
Abstract
Background:
The treatment efficacy of antithyroid drug (ATD) therapy, radioactive iodine (131I), or surgery for Graves' hyperthyroidism is well described. However, there are a few reports on the long-term total outcome of each treatment modality regarding how many require levothyroxine supplementation, the need of thyroid ablation, or the individual patient's estimation of their recovery.
Methods:
We conducted a pragmatic trial to determine the effectiveness and adverse outcome in a patient cohort newly diagnosed with Graves' hyperthyroidism between 2003 and 2005 (n = 2430). The patients were invited to participate in a longitudinal study spanning 8 ± 0.9 years (mean ± standard deviation) after diagnosis. We were able to follow 1186 (60%) patients who had been treated with ATD, 131I, or surgery. We determined the mode of treatment, remission rate, recurrence, quality of life, demographic data, comorbidities, and lifestyle factors through questionnaires and a review of the individual's medical history records.
Results:
At follow-up, the remission rate after first-line treatment choice with ATD was 45.3% (351/774), with 131I therapy 81.5% (324/264), and with surgery 96.3% (52/54). Among those patients who had a second course of ATD, 29.4% achieved remission (vs. the 45.3% after the first course of ATD). The total number of patients who had undergone ablative treatment was 64.3% (763/1186), of whom 23% (278/1186) had received surgery, 43% (505/1186) had received 131I therapy, including 2% (20/1186) who had received both surgery and 131I. Patients who received ATD as first-line treatment and possibly additional ATD had 49.7% risk (385/774) of having undergone ablative treatment at follow-up. Levothyroxine replacement was needed in 23% (81/351) of the initially ATD treated in remission, in 77.3% (204/264) of the 131I treated, and in 96.2% (50/52) of the surgically treated patients. Taken together after 6–10 years, and all treatment considered, normal thyroid hormone status without thyroxine supplementation was only achieved in 35.7% (423/1186) of all patients and in only 40.3% of those initially treated with ATD. The proportion of patients that did not feel fully recovered at follow-up was 25.3%.
Conclusion:
A patient selecting ATD therapy as the initial approach in the treatment of Graves' hyperthyroidism should be informed that they have only a 50.3% chance of ultimately avoiding ablative treatment and only a 40% chance of eventually being euthyroid without thyroid medication. Surprisingly, 1 in 4 patients did not feel fully recovered after 6–10 years. The treatment for Graves' hyperthyroidism, thus, has unexpected long-term consequences for many patients.
Introduction
Graves' disease (GD) is a common thyroid condition with an incidence of 20–50 per 100,000 inhabitants (1,2) and a lifetime risk that is highest among women between 30 and 60 years of age (2,3). Individuals who develop GD are mostly in the working age and the disease can lead to prolonged sick leave and overall decreased productivity (4). GD can also increase long-term morbidity and mortality, including short- and long-term cognitive deficits and impairment of quality of life (QoL) (5 –17). As GD has a major impact on affected individuals, the objectives of treatment are to safely and quickly normalize the thyroid function, avoid adverse treatment effects, prevent recurrence, and maintain long-term normal thyroid function with restoration of premorbid QoL.
The therapeutic possibilities for GD treatment include antithyroid drugs (ATD), radioactive iodine (131I), or surgery. The choice of both the initial and subsequent therapy for GD often differs according to guidelines and local traditions. Using a 42-year-old index woman with moderate hyperthyroidism without thyroid-associated ophthalmopathy (TAO), thyroidologists in Europe and Asia chose ATD as their first choice of therapy. In contrast, in the United States, the use of 131I treatment is favored although the prevalence of this choice seems to be declining (18 –20). Established treatment preferences and management may change over time due to experiences obtained from new studies, implementation of updated evidence-based guidelines, or changes in expert opinion of specialists (19,21 –24).
Each of the treatment modalities has specific limitations in effectiveness and possible adverse effects. Therapy with ATD carries a high recurrence rate (40–60%), leading to potential prolonged exposure to thyrotoxicosis, thereby causing adverse health outcomes (2,25 –27). In addition, there are both common mild adverse effects caused by ATD treatment, such as rash and pruritus, and rare but serious side effects such as agranulocytosis or liver failure (28 –30). The use of 131I treatment most often causes permanent hypothyroidism, increases the risk of TAO and morbidity as well as possible impaired long-term QoL (7,12,17,31 –37).
The third treatment option for GD, surgery, exposes the patient to surgical risks, such as damage of the recurrent nerves and surgical acquired hypoparathyroidism (38). Both 131I therapy and surgery are thyroid ablative treatments, necessitating lifelong thyroid hormone replacement (39). The choice of therapy for GD, consequently, requires the clinician to carefully consider both short- and long-term efficacy and risks in the discussion on therapeutic choices with the patient to ultimately decide which modality they prefer (9,10,20).
There are a few randomized trials of treatment of GD and, in particular, of the long-term effectiveness of the therapies (5,26,37,40,41). Our current knowledge of outcomes and adverse events is based on retrospective evaluations of clinical outcomes (18,20,30). In addition, most reported clinical outcomes after treatment of GD have been obtained with short-term follow-up and do not compare all three modalities. Understanding the impact of how one or more of the modalities for GD treatment affect health outcomes after a longer time frame would have important implications for choice of treatment for both clinicians and patients.
The aims of the present investigation were to study the clinical results 6–10 years after initial diagnosis regarding: (a) the efficacy of each therapeutic modality on disease remission; (b) the initial and subsequent utilization of each therapy during the whole period; (c) the efficacy of each therapy to normalize thyroid function and what proportion of patients maintain euthyroidism without levothyroxine replacement; and (d) the patients' long-term overall QoL and satisfaction with the different treatment modalities.
Materials and Methods
Study design
The study was planned as a pragmatic trial, as we wanted to investigate the effectiveness of the three modalities of therapy in our usual and standard practices throughout Sweden. In 2003–2005, all patients with newly diagnosed Graves' hyperthyroidism or toxic nodular goiter (TNG) (n = 2916) were registered in 7 cities in Sweden involving 13 endocrine clinics that covered a referral population corresponding to 40% of the Swedish population (1). GD was diagnosed by a suppressed thyrotropin (TSH) and elevated concentrations of more than one of the following thyroid hormones: free thyroxine (fT4), total triiodothyronine (T3), and/or free triiodothyronine (fT3) in combination with elevated thyroid-stimulating hormone receptor antibodies (TRAb) and/or an increased diffuse isotope uptake on thyroid technetium scintigraphy (1,3).
Patients with subclinical hyperthyroidism defined as only a low or suppressed TSH were excluded. Follow-up was between 6 and 10 years (2011–2013) after the original diagnosis. From the original 2003–2005 cohort of 2916 patients, the following were excluded: (a) 640 patients with TNG, (b) 8 patients in whom the diagnosis was not confirmed, (c) 64 patients who were younger than the age of 18 years at the time of diagnosis, (d) 137 patients who had died as verified by the Swedish Civil Registry, (e) 24 patients who had emigrated, and (f) 67 subjects who were lost to follow-up (Fig. 1).
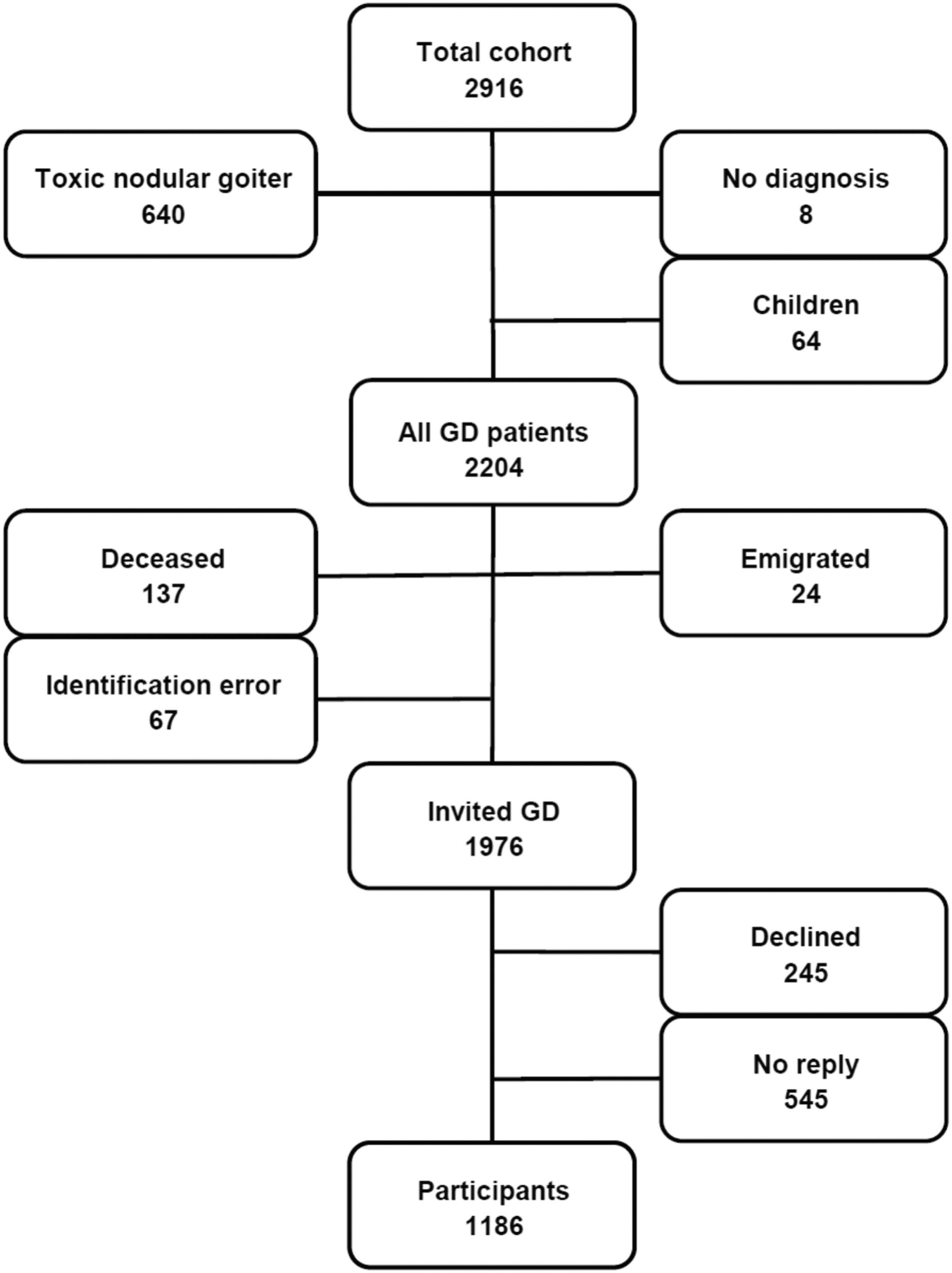
Flowchart illustrating the inclusion/exclusion of individuals in the study.
Altogether, 1976 patients who had GD were invited by letter to participate in the follow-up study. They received a clinical questionnaire comprising 68 questions (Appendix Table A1) together with 1 generic (SF-36) and 1 thyroid-specific (ThyPRO) QoL questionnaire, all in Swedish. If no answer was received, the patients were sent two additional reminders by mail and if there still was no reply, we attempted to contact the patients by telephone.
Subjects
A total of 1186/1976 (60%) of the patients agreed to participate whereas 245 patients (12.4%) declined (Fig. 1 and Table 1). The medical history records of the 1186 included patients were reviewed with respect to their treatment modality, the order of treatments, and the recurrence of disease after each treatment course. In addition, the medical history record was reviewed if an answer to a question in the questionnaire showed inconsistency or otherwise necessitated verification of issues such as diagnosis, treatment, or occurrence of TAO.
Baseline Data at Inclusion in Original Cohort 2003–2005 for the 1186 Included Participants with Graves' Disease in the Follow-Up 2011–2013 and for the 545 Individuals Who Did Not Reply to the Study Invitation (Nonrepliers)
The number of patients included in each analysis is noted.
ATD, antithyroid drugs; 131I, radioactive iodine; SD, standard deviation; TAO, thyroid-associated ophthalmopathy.
The remaining 545 (28%) of the 1976 invited GD patients did not reply and were defined as “non-repliers” (Fig. 1 and Table 1). The nonreplier group poses a risk for selection bias in relation to the 60% (1186) of the included study cohort. The medical records of each patient in the nonreplier group were, therefore, also reviewed with respect to their treatment modality, the order of treatments, and the recurrence of disease after each treatment course.
Treatment strategies for GD in Sweden 2003–2005
During 2003–2005, ATD was mostly administered as block-and-replace treatment. This approach was used due to our traditions and in hopes of promoting long-term remission in GD patients without the need for additional ATD or levothyroxine replacement. Only ∼2% of patients were treated by monotherapy with low-dose methimazole or propylthiouracil, which is generally the dominant approach in other countries such as the United States. Depending on the severity of disease and local clinical practice, the majority of patients (98%) were prescribed 10–15 mg methimazole twice daily or 100 mg propylthiouracil thrice daily with addition of levothyroxine after two to four weeks to achieve euthyroidism.
After two to six months of ATD therapy, the long-term strategy was discussed with the patient, and a decision was made to continue ATD with or without levothyroxine therapy or to choose an ablative treatment. The reasons for ablative thyroid therapy included a wish to soon become pregnant, adverse events to ATD, other compromising medical conditions exposing the patient to a higher medical risk, the persistence of high TRAb values, an estimated high recurrence rate (high hormone levels and/or moderate or large goiter), as well as the patient's preference. Some patients received 131I therapy without preceding ATD.
ATD treatment was generally given for 12–18 months, at which time TRAb was measured before the end of the ATD treatment. ATD therapy was discontinued if the TRAb level had been normalized or was very close to the upper reference range for the method. In cases where patients had mild to moderate or more severe TAO, continued ATD or surgery was chosen. In case of relapse of hyperthyroidism, if a second treatment period of ATD therapy was chosen, it was continued for at least 12 months with measurement of TRAb again to determine whether the medication could be stopped. However, patients were informed of the increased risk of future recurrence, and recommendations for ablative treatment were generally given.
Patients with mild disease were treated with beta-blockers only and were followed with monitoring of laboratory parameters. Our practice, in general, for using 131I therapy was to administer one dose of 131I aiming at achieving hypothyroidism. The dose of 131I activity was calculated individually in 464 out of 505 patients (91.9%) using the thyroid volume, percentage of 24-hour 131I uptake and after 5–7 days (T1/2) to achieve an absorbed dose of 120 Gy to the thyroid gland. In two centers (41/505 patients, 8.1%), 131I therapy was given as a fixed dose: 350 Mbq for TRAb-positive GD and 550 Mbq for TRAb-negative GD patients.
Surgical treatment was performed as total thyroidectomy. However, a subtotal thyroidectomy was performed in 5% (13/278 patients undergoing thyroid surgery).
Definition of parameters used for evaluation
First-line treatment was defined as the initial mode of treatment chosen.
A treatment period was defined as the period from the start of treatment until remission was expected. This period was predominantly between 12 and 18 months for ATD.
Remission was defined as euthyroidism three to six months after intervention (last ATD, surgery, or 131I). For patients with ATD discontinuation, most patients were followed for six months. If the patients did not reappear in the files and did not mention relapse in their questionnaire, we defined them as in remission.
Questionnaires
After informed consent was obtained, the patients were administered a 68-item clinical patient questionnaire developed for this specific study (Appendix Table A1). The questionnaire comprised questions regarding smoking habits, demographic data, comorbidity, autoimmunity, menopause, symptoms, presence and treatment of TAO, initial treatment of hyperthyroidism, recurrence of hyperthyroidism, its successive and final treatment, and a question as to whether the patient felt recovered from the thyroid disease (Appendix Table A1).
The QoL was assessed in three ways: (a) a visual analog scale graded 1–10 regarding “how do you feel today?,” where 1 represented as “very bad,” and 10 as “very good”; (b) ThyPRO, a thyroid-disease specific questionnaire for patients with benign thyroid disorders that have been translated into and validated in Swedish (42,43); and (c) the validated Swedish 36-item Short Form Health Status Survey questionnaire (SF-36) (44). The QoL results regarding ThyPRO and SF-36 results have been reported separately (17).
Data management and validation
All data capture sheets in the questionnaires were auto-scanned and transferred into a database by using a licensed scanning software (Remark Office OMR 8©; Remark, Malvern, PA). The study personnel validated the auto-scanning through manual control. Scanning errors were observed in 0.92% and were corrected in the data file. The database was validated with cross-checking of key points such as sex, age, eye symptoms, treatment number and modality, relapse, comorbidity, type 1 diabetes, and Addison's disease, with the medical history records from 5% of randomly selected patients. The noted discrepancies were less than 1% and were corrected in the database.
Statistical analyses
Demographic data were analyzed by using Pearson's chi-square for categorical variables and unpaired T-test for continuous variables. Odds ratios were analyzed by using linear and multivariate regression. Statistical analyses were performed by using IBM SPSS Statistics 22.0.0.1 64-bit edition (SPSS Institute, Chicago, IL). Statistical significance was set at p < 0.05.
Ethics
The study was approved by the Regional Ethics Committee in Uppsala (Dnr 2012/035, April 4, 2012). The same committee additionally approved a review of the nonreplier group (Dnr 2012/035/2, February 24, 2015). The study was performed according to the Declaration of Helsinki.
Results
Baseline characteristics at diagnosis
The follow-up time was 6–10 years (8 years ±0.9, mean ± standard deviation), and the mean age at diagnosis was 46.9 years. The female-to-male ratio was 4.6:1 (Table 1). The proportion of active smokers was 28.9%. Information on TAO was available in 1185 out of 1186 of the patients, and 21.1% were considered to have TAO by established criteria at the time of diagnosis and according to an experienced endocrinologist and/or ophthalmologist (1,45). Detailed information on TAO in the study will be published in a separate manuscript.
Long-term treatment outcome
ATD as first-line treatment—remission rates
Of the included 1186 patients, ATD was used as first-line treatment in 774 patients (65.3%) (Table 2). Of these, 178 patients switched to ablative treatment during the first treatment period whereas 596 (77%) patients completed one 12–18-month course of ATD. Of those completing one treatment period with ATD, 351 (58.9%) were in remission at follow-up (Table 2). However, due to change of treatment, the remission rate at follow-up for all who started ATD dropped to 45.3% (351/774). Relapse after the first treatment period was noted in 245 patients and 119 of these were re-treated with ATD, which resulted in 29.4% (35/119) still in remission at follow-up. Providing a second ATD course, thus, resulted in significantly fewer long-term remissions than the first ATD course (p < 0.001). Two treatment periods with ATD increased the total proportion of patients in remission only marginally from 45.3% to 49.9% (386/774).
Long-Term Result of First-Line Treatment with Antithyroid Drugs, 131I Radiotherapy, Surgery, or Conservative (Expectancy) Treatment in a Cohort of Patients Diagnosed with De Novo Graves' Hyperthyroidism 2003–2005
At the follow-up after the first-line treatment only.
At follow-up among the ones in remission after first-line treatment.
Due to adverse reactions, development or worsening of TAO, persistent or high levels of TRAb, patient wishes, or desired pregnancy.
At follow-up after changed treatment during the first treatment period.
Total number of patients in remission after first-line treatment inclusive of patients who underwent change of first-line treatment.
TRAb, thyroid-stimulating hormone receptor antibodies.
ATD as first-line treatment—preserved thyroid function
Of the 351 patients in long-term remission after one completed ATD course, 270 (77%) were without levothyroxine substitution at follow-up (Table 2). Of the 35 patients in remission after a second course of ATD, 25 (71.4%) were without levothyroxine substitution at follow-up. Of the total number of 396 patients who remained in remission after one or several ATD courses, 305 (77%) had normal thyroid function after 6–10 years (Table 3). The remaining 23% (91/396) received substitution with levothyroxine.
Total Number of Patients in the Treatment Groups and the Extent of Levothyroxine Treatment at Follow-Up After 6 to 10 Years
Administered treatment during the whole follow-up period in any order.
Number of levothyroxine-treated patients at the end of the study period.
ATD treatment only, one or several courses, and including patients who started with conservative treatment.
I but no surgery.
Surgery but no 131I.
I plus surgery.
Patients who were followed and monitored and when needed substituted with levothyroxine.
Taken together, of all the 774 patients who started ATD treatment, 325 (40.3%) had preserved thyroid function without the need for levothyroxine substitution 6–10 years after the diagnosis of GD.
ATD as first-line treatment—change to ablative treatment
Of all the 774 patients who started ATD, 178 (23%) patients changed to ablative treatment during the first treatment period. The reasons were: adverse effects, new development or worsening of an existing TAO, persistent high TRAb values, or the patient's desire to change therapy. Of the 119 patients who were selected for a second course of ATD after relapse, 36% (43/119) ultimately received surgery and 26.9% received (32/119) 131I therapy (Fig. 2a).

At the end of the study period, 27.8% (215/774) initially ATD-treated patients had undergone surgery and 21.9% (170/774) had been 131I treated (Fig. 2a). Taken together, a patient who was selected to ATD as first treatment and subsequently possibly had additional ATD treatment had 49.7% risk (385/774) of undergoing ablative treatment during the 6–10 years of follow-up.
131I as first-line treatment
131I was used as initial treatment in 324 patients (27.3%), of whom 264 (81.5%) were still in remission at follow-up after one treatment course (Table 2). In total, 42.6% (505/1186) were treated with 131I during the whole study period (Fig. 2a–d) and 131I treatment at any time resulted in hypothyroidism in 83.2% (420/505) patients requiring levothyroxine replacement post-therapy (Table 3). Although only 27% of the 1186 patients initially were chosen to receive 131I treatment, almost 45% had been treated with 131I at the end of the study period.
Surgery as first-line treatment
Surgery was chosen as the optimal first-line treatment in 54 (4.6%) patients (Fig. 2c). Among these, 52 (96.3%) patients were still in remission at the end of the study period (Table 2). Recurrence was noted in two patients, who received 131I therapy that resulted in remission (Fig. 2c). Among all the included GD patients in the study, 23.4% (278/1186) had thyroid surgery during the whole study period (Fig. 2a–c). Lifelong supplementation with levothyroxine was needed in 265 out of 278 (95.3%) of the patients but not in 13 out of 278 (4.7%) of the patients who were operated with subtotal thyroidectomy. Twenty patients received both 131I and surgery in varying order.
Conservative treatment
Conservative treatment (expectancy while monitoring the thyroid hormone levels) was chosen for 34 (2.9%) patients (Fig. 2d). Twenty-seven of these (79.4%) returned to a euthyroid state without any treatment, whereas the remaining 7 patients received ATD, of whom 2 patients ultimately were given 131I. At follow-up, 5 out of 27 (18.5%) patients with only conservative treatment were on lifelong substitution with levothyroxine.
The patients' evaluation of their treatment
At the end of the study period, 25.3% of the patients reported that they had not yet fully recovered. Among the patients who described a cause for this, the most common reasons were tiredness (25.3%), eye-related problems (13.5%), levothyroxine substitution problems (12.5%), or additional unspecified treatment problems (10.4%). Another 10.4% reported concerns about living with a lifelong disease with the risk of recurrence as the motive for not feeling fully recovered. There were no significant differences in the proportion of patients who felt fully recovered between the different treatment groups (data not shown). However, the proportion of patients who felt fully recovered was significantly lower in the patients with levothyroxine substitution (64.0%; 488/763) compared with the patients without levothyroxine replacement (81.1%; 343/423) (p < 0.001).
Comparison to the nonreplier group
The included group differed significantly from the nonreplier group regarding a number of variables (Table 1). The 1186 included patients were more often born in Sweden or Europe, were 4.4 years older, less frequently treated with ATD, and more often treated with 131I or surgery compared with the nonreplier group. The two groups did not differ regarding smoking status or presence of TAO. The proportion of patients who were in complete remission after first-line treatment was higher in the included patients with 58.5% (694/1186) compared with the nonreplier group with 41.8% (228/545; p < 0.001). Although there may be a number of defined and undefined reasons for a patient not to reply, it appears that they were more often born outside Europe and may have had a more complex treatment course.
Discussion
To the best of our knowledge, this is the largest and longest longitudinal study of patients treated for Graves' hyperthyroidism evaluating the three therapeutic modalities. The study evaluated a cohort of patients with overt and previously untreated hyperthyroidism due to GD. The main observations of the study are that a substantial number of patients with GD will need lifelong levothyroxine substitution independent of the initial treatment modality. The effects of ATD treatment to produce long-term remission in GD, in particular, are disappointing.
In the clinic, the possibility of a 58.9% chance that one completed course of ATD will result in long-term remission is quite promising to both the clinician and the patient. However, this promising chance is only true for those who complete a full ATD course and does not include the risk of subsequent levothyroxine substitution. When starting ATD and considering the possibility of a preserved thyroid function, the chance is considerably lower. The fact that about half of the initially ATD-treated patients end up with ablative treatment, and 23% of the ATD treated in long-term remission end up with levothyroxine treatment makes the actual percentage of preserved thyroid function drop to only 40.3%.
ATD treatment is the only modality that offers the patient a realistic chance of preserving normal thyroid function. Informing patients of this option has a major impact on the patient's choice of treatment. Even with ATD therapy alone without subsequent ablative therapy, our observation that almost one of four patients (23.8%) required levothyroxine replacement after 6–10 years indicates that the use of ATDs for therapy is not optimal with respect to preserve normal thyroid function. Our rate for levothyroxine replacement is higher than the 1% previously observed over a four-year period but in agreement with an early study (27,46).
The reason for levothyroxine-substitution of the patients may be several: The first supports the concept that ongoing immune thyroiditis in GD results in thyroid failure (2). Second, the patient's clinician may be more prone to prescribe levothyroxine to prevent hypothyroid symptoms and development or worsening of TAO (40). We have, in a previous study, observed the latter to be associated with unstable control of thyroid hormones, including suboptimal substitution with levothyroxine (26). Third, but less likely, some patients may have developed blocking TRAb. In conclusion, the risk of hypothyroidism in a GD population many years after ATD therapy is highly significant and needs to be disclosed as a possible risk when a new patient with Graves' hyperthyroidism is advised on choice of treatment.
What are the treatment options if there is recurrence of hyperthyroidism after ATD treatment? A second course of ATD will result in a chance of remission of 29.4%, but the chance of future preserved thyroid function (i.e., euthyroid without thyroid hormone therapy) is only 21%. Therefore, the recurrence of hyperthyroidism after ATD may be best treated with ablative therapy. This therapeutic option was corroborated by this study where a high proportion of patients (63%) who were selected for a second treatment period of ATD treatment ultimately received ablative treatment.
A second treatment period of ATD is also against recommended treatment guidelines by the European Thyroid Association published in 2018 (24). Taken together, a second course of ATD will, according to this study, result in only around 3 in 10 patients achieving long-standing remission. Further, only about one fifth of the patients will maintain normal thyroid function. The alternative to use daily long-term, low-dose ATD has in recent years been proven efficient and safe, but it was not in our practice during the study period (47,48).
The need for a second treatment after 131I therapy was 20%, a percentage much higher than after surgery, but in line with a previous prospective, randomized study of 21% (26). 131I therapy is supposedly ablative but 16.8% of the patients, who were in remission from hyperthyroidism by 131I as first treatment choice, needed no levothyroxine replacement at the end of the follow-up. These results may be related to the dose of 131I used, which may be lower in Sweden than the average activities in the United States and other locations.
Our study reveals a more than doubled proportion of patients selected to surgery as first-line treatment when compared with the 2.1% in a 2013 European survey of an index case of Graves' hyperthyroidism (22). One reason may be that surgery is an effective and relatively quick method to treat hyperthyroidism (26). A second reason is most likely that in premenopausal women with an explicit wish to become pregnant we prefer thyroid surgery and avoid ATD and 131I due to possible adverse effects on the fetus and the post-treatment rise in TRAb levels after 131I therapy, respectively (26,49,50). Finally, easy access to competent surgical care may also influence the choice of therapy (51).
The use of 131I as the first-line treatment was 27.3%, which is more frequent than the 14.1% in the 2013 European survey, and less frequent than the 59% in the 2011 U. S. survey of the same index case (19,22).
If patients with more active disease such as high thyroid hormone values and/or TRAb titers, young age, and/or large goiters are included, the risk of recurrence increases (18,25,52,53). This could be an explanation for the higher recurrence rates (60.5%) in the ATD-dominated initial treatment strategy from Korea by Kim et al. (18). Alternatively, using 131I as initial therapy will result in lower recurrence rates, for instance, 27.4% as reported from the United States by Sundaresh et al. (20).
The recurrence rate after surgery differs depending on the surgeon's experience and technique (54,55). Our recurrence rate after surgery was 3.8%, which is in line with the previously reported 1–28% (26,56). Use of surgery as first-line therapy is by tradition higher in Sweden than other European countries. At the end of the follow-up period, 23% of the patients had undergone thyroidectomy, which most likely can be due to Swedish preferences in subjects younger than 35 years of age.
One out of four patients did not feel fully recovered at follow-up, although their hyperthyroidism was in long-term remission and the patient was euthyroid. It is known that the recovery of well-being in many patients is delayed (7,16,26,57,58). They have an increased probability of sick leave the first year after diagnosis (4,5,26). In the next few years, they also have an increased risk of disability status (4,15). It is not known what specific symptoms or diagnosis are the major cause(s). However, the presence of TAO may contribute, as this condition significantly increases the risk for inability to work (4,5).
In our survey, patients not fully recovered reported tiredness as a cause more often than eye symptoms. In addition, patients on levothyroxine replacement therapy were also more likely to report nonrecovery compared with those without therapy. This difference may relate to the issue of levothyroxine substitution and concerns regarding living with a lifelong disease or to the reason why levothyroxine was initiated in the first place in nonablative patients. In this study, 25% of the patients did not feel fully recovered after 6–10 years, which differs from the 10% to 16% after 3 years in the study by Torring et al. (26).
The two studies, however, are different in size, design, and follow-up. The study by Torring et al. comprised 179 prospective, randomized patients followed for three years at one university center. The choice that the patients had to make for first-line treatment after comprehensive information was whether they would participate in the randomized study between treatment alternatives ATD, 131I, or surgery, or not. This may also have influenced the patients' report of a high percentage of satisfaction with their treatment in that study (90%). A question of overall treatment satisfaction was most unfortunately not included in the present follow-up, where instead SF36 and ThyPRO were used.
There were no significant treatment-related differences in the proportion of patients who felt fully recovered (data not shown). This corroborates our previous observation in the study by Torring et al., where the proportion of patients who did not feel recovered after >12 months was similar (16–20%) between ATD, 131I therapy, and surgery (26). This is also in accordance with our other previous studies estimating QoL outcome after treatment (5,7). However, in a substudy to this study on the same cohort, we did find treatment-related differences by the ThyPRO and SF36 questionnaires (17), possibly due to a larger number of subjects compared with our previous studies.
The long-term QoL and mental health consequences of GD and hyperthyroidism need further investigation, particularly in other more diverse populations. Our study demonstrates that the effects of lifelong medication need to be considered when planning therapy for GD (59). Our findings also support the latest European Thyroid Association guidelines suggesting an annual follow-up of treated GD patients (24).
Clinicians frequently assume that GD is a transient disease and when a patient reaches euthyroidism the premorbid QoL and health is restored. On the contrary, our results show that GD can be a chronic disease with both short- and long-term effects on overall patient well-being and that, despite choice of therapy, there is a high risk of permanent thyroid failure. Our study also demonstrates that there is an unmet need to improve GD treatment by being able to identify those who will be cured with one course of ATD treatment versus the 15% of patients who will have a recurrent complex disease and a need for ablative treatment (52). There are promising attempts at better baseline predictions of relapse using the clinical severity score and the GREAT score (52,60).
There are a number of strengths of our study. The pragmatic trial design reflects our usual practice, all three treatment modalities are included, the cohort is large, and the long follow-up of a predefined incidence cohort limits selection bias. An additional strength is our investigation of the nonreplier group comprising 28% (545/1976) of the total initial cohort in addressing possible major collection bias.
Limitations of this study include that the duration of treatment is lacking, that sufficient data regarding laboratory measurements are lacking, and that the response rate was only 60%, although this is not unusual in follow-up studies of this size and duration.
Due to differences between the participants and the nonrepliers, there is a risk of a slight underestimation of the recurrence rate. The nonreplier group may have chosen not to get involved in a follow-up study involving QoL aspects for various other reasons such as work situation or migration, among others.
In conclusion, the choice of treatment modality for GD requires adequate knowledge of both short- and long-term outcomes for the patient to aid in advising them in their choice. Our study demonstrates that only about one in every three GD patients will be able to continue life without thyroid hormone substitution and about one in four end up with total thyroidectomy. This means that surgery is a treatment modality in five times as many patients compared with their initial choice for surgery in our cohort. Most of these patients will require levothyroxine therapy, as subtotal thyroidectomy surgery is not highly successful in eliminating the need for medication. There is a high percentage of patients (one in four) who report that they are not fully recovered 6–10 years after diagnosis, supporting the recommendation that patients with GD should have long-term follow-up. In summary, our study demonstrates that treatment for Graves' hyperthyroidism has long-term consequences for many patients and reinforces the fact that GD is both a serious condition and the chronic nature of this disease.
Authors' Contributions
All authors treated these patients, collected data, and discussed the form for presentation.
Footnotes
Acknowledgment
Ole Brus, PhD, University of Örebro, for help with statistics and Dr. Anthony Firek, Loma Linda University, CA, for help with the language and text.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-717311+ALFGBG-790271), the Faculty of Medicine at Lund University, the Skåne Research Foundation, the Research Funds of Skåne University Hospital, and Research Foundation in the Uppsala and Örebro Region and Nyckelfonden.
The Questionnaire Was Administered to Patients in Swedish, and It Is Translated Here for Transparency
| 1 | Name ……………………………………………………………….. | ||
| 2 | Sex | Female □ | Male □ |
| 3 | In which country were you born? | Yes □ | No □ |
| 4 | If you were born abroad, which year did you move to Sweden? | …………………………. | |
| 5 | Have your parents, siblings, or children had thyrotoxicosis? | Yes □ | No □ |
| Questions to women (to be completed if you are 20years old or older) | |||
| 6 | Have you given birth to a baby? | Yes □ | No □ |
| 7 | If so, to how many? | …………………………. | |
| 8 | When were your children born (years)? | …………………………. | |
| 9 | Have you used birth control pills for more than 1 year? | Yes □ | No □ |
| 10 | Do you have regular periods? | Yes □ | No □ |
| 11 | If no, how old were you when the periods ceased? | I was …..…. years old. | |
| 12 | Have you used estrogen for menopausal symptoms? | Yes □ | No □ |
| 13 | If so, how many years did you use hormone replacement therapy? | ……………..……years. | |
| Tobacco habits (to be completed if you were 16 or older at the diagnosis of thyrotoxicosis) | |||
| 14 | Have you smoked regularly during any period of your life? | Yes □ | No □ |
| If no, go to question 22. | |||
| 15 | Did you smoke before you were diagnosed with thyrotoxicosis? | Yes □ | No □ |
| 16 | Did you smoke when diagnosed with thyrotoxicosis? | Yes □ | No □ |
| 17 | If so, how many cigarettes/day? | …………………………. | |
| 18 | Are you smoking now? | Yes □ | No □ |
| 19 | Number of cigarettes/day? | …………………………. | |
| 20 | If you stopped smoking, which year did this happen? | …………………………. | |
| 21 | How many years did you smoke? | …………………………. | |
| 22 | Have you regularly used snuff? | Yes □ | No □ |
| 23 | If so, how many years? | …………………………. | |
| 24 | Do you use snuff now? | Yes □ | No □ |
| Eye symptoms due to thyroid disease | |||
| 25 | Have you had eye symptoms related to your thyroid disease? | Yes □ | No □ |
| If yes, the eye problems appeared | |||
| 26 | Before symptoms of thyrotoxicosis | Yes □ | No □ |
| 27 | In connection with symptoms of thyrotoxicosis | Yes □ | No □ |
| 28 | 3 months or more after symptoms of thyrotoxicosis | Yes □ | No □ |
| 29 | Do you still have thyroid-related eye problems? | Yes □ | No □ |
| 30 | Have you received cortisone treatment for your thyroid-related eye problems? | Yes □ | No □ |
| 31 | At which hospital have you been treated for your eye problems? | …………………………. | |
| Treatment | |||
| How was your thyrotoxicosis treated at first onset? (multiple options can be checked) | |||
| Medical treatment question 32–36 | |||
| 32 | methimazole/propylthiouracil with levothyroxine | Yes □ | No □ |
| 33 | methimazole/propylthiouracil without levothyroxine >1 month | Yes □ | No □ |
| 34 | Did you change medication due to side effects during the treatment course? | Yes □ | No □ |
| 35 | Did you ever stop medical treatment (methimazole/propylthiouracil) due to side effects? | Yes □ | No □ |
| 36 | If yes, which side effects? | …………………………. | |
| 37 | Radioactive iodine treatment | Yes □ | No □ |
| 38 | Surgery | Yes □ | No □ |
| 39 | Did you relapse in your thyrotoxicosis after finishing treatment? | Yes □ | No □ |
| If yes, continue with question 40. | |||
| If no, go to question 48. | |||
| How was the thyrotoxicosis treated at relapse (multiple options can be crossed) | |||
| Medical treatment questions 40–44 | |||
| 40 | Methimazole/propylthiouracil with levothyroxine | Yes □ | No □ |
| 41 | Methimazole/propylthiouracil without levothyroxine >1 month | Yes □ | No □ |
| 42 | Did you change medication due to side effects during the treatment course? | Yes □ | No □ |
| 43 | Did you ever stop medical treatment (methimazole/propylthiouracil) due to side effects? | Yes □ | No □ |
| 44 | If yes, which side effects? | …………………………. | |
| 45 | Radioactive iodine treatment | Yes □ | No □ |
| 46 | Surgery | Yes □ | No □ |
| 47 | Have you had further relapses in your thyroid disease? | Yes □ | No □ |
| Order of treatments | |||
| 48 | If you have received several different treatments, in which order did you receive these? | ||
| Medical treatment = 1 | |||
| Radioactive iodine treatment = 2 | |||
| Surgical treatment = 3 | |||
| Box one is first treatment, Box 2 is second treatment, etc. | |||
| □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ | |||
| Current treatment | |||
| 49 | Do you medicate with methimazole/propylthiouracil today? | Yes □ | No □ |
| 50 | Do you medicate with levothyroxine today? | Yes □ | No □ |
| Do you have any of these diseases? (multiple answers can be checked) | |||
| 51 | Diabetes type 1 (diabetes of the young)? | Yes □ | No □ |
| 52 | Vitamin B12 deficiency and medication with Behepan/Betolvex? | Yes □ | No □ |
| 53 | Rheumatoid arthritis? | Yes □ | No □ |
| 54 | Gluten hypersensitivity/celiac disease? | Yes □ | No □ |
| 55 | Addison's disease? | Yes □ | No □ |
| 56 | Pigment changes/Vitiligo? | Yes □ | No □ |
| 57 | Psoriasis? | Yes □ | No □ |
| 58 | Have you or have you had Sarcoidosis? | Yes □ | No □ |
| 59 | Have you or have you had any other chronic illness? | Yes □ | No □ |
| 60 | If so, which one? | …………………………. | |
| 61 | Have you or have you had any cancer disease? | Yes □ | No □ |
| 62 | If so, which one? | …………………………. | |
| Current health status | |||
| 63 | Do you feel recovered after your thyroid disease? | Yes □ | No □ |
| 64 | If no, please state the reason | …………………………. | |
| 65 | How long did it take from the start of the treatment before you felt recovered? | …………………………. | |
| 66 | How do you feel today on a scale of 1–10? Please tick the box below | ||
| □ □ □ □ □ □ □ □ □ □ | |||
| (Very bad)1 5 10 (Very good) | |||
| Other questions | |||
| 67 | Do you have regular contact with the health service for your thyroid disease today? | Yes □ | No □ |
| 68 | If yes, at what hospital? | …………………………. | |
| Clinic? | …………………………. | ||
| Health center? | …………………………. | ||