
Abstract
Background:
Six to 20% of thyroid cancer (TC) patients develop distant metastases, and one-third become radioiodine refractory (RAIR). Available targeted therapies increase progression-free survival but are associated with toxicities. This study aims to characterize clinical, pathological, and molecular profiles of patients with RAIR TC.
Methods:
Data of TC patients seen during 2013–2017 at two tertiary care centers were retrospectively analyzed. Patients were considered RAIR according to American Thyroid Association guidelines. The control cohort was sex matched and age matched and had either regression or stable disease (by Response Evaluation Criteria in Solid Tumors) on follow-up at least three years after initial therapy. Molecular profiles on a subset of RAIR patients were reviewed.
Results:
Compared with 22 matched controls, 54 RAIR patients had an average age of 57 years (standard deviation [SD] = 13), 56% were male (41% in the control group); the average tumor size was 4 cm (SD = 2.5); tumors were multifocal in 54%, with involved surgical margins in 42%, focal invasion in 79%, and extrathyroidal extension (ETE) in 61%. Sixty-six percent had distant metastases at initial presentation with metastases to the lungs in 85%, bone in 56%, both sites in 43%, brain in 9%, and liver in 4%. There were no statistically significant differences between RAIR and controls in tumor size, focal invasion, ETE, and histology. The RAIR group received a higher cumulative radioactive iodine (RAI) dose and number of therapies compared with the controls (518 mCi vs. 302 mCi, p = 0.002 and 2.2 vs. 1.3 treatments, p = 0.001). Overall, patients >46 years had 4.5 times higher odds ratio (OR) of being RAIR; white race/ethnicity was associated with a reduced OR of RAIR disease (OR 0.33, p = 0.079). Molecular profiling data in the RAIR subgroup indicated that 50% of patients harbored mutations in the RAS/RAF pathway (11/22). Among 19 patients with a more extensive molecular panel, median tumor mutational burden was 5 megabase (range 3–16) and 26% (5/19) exhibited strong PD-L1 positivity.
Conclusion:
Among patients with metastatic differentiated thyroid carcinomas, patients with RAIR have similar histopathological and clinical characteristics as patients with RAI avid cancer. The risk of having RAIR TC is increased at age ≥46 and reduced in Caucasians.
Introduction
Thyroid cancer (TC) is the most common endocrine neoplasm. Based on recent data from the Surveillance, Epidemiology, and End Results (SEER) Program, ∼1.2% of men and women will be diagnosed with TC during their lifetime (1). Incidence rates for new TC cases have been rising on average 3.1% each year over the past 10 years. Death rates have been rising on average 0.7% each year between 2006 and 2015 (1 –4).
At least 94% of the TCs are differentiated thyroid carcinomas (DTCs), which can be either papillary thyroid carcinoma (PTC) or follicular carcinoma. PTC is the most common type of TC, accounting for 87% of the malignant thyroid lesions diagnosed in the United States. Follicular carcinoma accounts for 7% of the malignant thyroid lesions in the United States (3,4).
Most DTC patients are successfully treated with complete or partial thyroidectomy followed selectively by radioiodine ablation or adjuvant radioactive iodine (RAI) therapy, according to their risk stratification for residual, unresectable, or metastatic disease (5). The ability of thyroid tissue to concentrate iodine is the rationale for the use of RAI in the postoperative management of DTC patients (6,7). Approximately 6–20% of patients develop distant metastases, one-third of whom do not concentrate or retain enough RAI to achieve therapeutic benefit (8), thereby contributing to the majority of deaths associated with TC (9). In one long-term outcome study, the survival rate at 10 years from the time of detection of metastases was ∼56% for patients with RAI uptake but only 10% for patients without any significant radioiodine uptake (6).
The 2015 American Thyroid Association (ATA) Management Guidelines for Adult Patients with Thyroid Nodules and Thyroid Cancer classify radioiodine refractory (RAIR) DTC in four basic ways: (i) the malignant/metastatic tissue has never concentrated RAI, (ii) the tumor tissue has lost the ability to concentrate RAI after previous evidence of RAI-avid disease, (iii) RAI is concentrated in some lesions but not in others, and (iv) metastatic disease progresses despite significant concentration of RAI (5). RAIR patients constitute a great challenge in the management of DTC due to the lack of alternative effective and safe treatment choices. Systemic chemotherapy has been used to treat these patients, although these agents have potential toxicities (10).
Recent advances in the understanding of the molecular mechanisms underlying TC have enabled the use of more specific targeted therapies such as multikinase inhibitors (MKIs) (11). However, these therapies may be associated with significant systemic toxicity. In addition, their use has not generally led to an overall survival benefit, although they have significantly improved progression-free survival (12 –15).
There is a growing need to better understand and characterize RAIR TCs to predict their response to therapy earlier in the disease course and potentially to help development of effective therapeutic approaches. Clinical characteristics such as sex, age, race/ethnicity, presence of symptoms, and metastasis, as well as pathological features such as primary tumor size, extent of extrathyroidal extension (ETE), and molecular markers are important features that could be utilized for further characterization and prognostication of these tumors. These parameters may aid the development of potentially more effective and appropriate surveillance, treatment, and follow-up for patients based on their specific risk profile.
The goal of this study is to characterize the clinical, pathological, and molecular profiles of patients with RAIR TCs being followed at our institutions.
Materials and Methods
A retrospective observational study was performed using data from electronic medical records of patients in follow-up at MedStar Washington Hospital Center and MedStar Georgetown University Hospital between 2013 and 2017. Patients were included in the study if they met the following inclusion criteria: (i) Confirmed diagnosis of DTC after total or near total thyroidectomy. (ii) Presence of distant metastases based on post-therapy whole body scan (WBS) or on cross-sectional imaging examinations such as computed tomography (CT), magnetic resonance imaging (MRI) or position emission tomography-computed tomography (PET-CT). (iii) One or more complete follow-up examinations at least 3 years after 131I therapy, including serum thyroglobulin (Tg) levels, WBS, or other imaging techniques (CT, MRI, and PET-CT). Patients younger than 18 years of age were excluded.
Patients were considered RAIR according to the classification from the 2015 ATA Management Guidelines for Adult Patients with Thyroid Nodules and Thyroid Cancer (5). A control cohort was sex matched and age matched, and had metastatic disease that was radioiodine-avid (RAIA). Patients in the control group had either regression or stable disease on follow-up evaluation at least 3 years after initial therapy.
A commercially available next generation sequencing panel (592 genes; Caris Life Sciences, Phoenix, AZ) was employed to perform molecular analysis of a subset of the tumors (n = 20; 19 successfully sequenced by Caris). Testing consisted of DNA- and RNA-based sequencing of most known driver genes (including, among others, BRAF, RAS, RET, and NTRK1/2/3) and genomic landscape signatures (e.g., tumor mutational burden [TMB], microsatellite instability [MSI]). Immunohistochemistry to determine expression of select proteins associated with sensitivity or resistance to immune checkpoint inhibitors, platinum-based therapies, and anthracyclines was also performed, including PD-L1 tumor cell staining (SP142; Spring Biosciences), ERCC1 (8F1; Abcam), and TOP2A (3F6; LEICA), respectively. The panel includes sequencing of the TERT gene but not the promoter regions of the gene (16). Three patients were tested with other platforms that only included a limited set of driver mutations (UPMC Presbyterian).
Data analysis
We identified 76 DTC patients with distant metastases. RAI avidity was determined in all patients. To assess factors associated with RAI refractoriness, bivariate analysis was conducted, including chi-square tests for categorical variables and t-tests for continuous variables. Recursive partitioning and random forests were used to isolate the variables that are considered most important in discriminating between RAIA and RAIR patients. Recursive partitioning iterates through various thresholds in selected variables and selects thresholds based on minimizing mean squared error such that the cohort is classified into terminal nodes with significantly different proportions of avidity. Subsequently, based on the thresholds defined by the recursive partitioning, we estimated the association of the selected thresholds with RAI refractivity using logistic regression. All analyses were done in R 3.4 using the R2wd, doBy, rpart, and rpart.plot packages.
Results
Clinical and pathological characteristics of the RAIR and RAIA patients are summarized in Table 1.
Clinical and Pathological Characteristics of Radioactive Iodine Refractory Versus Radioactive Iodine Avid Groups
RAI, radioactive iodine; RAIA, radioiodine-avid; RAIR, radioiodine refractory; SD, standard deviation.
Of 76 TC patients with distant metastasis, 54 patients were identified as RAIR and 22 as RAIA. Mean age was 57 years (standard deviation [SD] = 13) among RAIR patients and 52 years (SD = 15) among control patients (p = 0.168). Both groups had more males compared with historical data of DTC (55.6% in RAIR group and 40.9% in RAIA group, p = 0.404) where the incidence of TC is approximately three to four times higher among females than among males (17).
Average tumor size was 4.1 cm in the RAIR group and 4.0 cm in the RAIA group (SD = 2.5, p = 0.894). Tumors were multifocal in the thyroid gland in 54.4% of the RAIR cohort and in 55.0% of the controls (p = 0.805). Among 35.1% of the RAIR group, surgical margins were positive compared with 31.8% of the control group (p = 0.805). Focal capsular invasion and ETE were present among 62.1.1% and 46.3% of the RAIR cohort, respectively, compared with 59.1% and 40.9% of the control group (p = 0.805 and 0.836, respectively). Distant metastasis was present at the time of diagnosis among 66% of the RAIR and 82% of the control group (p = 0.172). There was no significant difference in the distribution of distant metastases between the two cohorts (lung: 85.2% vs. 77.3%; bone: 50.0% vs. 36.3%; liver: 3.7% vs. 9.1%; and brain: 9.3% vs. 9.1% among RAIR vs. control, p = 0.340). Other metastatic locations included abdominal lymph nodes, heart, hilar lymph nodes, and pretracheal tumor, which were present in similar frequencies among the RAIR and the control cohort (22% and 23%, respectively).
The RAIR group had received both a significantly higher cumulative RAI dose and number of therapies compared with the control group (518 mCi vs. 302 mCi, p = 0.002 and 2.19 vs. 1.32 treatments, p = 0.001). Among the patients of the RAIR group, 28 patients (51.8%) had no RAI uptake on their first post-therapy scan, 19 patients (35.2%) received RAI doses exceeding 600 mCi, and 7 patients (12.9%) experienced disease progression despite RAI and adequate concentration of RAI in their tumor/metastatic tissue based on post-therapy scans.
Overall, patients >46 years had a 4.5 times higher odds ratio (OR) of having an RAIR cancer ([CI 1.42–14.89], p = 0.01). White race/ethnicity was associated with a reduced OR of RAIR disease (OR 0.33 [CI 0.09–1.15], p = 0.079).
Molecular studies of the primary tumor for 24 patients in the RAIR group were performed (Fig. 1). Two patients had insufficient tissue to perform genotyping in search of the driver mutation(s). These two patients are not included in the figure. Three patients (patients 20–22) were tested with other platforms that only included a limited set of driver mutations (UPMC Presbyterian). Activating alterations (pathogenic mutations or fusion events) in the RAS/RAF pathway occurred in 50% (11/22) of patients tested (BRAFV600E [n = 5], NRAS-Q61R [n = 4], KRAS-G12V [n = 1], and BRAF fusion [n = 1], fusion partner C5orf15). Mutations in other genes included TP53 (21%), and ATM, PIK3CA, RB1, ARID2, and MUTYH (n = 1 for each gene) (Fig. 1). None of the patients tested exhibited MSI (0/17) and median TMB was 6 (range 3–16). Although TMB has not been studied specifically in the context of TC, in general a TMB of >20 mutations/megabase has been associated with better response to immunotherapy (18). Two patients exhibited fusions in non-RAS/RAF genes, including one patient with an NTRK3-ETV6 fusion and one patient with an ROS1-EXR fusion. Strongly positive PD-L1 staining on tumor cells was identified in 5 of 18 (28%) patients (all ≥2+ intensity with staining of 10–95% of cells). ERCC1 and TOP2A expression occurred in 29% and 11% of patients, respectively.
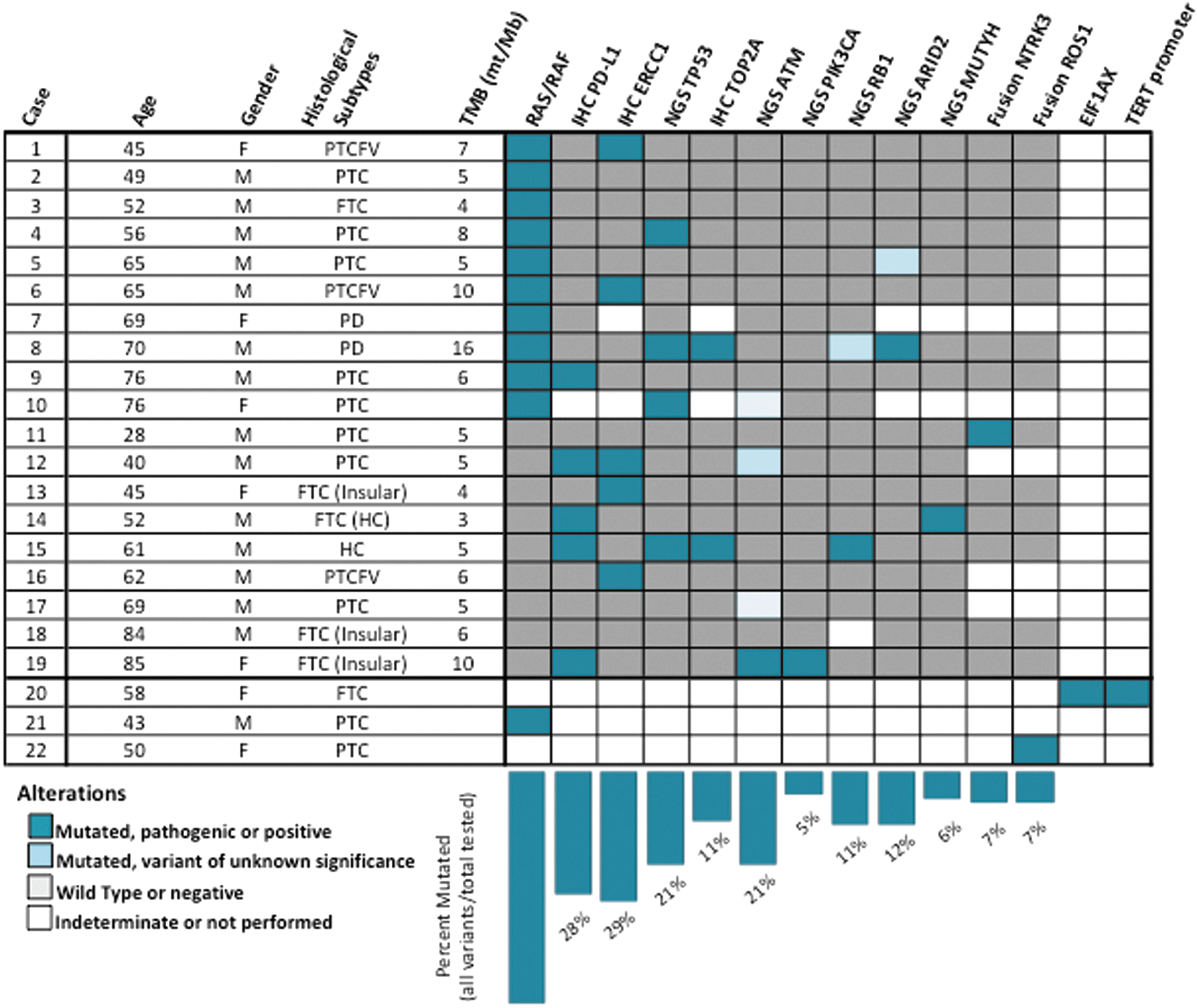
Genomic features observed in RAIR thyroid cancers. Oncoprint plot illustrating co-occurrence of driver events, genes with any pathogenic variant detected in the cohort, and other protein markers. Each RAIR tumor sample with available molecular studies corresponds to one row. Clinicopathological features (age at diagnosis, sex, and histological subtype cancer type) and TMB (mutations/megabase of DNA sequenced) are provided. Fill boxes correlate with gene/protein status: (1) dark blue, pathogenic variant detected or positive expression, (2) light blue, mutated, variant of unknown significance, (3) gray, wild type or low or negative expression, and (4) white, indeterminate result or test was not performed. Bars below columns and percentages below each bar represent total mutation frequency (including variants classified as pathogenic and/or variant of unknown significance). FTC, follicular thyroid cancer; HD, Hurtle cell; TMB, tumor mutational burden; PD, poorly differentiated; PTC, papillary thyroid cancer; PTCFV, papillary thyroid cancer follicular variant; RAIR, radioiodine refractory.
Discussion
The results highlight important characteristics of RAIR DTC, including its aggressive clinical and pathological nature and distinct genomic landscape.
The majority of patients had PTC (85%, classic and follicular variant), followed by follicular TC (21%) in keeping with available literature (3). There was a significantly larger proportion of patients with Hürthle cell and poorly DTC (10–14%) in the cohort, notably at a higher rate than reported in the literature (19). This observation is likely due to the fact that the study cohort consisted of patients with advanced disease and distant metastasis. Hürthle cell and poorly differentiated histologies are associated with aggressive TC with distant metastasis, and are often refractory to RAI therapy (19,20). The male sex preponderance among the RAIR group with 56% of patients being of male sex is noteworthy. Although TC has a strong female sex bias with three- to fourfold higher incidence among females, males generally have more aggressive disease, lower disease-free survival, and higher mortality than females (1). Given that the RAIR cohort represents patients with aggressive disease profiles refractory to standard therapy, the male sex bias observed in our study may be real, although the sample size is small.
No statistically significant differences were found between the RAIR and control group in terms of clinical and pathological characteristics, with the exception of the cumulative dose of RAI administered and the number of RAI treatments. These findings suggest that aggressive TCs, regardless of their response to therapy, may have similar clinical and pathological presentation. Assuming that the data are extrapolatable to a wider group of similar patients, clinical and pathological presentation in advanced DTC are not always predictive of the response to RAI therapy. It is also possible that this study does not have sufficient power to detect differences among the various clinical and pathological characteristics of patients in the RAIR group compared with the RAIA group.
The data indicate that age and race/ethnicity were important predictors of response to therapy. Patients >46 years had 4.5 times higher OR of having RAIR cancer ([CI 1.42–14.89], p = 0.01), and white race/ethnicity was associated with a reduced OR of RAIR disease (OR 0.33 [CI 0.09–1.15], p = 0.079).
The Cancer Genome Atlas (TCGA) provided a comprehensive genomic description of PTC identifying BRAF (59.7%), NRAS (8.5%), and HRAS (3.5%) as the most common driver mutations in PTC. However, these findings were based only on DTC and did not include clinically aggressive tumors (poorly DTC, Hürthle cell, and anaplastic thyroid carcinomas; ATCs) (21). Subsequent studies of poorly DTC and ATC showed a lower prevalence of BRAF mutations (33%) in PDTC and increased frequencies of additional mutations, such as EIF1AX (11%), TP53 (10%), and TERT promoter mutations (40%) (22 –24). In addition, the median mutation burden progressively increases when moving from well differentiated to poorly differentiated and to ATC. This is clinically relevant, given that a higher mutational burden is associated with larger tumor size and a higher frequency of distant metastasis and shorter overall survival (22).
The distinct clinical features in the presently described population may not allow for a direct comparison to available literature but the findings are in line with the emerging literature highlighting the diverse genomic landscape of clinically aggressive TC. The frequency of the BRAFV600 mutation was significantly lower in the cohort of RAIR patients than expected from the literature of DTC with a higher frequency of TP53 mutations, which are typical of poorly DTC (22,24) (Fig. 1). A higher prevalence of PD-L1 positivity was observed among the non-RAS/RAF group than among patients who harbored pathogenic alterations in the RAS/RAF pathway. Although this observation must be confirmed in a larger cohort, it may suggest antitumor immune tendencies in non-RAS/RAF-driven tumors. These results may have implication for relevant therapies, such as the use of immune checkpoint inhibitors.
Although a definition of RAIR has been outlined in the 2015 ATA practice guidelines (see introduction paragraph 4), identifying patients for whom RAI therapy is no longer of benefit or potentially harmful is not a simple task. As per ATA 2015 guidelines, a cumulative dose of 600 mCi has been suggested to indicate refractoriness to RAI therapy. Some patients with high disease burden may require a high cumulative dose of RAI to be effectively treated. Denying these patients further activities of RAI therapy to effectively provide adequate concentrations of radioiodine in affected tissues may be inappropriate. In addition, although some metastatic lesions may progress despite RAI treatment, RAI therapy may still be effective in treating other lesions and provide overall benefit in a given patient. Clinicians should recognize that disease progression within a year after RAI therapy suggests resistance to therapy, and that for many cancers, disease progression and patient survival measured in months can make the difference in selecting therapeutic options. Moreover, untreated patients may have a much faster rate of progression in the year after therapy. Currently, we do not have evidence from a randomized controlled trial to answer these controversial questions, and performing a randomized controlled trial in this setting may be difficult and possibly inappropriate. These are difficult questions that clinicians may struggle with when determining treatment options for advanced TC patients using radiological criteria.
The use of biochemical markers such as Tg is an important additional parameter to radiological approaches to determine treatment options and monitoring of patients with DTC. Although changes in serum Tg levels can provide useful information about the status of the disease, it is important to realize that serum Tg levels in advanced TC do not always accurately estimate the burden of disease or disease progression. In particular, poorly DTCs often produce low levels of Tg, rendering the measurement an unreliable marker of disease persistence or progression in these patients (25). As the cancer progresses, cancer cells may dedifferentiate and lose certain cell characteristics associated with normal thyroid cells. The loss of sodium–iodine symporter expression or function with a resultant inability of cancer cells to concentrate RAI in advanced TC patients is an example of cancer cell dedifferentiation.
Despite the challenges already described in identifying TC patients who are refractory to RAI therapy, it is important to establish RAI refractoriness early in the treatment course. Treating RAIR TC with additional radioiodine has not been shown to improve outcomes and moreover may lead to adverse side effects, including occurrence of secondary cancers, salivary gland dysfunction, pulmonary fibrosis, and bone marrow failure (25 –28). However, recent advances in strategies to redifferentiate TC cells to promote RAI uptake have been promising. Short-term use of specific targeted agents, such as MKIs, has led to improved ability of TC cells to concentrate RAI, a process termed redifferentiation. Although these strategies have not yet led to an overall improvement in patient survival in preliminary studies, disease-free survival among RAIR TC patients has been significantly prolonged (12,15).
Limitations of our study include the retrospective design with an inherent inability to control for bias. In addition, molecular profiling was only available for patients with RAIR TCs that does not allow a direct comparison of the RAIR and RAIA group in terms of their genomic profiles. Given the high financial costs associated with ordering molecular profiling of TC for patients in the clinical setting, only patients who do not respond to standard therapies or patients with negative RAI WBSs are routinely considered for molecular testing. The platform of molecular testing performed by Caris Life Sciences includes sequencing of the TERT gene, but does not include the promoter regions of the TERT gene that have emerged as important sites of mutations associated with clinically aggressive disease with higher prevalence of metastatic disease (29). Furthermore, given the small sample of our cohort, our findings need to be validated, ideally in a larger prospective study, utilizing multivariable analysis to examine the strength of association of different variables and the outcomes of RAIR disease.
This report provides clinical and molecular characterization of TC patients refractory to radioactive iodine therapy. Identification of RAIR patients early in their course may provide opportunities to consider other potential treatment strategies including closer monitoring with periodic cross-sectional radiologic studies, as well the use of MKIs, immunotherapies, or local treatments for metastatic lesions before disease progression may reduce their effectiveness.
Footnotes
Acknowledgments
We thank Drs. Priya Kundra, Jason Wexler, and Geanina Roman-Popoveniuc for their contribution in compiling cases for our study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Catherine Heron and Al Schneider Fellowship in Thyroid Cancer.