantly higher than that in T1 (p = 0.0039). The prevalence of isolated hypothyroxinemia in T1 was significantly higher than that in T2 and T3 (p < 0.0001). In a comparison with the 2010–2012 survey (Figs. 1 and 2), the prevalence of normal thyroid function was higher (p < 0.0001), and the prevalence of subclinical hypothyroidism was lower (p = 0.0124) in the 2015 survey. Although the prevalence of subclinical hyperthyroidism was increased (p = 0.0102) in the 2015 survey, the incidence was very low. Other abnormal thyroid functions showed no significant differences between 2010–2012 and 2015.
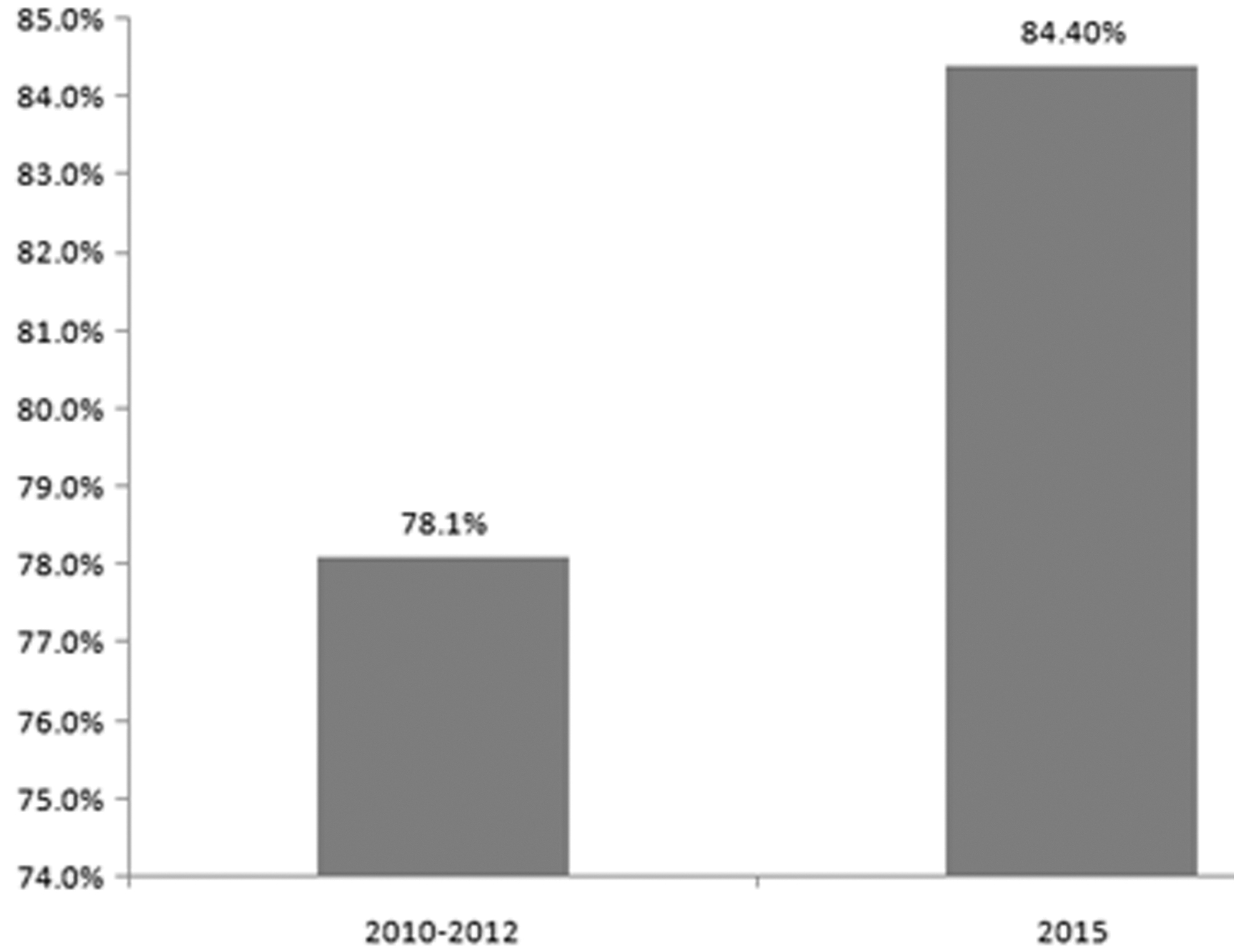
The prevalence of normal thyroid function of pregnant women in the 2010–2012 CNHS and the 2015 CACDNS. The prevalence of normal thyroid function of pregnant women in the 2015 CACDNS was higher than that in the 2010–2012 CNHS (p < 0.0001). CNHS, China Nutrition and Health Surveillance; CACDNS, Chinese Adults Chronic Diseases and Nutrition Surveillance.

The prevalence of different types of abnormal thyroid function of pregnant women in the 2010–2012 CNHS and the 2015 CACDNS. Compared with the results of the 2010–2012 CNHS, the prevalence of subclinical hypothyroidism was lower (p = 0.0124) in the 2015 survey. The prevalence of subclinical hyperthyroidism was increased (p = 0.0102) in the 2015 survey, but the incidence was very low. Other abnormal thyroid functions showed no significant differences between 2010–2012 and 2015 (*p < 0.05). Color images are available online.
The Prevalence for Different Types of Abnormal Thyroid Function and Normal Prevalence While Thyroglobulin Antibodies and Thyroid Peroxidase Antibodies Were Normal (%, 95% Confidence Interval)
HTOX, hypothyroxinemia; Hyper T, hyperthyroidism; Hypo T, hypothyroidism.
Plasma TSH, fT4, TG-Ab, and TPO-Ab levels, according to UIC levels
Plasma levels of TSH, fT4, TG-Ab, and TPO-Ab in the 1665 samples analyzed are reported according to 5 different UIC levels; the results are listed in Table 8. Compared with the group that had UIC >250 μg/L, TSH was significantly lower in the groups with UIC 120–149 and 150–249 μg/L. There was no significant difference in fT4 levels between the groups. Positive TG-Ab and TPO-Ab values were also not significantly different. TSH did not conform to a normal distribution; the Spearman correlation coefficient between UIC and TSH was 0.0054 (p = 0.8255).
Plasma Levels of Thyrotropin/Free Thyroxine/Free Triiodothyronine [Median (2.5th–97.5th Percentile Values)], Thyroglobulin Antibodies, and Thyroid Peroxidase Antibodies (%, 95% Confidence Interval)
p = 0.0056 for UIC between 120–149 and >250 μg/L.
p = 0.0272 for UIC between 150–249 and >250 μg/L.
TG-Ab, thyroglobulin antibodies; TPO-Ab, thyroid peroxidase antibodies; UIC, urinary iodine concentration.
Among the 1665 samples with a UIC level and plasma levels of TSH, fT4, TG-Ab, and TPO-Ab, the prevalence of normal thyroid function was 85.8% and that of subclinical hypothyroidism was 7.1% (Table 9). After excluding individuals with abnormal TPO-Ab and TG-Ab levels (Table 10), there was no significant difference in normal rates of thyroid function according to UIC level (p = 0.4252). When UIC values were further divided into three levels (Table 11), the prevalence of subclinical hypothyroidism was significantly increased, whereas the mUIC was >250 μg/L (p = 0.0247). The prevalence of other abnormal thyroid functions had no significant differences among three UIC levels.
Prevalence of Normal Thyroid Function and Thyroid Disorders According to Different Urinary Iodine Concentration Levels (%, 95% Confidence Interval)
HTOX, hypothyroxinemia; Hyper T, hyperthyroidism; Hypo T, hypothyroidism.
Prevalence of Normal Thyroid Function and Thyroid Disorders According to Different Urinary Iodine Concentration Levels with Normal Thyroglobulin Antibodies and Thyroid Peroxidase Antibodies (%, 95% Confidence Interval)
HTOX, hypothyroxinemia; Hyper T, hyperthyroidism; Hypo T, hypothyroidism.
Prevalence of Normal Thyroid Function and Thyroid Disorders According to Urinary Iodine Concentration Level with Normal Thyroglobulin Antibodies and Thyroid Peroxidase Antibodies (%, 95% Confidence Interval)
HTOX, hypothyroxinemia; Hyper T, hyperthyroidism; Hypo T, hypothyroidism.
Discussion
Iodine deficiency early in life can impair cognition and growth. Zimmermann (2009) reported that 18 million babies are born mentally impaired because of maternal iodine deficiency and 38 million are born at risk of iodine deficiency (9). However, in industrialized countries, such as the United States, the United Kingdom, and Australia, there has been a reemergence of newborns who are vulnerable to iodine deficiency (10 –13). In China, ∼370 million individuals have been affected by IDD since the 1970s (14). In 1994, a universal salt iodization program was implemented in China, which has been considered beneficial (15). The iodine status of Chinese residents was found to be improved after implementation of the universal salt iodization program (16,17).
At present, Chinese people generally have an adequate nutritional iodine status. However, vulnerable populations, such as pregnant women and children, are still at risk of iodine deficiency (6).
In the present study, there are more than half of pregnant women (52%) with an mUIC <150 μg/L and the mUIC is 146 μg/L. An mUIC of 146 μg/L is very close to the lower threshold of 150 μg/L that defines the WHO criterion for adequate levels. The prevalence of subclinical hypothyroidism among pregnant women with mUIC >250 μg/L is noteworthy. Compared with the 2010–2012 CNHS, the prevalence of normal thyroid function (84.4%, n = 2329) was found to be increased in the present study. This may be attributed to the iodized salt coverage rate and household coverage rate of qualified iodized salt. To monitor iodized salt in the 2015 CACDNS, the iodized salt coverage rate and qualified household iodized salt rate were 95.9% and 89.99%, respectively. These values are close to results of the 2014 National IDD Survey (6), 96.3% and 91.5%, respectively.
The WHO has indicated that if a universal salt iodization program is in effect for at least 2 years and covers the diet of >90% of the population, the iodine stored in the thyroid gland should be sufficient to ensure adequate hormone synthesis and secretion (18). At present, the coverage rate of iodized salt is suitable in China.
As for circulating TSH concentrations, pregnant women with mUIC >250 μg/L had higher TSH levels than those with mUIC 120–149 μg/L and mUIC 150–249 μg/L. Plasma TSH levels in participants with mUIC 120–149 μg/L were the lowest. Another study conducted by our team showed that after 20 years implementing universal salt iodization, expectant Chinese mothers with mUIC of 107.4 μg/L, less than the WHO's 150 μg/L benchmark, maintained thyroid function in both themselves and their newborn babies (19).
The main type of abnormal thyroid function detected in the present study was subclinical hypothyroidism. After exclusion of participants with positive TPO-Ab and TG-Ab (10%), the prevalence of subclinical hypothyroidism was 6.8%, which was higher in the last two trimesters. Compared with the 2010–2012 CNHS, the prevalence of subclinical hypothyroidism was lower in the 2015 CACDNS. According to a European Thyroid Society report, the global prevalence of subclinical hypothyroidism among pregnant women is 2–2.5% (20). Inadequate or excessive iodine intake can lead to subclinical hypothyroidism. With iodine deficiency, thyroid hormone synthesis is insufficient to maintain normal thyroid function and results in subclinical hypothyroidism. The cause of excess iodine in subclinical hypothyroidism is unclear; thyroid autoimmune disease may be the principal cause (21).
From a population perspective, iodine deficiency leads to irreversible mental impairment in the fetus and affects life quality across the life span. Greater attention is needed to iodine deficiency, especially with the current marketing of noniodized salt. To prevent iodine deficiency, it is necessary to maintain a qualified iodized salt coverage of not less than 90%.
Although the average iodized salt coverage rate and qualified iodized salt rate were both above 90% in the 2014 National IDD Survey (6), these rates in some provinces are <90%; for example, the iodized salt coverage rate and qualified rate in Jilin were 83.2% and 70.8%, respectively. The qualified rates in Tianjin, Shanxi, Shandong, Shanghai, Zhejiang, Yunnan, Xizang, Qinghai, and Ningxia were also <90%. The mUIC of pregnant women in the above regions was 140.7 μg/L (6) in the 2014 National IDD Survey. The qualified iodized salt rate in the above regions was 90.5% and the mUIC among pregnant women was 188.5 μg/L. However, the prevalence of subclinical hypothyroidism among pregnant women in the above regions was 9.4% in the present study. In the present study, we did not find a correlation between the salt iodine content and UIC, nor between the UIC and TSH.
Based on the following two aspects, we estimate that the iodized salt coverage and qualified rate may decrease in the next few years and IDD may reemerge in some areas. On the one hand, the state council issued the “reform plan of the salt industry system” in 2016, which abolished the monopoly in the salt industry and increased the supply of noniodized salt. On the other hand, some experts in China as well as in other countries doubt that the high incidence of hyperthyroidism is associated with an increased use of iodized salt (22 –25). Some people are more likely to choose noniodized salt, which raises concerns that the coverage rate and qualified rate will decline in the next few years. Therefore, it is necessary to carry out continuous monitoring of the iodine nutritional status of Chinese residents, especially vulnerable populations such as pregnant women.
In recent years, there have been several reports evaluating the thyroid function among pregnant women in China (26 –28), but to our knowledge, this is the first study to evaluate the iodine nutritional status according to thyroid function and urinary iodine level among pregnant women participating in the 2015 CACDNS. In the 2010–2012 CNHS, there were no urinary iodine data and no iodine salt survey was conducted. Serum samples of pregnant women in the present study are from a national survey, therefore, the present study can better reflect the overall thyroid function among pregnant women in China. A limitation of the present study is that we did not investigate whether pregnant women were taking thyroid medication, which could overestimate the normal rate of thyroid function in participants.
In summary, the present study results suggest that the overall normal rate of thyroid function among pregnant woman in China has improved and the prevalence of subclinical hypothyroidism is lower than in results of the 2010–2012 CNHS. With adjustment of the iodized salt standard in 2011, the iodine status in this population is generally adequate but it is close to the recommended UIC cutoff level. With freely available noniodized salt on the market, improvement is needed in related health education and continuous monitoring of iodine nutritional status and thyroid function in pregnant women.
Footnotes
Acknowledgments
We thank all the participants in our study and the staff working for 2015 Chinese Adults Chronic Diseases and Nutrition Surveillance (CACDNS).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We thank the grant “Study on the Appropriate Iodine Supplementation in General Population” from National Health Commission for funding support.