
Abstract
Background:
Tumor volume doubling time (TVDT) is considered as a dynamic indicator of tumor growth and progression. We aimed to clarify whether TVDT should be considered in the cytological diagnosis of follicular neoplasms (FNs).
Methods:
This retrospective cohort study included 100 consecutive FN patients with a TVDT >1 year for whom surgical resection was delayed for >1 year. Changes in tumor volume and the TVDT of each nodule were calculated by serial neck ultrasonography (US) over a median follow-up of 50 months.
Results:
Among 100 surgically resected FNs, 58 (58%) were benign and 42 (42%) were malignant tumors. At the 5-year follow-up, most FN nodules showed volume increases of >50%, accounting for 65% of benign and 62% of malignant nodules. No significant difference was observed in tumor growth rates and time to a >50% increase in tumor volume between benign and malignant nodules (p = 0.299 and p = 0.378, respectively). The calculated TVDT and a >50% volumetric increase showed a linear relationship with a high concordance (R 2 = 0.883; p < 0.001). The risk of malignancy was not significantly associated with TVDT (relative risk = 1.00; [95% confidence interval 0.99–1.01]; p = 0.784). Even when US features were considered, no significant association was found between TVDT and the risk of malignancy.
Conclusions:
The size of most FNs increased exponentially with time; the tumor growth rates of benign and malignant nodules were similar. Despite the usefulness of TVDT as an indicator of growing velocity of FN nodules, TVDT could not predict malignancy in FNs. Clinical surveillance based on the growth of thyroid nodules categorized as FNs on serial neck US does not predict the risk of malignancy.
Introduction
Follicular neoplasm (FN), consisting of a combination of high cellularity, microfollicular architecture, and scant or absent colloid, is a cytological term used to encompass both benign proliferation of thyroid follicular cells in adenoma and malignant proliferation in carcinoma (1 –3). These follicular-patterned lesions include follicular adenoma (FA), follicular thyroid carcinoma (FTC), follicular variant of papillary thyroid carcinoma (PTC), and noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) (4). The recently revised Bethesda System for Reporting Thyroid Cytopathology (BSRTC) reported that patients with FN have 10–40% risk of developing malignancy (5). Unfortunately, cytology cannot distinguish FTCs from FAs because the distinction between them is made based on capsular and vascular invasion, neither of which can be seen in cytology specimens (1,3). Therefore, diagnostic surgical excision is a long-established standard of care for nodules categorized as FNs. Additional molecular testing is also recommended (2). However, most diagnostic approaches based on molecular testing still have not reached the highest possible accuracy for the detection of all main types of thyroid carcinoma, and they may have limited performance in cases of FN nodules with high prevalence of FTC (6). Therefore, clinical biomarkers that can distinguish malignant from benign FN nodules are valuable for avoiding potentially unnecessary thyroid surgery.
Although thyroid nodule growth during surveillance has been used to assess the risk of malignancy (7), it remains unclear whether growth is a significant predictor of malignancy (2,8 –10). Few studies have evaluated the association between tumor growth rate and risk of malignancy, but most of them focused on patients with PTC. Therefore, whether these results are applicable to FN nodules mainly including FA or FTC remains unclear (11,12). We previously reported that growth kinetics on serial preoperative neck ultrasonography (US) cannot distinguish FTCs from FAs (13). However, this study did not take into account the cytologic categories of thyroid nodules (13). Therefore, it is necessary to evaluate growth rate of thyroid nodules based on the cytological results considering the clinical situation.
Tumor volume doubling time (TVDT) has been proposed as a dynamic indicator of growth rate and progression of the tumor (14 –16). Recent studies demonstrated that growth kinetics of tumor volume shows a classic exponential growth pattern, and calculated TVDT may facilitate early identification of tumors that will continue to grow (14,15). With the widespread use of US, TVDT can be calculated easily with at least three times of serial neck US examinations.
This study aimed to clarify whether TVDT should be considered in the cytological diagnosis of patients with FNs. We evaluated the growth kinetics of FN nodules in 100 patients whose diagnostic surgery was delayed, and determined whether TVDT and significant tumor growth are predictors for malignancy in patients with FN nodules.
Materials and Methods
Patients
We retrospectively reviewed 520 patients (ages ≥18 years) who underwent diagnostic thyroid surgery for nodules classified as FN between January 2014 and November 2017 at Asan Medical Center, Seoul, Korea. Although most patients with FN were recommended to undergo immediate diagnostic surgery, some patients underwent delayed surgical resection. We initially included 115 patients who underwent thyroid surgery >1 year after diagnosis of FN. Fourteen patients were excluded for the following reasons: 8 patients had preoperative neck US <3 times, and 6 patients had a thyroid nodule with a maximal dimension of 1 cm or less at diagnosis. One patient with TVDT <1 year was also excluded from our analysis. Finally, we included 100 patients with TVDT >1 year who underwent at least three preoperative neck US examinations in >1 year of follow-up for a thyroid nodule >1 cm. Although surgical resection is generally recommended when the nodule is cytologically diagnosed as FN, the reasons for delayed surgery in these patients were as follows: (i) initial fine-needle aspiration (FNA) cytology result was not FN (Hashimoto's thyroiditis, n = 2; nondiagnostic, n = 1; benign, n = 23; atypia of undetermined significance [AUS], n = 54), (ii) the patients had other malignancies (osteosarcoma, n = 1; breast cancer, n = 2; lung cancer, n = 1; colon cancer, n = 1), (iii) the patient was pregnant (n = 2), and (iv) the patient refused to undergo diagnostic surgery (n = 13). Thirty-one FN nodules were detected on thyroid cancer screening, as opposed to by other means. The median follow-up duration was 49.8 months (range 12.2–155.2 months). This study protocol was approved by the institutional review board of Asan Medical Center, Seoul, Korea.
US examinations and evaluation of tumor growth rate
All US examinations were performed using an iU22 unit (Philips Healthcare, Bothell, WA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz). As previously described, neck US examinations were performed by radiologists under the supervision of two experienced thyroid radiologists (J.H.L. and J.H.B. with 14 and 22 years of experience, respectively) (17,18). The radiologists prospectively measured the tumor diameters during the examinations in three directions: the longest axis and the other two orthogonal axes. Interobserver variations in measurements of the diameter and volume of thyroid nodules were ∼13% and 7%, respectively (17,18). For each nodule, the consensus ratings for each ultrasound feature were used to classify the risk of malignancy by employing the following systems: the Korean Thyroid Imaging Reporting and Data System (K-TIRADS) (19), the 2015 Guidelines of the American Thyroid Association (ATA) (2), and the European Thyroid Association's TIRADS (EU-TIRADS) (20).
The tumor volumes were calculated using the ellipsoid formula: length [cm] × width [cm] × depth [cm] × π/6 (8). The ATA guidelines define meaningful tumor growth as a ≥20% increase in at least 2 nodule dimensions, each representing an increase of at least 2 mm from the baseline diameter or a >50% increase in nodule volume (2). In all cases, a 50% increase in volume preceded the ≥20% increase in at least 2 diameters. Therefore, in this study, meaningful tumor growth was defined as a >50% volumetric increase from baseline. Since the tumor volume kinetics demonstrated a classic exponential growth pattern (Fig. 1), a TVDT was calculated using the Kuma calculator (
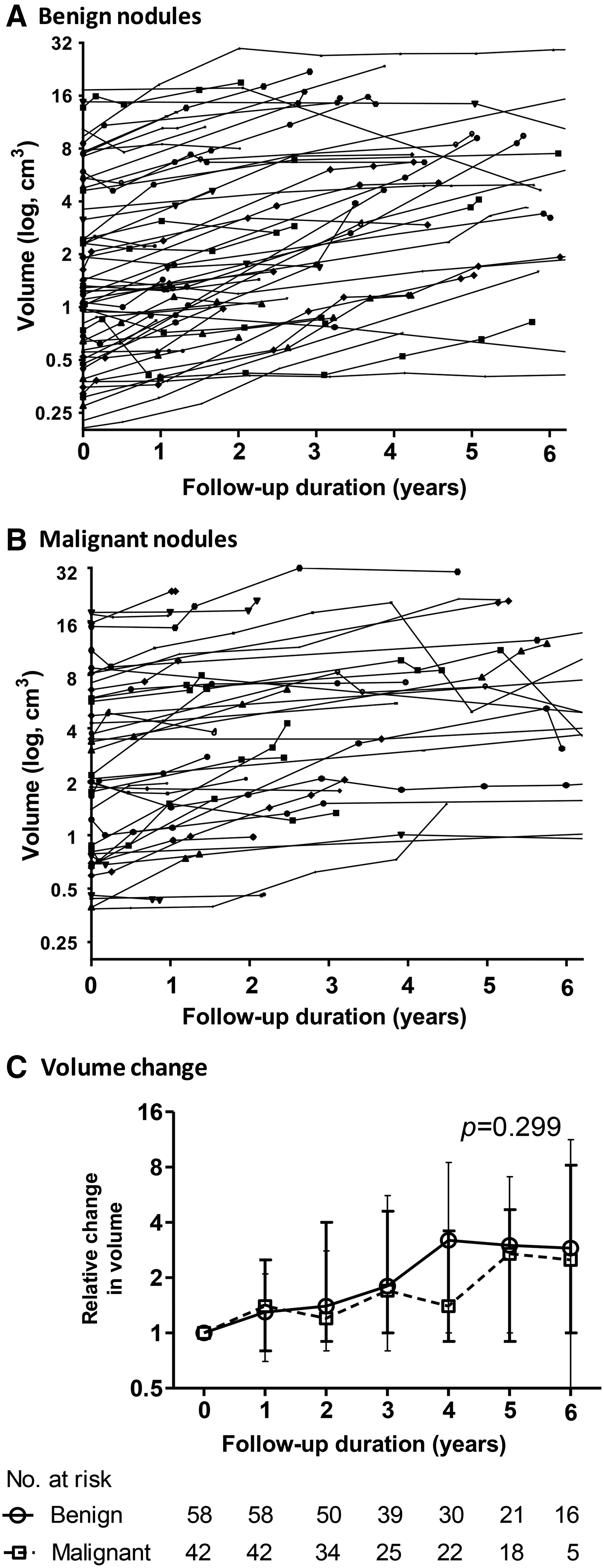
Changes in the tumor volume with time. Time–trend logarithmically transformed tumor volume measurements in each patient with (
Histopathological evaluation
FNA procedures were performed under US guidance by experienced radiologists, using a 23-gauge needle connected to a 10-mL syringe. The diagnostic category of the Bethesda system is used for all thyroid FNA samples (5). If a patient with a nodule underwent FNA more than once, the FNA cytology (FNAC) result was based on the highest one. Surgically removed specimens were reviewed and diagnosed using the World Health Organization classification criteria (22). All FNAC and surgical specimens were reviewed and diagnosed by an experienced endocrine pathologist (D.E.S.).
Statistical analysis
Data were analyzed using the R studio (version 3.4.0) and the R libraries (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline characteristics
The baseline characteristics are given in Table 1. After performing a diagnostic surgery in patients with thyroid nodules classified as FN, results showed that 58 (58%) had benign nodules and 42 (42%) had malignant tumors, of which 43 had FAs, 4 had nodular hyperplasias, 11 had adenomatous nodules, 25 had FTCs, and 17 had a follicular variant of PTC (FVPTC), including 5 noninvasive encapsulated FVPTCs (NI-EFVPTC/NIFTP), 9 invasive EFVPTCs, and 3 infiltrative FVPTCs (Supplementary Table S1). The median age at the time of initial neck US was 50 years (IQR 38–57 years), and 82 (82%) patients were women. There were no significant differences in age and sex between the benign and malignant groups. Median primary tumor sizes were 2.0 cm (IQR 1.5–2.9 cm) on initial US and 2.5 cm (IQR 1.7–3.5) in surgical specimens. There was no significant difference in tumor size between benign and malignant groups (p = 0.120 and p = 0.184, respectively). A total of 82 patients (82%) initially underwent diagnostic lobectomy, and surgical extent was not significantly different between the two groups (p = 0.620). Based on the K-TIRADS classification, 63 (63%), 34 (34%), and 3 (3%) patients were classified into the low, intermediate, and high suspicion categories, respectively. When we applied the ATA guidelines, four FN nodules could not be classified into any US-risk category (i.e., iso- or hyperechoic nodules with features indicative of high suspicion), and the results for the remaining nodules corresponded to the K-TIRADS classification. According to the EU-TIRADS system, five FN nodules with intermediate suspicion in the K-TIRADS were reclassified as high risk. The malignancy rate of FN nodules in the intermediate-to-high suspicion category was not higher than that of FNs in the low suspicion category in the K-TIRADS, ATA, and EU-TIRADS systems.
Baseline Clinical and Pathological Characteristics of Patients with Thyroid Nodules That Were Cytologically Diagnosed as Follicular Neoplasm
Continuous variables are presented as medians (interquartile ranges). Categorical variables are presented as n (%).
Excluding the four nodules that could not be classified with the ATA system (i.e., iso- or hyperechoic nodules showing features indicative of high suspicion).
ATA, American Thyroid Association; EU-TIRADS, European TIRADS; K-TIRADS, Korean-TIRADS; TIRADS, Thyroid Imaging Reporting and Data System; US, ultrasonography.
Tumor growth kinetics based on volume changes
The median time between the initial and last US examinations of benign and malignant nodules was 51.0 months (range 13.2–144.9 months) and 49.4 months (range 12.2–155.2 months), respectively. Figure 1A and B shows the time-dependent logarithmic-transformed actual tumor volume in each of the benign and malignant nodules, respectively. The change in median tumor volume from the baseline value is presented in Figure 1C. During the follow-up, changes in tumor volumes in FN nodules were variable (increased, remained stable, and decreased). Both benign and malignant nodules showed a significant increase in tumor volume (p < 0.001 and p < 0.001, respectively), and the rates of increase of the tumor volume between the two groups were similar (p = 0.299). The maximum diameters of benign and malignant nodules also significantly increased (p < 0.001 and p < 0.001, respectively), and the difference in the rates of increase was not statistically significant between the two groups (p = 0.279, Supplementary Fig. S2).
Association between TVDT and malignancy risk
The calculated TVDT and a >50% volumetric increase showed a linear relationship with a high concordance (R 2 = 0.883; p < 0.001, Fig. 2). Malignancy was not significantly associated with TVDT in FN nodules (RR = 1.00; [95% CI: 0.99–1.01]; p = 0.784, Table 2). In addition, there was no significant association between TVDT and the risk of malignancy among FN nodules according to the K-TIRADS classification (low suspicion, p = 0.905; intermediate suspicion, p = 0.378; and high suspicion, p = 0.999), ATA guidelines (low suspicion, p = 0.905; intermediate suspicion, p = 0.504; and high suspicion, p = 0.999), and EU-TIRADS system (low risk, p = 0.905; intermediate risk, p = 0.494; and high risk, p = 0.645).

Concordance between calculated TVDT and a volume increase >50%. The calculated TVDT and the >50% volumetric increase showed a linear relationship, with high concordance (R 2 = 0.883; p < 0.001). TVDT, tumor volume doubling time.
Relative Risk of Malignancy According to the Tumor Volume Doubling Time Per Year in Thyroid Nodules Classified as Follicular Neoplasm
Owing to small sample size.
Excluding the four nodules that could not be classified with the ATA system (i.e., iso- or hyperechoic nodules showing features indicative of high suspicion).
CI, confidence interval; NA, not applicable; RR, relative risk.
Incidence of volume increases of >50% in benign and malignant tumors
A volume increase of >50% was observed in 57 (57%) of 100 patients during the follow-up. The cumulative incidence of volume increases >50% in the benign and malignant group was 49% and 38% at 2 years, respectively, and 65% and 62% at 5 years, respectively (Fig. 3). Malignancy was not associated with an increased incidence of volume increase of >50% (hazard ratio 0.8; [95% CI 0.5–1.4]; p = 0.541). There was no significant difference in time to a >50% increase in tumor volume between benign and malignant nodules (p = 0.378). In addition, there was no significant difference in the incidence of volume increases >50% among different pathologic subtypes (p = 0.848, Supplementary Fig. S3).
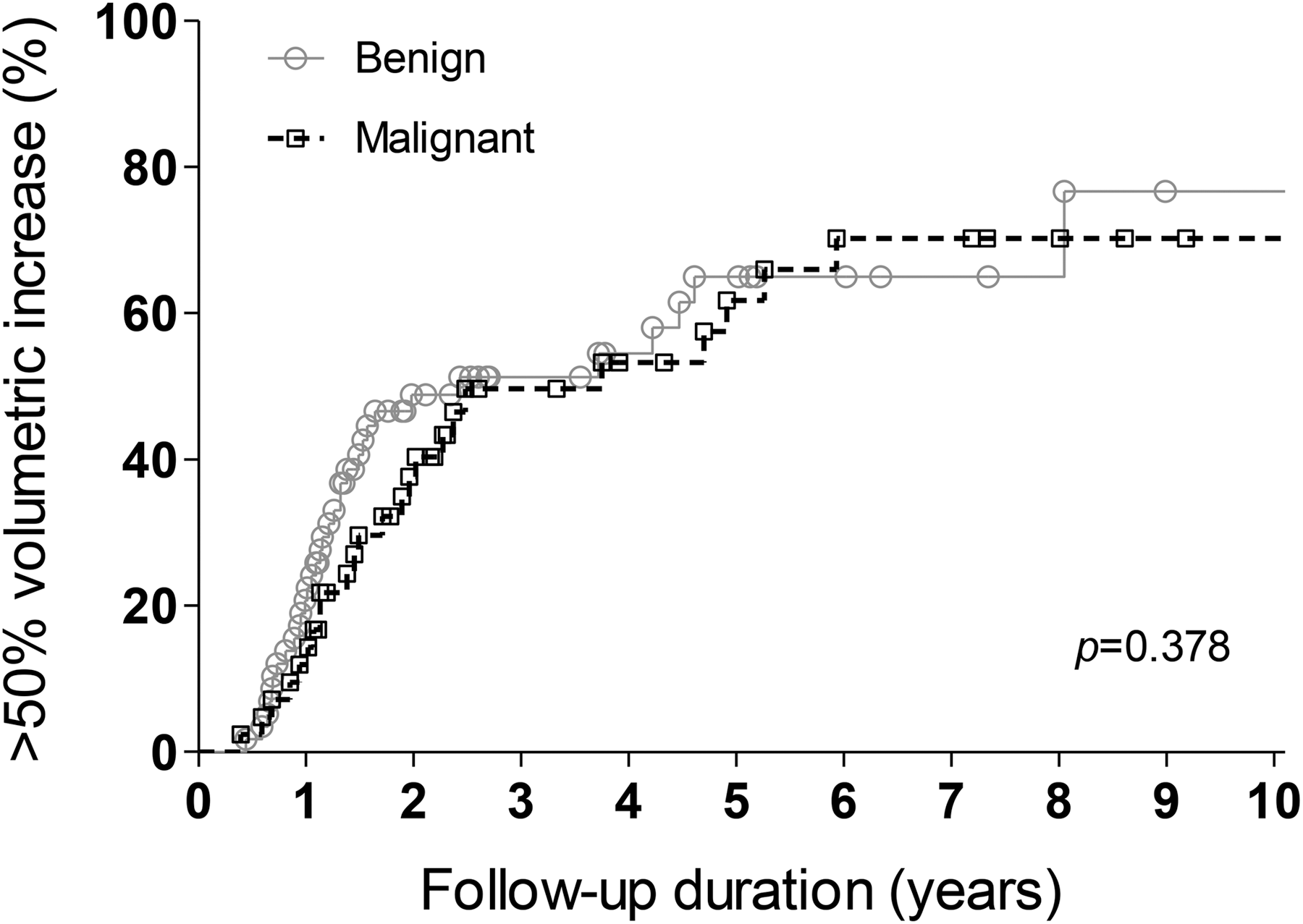
Cumulative incidence of volume increases of >50%. There were no significant differences in time to a >50% increase in tumor volume between benign and malignant nodules (p = 0.378).
Discussion
In this study, we describe the tumor growth kinetics of 100 surgically resected benign and malignant thyroid nodules cytologically diagnosed as FN. During the follow-up, most FN nodules showed volume increases >50%, accounting for 65% of benign and 62% of malignant nodules at 5 years. There was no significant difference in tumor growth rates and time to a >50% increase in tumor volume between benign and malignant nodules. The calculated TVDT and the >50% volumetric increase showed a linear relationship, with a high concordance. The risk of malignancy was not significantly associated with TVDT in FN nodules. Even when US features were considered, no significant association was found between TVDT and the risk of malignancy according to the K-TIRADS, ATA, and EU-TIRADS systems. These findings suggest that growth kinetics of each tumor has limited value for predicting malignancy in patients with thyroid nodules with FN cytology.
The estimated risk of malignancy of FN is 10–40% when NIFTPs are regarded as malignant tumors (5), and a considerable number of patients with FN nodules underwent unnecessary thyroid surgery. Although growth of thyroid nodules has been used to assess the risk of malignancy (7), few studies have evaluated the association between tumor growth rates and risk of malignancy in FN nodules. One previous study suggested that an increase in volume in FN nodules should be considered as a risk factor for malignancy, but that the growth rate itself does not correlate with malignancy (8). In accordance with that study, it is difficult to hypothesize that the growth rate of thyroid nodules can distinguish between benign and malignant nodules with FN cytology.
We previously reported that growth kinetics on serial preoperative neck US cannot distinguish FTCs from FAs in patients with a 37% overlap (13). This study did not take into account cytologic categories and US features of thyroid nodules (13). In this regard, we integrated the US features (degree of suspicion of malignancy according to the K-TIRADS, ATA, and EU-TIRADS classification systems) into the present study. We also reported that the growth rate does not predict malignancy in surgically resected thyroid nodules classified as Bethesda category III (AUS) with architectural atypia (AUS-A) (18). Thyroid nodule patients diagnosed with AUS-A usually undergo diagnostic surgery only if clinical or sonographic findings are suggestive of malignancy. The malignancy rate of AUS-A nodules was higher than that shown in other studies (5,23). Therefore, findings from surgically resected AUS-A nodules might not reflect the characteristics of the entire thyroid nodule in the AUS-A category. On the contrary, early diagnostic surgery is usually performed in most patients with FNAC-diagnosed FNs. In our study, we evaluated ∼88% of patients who underwent delayed surgery, and the proportion of malignancy in nodules with FN cytology after thyroid surgery was 42%, which is consistent with the risk of malignancy reported in the recently revised BSRTC (5). This suggests that our findings might represent the growth rate of FN nodules, even though we included the patients with FN who underwent delayed surgery. The heterogeneous reasons for delayed surgery might also have some effects on the study results. The proportion of patients with meaningful tumor growth during follow-up was higher in the group with removed FN nodules than that in the group with removed AUS-A nodules (18).
In this study, we verified that the calculated TVDT is a reliable prognostic indicator of tumor enlargement in patients with FN nodules. Previous studies suggested that tumor structural progression usually demonstrated a pattern of exponential growth that remains constant over time until large burdens of disease are achieved (14,15). In accordance with this hypothesis, the tumor volume of FN nodules linearly increased with time and there was a linear relationship between TVDT and an increase in tumor volume of >50%. In addition, the Kuma calculator allows physicians to easily calculate TVDT with at least three consecutive neck US examinations for a target nodule (15). Therefore, TVDT is a useful and easily calculated indicator to determine the growth rate of thyroid nodules during follow-up.
This study has some limitations. This is a retrospective study and there is a possibility of selection bias. We could not evaluate the growth of thyroid nodules without surgical excision. In addition, the results of this study may not apply to more rapidly growing FN nodules, with a TVDT <1 year. Owing to the small number of metastatic FTCs (n = 1) included in this study, we could not compare the tumor growth rate between metastatic and nonmetastatic malignant tumors. In fact, a 55-year-old female patient with bone metastatic FTC had a TVDT of 7.4 years. Nevertheless, this is the first study to evaluate the natural course of FNs over a median 50 months and compare growth rates of benign and malignant thyroid nodules that were diagnosed as FN in cytology.
In conclusion, most of the thyroid nodules with FN cytology increased exponentially with time and the tumor growth rates of benign and malignant nodules were similar. Despite the usefulness of TVDT as an indicator of growing velocity of thyroid nodules, TVDT could not predict malignancy in thyroid nodules cytologically diagnosed as FN. Moreover, clinical surveillance based on the growth rate of thyroid nodules with FN on serial neck US cannot distinguish malignant nodules from benign nodules. Therefore, further studies focusing on biomarkers are warranted to reduce unnecessary diagnostic surgery in patients with thyroid nodules diagnosed as FN.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the National Research Foundation (NRF) of Korea Research Grant (NRF-2018R1D1A1A02085365).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1