
Abstract
Background:
Expression of the programmed death-ligand 1 (PD-L1) in medullary thyroid carcinoma (MTC) has been rarely reported. In this study, we evaluated PD-L1 positivity in MTC and analyzed its correlation with clinicopathological characteristics, structural recurrence (SR), and biochemical recurrence/persistent disease (BcR/BcPD). We also evaluated the prevalence of PD-L1 expression in patients developing distant or unresectable locoregional recurrence.
Methods:
In total, 201 consecutive MTC patients who underwent initial surgery in our institution from January 2006 to December 2015 were included. PD-L1 expression was evaluated by immunohistochemical staining and was considered positive in case of a combined positive score ≥1. The association of PD-L1 positivity with clinicopathological characteristics, structural recurrence-free survival (SRFS), and BcR/BcPD was retrospectively investigated.
Results:
The median follow-up length of the entire cohort was 73 months. We observed positive PD-L1 staining in 29 (14.4%) patients who were more likely to have a larger tumor size (p = 0.002), lymph node metastases (p = 0.036), and advanced TNM staging (p = 0.019). The five-year SRFS of the PD-L1-negative and PD-L1-positive groups was 85.4% and 57.9% (p = 0.001). Multivariate Cox analysis showed that PD-L1 positivity was independently associated with SR (hazard ratio = 2.19 [95% confidence interval (CI) 1.01–4.77], p = 0.047). Furthermore, multivariate logistic analysis showed that PD-L1 positivity was significantly associated with BcR/BcPD (odds ratio = 3.16 [CI 1.16–8.66], p = 0.025). During the study period, 20 patients developed distant or unresectable locoregional recurrence, among whom 8 (40%) were PD-L1 positive, which was much higher than in the entire MTC population.
Conclusions:
Using a large cohort of MTC patients, we demonstrate that PD-L1 positivity is associated with aggressive clinicopathological features and is independently predictive of SR and BcR/BcPD. Furthermore, a higher rate of PD-L1 expression in patients with incurable recurrence has been observed. Therefore, immune checkpoint inhibitors targeting the programmed cell death-1 (PD-1)/PD-L1 pathway may be a potential therapeutic strategy to treat advanced MTC.
Introduction
Medullary thyroid carcinoma (MTC), characterized by Hazard et al. in 1959 (1), is a neuroendocrine malignancy deriving from the calcitonin-producing parafollicular cells (C cells). MTC represents 3–5% of all thyroid neoplasms but causes ∼13% of thyroid cancer-related mortality (2,3). For localized disease, thyroidectomy can be a curative strategy with an excellent five-year disease-specific survival of 98% (4). However, MTC remains largely incurable and lethal when distant metastasis or an unresectable recurrence occurs. In the metastatic setting, external beam radiation therapy and chemotherapy are mostly used as palliative means (5,6). At present, the U.S. Food and Drug Administration (FDA) has approved vandetanib and cabozantinib for the treatment of advanced or progressive MTC. Although the two kinds of tyrosine kinase inhibitors have achieved significant increase in progression-free survival, an overall survival benefit has not been demonstrated as of yet (7 –9). Effective additional or alternative treatment is still urgently needed.
Programmed cell death-1 (PD-1) and its ligand (PD-L1) are members of negative costimulatory signal molecules. It is generally acknowledged that the interaction between PD-1 and PD-L1 can protect tumor cells from cytotoxic T cell attack and induce the exhaustion of effector T cells. In recent years, anti-PD-1/PD-L1 therapy has shown promising clinical prospects in the treatment of advanced-stage malignancies. PD-L1 expression in the tumor microenvironment (TME) is reported to be predictive of patient outcomes and immunotherapy responses (10 –14), and thus, a reproducible scoring method called combined positive score (CPS) was developed (15). CPS represents PD-L1 expression on both tumor cells and immune cells in the TME and is presently used to identify and enroll potential immunotherapy responders into clinical trials for patients with various solid tumors (16 –20). Bongiovanni et al. and Bi et al. have separately explored PD-L1 expression in MTC using 16 and 89 patients (21,22). However, the two studies did not further investigate the impact of PD-L1 expression on structural recurrence (SR) or biochemical status, which is probably due to insufficient cases. To our knowledge, for patients with MTC, it remains unknown whether PD-L1 is predictive of prognosis.
In the present study, using a large cohort of patients with this relatively rare malignancy, we evaluated the prevalence of PD-L1 expression based on the CPS, and investigated its correlation with clinicopathological factors, SR, and biochemical recurrence/persistent disease (BcR/BcPD). Furthermore, we also evaluated the proportion of PD-L1-positive disease among patients with incurable recurrences who need novel treatments, including immunotherapy targeting the PD-1/PD-L1 axis.
Materials and Methods
Patients and samples
Patients who met the following criteria were included in the study: (i) confirmed histopathological diagnosis of MTC; (ii) underwent initial surgery in our institution (Fudan University Shanghai Cancer Center, FUSCC); (iii) no previous malignancies; (iv) available clinicopathological data and medical history; (v) available formalin-fixed, paraffin-embedded tumor tissues with or without the corresponding para- or peritumor tissues. The paratumor tissue refers to the thyroid tissue obtained more than 1 cm away from the tumor foci (either in the ipsilateral or the contralateral lobe), and it is microscopically confirmed to be free of cancer involvement. The peritumor tissue refers to the thyroid tissue around the tumor foci (generally less than 0.5 cm away), and has been microscopically confirmed to consist of nontumor thyroid tissue adjacent to the tumor margin under low-power field (100 × ). In addition, we excluded patients with postoperative persistent disease (distant metastasis at diagnosis, gross residual disease, and microscopic positive margins) because the time to SR could not be calculated. Before the study began, all available hematoxylin/eosin-stained and immunohistochemical slides were re-examined by two experienced pathologists to confirm the diagnosis of MTC according to the present World Health Organization criteria.
In total, 201 MTC patients surgically treated at our institution in a 10-year period (from January 2006 to December 2015) were consecutively identified. This study was approved by the Institutional Review Board of FUSCC and informed consent was provided by each patient. Demographics, tumor characteristics, treatment details, pathological findings, and imaging information of the patients were obtained.
Initial treatment, calcitonin measurement, and follow-up
The patients initially underwent total thyroidectomy or hemithyroidectomy or completion thyroidectomy if a lobectomy/nodule excision had been performed to treat a benign disease. Central compartment (level VI) neck dissection was routinely performed for suspicious thyroid malignancies in our institution. Modified lateral neck and/or upper mediastinal lymphadenectomy were performed if there were biopsy-proven or preoperative suspicious lateral neck and/or level VII metastases.
In our institution, stimulated serum calcitonin was not routinely measured. Basal serum calcitonin (Ctn) was assessed by different methods over time. From January 1993 to September 2011, basal serum Ctn levels were measured using a direct radioimmunoassay (RIA) kit (China Institute of Atomic Energy, Beijing, China). The reference range of this kit was 0–300 pg/mL according to the manufacturer. As illustrated in other previous studies, direct RIA methods generally have a high functional detection limit and a broad reference range (23,24). From October 2011 to January 2017, basal serum Ctn levels were measured using a chemiluminescence immunoassay (CLIA) system (SNIBE Co., Ltd, Shenzhen, China) with a reference range of 0–50 pg/mL. In February 2017, the CLIA system was replaced by the Elecsys® Calcitonin test system (Roche Diagnostics, Shanghai, China), which is an electrochemiluminescence immunoassay (ECLIA). According to the manufacturer, the reference range is 0–9.52 pg/mL for males and 0–6.40 pg/mL for females (25).
Patients were followed up by telephone contact and review of inpatient or outpatient medical records in our institution. Follow-up length was calculated from the date of initial surgery to the date of death or the last contact. SR was confirmed by fine-needle aspiration biopsy, repeated neck surgery, or imaging scans after careful review of preoperative imaging to exclude residual disease. One of the endpoints of this study was structural recurrence-free survival (SRFS), the duration of which was calculated from the date of initial surgery to the first confirmed SR based on histopathological or radiological findings. The other endpoint was BcR/BcPD. The ATA guidelines and relevant references therein define biochemical cure as a postoperative Ctn level within the reference range (5,24,26). Therefore, in this study, BcR/BcPD was defined as relapsed/persistent increased postoperative basal serum Ctn above the corresponding reference range during the study period.
Immunohistochemistry staining and evaluation
Both the whole sections of surgical specimens and previously constructed tissue microarrays (TMAs) were used in this study. Regarding tumor tissues, for patients with large tumors (generally larger than 2 cm), immunohistochemistry (IHC) staining and evaluation of PD-L1 positivity were based on whole sections; TMAs were stained and used as surrogates to evaluate PD-L1 expression if the patient's primary tumor was small. Regarding the para-/peritumor tissues, only TMAs were evaluated. Dako PD-L1 IHC 22C3 pharmDx assay (Agilent, Carpinteria, CA), as the first FDA-approved PD-L1 IHC companion diagnostic, was used for IHC staining on a Dako Autostainer Link 48 system (Agilent) with an EnVision FLEX visualization system according to the manufacturer's instructions.
PD-L1 expression was determined by CPS, defined as the ratio of PD-L1-stained cells (tumor cells, lymphocytes, and macrophages) out of the total number of viable tumor cells, multiplied by 100. A tumor cell was counted as “stained” if complete or partial membrane PD-L1 staining was observed, while an immune cell was considered “stained” if it featured any PD-L1 staining (membrane/cytoplasm), as described by Kulangara et al. who developed the CPS algorithm (15,27). The specimen was regarded as PD-L1-positive if the CPS was ≥1 (17,27,28). Furthermore, patients with positive PD-L1 staining were separated into low (1 ≤ CPS <5), moderate (5 ≤ CPS <20), and high (CPS ≥20) expression groups. Two experienced pathologists blinded to the clinicopathological and follow-up data independently evaluated the results of IHC staining.
Statistical analysis
Continuous variables were compared by Student's t-test and categorical variables were compared by chi-square test or Fisher's exact test, as appropriate. Kaplan–Meier analysis and log-rank test were used to generate and compare the survival curves. Multivariate Cox proportional hazard regression models were used to investigate the impact of PD-L1 expression on SR after adjusting for potential confounders, for which the results were presented as hazard ratios (HR) with 95% confidence intervals (CI). In multivariate Cox analyses, the postoperative basal serum Ctn level was also incorporated as a confounding predictive factor for SR, and for patients without SR, the level included in Cox analyses referred to the Ctn level at the last follow-up; for patients with SR, the level referred to the latest measurement before the first confirmed SR. Multivariate logistic analyses were used to investigate the correlation between PD-L1 expression and BcR/BcPD, for which the results were presented as odds ratios (OR) with CI.
To make the results more convincing, we performed two types of multivariate analyses (MVA): (i) the first type of MVA incorporated tumor size, extrathyroidal extension (ETE), lymph node metastasis (LNM), and other factors. The TNM staging was not included in this type because tumor size, ETE, and LNM constituting the T and N classification already provided similar prognostic information; repeated information adjusted twice in the same analysis would cause statistical overadjustment; and (ii) the second type of MVA incorporated the TNM staging and other factors, while tumor size, ETE, and LNM were not included.
The Kaplan–Meier survival plots were generated by GraphPad Prism 7.0 (GraphPad Software, San Diego, CA). Student's t-test, chi-square test, log-rank test, and multivariate Cox and logistic analyses were performed using SPSS Statistics v23.0 (SPSS, Inc., Chicago, IL). A two-sided p-value <0.05 was considered statistically significant.
Results
Immunohistochemical findings
PD-L1 expression was evaluated by IHC staining. Of the 201 patients included, 184 (91.5%) had available para- or peritumor tissues, in which we did not observe any positive PD-L1 staining except for lymphocytes in patients with Hashimoto's thyroiditis. Representative images are shown in Figure 1A and B. For tumor tissues, positive PD-L1 expression was observed in 29 patients (14.4%), among whom 7, 15, and 7 patients had low, moderate, and high expressions, respectively. The remaining 172 patients (85.6%) were determined as having PD-L1-negative tumors. Representative images showing negative, low, moderate, and high PD-L1 expression are illustrated in Figure 1C–F, respectively.

Representative low (100 × ) and high (400 × ) magnification immunohistochemistry images showing (
Patient characteristics and their correlation with PD-L1 expression
Patient characteristics are listed in Table 1. For the overall cohort, the median follow-up length was 73 months (range: 2–153 months). The median age at diagnosis was 49 (range: 12–80) years and more than half (n = 106, 52.7%) were male. In the pathology reports, 137 patients (68.2%) had LNM, among whom 103 metastasized to lateral neck and/or upper mediastinum. More than half of the patients (n = 104, 51.7%) had stage IV disease according to the eighth TNM/AJCC staging system. None of the 201 patients had distant metastases at diagnosis. During the follow-up period, 44 patients (21.9%) had SR, 99 patients (49.3%) had BcR/BcPD, and 12 patients (6.0%) died of MTC.
Patient Clinicopathological Characteristics and Events During the Study Period (n = 201)
AJCC, American Joint Committee on Cancer; BcR/BcPD, biochemical recurrence/persistent disease; HT, Hashimoto's thyroiditis; MTC, medullary thyroid carcinoma.
PD-L1 positivity was associated with larger tumor size (p = 0.002), LNM (p = 0.036), TNM staging (p = 0.019), SR (p = 0.006), and BcR/BcPD (p = 0.002). Other clinicopathological factors did not present significant correlations with PD-L1 positivity (Table 1).
PD-L1 expression and SRFS of MTC patients
The Kaplan–Meier survival analysis demonstrated that the five-year SRFS rate of the overall cohort was 81.6% (Fig. 2A), while the five-year SRFS of the PD-L1-negative and PD-L1-positive groups was 85.4% and 57.9%, respectively (Fig. 2B). In the log-rank test, significant differences were observed between the two groups (p = 0.001). Furthermore, the five-year SRFS of the negative/low, moderate, and high PD-L1 expression groups was 84.2%, 72.4%, and 34.3%, respectively (Fig. 2C). In the log-rank test, a significant difference in SRFS was observed between the high and the negative/low groups (p = 0.001), but the difference between the negative/low and moderate groups (p = 0.286), or between the moderate and high groups (p = 0.084), failed to meet statistical significance, which was probably due to the small number of patients in the PD-L1-positive subgroups.

Kaplan–Meier survival plots presenting structural recurrence-free survival of (
The first type of multivariate Cox model showed that PD-L1 positivity was independently associated with SR (HR = 2.19 [CI 1.01–4.77], p = 0.047). Level VII LNM was the strongest predictive factor (HR = 9.01 [CI 1.48–54.98], p = 0.017), and postoperative basal serum Ctn levels of 101–1000 pg/mL (HR = 5.03 [CI 1.85–13.73], p = 0.002) or >1000 pg/mL (HR = 5.21 [CI 1.78–15.29], p = 0.003) were also independently predictive of SR (Table 2).
The First Type of Multivariate Cox Analysis for Structural Recurrence-Free Survival in Patients with Medullary Thyroid Carcinoma (n = 201)
For patients without SR, the level included in Cox analyses referred to the Ctn level at the last follow-up; for patients with SR, the level referred to the latest measurement before the first confirmed SR.
CI, 95% confidence intervals; Ctn, calcitonin; PD-L1, programmed death-ligand 1; SR, structural recurrence.
In the second type of multivariate Cox model, PD-L1 positivity also proved to be an independent predictor of SR (HR = 2.17 [CI 1.04–4.53], p = 0.039). Stage IV disease (HR = 5.22 [CI 1.02–27.45], p = 0.046) and postoperative basal serum Ctn of 101–1000 pg/mL (HR = 5.09 [CI 1.89–13.71] p = 0.001) or >1000 pg/mL (HR = 6.32 [CI 2.28–17.58], p < 0.001) were also strong and independent predictors (Supplementary Table S1).
PD-L1 expression and BcR/BcPD of MTC patients
The first type of multivariate logistic analysis showed that PD-L1 positivity was independently associated with BcR/BcPD (OR = 3.16 [CI 1.16–8.66], p = 0.025). Moreover, level VI (OR = 5.44 [CI 1.52–19.49], p = 0.009), lateral neck (OR = 31.58 [CI 9.91–100.67], p < 0.001), and level VII LNM (OR = 26.85 [CI 4.60–156.68], p < 0.001) were also independent risk factors for BcR/BcPD (Table 3).
The First Type of Multivariate Logistic Analysis for Biochemical Recurrence/Persistent Disease in Patients with Medullary Thyroid Carcinoma (n = 201)
In the second type of multivariate logistic analysis, PD-L1 positivity also proved to be an independent predictor of BcR/BcPD (OR = 3.09 [CI 1.26–7.59], p = 0.014). Stage III (OR = 6.64 [CI 1.92–22.98], p = 0.003) and stage IV disease (OR = 33.45 [CI 11.18–100.09], p < 0.001) were also strong and independent risk factors (Supplementary Table S2).
Prevalence of PD-L1 expression in patients developing distant or unresectable locoregional recurrence
Distant or unresectable locoregional recurrence was detected in 20 cases during a median follow-up of 23 (range: 4–137) months after initial surgery. Information of these patients is provided in Table 4. All patients were stage IV at diagnosis and eight (40%) were PD-L1-positive. PD-L1 IHC staining and radiographic images of four representative patients (two PD-L1-positive and two PD-L1-negative) are shown in Figure 3.
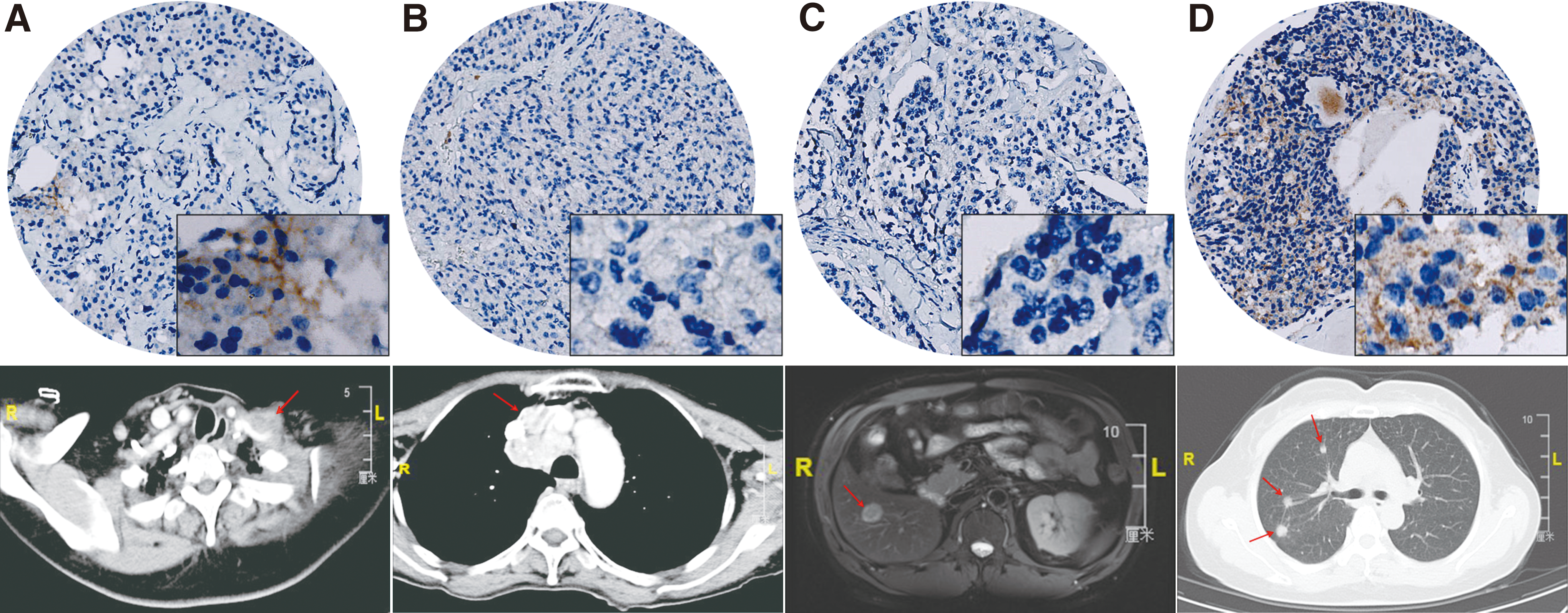
Low (100 × ) and high (400 × ) magnification immunohistochemistry images and radiographic images of four representative patients with distant or unresectable locoregional recurrence. (
Characteristics of Patients Developing Distant or Unresectable Locoregional Recurrence During the Follow-Up Period (n = 20)
Two patients had lateral neck recurrence and received repeated neck dissection before the unresectable metastases occurred.
Some patients had multiple sites of incurable metastases.
Two patients were separately enrolled in two phase II clinical trials for anlotinib (NCT01874873) and sulfatinib (NCT02614495) in the treatment of advanced MTC.
EBRT, external beam radiation therapy.
After initial surgery, two patients had lateral neck recurrences and underwent repeated neck dissections before unresectable metastases became apparent during follow-up. Two patients were separately enrolled in two phase II trials for anlotinib (
Discussion
For thyroid malignancies, most PD-L1-related studies focused on tumors derived from follicular cells. Regarding PD-L1 expression in MTC, as mentioned above, there were only two previous studies on this topic. Bongiovanni et al. stated that there was very low PD-L1 expression in MTC. In that study, the authors mainly focused on weakly positive staining (1–5%) and a small number (n = 3) of PD-L1-positive patients. However, their study included only 16 patients. In fact, when we reanalyzed the IHC results of these patients (listed in Table 1 in their study) using the CPS algorithm, we found that 18.8% (3/16) could be determined as PD-L1-positive, and one-third (n = 1, CPS = 5) could be determined as having moderate PD-L1 expression (21). In addition, in the other prior study, Bi et al. reported a positive rate of 21.8% (19/89) among 89 MTC patients (22). In the present study, using a much larger cohort of MTC patients, we observed a positive rate of 14.4% (29/201), among whom seven patients had high PD-L1 expression.
Before this study, there was insufficient evidence regarding the prognostic significance of PD-L1 positivity in MTC patients. Regarding the clinicopathological associations, although Bi et al. have reported that coexpression of PD-1 and PD-L1 in MTC was correlated with advanced pathological TNM stages (III/IV) and distant metastases at surgery (22), studies with larger sample sizes are still required to perform a more comprehensive analysis. Our results show that PD-L1-positive MTC is positively associated with a larger tumor size, LNM, as well as more advanced TNM staging, indicating that these patients tend to have a higher preoperative tumor burden. More importantly, to the best of our knowledge, this is the first study to demonstrate the correlation of PD-L1 positivity with SR and BcR/BcPD in MTC. In our study, the Kaplan–Meier survival analysis shows that the five-year SRFS rate of patients with PD-L1-positive tumors is nearly 28% lower than those with PD-L1-negative tumors (57.9% vs. 85.4%). In addition, in both types of MVA, the PD-L1-positive group also has an approximately twofold elevated risk of SR and a threefold higher risk of BcR/BcPD.
In addition to PD-L1 expression, in two types of MVA, TNM staging, postoperative basal Ctn level, and LNM are independently predictive of SR, while TNM staging and LNM are also confirmed to be risk factors for BcR/BcPD. The ATA guidelines recommend that clinicians should consider TNM classification and postoperative Ctn level when predicting outcomes and planning long-term follow-up (5), as they have been documented as the most important prognostic factors (29,30). In the present study, for characteristics (tumor size/ETE/LNM) constituting the T and N classification, LNM, especially level VII metastasis, appears to have the strongest prognostic impact. Previous studies also reported that LNM is the strongest indicator for biochemical cure (31,32). These results suggest that extensive LNM may largely reduce the likelihood of surgical cure, while the compromised prognosis associated with level VII metastases may be explained by an increased risk for lung metastases (33).
Despite the relatively low positive rate (14.4%) in the entire MTC population, PD-L1 expression in distant or locally advanced disease may have a greater clinical significance. In this study, 8 (40%) of the 20 cases developing distant or unresectable locoregional recurrences were found to have PD-L1-positivity. The increased tumor aggressiveness and recurrence risk of the PD-L1-positive disease may explain the higher positive rate in advanced disease, which suggests a potential for PD-1 blockade in the treatment of late-stage MTC.
For patients with advanced MTC, there is almost no treatment that can prolong overall survival (6). In China, cabozantinib and vandetanib have not been approved due to the lack of clinical trials in Chinese patients with advanced MTC, for whom effective therapies become even more limited. There is no robust evidence of improved outcomes based on the clinical trials for small-molecule kinase inhibitors such as sorafenib and sunitinib (34 –37). Furthermore, conventional cytotoxic drugs are characterized by low response rates of short duration (5). Anti-PD-1/PD-L1 therapies may provide additional options for patients with advanced MTC, but this requires formal demonstration in clinical trials.
Of note, the therapeutic effect of immune checkpoint inhibitors (ICIs) is not simply influenced by PD-L1 expression of primary lesions. Although positive PD-L1 expression in primary tumor increases the likelihood of treatment responses (38,39), it is not a completely reliable predictive biomarker. It is reported that the results of PD-L1 staining may vary with IHC assays, which may result in “misclassification” of the PD-L1 status for some patients and this could lead to a reduction in the predictive ability of response to ICIs (40,41). The discordance of PD-L1 positivity in primary and metastatic lesions may be another reason for variable therapeutic responses (42,43). However, the primary tumor is still used more frequently to screen patients for clinical trials because it is usually much easier to obtain and analyze. If feasible, analysis of both the primary tumor and metastatic foci may be a better way to evaluate and predict the potential benefits of ICIs for an individual patient.
In addition to PD-L1 expression, microsatellite instability (MSI) and tumor mutational burden (TMB) are also found to be important predictive biomarkers. High MSI (MSI-H) or high TMB (TMB-H) status is correlated with increased neoantigen load, which elicits stronger immune responses and upregulation of immune checkpoints, including PD-1 (44). MSI-H and TMB-H status may partly explain why some patients with low or even negative PD-L1 expression can respond to anti-PD-1 antibodies. Meanwhile, in clinical practice, some nonresponders with high PD-L1 expression are also observed. It is generally accepted that even if tumor cells highly express PD-L1, an effective response still requires tumor-infiltrating lymphocytes with PD-1 expression in the TME (44 –46). For a more comprehensive evaluation, a T cell-inflamed gene expression profile (GEP), including 18 genes related to chemokine expression, immunological infiltration, and adaptive immune resistance, has been developed and it was shown to independently predict the therapeutic effect of PD-1 blockade (38,47). It is also noteworthy that although PD-L1 expression cannot accurately predict the therapeutic benefit for each individual, PD-L1-positive patients are generally more likely to obtain survival benefit from ICIs (48,49). Ott et al. also reported that PD-L1 expression can still independently predict therapeutic responses after controlling for TMB and GEP across 20 cancers (38). Consequently, comprehensive assessment of MSI, TMB, and T cell-inflamed GEP, as well as PD-L1 expression, can be useful to better identify patients who have a higher likelihood of response to ICIs in future clinical trials for advanced MTC.
Some limitations should be acknowledged. First, on account of the relatively good overall prognosis of MTC, only 12 disease-related deaths (4 of them in patients with PD-L1-positive tumors) have been observed; therefore, an association between PD-L1 positivity and mortality cannot be evaluated due to the insufficient events. Similarly, only 20 patients developed incurable recurrences. Although a high PD-L1-positive rate is observed, more late-stage patients with available tissue for analysis are needed for validation if large-scale multicenter studies are conducted in the future. Second, the RIA kit used before September 2011 has a broad reference range. Fortunately, most patients treated before this time have records of basal Ctn levels measured by CLIA or ECLIA in recent years, and thus, the postoperative basal Ctn levels included in MVA are minimally affected by the insensitive RIA results. Third, this study is also limited by its retrospective nature.
In conclusion, we demonstrate that PD-L1 positivity is associated with aggressive clinicopathological characteristics and is predictive of structural disease recurrence and BcR/BcPD in patients with MTC. Meanwhile, compared with the entire MTC population, the higher PD-L1 prevalence in patients who developed incurable recurrent disease may suggest a promising prospect of anti-PD-1/PD-L1 immunotherapy in the treatment of advanced MTC. Further prospective multicenter studies are expected to confirm our conclusions and the actual therapeutic effect of PD-1 blockade should await the results of clinical trials.
Footnotes
Acknowledgment
This study was supported by the National Science Foundation of China (81472498 and 81772851 to Y.-L.W. and 81572622 to Q.-H.J.).
Author Disclosure Statement
The authors declare that there are no potential conflicts of interest.
Supplementary Material
Supplementary Table S1
Supplementary Table S2