
Abstract
Background:
A subset of Hashimoto's thyroiditis (HT), reported as immunoglobulin G4 (IgG4) thyroiditis, is characterized by IgG4+ plasma cell-rich inflammation and marked sclerotic changes, which suggests a close relationship with immunoglobulin G4-related disease (IgG4-RD). However, to date, there is no consensus regarding the cutoff values used to define a significant IgG4+ plasma cell count in thyroid inflammation. We, therefore, sought to validate both the cutoff value of the comprehensive diagnostic criteria (CVC) and the cutoff value of thyroid-specific diagnostic criteria (CVT) for diagnosing IgG4 thyroiditis.
Methods:
One hundred twenty cases of HT were retrospectively reviewed. According to the CVC (IgG4+ plasma cells >10/HPF (high-power field) and IgG4+/IgG+ plasma cell ratio >40%) and the CVT (IgG4+ plasma cells >20/HPF and IgG4+/IgG+ plasma cell ratio >30%), cases were subclassified as IgG4 thyroiditis or non-IgG4 thyroiditis. Clinical, serological, sonographic, and histopathological characteristics of the two subsets, and the cases diagnosed as IgG4 thyroiditis using different thresholds were compared.
Results:
Both the CVC and CVT identified the same set of distinct clinical, laboratory, and sonographic features of the cases diagnosed as IgG4 thyroiditis. All 120 cases of HT were able to be divided into four distinct groups. Group A included the 25 cases who were assigned as IgG4 thyroiditis by both the CVC and CVT, whereas Group D included the 85 cases who did not meet either of the cutoff values. Group B and Group C comprised the borderline cases who only met one of the two thresholds. Based on histological evaluation, the cases in Group B who met the CVT demonstrated similar histological features of IgG4 thyroiditis.
Conclusions:
Although both of the cutoff values can efficiently distinguish IgG4 thyroiditis from its non-IgG4 counterpart, the thyroid-specific cutoff value (CVT, IgG4+ plasma cells >20/HPF, and IgG4+/IgG+ plasma cell ratio >30%) can better identify borderline cases of HT with more fibrotic changes, which may represent an early phase lesion of IgG4 thyroiditis. We propose a new series of clinical and pathological diagnostic clues for both endocrinologists and pathologists to improve the early recognition of IgG4 thyroiditis.
Introduction
Immunoglobulin G4
In 2009, our group first reported a subset of Hashimoto's thyroiditis (HT) exhibiting similar histopathological features of IgG4-RD, particularly the marked infiltration of IgG4+ plasma cells into the inflamed sclerotic thyroid tissue, and proposed that HT can be divided into the IgG4+ plasma cell-rich group and IgG4+ plasma cell-poor group. The nomenclature of “IgG4 thyroiditis” and “non-IgG4 thyroiditis” was initially used to describe these entities (3). Since then, endocrinologists and pathologists have investigated the relationship between other thyroid autoimmune diseases and IgG4-RD, and discovered a subgroup of Graves' disease, Riedel's thyroiditis (RT), and a so-called IgG4-related thyroiditis found in patients with IgG4-RD in other organs, which may also be manifestations of IgG4-rich inflammation in the thyroid (4 –11). Although their relationship and IgG4-related nature remain controversial, recent studies have demonstrated that these IgG4-rich thyroid diseases are associated with significant clinical symptoms (12,13).
An international consensus statement on the pathology of IgG4-RD was published in 2012 (14). It emphasized that IgG4 immunostaining is essential for the pathological diagnosis of IgG4-RD because it is a simple and highly reproducible test that provides strong confirmatory evidence for the diagnosis. At the same time, comprehensive diagnostic criteria were introduced for the diagnosis of IgG4-RD by the Japanese Ministry of Health, Labour and Welfare (MHLW) IgG4 team (15). The recommended diagnostic thresholds for IgG4 staining are IgG4+ plasma cells >10/HPF (high-power field) and a IgG4+/IgG+ plasma cell ratio >40%, and these have been widely adopted in pathological practice as the general cutoff values for all involved organs. Although both of these diagnostic consensus statements emphasized the importance of establishing organ-specific diagnostic criteria because of the variability in the pathological findings across organs, there was no particular comment on how to diagnose similar lesions in the thyroid.
In contrast, thyroid-specific diagnostic criteria for IgG4+ plasma cell-rich inflammation proposed by our group were accepted and demonstrated to be useful to identify this unique subtype, IgG4 thyroiditis, in patients with HT by other researchers (16,17). The cutoff values for IgG4 staining are IgG4+ plasma cells >20/HPF and a IgG4+/IgG+ plasma cell ratio >30% (18,19).
In this study, we investigated the validity of the cutoff values of comprehensive diagnostic criteria (CVC) for IgG4-RD published by Umehara et al. and the cutoff values of thyroid-specific diagnostic criteria (CVT) proposed by our group for diagnosing IgG4 thyroiditis, and evaluated whether using different threshold values alters the collective phenotype of IgG4 thyroiditis by focusing on borderline cases. Furthermore, we propose organ-specific and clinically practical diagnostic criteria for both endocrinologists and pathologists for accurate diagnosis.
Patients and Methods
Patients and clinical assessment
A total of 120 cases of HT treated by total thyroidectomy who had sufficient paraffin-embedded tissue for histological evaluation and immunostaining were retrospectively recruited from Kuma Hospital (Kobe, Japan), Wakayama Medical University (Wakayama, Japan), and the affiliated hospital of Taishan Medical University (Tai'an, China) from January 1983 to December 2017.
The patients underwent surgery for various reasons: marked swelling (n = 57), tracheal stenosis (n = 19), pain and tenderness (n = 4), nodular lesion (n = 13), suspected malignant lymphoma (n = 12), or suspected papillary thyroid carcinoma (n = 2). There were 13 cases who did not have clear records of indications for thyroidectomy. Thyroidectomies performed for malignancy were excluded to avoid confounding factors, especially increased peritumoral fibrosis or inflammation. In addition, 100 cases were involved in our previous study for a different research purpose (19). To maintain diagnostic consistency for the cases from different hospitals, we applied rigorous diagnostic criteria to select cases mainly based on the Guidelines of the Japan Thyroid Association for HT (20).
The majority of patients enrolled in this study had integrated clinical information. The data of presenting clinical and sonographic findings, medical history, and disease outcomes were obtained from the patients' medical records. If patients developed hypothyroidism or thyrotropin (TSH)-dependent goiter, levothyroxine (LT4) was administered to provide resolution of symptoms and signs of hypothyroidism, or to relief the patients from compression symptoms. The doses of LT4 were also extracted from the electronic medical records. Furthermore, the clinical charts were meticulously examined to evaluate whether there were any possible signs or symptoms of extrathyroidal involvement of IgG4-RD. Institutional ethics committee approvals were obtained.
Laboratory and thyroid function evaluation
Antithyroglobulin antibodies (Tg-Abs) and antithyroid peroxidase antibodies (TPOAbs, formerly antimicrosomal antibodies) of the majority cases in this study were measured by the hemagglutination method using commercially available kits (Fuji Rebio, Inc., Tokyo, Japan). By this procedure, the normal range of antibody titers was considered <100-fold.
TSH and free thyroxine (fT4) levels were evaluated at multiple time points before surgery by chemiluminescent immunoassay (Abbott Diagnostics, Tokyo, Japan). Reference ranges were as follows: TSH 0.30–5.00 mIU/L and fT4 0.70–1.60 ng/dL.
In this study, all 120 patients showed serum fT4 levels within the reference range. They were stratified into three groups according to serum TSH levels, as follows: Group I (GI), those with TSH levels >5.00 mIU/L; Group II (GII), those with TSH levels between 0.3 and 5.00 mIU/L; and Group III (GIII), those with TSH levels <0.3 mIU/L. As serum TSH levels fluctuated during the clinical course in patients who were on LT4 therapy (n = 72), the patients were classified into the mentioned groups based on the longest duration of the respective TSH levels. The thyroid function of patients without LT4 therapy (n = 33) was evaluated based on their preoperative thyroid function tests (18).
Serum levels of IgG4 were measured with the Behring nephelometric immunoassay (MBL, Nagoya, Japan). The reference range for IgG4 was 4.8–105 mg/dL. However, because the comprehensive diagnostic criteria for IgG4-RD include a serum IgG4 level >135 mg/dL, we defined this as the cutoff value in our study (15).
Histological evaluation
Two thyroid pathologists (Y.L. and K.K.) retrospectively reviewed >5 HE sections for each case to confirm the previous histological diagnosis of HT and selected a representative paraffin block for immunohistochemical analysis in each case. Incidental findings of focal (nonspecific) lymphocytic thyroiditis in tumor-bearing thyroid tissue were excluded from this study.
The intensities of the following histopathology features were graded from negative to 3+: degree of stromal fibrosis, lymphoplasmacytic infiltration, follicular cell degeneration, lymphoid follicle formation, and giant cell/histiocyte infiltration. The predominant type of stromal fibrosis was recorded as interfollicular, interlobular, or scar pattern, the thyroid follicle size was described as microfollicular, normofollicular, or macrofollicular, and the presence of obliterative phlebitis was also examined. The mentioned grading system and the validation protocol were described in detail in our previous publication (19).
Immunohistochemistry and cutoff values for IgG4 thyroiditis
Immunostaining was carried out using the Envision immunohistochemical detection system (Dako Cytomation, Glostrup, Denmark). The slides were stained using antibodies against IgG4 (MC011, 1:500; Binding Site, Birmingham, UK) and IgG (A0423, 1:8000; Dako Cytomation).
Quantitative assessment of the IgG4 staining was performed according to the methods summarized in the consensus statement (14). For each specimen, five nonoverlapping HPFs with the highest density of positive cells were counted, and the average number of positive cells per HPF was calculated using the image analysis software Win ROOF version 5.8 (Mitani Corp., Tokyo, Japan). One HPF covered an area of 0.034 mm2 (AX80T microscope, × 10 eyepiece, and × 40 lens; DP70 camera and DP controller software; Olympus, Tokyo, Japan). The average IgG4+/IgG+ plasma cell ratio was also recorded.
All 120 cases of HT were categorized into the IgG4 thyroiditis group or non-IgG4 thyroiditis group using the CVC (IgG4+ plasma cells >10/HPF and IgG4+/IgG+ plasma cell ratio >40%) and CVT (IgG4+ plasma cells >20/HPF and IgG4+/IgG+ plasma cell ratio >30%), respectively.
Statistical analysis
The clinical and histopathology features of the IgG4 thyroiditis and non-IgG4 thyroiditis were compared using the Mann–Whitney U-test and unpaired t-test (for continuous variables: age, disease duration, and weight of thyroid gland). Data with a skewed distribution, including TPOAbs and Tg-Abs titers, are summarized as the geometric mean and 95% confidence interval. Fisher's exact test or χ 2 test was used for comparison by sex, indication for thyroidectomy, thyroid function, sonographic features, predominant pattern of stromal fibrosis, and thyroid follicle size. The correlation among the weight of thyroid gland, LT4 therapy, and thyroid function was assessed by Spearman's ρ test. Analyses were performed using GraphPad Prism version 7.0 (GraphPad Software, Inc., CA), and p < 0.05 was considered significant.
Results
Using the CVC proposed by Umehara et al., 27 cases of HT (22.5%) were categorized into the IgG4 thyroiditis group and the remaining 93 cases (77.5%) were subclassified into the non-IgG4 thyroiditis group. In contrast, based on the CVT proposed by our group, 33 cases of HT were subclassified as IgG4 thyroiditis (27.5%), and the remaining 87 cases (72.5%) were subclassified as non-IgG4 thyroiditis.
The IgG4 immunostaining results are presented as a scatter plot in Figure 1. Each case appears as a symbol representing the number of IgG4+ plasma cells/HPF and the IgG4+/IgG+ plasma cell ratio. As shown in Figure 1, these cases span a continuum from no IgG4 staining to intense IgG4 staining. Moreover, by applying both the CVC and CVT, all the cases represented in this scatter plot were able to be separated into four distinct groups. Group A represented the 25 cases that were able to be classified as IgG4 thyroiditis by both the CVC and CVT, whereas Group D included the 85 cases who did not meet either of the cutoff values and should be classified as non-IgG4 thyroiditis.
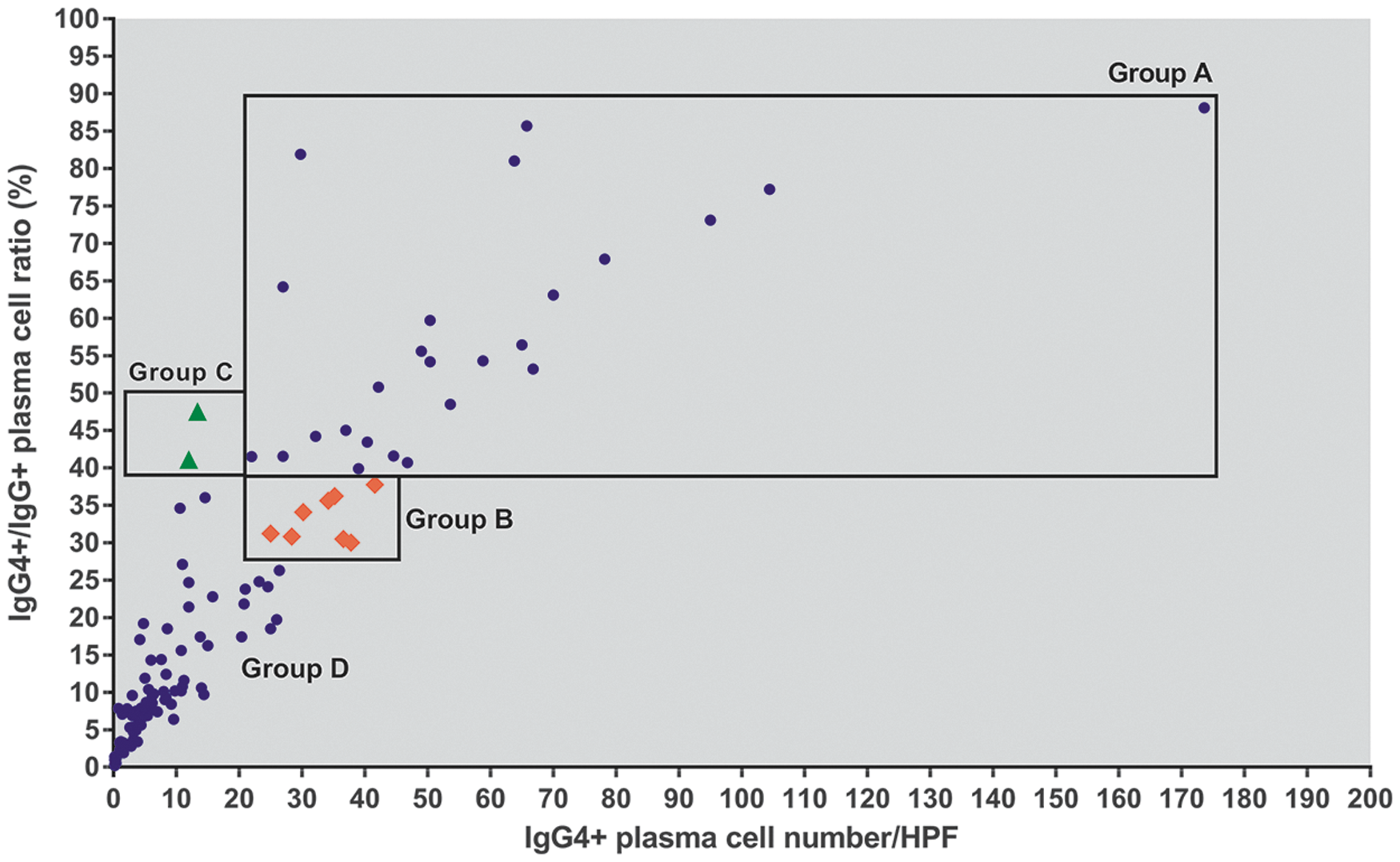
Scatter plot illustrating the number of IgG4+ plasma cells per HPF and the IgG4+/IgG+ plasma cell ratios for the 120 cases of HT. Group A (indicated as blue dots) comprises the 25 cases diagnosed as IgG4 thyroiditis by both of the cutoff values. Group B (indicated as red diamonds) includes the eight cases assigned to the IgG4 thyroiditis group by the CVT (IgG4+ plasma cells >20/HPF, and IgG4+/IgG+ plasma cell ratio >30%) who did not fulfill the CVC (IgG4+ plasma cells >10/HPF, and IgG4+/IgG+ plasma cell ratio >40%). Group C (indicated as green triangles) comprises the two cases who did not meet the CVT but were classified as IgG4 thyroiditis based on the CVC. In Group D (indicated as blue dots), the cluster of dots in the bottom left corner outside of the black squares comprises the 85 cases categorized as non-IgG4 thyroiditis by both the CVT and CVC. CVC, cutoff values of comprehensive diagnostic criteria; CVT, cutoff values of thyroid-specific diagnostic criteria; HT, Hashimoto's thyroiditis; HPFs, high-power fields. Color images are available online.
However, there were eight cases (IgG4+ plasma cell number >20/HPF and 30% < IgG4+/IgG+ plasma cell ratio <40%) who were categorized into the IgG4 thyroiditis group by the CVT without fulfilling the CVC. In addition, there were two cases (10/HPF < IgG4+ plasma cell number <20/HPF and IgG4+/IgG+ plasma cell ratio >40%) who did not meet the CVT but were classified as IgG4 thyroiditis by the CVC. These two subgroups were referred to as Group B and Group C, respectively, in this study. Until a more detailed understanding of these conditions can suggest a precise nature, we propose Group B and Group C cases to be borderline lesions.
Comparisons of clinical and histopathological features of IgG4 thyroiditis based on different cutoff values
The demographic, clinical, serological, and sonographic features of the patients in the two subgroups were compared, and the results are summarized in Table 1. Both the CVC and CVT of IgG4 immunostaining identified the same set of distinct demographic, clinical, laboratory, and sonographic features of IgG4 thyroiditis, including a younger age group, a lower female-to-male ratio, a more progressive course, elevated serum IgG4 concentrations, higher level of circulating thyroid autoantibodies, and diffuse low echotexture.
Comparison of IgG4 Thyroiditis and Non-IgG4 Thyroiditis Based on Different Cutoff Values: Demographic, Clinical, Serological, and Sonographic Features
Data are the mean ± standard deviation.
Data are the geometric mean and 95% confidence interval.
Not all of the patients had complete clinical data.
GI, Group I, TSH >5.00 mIU/L; GII, Group II, 0.3 ≤ TSH ≤5.00 mIU/L; GIII, Group III, TSH <0.3 mIU/L.
CVC, cutoff values of comprehensive diagnostic criteria; CVT, cutoff values of thyroid-specific diagnostic criteria; HPFs, high-power fields; IgG4-RD, immunoglobulin G4-related disease; MS, marked swelling; TS, tracheal stenosis; P&T, pain and tenderness; NL, nodular lesion; sML, suspected malignant lymphoma; sPTC, suspected papillary thyroid carcinoma; TgAb, thyroglobulin autoantibodies; TPOAb, thyroid peroxidase antibodies; LT4, levothyroxine; TSH, thyrotropin.
In addition, as to thyroid function test, by using both the CVC and CVT, we found that the proportion of patients in Group I (with elevated TSH levels) was significantly higher in the IgG4 thyroiditis group (CVC: 45.45%; CVT: 39.29%) than in the non-IgG4 thyroiditis group (CVC: 12.05%; CVT: 11.69%).
Furthermore, patients in the IgG4 thyroiditis group received a higher dose of LT4 than those in the non-IgG4 thyroiditis group, although this difference was not statistically significant. It was noted that thyroid function was significantly affected by the doses of LT4 before thyroidectomy (Spearman's ρ: r = 0.222, p = 0.0334). Therefore, the fact that the patients in Group I needed higher doses of LT4 but still had a higher TSH levels while on LT4 treatment indicates more severe hypothyroidism in the IgG4 thyroiditis group than that in the non-IgG4 thyroiditis group. These results are consistent with our previous clinical study determining thyroid function tests of IgG4 thyroiditis and non-IgG4 thyroiditis (18).
Moreover, there was no evidence of IgG4-RD reported in other organ systems in the 120 cases during the follow-up period, indicating the organ-specific nature of the disease.
The comparison of the histopathological features of IgG4 thyroiditis and non-IgG4 thyroiditis is summarized in Table 2. Both cutoff values revealed that IgG4 thyroiditis cases had significantly higher grades of lymphoplasmacytic infiltration, stromal fibrosis, follicular cell degeneration, giant cell/histiocyte infiltration, and smaller thyroid follicles than the non-IgG4 thyroiditis cases. Characteristic interfollicular fibrosis was observed in the majority of IgG4 thyroiditis cases diagnosed by both the CVC and the CVT. No case in our study demonstrated obliterative phlebitis. These results confirm our previous histological study and suggest that IgG4 thyroiditis represents a subset of cases with more destructive thyroid architecture (19).
Comparison of IgG4 Thyroiditis and Non-IgG4 Thyroiditis Based on Different Cutoff Values: Histopathological Features
In summary, neither the cutoff value for general organ systems, the CVC, nor the thyroid-specific cutoff value, the CVT, alters the distinct collective phenotypes of the cases diagnosed as IgG4 thyroiditis.
Clinicopathological characteristics of the borderline cases
For cases of the borderline condition of IgG4-RD, careful correlation with the clinical scenario, imaging characteristics, and histopathological features of a particular patient is often required to arrive at a definitive diagnosis (21). Thus, we focused on analyzing the particular manifestations in cases in Group B and Group C.
The clinicopathological profiles of the eight cases in Group B are summarized in Table 3. These cases demonstrated borderline IgG4 immunostaining results that met the CVT but did not fulfill the CVC. Of the eight cases, seven were females and only one occurred in a male patient. The age of the patients ranged from 49 to 73 years. The disease duration was 5–30 years. Five patients (Cases 1, 2, 4, 5, and 6) underwent total thyroidectomy because of marked swelling, whereas the other two patients (Cases 3 and 7) underwent surgical treatment because of tracheal compression by the markedly enlarged thyroid glands. TgAb and/or TPOAb levels were markedly elevated in most cases except for Case 1 and Case 6. Thyroid function tests showed that with LT4 substitution, one patient had elevated TSH levels; the other six patients exhibited TSH levels within reference range. Ultrasound examinations for four patients (Cases 1, 3, 4, and 5) revealed diffuse hypoechogenic areas in the thyroid gland. Moreover, the serum IgG4 level was examined in three patients (Cases 5, 6 and 7), and two had elevated concentrations >135 mg/dL. Although some features were typical, the eight cases in Group B demonstrated relatively incomplete clinical characteristics of IgG4 thyroiditis.
Summary of Clinicopathological Features of Group B (8 Cases)
GI, Group I, TSH >5.00 mIU/L; GII, Group II, 0.3 ≤ TSH ≤5.00 mIU/L; GIII, Group III, TSH <0.3 mIU/L.
MS, marked swelling; TS, tracheal stenosis.
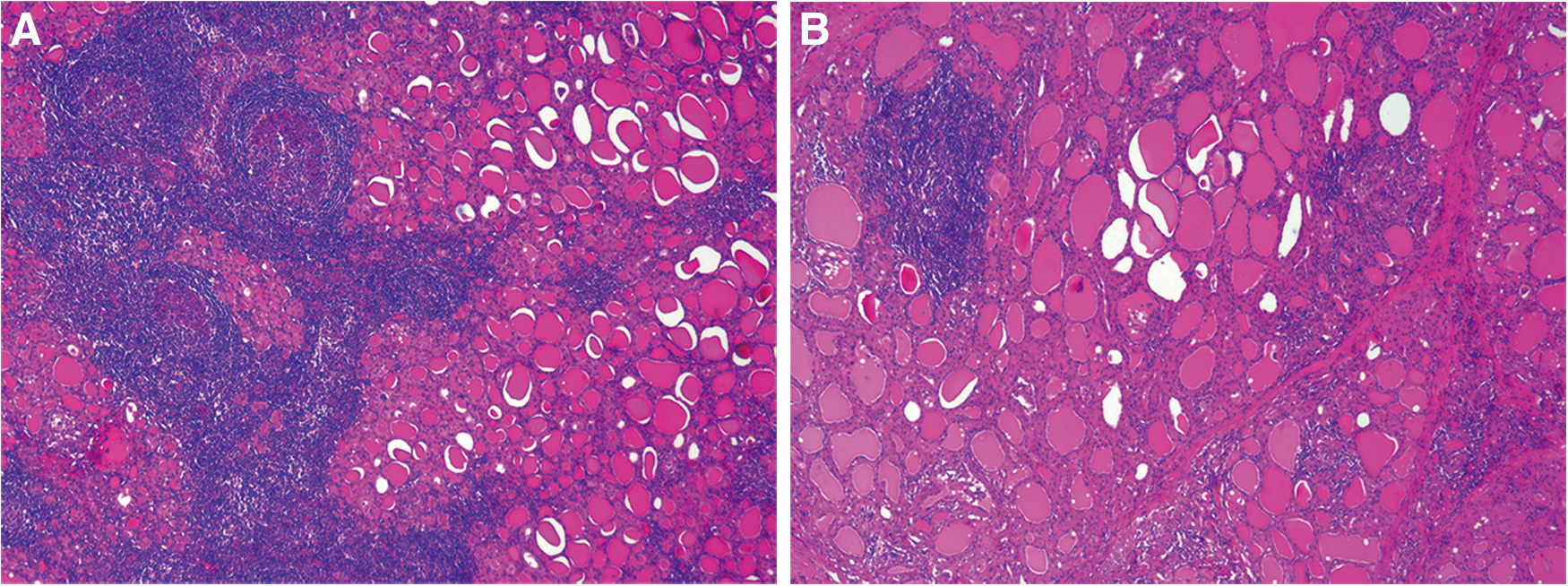
However, based on the histological examination of the same group, the majority of the cases (6/8; Cases 1, 2, 3, 4, 5, and 7) had marked lymphoplasmacytic infiltration, variable stromal fibrosis, notable follicular cell degeneration, and numerous microfollicles (Fig. 2), which are considered to be the typical histopathological features of IgG4 thyroiditis. The most common pattern of stromal fibrosis observed in these cases was predominant interfollicular fibrosis (5/6; Cases 1, 2, 3, 4, and 5). Of note, in Case 5 (Fig. 2B), the fibrous elements were slightly less dense than the common sclerotic areas found in other cases. Similarly, in Case 7 (Fig. 2C), although stromal fibrosis was predominantly the interlobular type, small bands of sclerotic tissue were diffusely identified between the interfollicular spaces. There were only two cases (Case 6 and Case 8, respectively) demonstrating major scar fibrosis and interlobular fibrosis. The thyroid follicles were almost normal in size in these two cases.

Histopathological features of Group B.
In Group C, the two patients were elderly females with disease durations between 5 and 10 years. The titers of circulating antibodies were elevated in both patients, whereas euthyroidism was found biochemically and diffuse coarse echogenicity was identified on ultrasound (Table 4). Moreover, as shown in Figure 3, histological examination revealed mild to moderate lymphoplasmacytic infiltration, negligible to mild interlobular type stromal fibrosis, lymphoid follicle formation, and oxyphilic change of the follicular epithelium. These morphological features are consistent with the histological diagnosis of HT but insufficient for a diagnosis of IgG4 thyroiditis with massive sclerosis and destructive changes.
Histopathological features of Group C. Both Case 1
Summary of Clinicopathological Features of Group C (2 Cases)
GI, Group I, TSH >5.00 mIU/L; GII, Group II, 0.3 ≤ TSH ≤5.00 mIU/L; GIII, Group III, TSH <0.3 mIU/L.
MS, marked swelling; NL, nodular lesion.
Furthermore, although the IgG4+/IgG+ plasma cell ratio exceeded 40%, and the absolute number of IgG4+ plasma cells was between 10/HPF and 20/HPF, which were sufficient to suggest an increase in IgG4+ plasma cells according to the CVC, neither case was able to be categorized as RT, fibrotic HT, or thyroid manifestation of systematic IgG4-RD. The central pathology features, including obliterative phlebitis and storiform fibrosis, were not observed in these cases.
Discussion
More than 100 years ago, in his well-known original report on HT, Dr. Hakaru Hashimoto pointed out the histopathological similarity with Mikulicz's disease (22), which was recently demonstrated to be IgG4-RD. Since our first description of IgG4 thyroiditis in 2009, the identification of IgG4-rich inflammation in the thyroid gland has attracted growing interest. However, the determination of the true prevalence of IgG4 thyroiditis remains a challenge, as the heterogeneity of the histological criteria for diagnosing IgG4 thyroiditis adopted in different studies represents a major factor accounting for epidemiological discrepancies (23).
In our original retrospective clinical study, based on the cutoff values of IgG4+ plasma cells >20/HPF and an IgG4+/IgG+ plasma cell ratio >30% (CVT), 27.1% of patients with HT (19/70) were diagnosed with IgG4 thyroiditis (18). Later, a study from China reported a similar prevalence, with 22.6% of patients with HT (12/53) having IgG4-rich inflammation according to the same diagnostic threshold (16). In contrast, a research group from Germany reported a considerably lower incidence of IgG4 thyroiditis of 12.6% (24/191) in their cohort by defining IgG4+ plasma cells >20/HPF and an IgG4+/IgG+ plasma cell ratio >40% as increased IgG4 in thyroid tissue (24). Furthermore, a study from the United States considered IgG4+ plasma cells >30/HPF or an IgG4+/IgG+ plasma cell ratio >30% to be diagnostic, and the incidence of HT with an increased IgG4 plasma cell count in their study was 36.4% (8/22) (25). However, it must be noted that selection bias results in a relatively higher prevalence of IgG4 thyroiditis in the mentioned reports, as these studies were retrospective pathological analyses using surgical specimens in which more patients with severe clinical manifestations, such as marked swelling or tracheal stenosis, were enrolled and milder cases may have been overlooked.
Very recently, two prospective studies from Japan evaluating serum IgG4 concentrations in patients with HT were conducted. Takeshima et al. demonstrated that only 6 of 149 (4%) unselectively evaluated patients with HT had increased serum IgG4 levels >135 mg/dL (26). Kawashima et al. showed a similar incidence rate (5.4%, 5/94) (27). Thus, it is important to emphasize that the true prevalence of IgG4 thyroiditis may be lower in routine practice than that in our cohort. Other possible reasons for the epidemiological discrepancies are genetic, dietary, and geographic differences among studies.
Establishing thyroid-specific diagnostic criteria is important to improve our understanding of the epidemiology and pathophysiology of IgG4 thyroiditis, as well as to elicit clinical awareness of this unique entity. In this study, we validated the CVC and CVT for diagnosing IgG4 thyroiditis associated with HT in a large cohort of patients. According to the CVC and CVT, the 120 cases of HT were categorized into four groups. Twenty-five cases (25/120, 20.83%) satisfying both cutoff values comprised Group A and are thought to have definite IgG4 thyroiditis. On the contrary, there were 85 cases (85/120, 70.83%) who did not meet either of the cutoff values. We refer to this subset as Group D and suggest a definitive diagnosis of non-IgG4 thyroiditis. The remaining 10 cases with borderline IgG4+ cell counts only met one of the two thresholds. We propose these cases to be borderline lesions, and refer to them as Group B (8/120, 6.67%) and Group C (2/120, 1.67%).
Clinical, serological, sonographic, and histopathological characteristics of IgG4 and non-IgG4 thyroiditis were compared. Our study reveals that both the CVC and CVT can identify the IgG4 thyroiditis group with the same distinct phenotypes described in our previous reports (18,19). This suggests that the CVC and CVT are equally efficient for diagnosing IgG4 thyroiditis in HT because the included diagnostic criteria can distinguish a group of cases with unique clinical and histological features. As stated in the proposal on comprehensive diagnostic criteria (15), our findings highlight the practical utility of the CVC for clinicians who may not be familiar with the CVT when diagnosing a patient with IgG4 thyroiditis.
From the standpoint of a pathologist, we recommend an evaluation including IgG4 immunostaining and simultaneous use of the CVC and CVT because this permits to better identify early phase IgG4 thyroiditis. In Group B, we found TSH levels within the reference range under LT4 treatment in six cases, and diffuse coarse echogenicity in three cases. However, the histological changes in the majority of these cases were similar to those observed in representative IgG4 thyroiditis, but with less sclerotic changes in the interfollicular area. We propose that similar conditions in the eight cases in Group B represent an “early phase” of IgG4 thyroiditis, and that morphological evolution from a predominantly lymphoplasmacytic infiltration with little fibrosis to markedly dense interfollicular sclerosis may occur in this group. When encountering such cases, making a descriptive diagnosis followed by the qualifier “with increased IgG4+ plasma cells” (with a report indicating the actual numbers) and advising further clinical examination and follow-up are recommended to pathologists.
Awareness of this subset is also important for clinicians because a major determinant of treatment effectiveness is the degree of fibrosis. Patients in whom fibrosis is well established are less likely to respond to glucocorticoids (28 –30). Therefore, it is possible that early detection and intervention can improve the treatment management and prognosis of these patients. Ultimately, it is worth emphasizing that a case meeting the threshold of IgG4 staining alone does not qualify for a diagnosis of IgG4 thyroiditis. Strehl et al. reported an increased number of IgG4+ plasma cells in many nonspecific diseases and neoplastic disease (31).
When confronted with patients such as the two in Group C who exhibited neither morphological nor clinical features compatible with IgG4 thyroiditis, clinicians should interpret the immunostaining results cautiously (32). Although no consensus regarding glucocorticoid therapy in IgG4-rich inflammatory thyroid lesions has been established yet, several reports have demonstrated that glucocorticoid treatment might improve local symptoms such as rapidly progressive thyroid swelling and thyroid pain, or hypothyroidism of patients with IgG4 thyroiditis or so-called IgG4-related thyroiditis (3,11,12). However, patients who were categorized in Group C should not be considered as candidates for glucocorticoid therapy, because there is no evidence indicating that they will benefit from this type of treatment.
To improve evidence-based diagnostic criteria for IgG4 thyroiditis, we have summarized the clinicopathological features as diagnostic clues in Table 5. We provide a more practical tool for both pathologists and treating clinicians to recognize this distinct entity. Typical IgG4 thyroiditis cases exhibit almost all of the characteristics listed in this table as, for example, illustrated by the first case of IgG4 thyroiditis reported in a non-Asian patient by Luiz et al. (12). However, in most situations, patients may only exhibit some clinicopathological features or have a borderline IgG4+ plasma cell count. The dialogue between the pathologists and clinicians becomes essential, and an accurate diagnosis of IgG4 thyroiditis requires a combination of clinical, laboratory, imaging, and histological features; however, a satisfactory morphology together with a large number of IgG4+ plasma cells remains the gold standard for diagnosis. Serological IgG4 levels, imaging findings, or response to steroids may help in establishing the diagnosis if tissue samples are not available.
Clues for Diagnosis of IgG4 Thyroiditis in Patients with Hashimoto's Thyroiditis
Storiform fibrosis and obliterative phlebitis have been recognized as major pathological features of IgG4-RD in other organs (14). However, typical storiform fibrosis is rare, and no evidence of obliterative phlebitis was identified in the IgG4 thyroiditis cases in this study or previous reports (16,24). Moreover, there are no reports on extrathyroid involvement in HT patients with IgG4-rich inflammation in thyroid tissue, suggesting that IgG4 thyroiditis is an organ-specific form of IgG4-rich inflammation (16,24,33). Although the underlying etiology of IgG4+ plasma cell-rich inflammation in the thyroid remains unclear, Inomata et al. from our group recently reported that the major autoantigen recognized by serum IgG4 antibodies in patients with IgG4 thyroiditis is thyroglobulin and its isoforms (34). This observation may explain the solitary nature of IgG4 thyroiditis and will be the first step to elucidate the pathogenesis of IgG4 thyroiditis.
In conclusion, we retrospectively reviewed 120 cases of HT, and determined the clinicopathological phenotypes of IgG4 thyroiditis using the CVC and CVT. Although the different cutoff values can precisely distinguish the IgG4 thyroiditis group with the same set of unique clinical and pathological features, the thyroid-specific cutoff value can more efficiently identify borderline cases, which may represent an “early phase” of IgG4 thyroiditis. We, therefore, propose a new series of diagnostic clues for both endocrinologists and pathologists to improve the recognition of IgG4 thyroiditis in HT in clinical practice, and to prompt further investigation of potential alternative therapeutic options for patients in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China Grant No. 81300647 and a Startup Foundation for Young Scientists from Taishan Medical University to Y.L.