
Abstract
Background:
Mandatory universal salt iodization (USI) has been implemented in China for 20 years. Although iodine deficiency disorders are effectively controlled, the risk of excess iodine have been debated.
Methods:
A nationally representative cross-sectional study with 78,470 enrolled participants, aged 18 years or older, from all 31 provincial regions of mainland China was performed. The participants were given a questionnaire and underwent B-mode ultrasonography of the thyroid. Serum concentrations of thyroid hormones, thyroid antibodies, and urine iodine concentration (UIC) were measured.
Results:
The median UIC of the adult population was 177.89 μg/L. The weighted prevalence of thyroid disorders in adults were as follows: 0.78% of overt hyperthyroidism, 0.44% of subclinical hyperthyroidism, 0.53% of Graves' disease, 1.02% of overt hypothyroidism, 12.93% of subclinical hypothyroidism, 14.19% of positive thyroid antibodies, 10.19% of positive thyroid peroxidase antibodies, 9.70% of positive thyroglobulin antibodies, 1.17% of goiter, and 20.43% of thyroid nodules. Iodine excess was only associated with higher odds of overt hyperthyroidism and subclinical hypothyroidism, while iodine deficiency was significantly associated with higher odds of most thyroid disorders. In addition, increased iodine intake was significantly associated with elevated serum thyrotropin levels but was inversely associated with thyroid antibodies and thyroid nodules.
Conclusions:
The long-term mandatory USI program with timely adjustments is successful in preventing iodine deficiency disorders, and it appears to be safe. The benefits outweigh the risks in a population with a stable median iodine intake level of up to 300 μg/L.
Introduction
Iodine is a trace element that is essential for thyroid hormone synthesis and an indispensable component of the microenvironment for thyroid cell function. At both ends of the spectrum, inadequacy or excess of iodine intake can lead to thyroid disorders (1,2). As a country suffering from mild-to-moderate iodine deficiency, China implemented universal salt iodization (USI) legislation nationally in 1996, covering all 31 provincial regions of mainland China. The success of USI was honored by that 28 provinces had reached the goal of eliminating iodine-deficient disorders (IDD) and the other 3 were close to this goal, according to the data collected by 2010 (3).
During the two decades of USI enactment, the Chinese population has been consecutively exposed to an iodine nutrition status of excessive iodine intake (EI; median urine iodine concentration [UIC] ≥300 μg/L) for 5 years (1996–2001), more than adequate iodine intake (MAI; median UIC 200–299 μg/L) for 10 years (2002–2011), and adequate iodine intake (AI; median UIC 100–199 μg/L) for 5 years (2012–2016) (Supplementary Fig. S1) (3,4). Twenty years after the commencement of USI, the present cross-sectional study at the national scale across China, conducted between 2015 and 2017 by the Chinese Society of Endocrinology and the Chinese Thyroid Association, aims to re-evaluate the current situation of iodine nutrition and the prevalence of thyroid disorders, as well as the relationships between them.
Materials and Methods
Study population
The entire study advanced through four stages of random sampling from urban and rural locations in parallel (Supplementary Fig. S2). At the first stage, 31 cities were selected and divided into 10 developed, 13 developing, and 8 underdeveloped cities, based on population size and economical levels. At the second stage, one district was randomly selected from each city. At the third stage, two residential communities were randomly selected from the district. And at the final stage, eligible individuals who met the inclusion criteria were randomly selected and stratified by age and sex. The age and sex composition of each community and the urban–rural ratio were decided referring to the 2010 China's national census data (5). A parallel random sampling was performed in rural locations. The inclusion criteria of the adult respondents were as follows: aged 18 years or older, living in the selected community for at least 5 years, having not received iodine drugs or contrast agents within 3 months, and nonpregnant women. In addition, sixty 9- to 11-year-old school-children in each province were randomly selected to evaluate the local iodine status according to the World Health Organization/Iodine Global Network (IGN)/United Nations International Children's Emergency Fund (UNICEF) recommendation. The research protocols were approved by the Medical Ethics Committee of China Medical University. All subjects were provided written informed consent following a thorough explanation of the research procedures. Some measures were taken to ensure the project quality. First, the investigation team of each province received centralized training. Second, a standardized investigation protocol for each province ensured consistency. Third, data entry was subjected to double checking to ensure the accuracy and authenticity. Finally, the center sent supervision personnel to each survey site for quality control.
The content of the standard questionnaire included demographic characteristics, personal and family medical history of thyroid disorders, current smoking status, family income, education levels, and household salt consumption. From each participant, fasting blood and spot urine samples were collected. Sera were obtained by centrifugation of the blood samples and preserved at −20°C before further processing. Upon completion of the survey and specimen collection, all specimens were airlifted by the cold chain system to the central laboratory in Shenyang, China, for centralized testing. All participants underwent thyroid ultrasonography by qualified observers, who had trained and passed examination in the project center, using a portable instrument (LOGIQ 100 PRO; GE, Milwaukee, WI with 7.5 MHz linear transducers). In each province, sixty 9- to 11-year-old school-children were sampled for B-mode ultrasonography examination of the thyroid gland and fasting urine collection.
Laboratory tests
Serum thyrotropin (TSH), thyroid peroxidase antibodies (TPOAb), and thyroglobulin antibodies (TgAb) were measured using an electrochemiluminescence immunoassay on a Cobas 601 analyzer (Roche Diagnostic, Switzerland), in the central laboratory in Shenyang. Free thyroxine (fT4) and free triiodothyronine (fT3) levels were measured only if TSH was outside the reference range. TSH receptor antibodies (TRAb) were tested in subjects with TSH below 0.27 mIU/L. The reference ranges for TSH, fT4, fT3, TPOAb, TgAb, and TRAb were 0.27–4.2 mIU/L, 12.0–22.0 pmol/L, 3.1–6.8 pmol/L, <34.0 IU/mL, <115.0 IU/mL, and ≤1.75 IU/L, respectively, and provided by the test kit manufacturers. The functional sensitivity of the serum TSH assay was 0.014 μIU/mL. The repeatability of serum assays of TSH, fT4, fT3, TPOAb, TgAb, and TRAb was ensured by intra-assay coefficients of variation (CV) of 1.1–6.3% and inter-assay CV of 1.9–9.5%. UIC was determined using inductively coupled plasma mass spectrometry (Agilent 7700x; Agilent Technologies, Santa Clara, CA). The measurement quality was controlled against the certified reference material (GBW09108, GBW9109, and GBW9110) from the Center for Disease Control in China. The target values of the standards were 70.8 ± 9.0, 143 ± 10, and 224 ± 14 μg/L, with an inter-assay CV of 2.3%, 2.5%, and 2.4%, and an intra-assay CV of 2.7%, 1.4%, and 2.3%, respectively. The specimens were analyzed in the order of arrival. We performed quality controls three times (before, during, and after) for each test, and three samples were randomly selected from high, middle, and low values to re-analysis after each procedure.
Clinical diagnosis
The diagnostic criteria for thyroid disorders are listed in Supplementary Table S1.
Statistical analyses
To obtain national estimates, all calculations were weighted to represent the overall Chinese adult population aged 18 years or older using the weighted coefficients derived from the 2010 China population census data and the sampling scheme of the current survey. Standard errors were calculated with appropriate statistical techniques with data from the complex survey design. Categorical data presented as counts and percentages were analyzed with the chi-square test and Fisher's exact test, as appropriate. The statistical significance of differences between continuous variables was assessed by analysis of variance. Adjusted odds ratios (ORs) with 95% confidence interval [CI] were calculated by multivariable logistic regression to examine the association between the four UIC categories with the prevalence of thyroid disorders. Two models with progressively increased adjustment of risk factors were applied. A p-value of <0.05 was considered statistically significant. All statistical analyses were conducted using Statistical Analysis System version 9.3 (SAS Institute, Inc.) and SUDAAN software version 10.0 (Research Triangle Institute).
Results
With an overall response rate of 92.08%, 80,937 participants had completed the study. Among them, 2467 subjects were excluded owing to missing information on sex, age, or thyroid function tests and 78,470 samples remained eligible for analysis (Supplementary Fig. S2).
As shown in Table 1, the median UIC in school-age children was 199.75 μg/L [CI 128.41–303.37 μg/L], with a goiter prevalence of 3.50% [CI 2.93–4.13%]. The median UIC in the adult population was 177.89 μg/L [CI 117.99–263.90 μg/L], and the prevalence of goiter was 1.17% [CI 0.95–1.43%]. Judged by the median UIC in school-age children, 16, 11, and 4 provinces were defined as having an iodine status of AI, MAI, and EI, respectively, and none of deficient iodine intake (DI), defined as a median UIC <100 μg/L (Fig. 1). In the adult population, the distribution of iodine status of DI, AI, MAI, and EI, as revealed by the UIC levels, was 17.82% [CI 15.78–20.06%], 40.21% [CI 38.68–41.77%], 23.23% [CI 21.77–24.76%], and 18.74% [CI 16.87–20.75%], respectively.

Current iodine nutrition status in mainland China according to median UIC in school-age children. UIC, urine iodine concentration.
Demographic Characteristics and Iodine Status of Subjects
AI, adequate iodine intake; CI, 95% confidence interval; EI, excessive iodine intake; MAI, more than adequate iodine intake; UIC, urine iodine concentration.
As displayed in Table 2, the overall prevalence of overt hyperthyroidism, subclinical hyperthyroidism, and Graves' disease was 0.78% [CI 0.69–0.87%], 0.44% [CI 0.37–0.51%], and 0.53% [CI 0.47–0.61%], respectively. The prevalence of overt hyperthyroidism (1.00% vs. 0.55%, p = 0.0003), subclinical hyperthyroidism (0.58% vs. 0.29%, p < 0.0001), and Graves' disease (0.69% vs. 0.38%, p = 0.001) was significantly higher in women than in men. The prevalence of overt hyperthyroidism (p = 0.005 for trend) and Graves' disease (p = 0.01 for trend) decreased with age. The multivariable-adjusted analysis indicated that DI was significantly associated with overt hyperthyroidism (OR = 1.53 [CI 1.15–2.04], p = 0.005) and Graves' disease (OR = 1.77 [CI 1.20–2.60], p = 0.005), while EI was significantly associated with overt hyperthyroidism (OR = 2.05 [CI 1.59–2.63], p < 0.0001) (Table 3).
Age- and Sex-Standardized Prevalence of Thyroid Disorders and Risk Factors in the Chinese Adult Population
Compared with the 100–199 μg/L group, the prevalence had no significant difference (p > 0.05).
Compared with the 100–199 μg/L group, the prevalence was significantly lower (p < 0.05).
Never-smoker was defined as having smoked <100 cigarettes in one's lifetime; occasional smoker was defined as having smoked at least 100 cigarettes in one's lifetime and smoking <20 cigarettes per day; regular smoker was defined as having smoked at least 100 cigarettes in one's lifetime and smoking ≥20 cigarettes per day.
The BMI is the weight in kilograms divided by the square of the height in meters.
BMI, body mass index.
Odds Ratios of Thyroid Disorders Among Stratified Urine Iodine Concentration Groups
Model 1: Adjusted for age and sex.
Model 2: Adjusted for age, sex, location, education level, income, consumption of iodized salt, family history of thyroid disease, cigarette smoking, and BMI.
DI, deficient iodine intake; OR, odds ratio; TgAb, thyroglobulin antibodies; TPOAb, thyroid peroxidase antibodies.
Concerning hypothyroidism, the overall prevalence of overt hypothyroidism and subclinical hypothyroidism was 1.02% [CI 0.88–1.18%] and 12.93% [CI 11.99–13.94%], respectively. Women had a significantly higher prevalence of overt hypothyroidism (1.53% vs. 0.53%, p < 0.0001) and subclinical hypothyroidism (16.06% vs. 9.87%, p < 0.0001) than men. Unlike hyperthyroidism, the prevalence of both overt hypothyroidism (p < 0.0001 for trend) and subclinical hypothyroidism (p = 0.005 for trend) increased with age (Table 2). Significant associations were found between DI and overt hypothyroidism (OR = 1.49 [CI 1.12–1.98], p = 0.007), and between EI and subclinical hypothyroidism (OR = 1.37 [CI 1.22–1.55], p < 0.0001) (Table 3). According to the National Academy of Clinical Biochemistry (NACB) standards, the reference interval of serum TSH derived in this study was 0.74–7.04 mIU/L and is affected by age, sex, heredity, and other factors. Iodine intake is one of the most important factors. Serum TSH levels increased significantly with the increase of iodine intake (Fig. 2A). Furthermore, the association was only found in nonautoimmune subclinical hypothyroidism (negative thyroid antibodies) but not in autoimmune subclinical hypothyroidism (positive thyroid antibodies) (Fig. 2B).
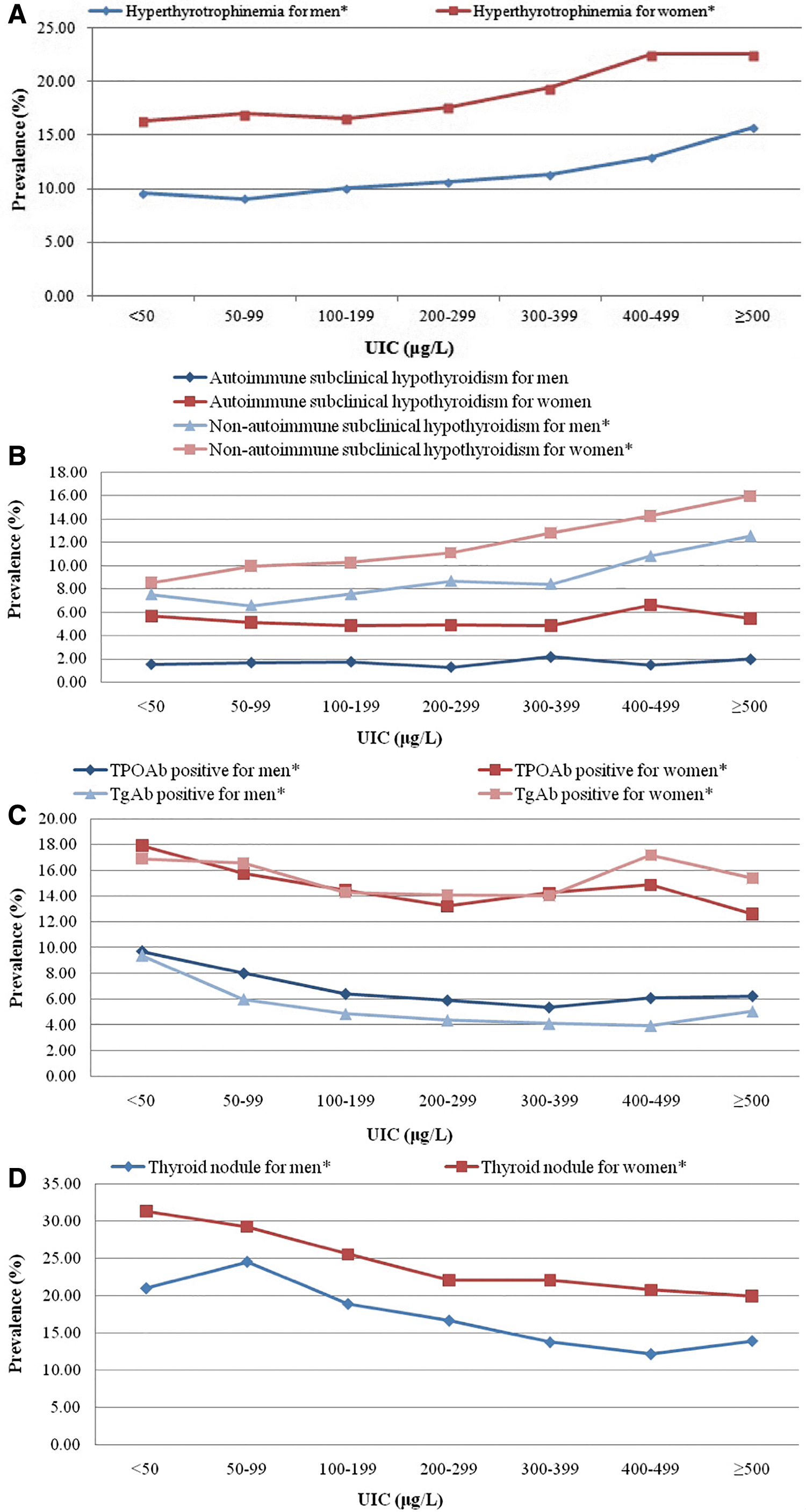
Age-standardized prevalence of thyroid disorders in male and female Chinese adult population stratified by UIC. (
The overall prevalence of positive thyroid antibodies was 14.19% [CI 13.74–14.66%], significantly higher in women than in men (20.35% vs. 8.16%, p < 0.0001), and increasing with age (p < 0.0001 for trend) (Table 2). In addition, positive TPOAb and TgAb were detected in 10.19% [CI 9.80–10.59%] and 9.70% [CI 9.28–10.13%] of the subjects, respectively, with a female dominance (14.17% vs. 6.29% for TPOAb and 14.71% vs. 4.80% for TgAb). DI was significantly associated with positive thyroid antibodies (OR = 1.19 [CI 1.06–1.32], p = 0.004), TPOAb (OR = 1.19 [CI 1.05–1.34], p = 0.008), and TgAb (OR = 1.20 [CI 1.05–1.37], p = 0.009), while MAI was inversely associated with positive thyroid antibodies (OR = 0.91 [CI 0.84–0.98], p = 0.01) and TPOAb positivity (OR = 0.90 [CI 0.81–0.99], p = 0.04) (Table 3). A decreased trend between the stratified UIC category and the positivity rates of TPOAb and TgAb among men and women is shown in Figure 2C (p < 0.05 for trend).
A similar sex disparity appeared in the prevalence of thyroid nodules, which was significantly higher in women than in men (23.68% vs. 17.24%, p < 0.0001), with an overall prevalence of 20.43% [CI 18.39–22.63%], and increasing with age (p < 0.0001 for trend). DI was positively associated with thyroid nodules (OR = 1.27 [CI 1.19–1.37], p < 0.0001), while MAI (OR = 0.88 [CI 0.80–0.97], p = 0.01) and EI (OR = 0.74 [CI 0.65–0.85], p = 0.0001) were associated with a lower prevalence of thyroid nodules (Table 3). Figure 2D depicts a significant decreasing trend of the association between UIC and thyroid nodules among men and women (p < 0.05 for trend).
As shown in Supplementary Figure 2, there was no significant increase in the prevalence of all thyroid disorders in the UIC 200–299 μg/L group compared with the 100–199 μg/L group.
Discussion
In the present study, the very high response rate of 92.08% was the result of a joint effort by all stakeholders. The median UIC of school-age children and adults was 199.75 and 177.89 μg/L, with a goiter prevalence of 3.50% and 1.17%, respectively, which evidently demonstrates an adequate iodine status in current mainland China. The balanced frequencies of iodine deficiency (17.82%) and iodine excess (18.74%) are in keeping with the spontaneous variation in UIC, which suggests that the main result is reliable and reflects that the population is iodine replete. In addition, sociodemographic factors did not affect the prevalence of thyroid disorders, which might highlight the implementation of the consistency for USI (Supplementary Table S2). Although USI has been successfully implemented, ongoing caution is needed that there are potential side effects of EI by USI.
Reports based on epidemiological studies from a number of countries have pointed out that high iodine intake can lead to an increased risk for the development of thyroid disorders, including hyperthyroidism, hypothyroidism, and autoimmune thyroiditis (1,2,6). Compared with our previous findings collected in 1999, the prevalence of overt thyroid dysfunction and thyroid autoantibodies remained stable (Supplementary Table S3); these results reinforce the safety and efficacy of USI application in the prevention of IDD. However, there was a remarkably increased prevalence of subclinical hypothyroidism and thyroid nodules in the present study using the same method of evaluation in the two time periods (Supplementary Table S4) (7).
DI and EI were associated with higher prevalence of overt hyperthyroidism resulting in an U-shaped curve. However, Graves' disease was only associated with DI, but not EI. This could be explained by the fact that autoantibodies play an important role in Graves' disease, and the elevated positive thyroid antibodies were also only associated with DI. Meanwhile, the prevalence of subclinical hyperthyroidism was not affected by iodine intake.
In iodine-sufficient countries, the prevalence of overt hypothyroidism ranges from 0.2% to 10.94%, with 0.3% to 3.7% in the United States and 0.2% to 5.3% in Europe, with a wide spectrum due to differences in diagnostic criteria and dietary iodine intake (6,8 –10). In our cross-sectional study of the data collected in 1999, the prevalence of overt hypothyroidism was 1.03% and increased incrementally with higher iodine intake, but not in the 5-year follow-up study in 2004 (7). In keeping with this observation, the prevalence of overt hypothyroidism was 1.02% in the current study, and MAI and EI did not confer a higher risk. Nevertheless, DI remains the major hazard for developing overt hypothyroidism.
The prevalence of subclinical hypothyroidism reported in the literature varies greatly due to the use of different TSH reference values (11). Based on a reference range of 0.27–4.20 mIU/L provided by the manufacturer, the prevalence of subclinical hypothyroidism calculated in this study was 12.93%, lower than 16.7% in 2010, but much higher than the 3.21% reported by our group in 1999 (7,12). As early as 2008, we reported a concomitant increase of TSH levels with higher iodine intake (13). A very high reference range for TSH of 0.73–7.04 mIU/L established based on the NACB criteria was found in this study, which is comparable to the TSH range of 0.62–6.84 mIU/L recently reported by a study from South Korea, and presumably due to a high iodine intake in both countries (14). The present study found that the prevalence of subclinical hypothyroidism increased with improved iodine intake, which was only seen in nonautoimmunity individuals, but not in autoimmune individual (Fig. 2C). This phenomenon suggests that iodine-induced nonautoimmune subclinical hypothyroidism is not the result of thyroid autoimmunity. Our animal studies showed that chronic high iodine intake could inhibit type 2 deiodinase activity in the pituitary, which leads to decreased thyroxine to triiodothyronine conversion and increased production of TSH (15).
The increased frequency of thyroid autoimmunity following salt iodization programs was demonstrated in evidence provided by some studies, whereas higher risk of thyroid autoimmunity in populations with DI was reported in studies from others (16 –21). The present study demonstrates that the prevalence of positive thyroid antibodies decreased with an increased iodine intake, accompanied by an individual decrease of TPOAb and TgAb. Nevertheless, DI still remains a risk factor for the occurrence of both antibodies. These results suggest that the relationship between iodine intake and thyroid autoimmunity is similar to the relationship between iodine intake and hyperthyroidism. Most studies have proved that iodine-induced hyperthyroidism is a transient phenomenon. The prevalence of hyperthyroidism rose sharply after iodine supplementation. However, after 3–5 years, the prevalence of hyperthyroidism dropped back to the level before iodine supplementation. It was found in present study that iodine-induced thyroid autoimmunity also presented transient tendency. After 20 years of iodine supplementation, the prevalence of thyroid-positive antibodies has fallen back to pre-iodine supplementation levels. Therefore, we concluded that long-term iodine supplementation might not increase thyroid autoimmunity, because the thyroid gland and immune system have been adapted to the elevated iodine nutritional environment.
A very high prevalence of thyroid nodules of 20.43% was found in this study, which is in line with 19.0–46.6%, reported in most countries (22 –24). A similar prevalence of thyroid nodules (22.70%) was also discovered in our previous meta-analysis of 52 studies from 14 provinces in China (25). The high prevalence of thyroid nodules could not be attributed to the increase of iodine intake given that an increased iodine intake is a protective factor against the development of thyroid nodules. We used the same resolution (7.5 MHz) ultrasound equipment to evaluate the thyroid nodules with the same diagnostic criteria (>5 mm in diameter) in 1999 and this study; however, the causes of the increased prevalence of thyroid nodules require further study.
In the light of the compelling evidence provided by Zimmermann et al. (26), the IGN and UNICEF have proposed a combination of MAI and AI into a single category to denote adequate iodine nutrition. By presenting a new piece of evidence that the prevalence of thyroid disorders in adult populations is not distinguishable between MAI and AI in this study, we support that AI and MAI can be merged as an indicator of iodine adequacy, that is, iodine intake within the range of 100–299 μg/L. Raising the upper limit of iodine intake has profound significance for pregnant women whose iodine intake should be maintained between 150 and 249 μg/L (27).
Several limitations and constraints are recognized in the study. First, the epidemiological survey at such a massive national scale is methodologically challenged by the control of the geographical, environmental, genetic, and other factors, which may influence the disease outcomes, thus caution should be exercised when interpreting the results. Second, patients with thyroid nodules did not undergo further evaluation but were simply advised to follow at a local hospital. Third, as a cross-sectional survey, this study was not able to unveil the mechanisms involved in the observed phenomena. Finally, individuals with differences in iodine status before the implementation of USI might affect the prevalence of thyroid disorders.
In conclusion, 20 years of mandatory USI program in China has successfully transformed and corrected the iodine intake of the population from deficiency into adequacy, thereby resulting in a decrease of the prevalence of most thyroid disorders. Excessive iodine is only associated with a higher prevalence of overt hyperthyroidism and subclinical hypothyroidism. However, iodine deficiency is a risk factor for most thyroid disorders indicating that the risk of iodine deficiency clearly outweighs that of iodine excess. Iodine supplementation is necessary not only to prevent IDD but also to reduce the prevalence of thyroid disorders, especially for the higher thyroid nodule prevalence of 20.43%. Our findings also support combining AI and MAI into a single category to indicate an optimal iodine intake for the general population. Needless to say, continuous monitoring of the iodine status at the population levels is needed.
Footnotes
Acknowledgments
We thank the participants of this study. For continuous support, assistance, and cooperation, we thank Jiang He and Chung-Shiuan Chen (Tulane University); Wei Gong, Chenling Fan, Hong Wang, Hongmei Zhang, Shuangning Ding, Xiaochen Xie, and Tingting Liu (The First Hospital of China Medical University); Caiping Li and Jian Huangfu (The Affiliated Hospital of Inner Mongolia University); Nan Jin (Chinese PLA General Hospital); Wuquan Deng and Fang Deng (Third Military Medical University); Haicheng Zhou (The First Affiliated Hospital of Dalian Medical University); Qingling Lu (Cardiovascular and Cerebrovascular Disease Hospital of Ningxia Medical University); Yunfeng Shen (The Second Affiliated Hospital of Nanchang University); Guodong Liu (The First Affiliated Hospital of Harbin Medical University); Junxiu Hou and Zhiqiang Zhang (The Affiliated Hospital of Inner Mongolia Medical University); Hong Zhang (The Second Xiangya Hospital); Xiaodong Mao, Qifeng Wang, and Kun Wang (Nanjing University of Chinese Medicine); Yanping Wang (Fujian Medical University Union Hospital); Xiaojun Ma (The First Affiliated Hospital of Zhengzhou University); Liheng Meng (First Affiliated Hospital of Guangxi Medical University); Weihua Linle and Tuanyu Fang (Hainan General Hospital); Xingjun Liu and Yanru Zhao (The First Affiliated Hospital of Xi'an Jiaotong University); Lulu Chen, Jiaoyue Zhang, and Hanyu Wang (Huazhong University of Science and Technology); Jingfang Liu and Songbo Fu (The First Hospital of Lanzhou University); Qingguo Lv (West China Hospital); Chenglin Sun (The First Hospital of Jilin University); Qiuming Yao and Ronghua Song (Shanghai University of Medicine and Health Science Affiliated Zhoupu Hospital); Tingting Chen (The First Hospital of Anhui Medical University); Ben Niu (The First People's Hospital of Yunnan Province); Mingtong Xu and Feng Li (Sun Yat-sen Memorial Hospital); Lizhen Lan (The First Hospital of Shanxi Medical University); Jun Yue and Jia Song (People's Hospital of Tibet Autonomous Region); Yanan Li and Wei Luo (Qinghai Provincial People's Hospital); Xiaoming Lou and Zhe Mo (Zhejiang Provincial Center for Disease Control and Prevention); Nianchun Peng and Lixin Shi (Affiliated Hospital of Guiyang Medical University); Mian Wang, Qiuxiao Zhu, and Lingling Yuan (Second Hospital of Hebei Medical University); Haiqing Zhang (Shandong Provincial Hospital Affiliated with Shandong University); Yong Fan (The First Affiliated Hospital of Xinjiang Medical University); and Hongyan Wei (Tianjin Medical University General Hospital).
Authors' Contributions
Z.Y.S., W.P.T., Y.Z.L., G.N., Y.M.M., J.J.Z., X.C.T., D.T., and X.G.S. conceived and designed the study. Z.Y.S. and W.P.T. supervised the study. Z.Y.S., W.P.T., and Y.Z.L. did the statistical analyses. All authors contributed to acquisition, analysis, or interpretation of data. Z.Y.S. and W.P.T. drafted the article. All authors revised the report and approved the final version before submission.
Author Disclosure Statement
The authors hereby confirm that no part of this article has been published or is under consideration for publication elsewhere. The authors have no potential conflicts of interest to declare.
Funding Information
This work is supported by the Research Fund for Public Welfare from the National Health and Family Planning Commission of China (Grant No. 201402005).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4