
Abstract
Background:
Thyroid autoimmunity has been associated with pregnancy loss. Suggested mechanisms include thyroid function aberrations or an underlying breach of immunotolerance. We hypothesized that thyroid autoimmunity is a marker of the latter in women with recurrent pregnancy loss. This study investigated thyroid peroxidase antibody (TPOAb) status as a predictor of live birth in women with unexplained recurrent pregnancy loss.
Methods:
Cohort study of 825 consecutive women with recurrent pregnancy loss followed at the tertiary referral center for Recurrent Pregnancy Loss, Copenhagen University Hospital (Rigshospitalet), from 2011 to 2017. Recurrent pregnancy loss was defined as ≥3 consecutive losses, and as unexplained by absence of antiphospholipid syndrome, parental chromosome abnormality, or uterus malformation. Upon first visit, all women were screened for thyrotropin (TSH) and TPOAbs (TPOAb positivity: ≥60 kIU/L). Adjusted logistic regression analyses included as covariates the following: maternal age, TSH, previous number of losses, body mass index, smoking, pregnancy achieved by assisted reproductive technology, and thyroxine replacement (T4) treatment.
Results:
We included 825 women with a total of 3246 previous losses, of whom 139 (16.8%) were TPOAb positive. TPOAb positivity was not associated with the previous number of losses (p = 0.41). Women with unexplained recurrent pregnancy loss had a live birth rate in the first pregnancy after referral of 62.8% (285 of 454). TPOAb positivity was found in 78 of 454 (17.2%) women and was associated with a reduced live birth rate (51.3% vs. 65.2%, p = 0.02, adjusted odds ratio [aOR] 0.2 [0.1–0.6] p = 0.001). Treatment with T4 increased live birth rate significantly (aOR 3.7 [1.4–9.8], p = 0.007), and TPOAb-positive women receiving T4 had a live birth rate similar to that of TPOAb-negative women not receiving T4 (p = 0.70). Only 30% of TPOAb-positive women and 39% of women treated with T4 during pregnancy had known thyroid disease at referral.
Conclusion:
In a large cohort of women with unexplained recurrent pregnancy loss, TPOAb positivity was predictive of a reduced live birth rate. However, T4 treatment improved odds of live birth. The study supports screening for TPOAbs as a risk factor in women with unexplained recurrent pregnancy loss. The beneficial effect of T4 treatment in this high-risk group needs confirmation by randomized controlled trials. Close collaboration between fertility experts and endocrinologists is paramount.
Introduction
Pregnancy loss is the most common pregnancy complication occurring in more than 25% of all wanted pregnancies (1,2). A subset of women experiences recurrent pregnancy loss defined as a minimum of three consecutive pregnancy losses or two pregnancy losses in the second trimester or later (3). It is a physically and psychologically challenging condition associated with reduced quality of life, depression, and comorbidities later in life (2,4 –6). An explanation for the condition is only found in ∼40% of investigated cases (including risk factors such as parental chromosomal abnormalities, uterine malformations, or antiphospholipid syndrome), while the remaining cases are categorized as unexplained recurrent pregnancy losses (7).
Thyroid autoimmunity has been associated with reproductive challenges such as infertility, pregnancy loss, and preterm delivery (8,9). In women of reproductive age, thyroid autoimmunity is the most common autoimmune disturbance (8). In previously thyroid-healthy Danish pregnant women (10), we have shown a prevalence of thyroid antibody positivity (thyroid peroxidase and/or thyroglobulin antibodies ≥60 kU/L) of 16.1%, in accordance with findings in the background population (11). In a meta-analysis by Thangaratinam et al. (12), 6–20% of women of reproductive age were thyroid antibody positive, while the prevalence increased to 17–33% in women with recurrent pregnancy loss and 10–31% in subfertile women. In 1990, Stagnaro-Green et al. (13) found a miscarriage rate of 17% in thyroid antibody-positive women compared with 8.4% in thyroid antibody-negative women (p < 0.05). Many studies have since confirmed this association (12,14,15), while others have questioned the association between thyroid antibodies and reproductive failure (16,17). Despite discrepancies and lack of evidence from randomized controlled trials, international guidelines (2,8) recommend screening for thyroid antibodies in women with reproductive failure, including those with recurrent pregnancy loss, and a lenient attitude toward thyroxine replacement (T4) treatment in case of thyroid peroxidase antibody (TPOAb) positivity (i.e., considering treatment at thyrotropin [TSH] concentrations >2.5 mIU/L).
In the present study, we investigated whether screening for TPOAbs at referral could predict live birth rate in a large cohort of women with unexplained recurrent pregnancy loss.
Materials and Methods
Participants
The study was a cohort study of consecutive women followed at the tertiary referral center for Recurrent Pregnancy Loss (which admits patients from all of Denmark) at Copenhagen University Hospital (Rigshospitalet) from January 2011 until May 2017. Recurrent pregnancy loss was defined as three or more consecutive pregnancy losses or two second trimester losses/still births. Upon referral, all women were asked to fill out a questionnaire with information on previous pregnancies and their outcome, previous diseases, height, weight, and smoking status, and the answers were reviewed together with a doctor and a nurse at the first visit. Furthermore, screening for parental chromosome abnormalities (both in the women and their male partners) and a thorough blood workup of the women were performed. Antiphospholipid syndrome was defined as either a positive lupus anticoagulant test or anticardiolipin antibodies >20 kIU/L in both the initial screening samples and by retesting with 12 weeks of interval. Before referral, the women had had a hysterosalpingography, a hydrosonography, or hysteroscopy to examine their uterine anatomy. The couples were asked to abstain from any pregnancy attempt until after completion of the initial screening program. Some women had blood drawn as part of the screening and later realized that they were pregnant with a last menstrual period date before the blood sampling date. Based on evidence regarding the dynamics of both TPOAbs and TSH levels during pregnancy (18,19), we allowed for women to remain included if the blood samples had been drawn no later than gestational week 8. It is highly unlikely that alterations to their thyroid status had occurred at that time point, and unlike the women with a known pregnancy at referral, these women followed the same screening and treatment program as the rest of the cohort.
When achieving a pregnancy after referral, the pregnancy was confirmed by two blood samples measuring human choriogonadotropin concentrations (gestational week 4) with repetition after one week. Weekly ultrasound scans were performed from 6 to 9 weeks of gestation and thereafter every second week until 16 weeks of gestation or pregnancy loss. In case of a normal nuchal translucency scan (11–15 weeks of gestation) and ongoing pregnancy at 16 weeks of gestation, the women were referred to standard obstetric care at their local hospital. Information on the final obstetric outcome was provided by a standardized questionnaire filled out and mailed by the women to the Recurrent Pregnancy Loss Unit. In case of a suspected pregnancy loss, the women contacted the department and were offered an ultrasound scan and/or sequential measurements of human chorionic gonadotropin.
TPOAbs and TSH were measured in each woman as part of a broad screening program upon referral. Measurement of free thyroxine (fT4) concentrations was not recommended in accordance with guidelines (8,20,21) and was not part of the standard evaluation. Nevertheless, the majority of women had an fT4 measurement together with their TPOAb measurement, and thus, fT4 concentrations are described briefly, but not included in further analyses in this study. Women with a TSH <0.4 or >2.5 mIU/L and/or TPOAbs >60 kU/L were referred for evaluation at the Department of Medical Endocrinology, Copenhagen University Hospital (Rigshospitalet). T4 treatment was recommended in case of TPOAb positivity and a TSH >2.5 mIU/L or TPOAb negativity and a TSH >4.0 mIU/L. However, patients were informed of the sparse evidence and depending upon the patient's own wish, she was either monitored without treatment, started on T4 treatment immediately, or was reevaluated upon achieved pregnancy and started on T4 treatment if considered relevant. Thus, most women with positive TPOAbs and/or a high TSH were treated with T4 before achieving their first pregnancy after referral. T4 treatment was titrated to a treatment goal of TSH <2.5 mIU/L. In case of hyperthyroidism, further testing and treatment followed national guidelines (22).
Laboratory analyses
Blood samples were drawn between mid-morning and afternoon, centrifuged within 6 hours, and stored at 2–8°C for a maximum of 72 hours before analyses were performed at the Department of Clinical Biochemistry, Copenhagen University Hospital (Rigshospitalet). TPOAbs were measured by the automated Kryptor immunofluorescense assay (functional assay sensitivity <50 kU/L); on a Kryptor Classic instrument (until February 2017) and later on a Kryptor Classic Gold instrument, BRAHMS (Hennigsdorf, Germany). TPOAb positivity was defined as ≥60 kU/L according to the cutoff used in the clinic. TSH and fT4 were measured by a Roche Modular E170 electrochemiluminescence immunoassay, Roche (Basel, Switzerland), with an interassay coefficient of variance of 7.2%, 3.2%, and 3.3% at concentrations of 0.04, 0.2, and 3.7 mIU/L, respectively, for TSH, and an interassay coefficient of variance of 2.7%, 2.6%, and 3.6% at concentrations of 14.9, 17.5, and 35.9 pmol/L, respectively, for fT4. From June 2015, the Cobas8000 electrochemiluminescence immunoassay (Roche) was used with an intermediary precision of 11.3%, 2.5%, and 2.3% at concentrations of 0.009, 0.2, and 1.9 mIU/L for TSH, respectively, and 8.1%, 2.6%, and 3.6% at concentrations of 1.6,12.9, and 90.9 pmol/L for fT4, respectively.
Statistical analyses
The main outcomes of the present study were TPOAb status in women with recurrent pregnancy loss and live birth rate in the first pregnancy after referral, respectively. Women with no data on TPOAbs, women who were pregnant at referral, and women who did not fulfill the criteria for recurrent pregnancy loss were excluded from all analyses. Furthermore, in analyses regarding the first pregnancy after referral, exclusion criteria were as follows: pregnancies achieved by egg donation; twin pregnancies; ectopic pregnancies; terminated pregnancies; known explanation for prior pregnancy losses (parental chromosome abnormalities, severe uterine anomalies, or antiphospholipid syndrome); three or more previous live births; only two late losses and no early losses; incomplete evaluation of risk factors, or missing information on the pregnancy outcome. Apart from the last two, these were all factors known to affect the risk of another pregnancy loss without relation to the condition of recurrent pregnancy loss itself. Furthermore, two TSH receptor antibody-positive women treated with antithyroid drugs were excluded from pregnancy outcome analyses.
Data analysis included test for trends by chi-square, independent t-tests, or Mann–Whitney-U tests as appropriate. Adjusted logistic regression analyses included as covariates the following: maternal age at referral, TSH (log transformed), number of previous losses, body mass index (BMI), smoking (smoker = 1, nonsmoker = 0), pregnancy achieved by assisted reproductive technology (ART) (ART = 1, spontaneous pregnancy = 0), and T4 treatment (treatment = 1, no treatment = 0). Interactions between TPOAb positivity and T4 treatment, TPOAb positivity and TSH, and TSH and T4 treatment were explored in the model but did not reach significance (p > 0.05) and were therefore omitted from the final model. When adding second-order terms of the continuous covariates, these were not significant and thus not included in the final model.
Missing values were not replaced by dummy variables or missing indicators. A p-value of <0.05 was considered significant. Apart from the predefined primary outcome and logistic regression model, Bonferroni correction was applied to all other analyses (Tables 1 and 4). All statistical analyses were performed in SPSS version 22 (IBM SPSS, NY).
Characteristics of Women with Recurrent Pregnancy Loss With or Without Thyroid Peroxidase Antibodies
Characteristics of 825 women with recurrent pregnancy loss according to TPOAb status. Data provided upon first visit at the recurrent pregnancy loss unit.
BMI, body mass index; GA, gestational age in weeks; IQR, interquartile range; SD, standard deviation; TPOAb, thyroid peroxidase antibodies; TSH, thyrotropin.
Figures were prepared in Microsoft Excel 2016 (Microsoft, WA). Sample size calculation using SAS Enterprise Guide 7.1 (SAS, NC) was performed with an expected skewed weight between TPOAb-positive and TPOAb-negative women (1:4) and an aim of detecting a 20% difference in live birth rate with a power of 0.8 yielding a total sample size of 370.
Ethical approval
Since 2009, all data from women followed at the Recurrent Pregnancy Loss Unit, Copenhagen University Hospital (Rigshospitalet), had been prospectively gathered and stored in a secured database. The database included background information as described above, as well as data on all treatments given and outcomes achieved. The database was approved by the Danish Data Protection Agency (file number 2009-41-3686). Data extraction from the database for the present study was approved by the Danish Data Protection Agency (file number 2017-41-5005). Permission to access medical records for data on endocrine and obstetric follow-up was granted by the Danish Health Authorities (file number 3-3013-1996/1).
Results
Of the 944 women followed at the Recurrent Pregnancy Loss Unit, Copenhagen University Hospital (Rigshospitalet), between 2011 and 2017, 825 women were included with a total of 3915 pregnancies, including 3246 pregnancy losses before referral (Fig. 1 illustrates the inclusion process). The median previous number of losses was 3 (mean 3.9, range: 2–12). The median gestational week at the time of the women's previous losses was 7.5 (range 4–28, interquartile range: 6–9). Women with a previous live birth (secondary recurrent pregnancy loss) constituted 42.5% of the cohort. The median age at referral was 35 (mean: 34.9, range: 22–45 years).
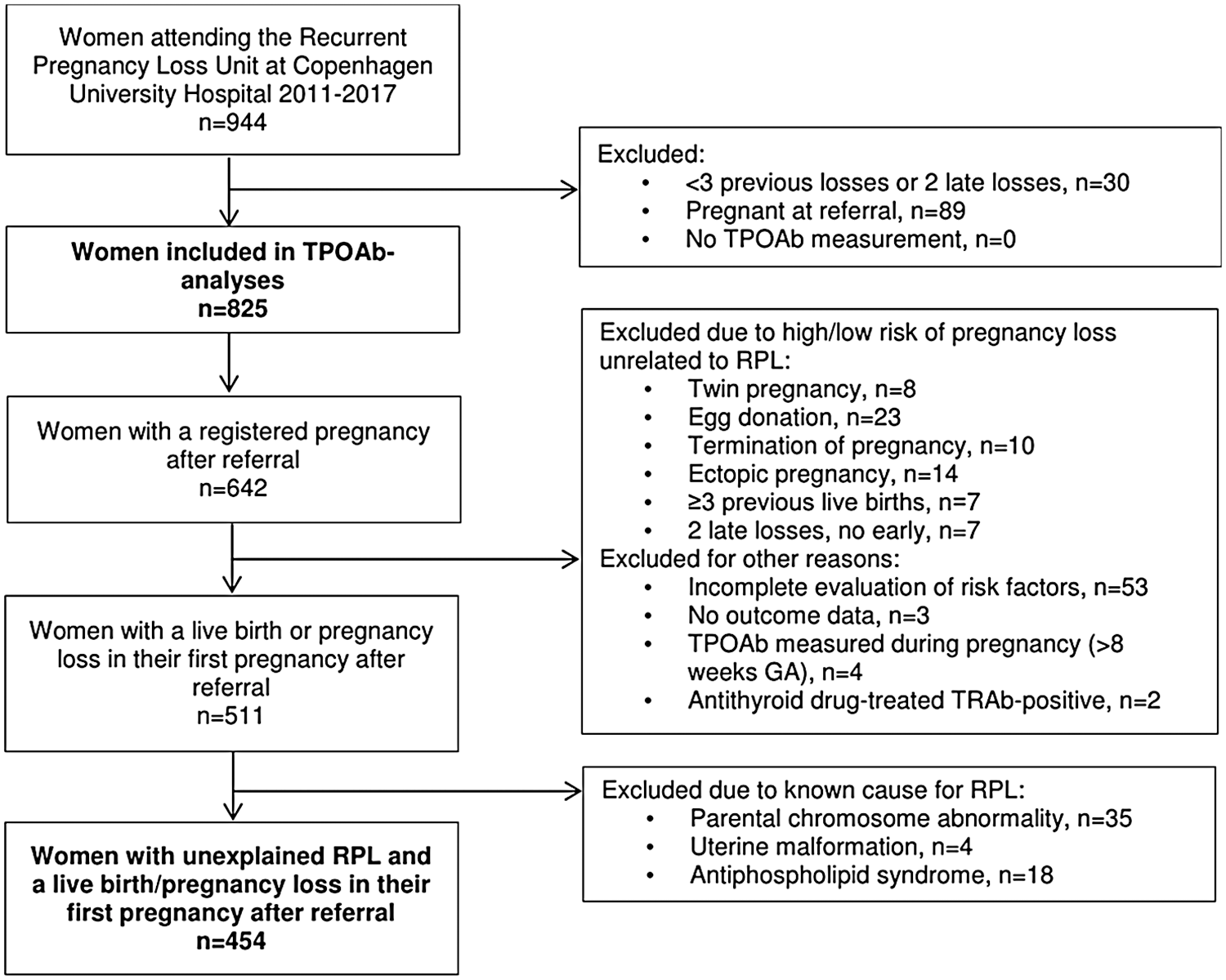
Flowchart of inclusion process. Inclusion process of women with recurrent pregnancy loss followed at the recurrent pregnancy loss unit between January 2011 and May 2017. GA, gestational age; RPL, recurrent pregnancy loss; TPOAbs, thyroid peroxidase antibodies; TRAb-positive, TSH receptor antibody positive; TSH, thyrotropin.
TPOAb status
In total, 139 of the 825 (16.8%) women were TPOAb positive. Among the TPOAb-positive women, the median TPOAb concentration was 550 kIU/L (range 60–19,100 kIU/L, 2.5th percentile 64 kIU/L, 97.5th percentile 11,298 kIU/L). TPOAb positivity was neither associated with number of previous losses (p = 0.41, odds ratio [OR] adjusted for maternal age 0.95 [0.82–1.09], p = 0.44), nor with number of previous pregnancies (p = 0.51, OR adjusted for maternal age 0.96 [0.86–1.06], p = 0.40). As illustrated in Table 1, there were no significant demographic differences between the TPOAb-negative and TPOAb-positive women.
Table 2 illustrates the thyroid status, including treatment at referral according to TPOAb status in the full cohort of 825 women. Previously diagnosed thyroid disease was reported by 63 (7.6%) women, of whom one-third were TPOAb positive. Among the TPOAb-positive women, one-third had previously known thyroid disease and received treatment with T4 at referral. Excluding all women receiving T4 treatment, TPOAb-positive women had significantly higher TSH levels (p < 0.001) and lower fT4 levels (p = 0.04) compared with TPOAb-negative women.
Thyroid Status in Women with Recurrent Pregnancy Loss With or Without Thyroid Peroxidase Antibodies
Thyroid status at screening in 825 women with recurrent pregnancy loss according to TPOAb status.
TSH measurements available from 819 women.
p-Value for independent samples t-test of log-transformed values.
fT4 measurements available from 724 (87.8%) women (606 TPOAb negative and 118 TPOAb positive).
fT4, free thyroxine; T4 treatment, thyroxine replacement treatment.
First pregnancy after referral
Among the included 825 women, 642 (77.8%) had a first pregnancy after referral, of whom 454 (70.7%) fulfilled the inclusion criteria for outcome analyses (Fig. 1). Four women were excluded due to uterine factors (three with large intrauterine septa and one with cervical insufficiency) and 35 women due to chromosome abnormalities (i.e., significant parental balanced translocations or Turner mosaicism). Between those who had a first pregnancy after referral and those who had not, there was no significant difference in the proportion of TPOAb-positive women (16.7% vs. 17.5%, p = 0.79), age at referral (p = 0.14), or number of previous losses (p = 0.96).
Thyroid status
A total of 78 of 454 (17.2%) women were TPOAb positive at screening. Table 3 depicts details on the thyroid status in the 444 included women who achieved pregnancy after referral and had information on both TPOAb positivity and T4 treatment during pregnancy. Nine of the TPOAb-positive women participated in an ongoing randomized placebo-controlled trial on T4 treatment of euthyroid women [T4-LIFE (8,23)], and thus, information was missing on T4 treatment during their pregnancy. Furthermore, one TPOAb-negative woman was excluded in analyses of T4 treatment due to intake of liothyronine after (reportedly) having had a low triiodothyronine measured at a private endocrine clinic. Of the remaining TPOAb-positive women, 52 (75.4%) received T4 treatment during pregnancy. Fourteen TPOAb-negative women received T4 treatment. Four of the women were treated with Euthyrox® (Merck), one woman with Levaxin® (Takeda) (75 μg/day), and the rest with Eltroxin® (Aspen). Most of the women (53 of 66) were started on T4 treatment before pregnancy and 78% of these achieved a TSH below 2.5 mIU/L (data from 51) before pregnancy. Reasons for initiating T4 treatment later during pregnancy (n = 13) were as follows: watchfull waiting because of TSH within normal range (n = 4), evaluation by endocrinologist after date of last menstrual period (n = 5), previously treated and planned to initiate treatment at positive pregnancy test (n = 1), noncompliant (n = 1), planned to be included in randomized controlled trial but had TSH increase during early pregnancy (n = 1), and treatment not indicated prepregnancy but retested during pregnancy due to symptoms (n = 1).
Thyroid Status and Thyroxine Replacement Treatment in the First Pregnancy After Referral in Women with Unexplained Recurrent Pregnancy Loss
Thyroid status and treatment characteristics in 444 women with unexplained recurrent pregnancy loss according to TPOAb positivity and treatment with T4 during their first pregnancy after referral to the recurrent pregnancy loss unit. Women taking part in randomized controlled trials on T4 treatment (n = 9) and one woman taking T3 were excluded from analyses.
Not retested during pregnancy due to normal evaluation at screening.
Planned for inclusion in RCT, but became pregnant before inclusion.
Data on TSH and T4 dose during pregnancy missing for women followed by endocrinologists at their local hospitals during pregnancy.
T4+, treatment with thyroxine replacement treatment during pregnancy; T4−, no treatment with thyroxine replacement treatment during pregnancy; TPOAb-positive, thyroid peroxidase antibody positive; TPOAb-negative, thyroid peroxidase antibody negative.
Predictors of live birth
The overall live birth rate was 62.8% (285 of 454 pregnancies) in the first pregnancy after referral. Table 4 depicts differences between women who achieved a live birth and those who suffered another pregnancy loss. The chance of the pregnancy resulting in a live birth was significantly reduced in TPOAb-positive women compared with TPOAb-negative women (51.3% vs. 65.2%, p = 0.02, adjusted odds ratio [aOR] 0.2 [0.1–0.6] p = 0.001). As such, testing for TPOAbs at referral had a sensitivity of 22.5%, a specificity of 86%, a positive predictive value of 48.7%, and a negative predictive value of 67.9%.
Characteristics of Women According to Outcome of Their First Pregnancy After Referral
Characteristics of 454 women with unexplained recurrent pregnancy loss and either a live birth or a pregnancy loss in their first pregnancy after referral to the recurrent pregnancy loss unit. Other treatments than T4 included the following. Intravenous immunoglobulin (indications: three or more losses after IVF or ICSI, five or more losses after a birth [secondary recurrent pregnancy loss], or known autoimmune disease not including thyroid autoimmunity [systemic lupus erythematosus, rheumatoid arthritis, Crohn's disease, colitis ulcerosa, myasthenia gravis]), prednisolone in adjuvance to immunoglobulin in pregnancies achieved by ART, and plaquenil in case of a minimum of four consecutive losses.
p-Value for difference of mean of log-transformed TSH-values.
ART, assisted reproductive technology; TPOAb, thyroid peroxidase antibodies.
There was no difference in TSH concentrations at screening between women achieving a live birth versus a pregnancy loss (p = 0.69, aOR 1.2 [0.6–2.5], p = 0.63). Neither were TSH concentrations at screening associated with live birth rate in subanalyses of TPOAb-positive and TPOAb-negative women, nor in subanalyses of women receiving or not receiving T4 during pregnancy, respectively.
Live birth rate according to TPOAb status and T4 treatment is illustrated in Figure 2. In the logistic regression model, T4 treatment was a significant predictor of live birth (aOR 3.7 [1.4–9.8], p = 0.007). Subanalyses of TPOAb-positive women showed a significantly improved live birth rate in those who received T4 treatment (61.5% compared with 29.4% in nontreated women (p = 0.02, aOR 5.5 [1.4–21.2] p = 0.01).
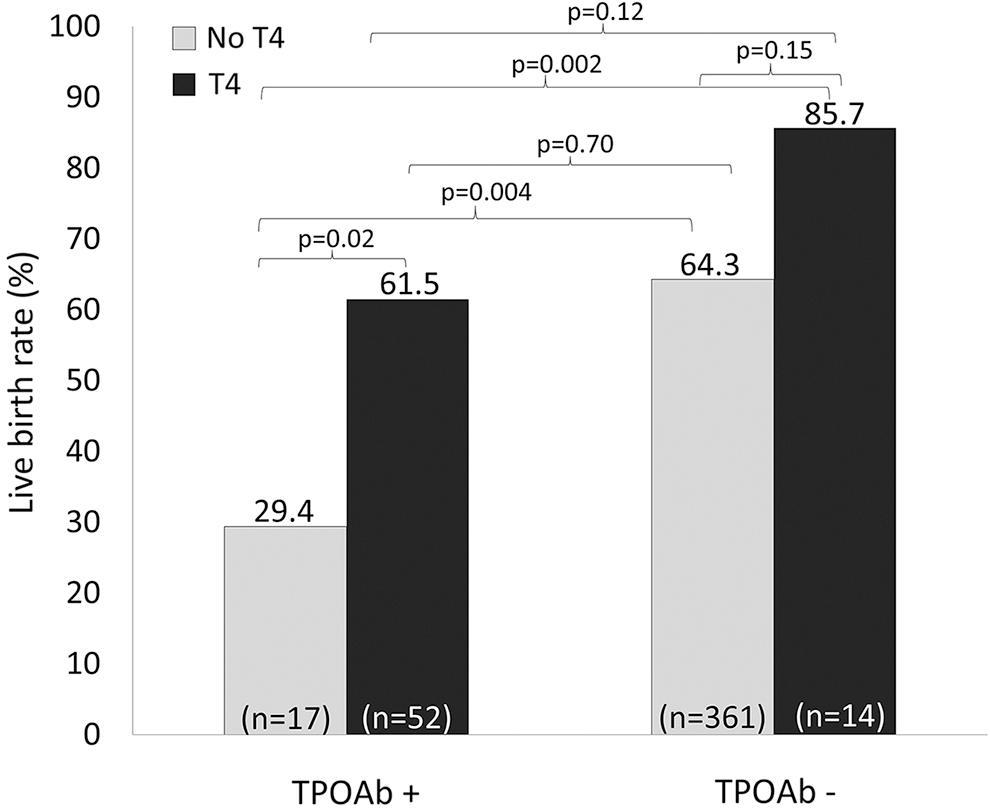
Live birth rate according to thyroid peroxidase antibody status and treatment with T4. Live birth rate according to TPOAb positivity and T4 treatment in the first pregnancy obtained after referral in 444 women with unexplained recurrent pregnancy loss and available information on T4 treatment. Adjusted logistic regression (covariates: TPOAb positivity, maternal age at referral, TSH, number of previous losses, body mass index, smoking, pregnancy achieved by assisted reproductive technology, and T4 treatment) showed a reduced live birth rate in TPOAb-positive women (aOR 0.2 [0.1–0.6], p = 0.001) and an improved live birth rate with T4 treatment (aOR 3.7 [1.4–9.8], p = 0.007). p-Values in figure refer to a priori analyses by chi-square testing. Women taking part in randomized controlled trials on T4 treatment (n = 9) and one woman taking T3 were excluded from analyses. Gray boxes: no T4 treatment. Black boxes: T4 treatment. aOR, adjusted odds ratio; T4, thyroxine replacement; TPOAb−, thyroid peroxidase antibody negative; TPOAb+, thyroid peroxidase antibody positive.
Only two of the TPOAb-positive women smoked during their pregnancy. Excluding all smokers (n = 31) from the analyses did not alter the significance of TPOAb positivity on live birth rate (52.6% vs. 66.0%, p = 0.028, aOR 0.23 [0.1–0.6], p = 0.001).
No other covariates reached statistical significance in the model (maternal age at referral aOR 1.0 [1.0–1.0], p = 0.78; number of previous losses aOR 0.9 [0.8–1.1], p = 0.20; smoking aOR 0.7 [0.3–1.5], p = 0.35; BMI aOR 0.96 [0.9–1.0], p = 0.06; or pregnancy achieved by ART aOR 0.9 [0.5–1.5], p = 0.65).
Live birth in both explained and unexplained pregnancy loss
Among women who became pregnant after referral, inclusion of both the women with explained and unexplained recurrent pregnancy loss (n = 511) gave similar results. Thus, live birth rate in the 88 (17.2%) TPOAb-positive women was 50.0% compared with 64.1% in the 423 TPOAb-negative women (p = 0.014). In the adjusted model, the odds ratio for live birth with TPOAb positivity was 0.3 (0.1–0.7), p = 0.003, and with T4 treatment 2.4 (1.0–5.4), p = 0.04.
Discussion
In this large cohort study of women with unexplained recurrent pregnancy loss, TPOAb positivity was associated with a reduced live birth rate in the first pregnancy after referral. However, with T4 treatment, the live birth rate was comparable with that of TPOAb-negative women. Only 30% of TPOAb-positive women had known thyroid disease at time of referral, and 61% of those receiving T4 treatment during pregnancy had no known thyroid disease at referral.
A strength of the present study is the opportunity to evaluate the value of screening for TPOAbs at referral as a predictor of outcome in a subsequent pregnancy. There was no significant difference in the chance of getting pregnant, but TPOAb positivity reduced the chance of pregnancy resulting in a live birth. This was even true when including women with known risk factors for recurrent pregnancy loss and not only those with unexplained losses. In the hitherto largest study by Rushworth et al. (24), 105 women with recurrent pregnancy loss and no known thyroid disease had a prospective live birth rate, which was similar between the 24 euthyroid TPOAb- and/or thyroglobulin-antibody-positive women and women without these antibodies (58% vs. 58%) (24). Thus, the predictive value of thyroid antibodies may be lower in women with unaffected thyroid function and no need for treatment, or it may differ between TPOAb-positive and thyroglobulin-antibody-positive women. In our study, the specificity of TPOAb testing was quite high, but sensitivity and positive predictive value were low, which serves as a reminder of the many competing (unknown) risk factors in recurrent pregnancy loss. We were able to test for chromosome abnormalities as the only well-established male factor (25), but the role of the male partner is a quickly evolving field of investigation, which will likely provide much needed information in the future (26,27).
We found a reduction in the odds ratio for live birth of 10% per previous loss (aOR 0.9 [0.8–1.1], p = 0.20) in accordance with other studies (28). However, this was not statistically significant, likely due to a lack of power, or because studies were not comparable in terms of spectrum of prior pregnancy losses or treatment strategy. A longer follow-up period with more included pregnancies could have improved this, although there was no significant difference in the number of previous losses among the women achieving and not achieving a pregnancy.
Although the present study confirms an association between TPOAbs and pregnancy loss, no causality can be inferred from the results and the mechanisms remain unclear. One hypothesis is that thyroid antibody presence is an epiphenomenon of an underlying (auto)immune imbalance causing reduced tolerance toward the fetus (29,30). This is in line with findings that women with unexplained recurrent pregnancy loss often display an imbalance between effector T cells and regulatory T cells and have HLA types associated with poorer pregnancy outcomes (31 –33). Thus, TPOAb-positive women with recurrent pregnancy loss have been suggested to have a reduced ability to regulate the humoral response during pregnancy (34) and are more often positive for other autoantibodies (i.e., lupus anticoagulant, antinuclear antibodies, double-stranded DNA antibodies, and antimitochondrial antibodies) (35,36) than unselected pregnant women (37). Finally, in women with known antiphospholipid antibodies and recurrent pregnancy loss, De Carolis et al. (38) showed that the additional presence of thyroid autoantibodies increased the risk of pregnancy loss, however, with a comparable live birth rate between women with multiple types of autoantibodies and those positive for thyroid antibodies alone. Thus, while the present study included only TPOAbs (and excluded women with antiphospholipid syndrome), these antibodies likely serve as a relevant marker of a tolerance breach if recurrent pregnancy loss can be considered an immunological (over)reaction (39). Further studies of autoimmunity [including the role of thyroglobulin antibodies (8,40)] in women with recurrent pregnancy loss are warranted.
A second hypothesis regarding the association between thyroid autoimmunity and pregnancy loss is that thyroid antibody-positive women have subtle degrees of thyroid dysfunction affecting their reproductive ability. Thyroid hormones are highly involved in reproduction (41,42) and a physiological increase in maternal thyroid hormone production is required during pregnancy (43), an increase that women with thyroid autoantibodies often fail to achieve (10,18). However, van Dijk et al. (44) recently reported that subclinical hypothyroidism compared with euthyroidism in women with unexplained recurrent pregnancy loss did not reduce the chance of live birth (45% vs. 52%, OR 0.69 [95% confidence interval: 0.28–1.71]) (no thyroid antibodies were measured). In the present study, TSH concentrations at screening were not predictive of the chance of subsequent live birth.
Finally, it should be noted that thyroid hormones impact the immune system per se (45 –48) and, therefore, a combination of loss of tolerance and thyroid impairment could be involved in recurrent pregnancy loss. Thus, we speculate that the potential benefits of T4 treatment could also be explained by a regulation of the immune system by sustained euthyroidism.
T4 treatment before and during pregnancy was associated with a significantly increased live birth rate in adjusted logistic regression analysis, and in subanalyses of TPOAb-positive women, live birth rate was doubled compared with those not receiving T4. Notably, results on T4 treatment may be biased by “treatment by indication” with those with the most affected thyroid function receiving T4 treatment. Although a strength of our study was the potential of correcting any thyroid aberrations by T4 treatment before a subsequent pregnancy, this was also a limitation as we did not have longitudinal thyroid measurements during pregnancy of the women with a healthy thyroid function.
Several randomized controlled trials of T4 treatment in TPOAb-positive women with pregnancy loss as outcome have been conducted in both healthy pregnant women and women undergoing ART (49 –53). The results have been ambiguous; perhaps due to differences in timing of treatment initiation and adjustment during pregnancy, as well as to low numbers of pregnancy losses in some groups (54,55). However, recurrent pregnancy loss should be considered a distinct disease entity. To our knowledge, only a few smaller studies have previously described the effect of T4 treatment in thyroid antibody-positive women with recurrent pregnancy loss and conclusions have been mixed (56 –58).
Recently, the large TABLET trial (59) showed no difference in live birth rate in 952 euthyroid TPOAb-positive women with one or more previous pregnancy losses or being treated for infertility who were randomized to receive either 50 μg/day T4 or placebo before and during pregnancy. A subgroup of women had three or more pregnancy losses, but no information was provided on the losses being consecutive or whether known risk factors for recurrent pregnancy loss existed. Although the results of the TABLET trial are very comforting with regard to the unnecessary treatment of otherwise thyroid-healthy women, they are not easily applicable to the highly selected high-risk women included in our study.
Given the low costs, minimal side effects, and noninvasiveness of T4 treatment, our study does favor such treatment in TPOAb-positive women with TSH levels >2.5 mIU/L and with unexplained recurrent pregnancy loss upon detailed evaluation of risk factors. The important contribution from the TABLET study (59) has provided evidence that treatment is generally not needed in euthyroid TPOAb-positive women with previous pregnancy losses. More studies on high-risk women with recurrent pregnancy losses are therefore needed. Meanwhile, we believe it is reasonable to screen all women with recurrent pregnancy loss for TPOAbs and TSH concentrations given the high prevalence of thyroid abnormalities in women of reproductive age, the importance of thyroid hormones for fetal development, and the psychological factor of identifying potential risk factors in every woman. However, the challenging interpretation of the results and decision on T4 treatment call for a close collaboration between fertility doctors and endocrinologists.
In conclusion, this large cohort study of women with unexplained recurrent pregnancy loss demonstrates a reduced live birth rate in the first pregnancy after referral in TPOAb-positive women. The TPOAb-positive women who received T4 had a live birth rate similar to that of the TPOAb-negative women. Although the findings need confirmation from placebo-controlled trials, the present results speak in favor of screening for thyroid autoantibodies in this patient group. A close collaboration between fertility doctors and endocrinologists is pivotal in insuring the best possible management of these women, both before and during pregnancy.
Footnotes
Acknowledgments
We owe great thanks to the persistently hard work and kind care-taking toward the many women with recurrent pregnancy loss provided by nurses Karen Kircheiner and Louise Lunøe. We greatly appreciate the continuous support in the planning and interpretation of statistical analyses provided by the Biostatistical Department at the Copenhagen University, in particular, associate professor Julie Lyng Forman.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The research of S Bliddal is kindly supported by the Copenhagen University Hospital (Rigshospitalet), Musikforlæggerne Agnes and Knut Mørk's Foundation, Desiree and Niels Yde's Foundation, the Danish Medical Association's Research Foundation, the A.P. Møller Foundation for the Advancement of Medical Science, and the Danish Thyroid Patient Association. U Feldt-Rasmussen is supported by a grant from the Novo Nordisk Foundation. H Svarre Nielsen and A Marie Kolte are supported by grants from the Copenhagen University Hospital (Rigshospitalet). The funding sources had no influence on the study design and conduct hereof, or on the preparation of the present article.