
Abstract
Background:
The number of thyroidectomies in South Korea has been increasing rapidly due to extensive checkups for thyroid cancer. However, few studies have examined the association between thyroidectomy and major depressive disorder (MDD). We investigated the association between thyroidectomy and the risk of MDD.
Methods:
A population-based electronic medical records database from South Korea was used to identify 187,176 individuals who underwent partial or total thyroidectomy between 2009 and 2016. A self-controlled case series design and Cox regression analyses were used to identify risk factors for MDD.
Results:
Among the 187,176 individuals who underwent thyroidectomy, 16,744 (8.9%) were diagnosed with MDD during the observation period. Of those, 3837 (22.9%) underwent partial thyroidectomy and 12,907 (77.1%) underwent total thyroidectomy. An elevated MDD risk was found during the one-year period before thyroidectomy, with incidence rate ratios (IRRs) of 1.29 ([95% confidence interval [CI] 1.18–1.41], p < 0.0001) for subjects with partial thyroidectomy and 1.27 ([95% CI 1.21–1.33], p < 0.0001) for subjects with total thyroidectomy. After total thyroidectomy, the IRR increased for 31–60 days (IRR 1.81; [95% CI 1.59–2.06], p < 0.0001) and remained elevated for up to 540 days, whereas after partial thyroidectomy, the IRR increased for 31–60 days (IRR 1.68; [95% CI 1.32–2.13], p < 0.0001) but returned to baseline levels after 270 days. Total thyroidectomy was associated with a prolonged risk of MDD compared with partial thyroidectomy in patients with cancer, which was different from the results in patients without cancer.
Conclusion:
The incidence of MDD increased in the period immediately after thyroidectomy and remained high for one to two years. This study highlights the importance of relatively long-term regular psychiatric assessments in patients who undergo partial or total thyroidectomy.
Introduction
Major depressive disorder (MDD) is one of the most detrimental psychiatric disease, characterized by depressive episodes lasting at least two weeks, overt changes in mood and cognition, and vegetative symptoms (1). Although MDD is known to affect ∼6% of the adult population worldwide each year, the estimated lifetime prevalence of MDD ranges from 11.3% to 16.6%, with a female predominance (2). Moreover, MDD has become a serious public health problem because of its strong association with suicide attempts; patients with MDD are at a higher risk (up to 20-fold) of committing suicide than the general population (3 –6).
The link between thyroidectomy and affective disorders such as MDD has not been well established. Several studies have investigated the association between thyroidectomy and postoperative quality of life (QoL) in patients with thyroid cancer (7 –10). Those short-term prospective studies showed improvement or recovery of QoL in the late postoperative period (from four to six months) compared with the preoperative period (9,10). However, Gou et al. found that the QoL of thyroid cancer patients, especially the mental component summary score, was lowest one month after surgery, and it was still worse than the preoperative score two years after surgery (8). Two studies have assessed QoL before and after thyroid surgery for benign thyroid goiters or nontoxic nodular goiters (11,12). However, those studies had several limitations. The cohort of research participants was small (tens or hundreds of subjects) and was recruited from a single center or several selected areas, so those data might not be generalizable to the whole population. When investigating the effects of thyroid surgery on patient mental health, it might be more appropriate and accurate to assess the risk or prevalence of MDD before and after thyroid surgery, using nationwide population data.
To the best of our knowledge, the potential effect of thyroid surgery on MDD risk is still uncertain. Therefore, our purpose in this study was to examine the association between thyroidectomy and MDD incidence using data from a nationwide health insurance-based database. We also investigated the possible effects of thyroidectomy type, along with other contributing MDD risk factors.
Materials and Methods
Database
This study used medical claims data reported to the Health Insurance Review and Assessment Service (HIRA) by ∼80,000 health care service providers (13) as part of the national health insurance program in South Korea. The HIRA claims database contains information about ∼50 million patients per year, ∼98% of the total population of Korea. All diagnoses are coded according to the International Classification of Diseases, 10th revision (ICD-10). Data from HIRA have been previously validated and evaluated in various investigations (14 –19). We obtained the claims data for people who underwent thyroidectomy (ICD-10 codes P4551–4554, P4561) and whose information was submitted by health care providers between January 1, 2009 and December 31, 2016. Patient-specific HIRA data include anonymized identifiers representing each patient together with their age, sex, diagnoses, prescription medications, and type of surgery (13). This study protocol was approved by the institutional review board of Samsung Medical Center in Seoul, South Korea.
Self-controlled case series design
We used a self-controlled case series (SCCS) design to investigate the association between thyroidectomy and depression (20). The SCCS design depends on within-person comparisons in a population of subjects who have experienced both the outcome and the exposure of interest (21). We derived incidence rate ratios (IRRs) by comparing the rate of events during periods in which subjects were exposed to thyroidectomy with the rate during all other observed time periods (i.e., nonexposed period). We used a bidirectional study design and collected data on major depressive events that occurred during the unexposed time both before and after exposure. This study design minimizes confounding because the subjects each act as their own control. The SCCS design controls for potential effects of known and unknown time-invariant confounders such as sex, genetic factors, disease severity, and socioeconomic status (21,22). We adjusted for time-varying factors, such as age and season.
Case identification for SCCS
All data were obtained from secondary electronic records for the study participants. These subjects underwent partial (codes P4551, P4553) or total thyroidectomy (codes P4552, P4554, P4561) between January 1, 2011 and June 30, 2015, and were diagnosed with MDD (codes F32–F33) by psychiatrists at least once between January 1, 2010 and December 31, 2016.
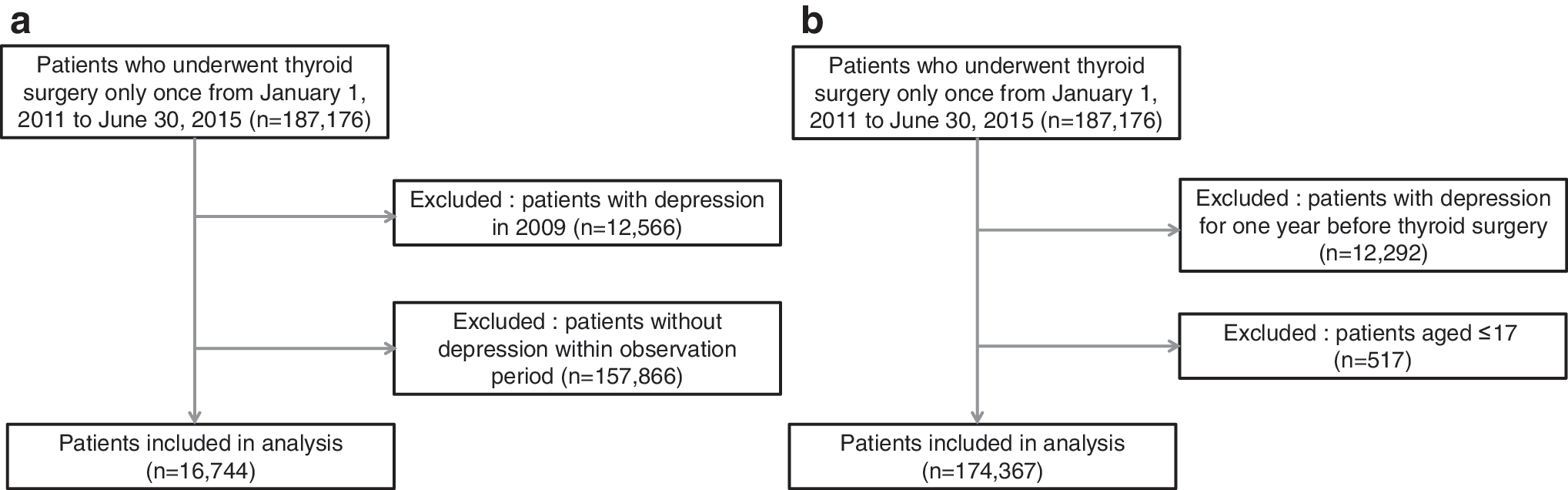
To determine the acute effect of thyroid surgery on MDD, we first defined the pre-exposure and postexposure periods as 360 days before and after surgery, respectively. Later, to rule out the possible postoperative relevant risk of MDD, we redefined the postexposure period as one and a half years (540 days) after surgery. Because we defined the pre-exposure period as the time from 1 year before thyroidectomy to 1 day before surgery and the exposure period as the time from the date of surgery to 540 days after surgery, we narrowed our recruitment period for subjects with thyroidectomy. We excluded subjects who underwent two or more instances of thyroidectomy to avoid any effects that could be caused by multiple surgeries. Also, because subjects with MDD were considered as new patients, we excluded patients who had been diagnosed during the year preceding surgery. For this reason, we also limited our recruitment period for subjects with MDD from January 1, 2010 to December 31, 2016. Figure 1a presents a flowchart describing the selection of participants from the HIRA database for inclusion in this study.
(
Exposures and outcomes
The index date was defined as the first date of thyroid surgery registered in the HIRA database. We calculated postoperative days using information about the surgical date. We divided patient time into three discrete categories: pre-exposure period (one year before the thyroid surgery), exposure (or risk) period, and unexposed period. The risk period of thyroidectomy exposure was divided into 8 subperiods: 1–30, 31–60, 61–90, 91–180, 181–270, 271–360, 361–450, and 451–540 days after thyroidectomy. All remaining time (outside the pre-exposure and exposure periods) was considered to be unexposed time. The date for MDD was identified as the first date of diagnosis. To ensure accurate diagnoses, we defined subjects with MDD as those who were diagnosed with MDD (F32–33) by a psychiatrist at least once in the HIRA database.
Cox proportional hazard models
We used Cox proportional hazard models to investigate the risk of MDD due to partial or total thyroidectomy, with thyroid cancer status, hypertension, diabetes, cerebrovascular disease, and ischemic heart disease as possible confounding factors (23,24). The Cox proportional hazard models were stratified according to subject age (older or younger than 50 years) and sex. According to data from the Korean National Health and Nutritional Examination Survey and a recent genome-wide association study, the mean age at onset of menopause was ∼50 years in South Korea (25,26). The outcome variable was MDD occurrence (F32–33). The other variables in the model were patient age; type of surgery (partial: P4551, P4553 vs. total: P4552, P4554, P4561); cancer status (cancer: C73, C75 vs. no cancer); and the presence of hypertension (I10–15), diabetes mellitus (E10–14), cerebrovascular disease (I60–69), or ischemic heart disease (I20–25).
Individuals who underwent partial (codes P4551, P4553) or total (codes P4552, P4554, P4561) thyroid surgery only once were included in the Cox proportional hazard models. Individuals who were diagnosed with MDD (F32–33) during the preceding year were excluded because subjects were considered as new patients with MDD. Individuals younger than 18 years were excluded from these analyses to evaluate the risk factors among adult patients only (Fig. 1b).
Statistical analysis
We determined the duration of exposure during the study period and estimated incidence rate for MDD in each of the exposure risk periods after thyroidectomy. IRRs in periods of exposure to thyroid surgery compared with unexposed periods were calculated using a conditional Poisson regression and adjusted for age and season. We estimated the MDD-adjusted IRRs and their 95% confidence intervals (CIs) for exposure overall and for each predefined exposure risk period. In addition, Cox proportional hazard models were used to calculate the risk of depression due to partial or total thyroidectomy in conjunction with various confounding factors (age, sex, type of surgery, cancer status, and other medical conditions). All tests were two-tailed with an adopted significance level (alpha) of 0.05. Analyses were performed using SAS Enterprise statistical software version 6.1 (SAS Institute, Inc., Cary, NC).
Results
Among 187,176 individuals who underwent partial or total thyroidectomy, 12,566 were diagnosed with MDD during the washout period (January 1, 2009–December 31, 2009). To include only subjects with newly developed MDD after thyroid surgery, we excluded the subjects who had been diagnosed during the washout period. After those exclusions, 16,744 patients (8.9%) were diagnosed with MDD at least once during the observation period (January 1, 2010–December 31, 2016) and included in the SCCS analyses (Fig. 1a). Of these, 3837 (22.9%) underwent partial thyroidectomy and 12,907 (77.1%) underwent total thyroidectomy. The mean (standard deviation) age at baseline was 47.5 (12.6) years for subjects undergoing partial thyroidectomy and 49.3 (12.2) years for those undergoing total thyroidectomy. Regarding sex, 3292 (85.8%) subjects undergoing partial thyroidectomy were female and 11,343 (87.9%) subjects undergoing total thyroidectomy were female (Table 1).
Patient Characteristics and Incidence of Major Depressive Disorder Among Subjects Who Underwent Partial or Total Thyroidectomy
CI, confidence interval; SD, standard deviation.
Analysis indicated an association between partial or total thyroidectomy and MDD. After adjusting for age and season, the IRRs were calculated by comparing the rate of events during periods of exposure or pre-exposure with the rate during all other observed time periods (i.e., nonexposed period). As given in Table 2, we found an increased MDD risk during the one-year period before thyroidectomy, with an IRR of 1.29 ([95% CI 1.18–1.41], p < 0.0001) for subjects with partial thyroidectomy and 1.27 ([95% CI 1.21–1.33], p < 0.0001) for subjects with total thyroidectomy. After partial thyroidectomy, the IRR increased for the first 60 days (IRR [30–60 days]: 1.68; [95% CI 1.32–2.13], p < 0.0001) and then returned to baseline levels by 271 to 360 days after the surgery (IRR 0.99; [95% CI 0.83–1.19], p = 0.932). In contrast, after total thyroidectomy, the IRR increased for the first 60 days (IRR [30–60 days]: 1.81; [95% CI 1.59–2.06], p < 0.0001) and remained elevated for 451 to 540 days after the surgery (IRR 1.11; [95% CI 1.01–1.22], p < 0.028).
Incidence Rate Ratios of Major Depressive Disorder from the Results from Self-Controlled Case Series Analysis of All Patients
We conducted SCCS analysis according to patient cancer status. In patients with cancer, we found an increased MDD risk during the one-year period before thyroidectomy, with an IRR of 1.24 ([95% CI 1.11–1.39], p = 0.0002) for subjects with partial thyroidectomy and 1.27 ([95% CI 1.21–1.34], p < 0.0001) for subjects with total thyroidectomy (Table 3). After partial thyroidectomy in patients with cancer, the IRR increased during the 30–60-day period (IRR [30–60 days]: 1.65; [95% CI 1.22–2.45], p = 0.0013) and returned to baseline levels by 271–360 days after surgery (IRR 0.96; [95% CI 0.76–1.22], p = 0.743). In contrast, after total thyroidectomy in patients with cancer, the IRR increased during the first 60 days (IRR [30–60 days]: 1.85; [95% CI 1.63–2.11], p < 0.0001) and remained elevated for 361–450 days after surgery (IRR 1.27; [95% CI 1.15–1.39], p < 0.0001). In patients without thyroid cancer, the IRR was increased only during the one-year period before partial thyroidectomy (Table 4). Compared with subjects with partial thyroidectomy, subjects with total thyroidectomy showed an increased IRR of MDD during 271–540 days postsurgery in a delayed manner (IRR [361–450 days]: 1.73; [95% CI 1.24–2.41], p = 0.0013).
Incidence Rate Ratios of Major Depressive Disorder from the Results from Self-Controlled Case Series Analysis for Patients with Cancer
Incidence Rate Ratios of Major Depressive Disorder from the Results from Self-Controlled Case Series Analysis for Patients Without Cancer
The demographic and disease prevalence data used in the additional Cox regression analyses are summarized in Table 5. After excluding subjects younger than 18 years, 174,367 subjects were included in these analyses (Fig. 1b); among them, 41,041 underwent partial thyroidectomy and 133,326 underwent total thyroidectomy.
Patient Characteristics for the Cox Proportional Hazard Models (≥18 Years Old)
After the stratified Cox regression analysis, as given in Table 6, total thyroidectomy was associated with an increased MDD hazard ratio (HR) compared with partial thyroidectomy (HR 1.40; [95% CI 1.06–1.85], p = 0.017) only in male subjects older than 50 years after adjusting for cancer status, hypertension, diabetes mellitus, cerebrovascular disease, and ischemic heart disease. No other groups (male subjects younger than 50 years or females of any age) showed any association between thyroidectomy type and MDD incidence. In subjects younger than 50 years, hypertension was associated with an increased MDD risk (HR 1.81; [95% CI 1.33–2.48], p = 0.0002 in males; and HR 1.26; [95% CI 1.06–1.49], p = 0.009 in females). In female subjects younger than 50 years, thyroid cancer and diabetes mellitus were associated with an increased MDD HR (HR 1.24; [95% CI 1.04–1.48], p = 0.018 for thyroid cancer; HR 1.58; [95% CI 1.27–1.96], p < 0.0001 for diabetes mellitus). In male subjects aged 50 years or older, thyroid cancer status was negatively associated with MDD occurrence (HR 0.62; [95% CI 0.46–0.83], p = 0.0014). In female subjects aged 50 years or older, cerebrovascular disease and ischemic heart disease were positively correlated with MDD occurrence (HR 1.45; [95% CI 1.25–1.69], p < 0.0001 for cerebrovascular disease; HR 1.23; [95% CI 1.07–1.41], p = 0.0045 for ischemic heart disease).
Hazard Ratios of Major Depressive Disorder from the Results from Cox Proportional Hazard Models Stratified by Sex and Age (≥18 Years Old)
HR, hazard ratio.
Discussion
This study shows a long-term association between the risk for MDD and thyroidectomy. To our knowledge, this study is the first to reveal an association between the type of thyroidectomy and the risk of MDD using nationwide cohort data for all patients who underwent thyroid surgery. In this study, we present three important findings. First, the incidence of MDD increased and was at its highest immediately after thyroidectomy, and the risk remained increased for a longer period in subjects who received total thyroidectomy than in those who received a partial thyroidectomy. Second, we found a different chronologic pattern for the risk of MDD after thyroid surgery depending on patient cancer status (cancer patients vs. noncancer patients). Third, total thyroidectomy was associated with increased risk for MDD, especially in male subjects aged 50 years or older.
To our knowledge, this is the first study to reveal the incidence of MDD in South Korea specifically in subjects who underwent thyroidectomy. Our demographic data are consistent with nationwide studies from other countries (27,28). This study reports a lower level of MDD incidence in patients with thyroidectomy than was found in the general population in a previously published review article (29). Considering the lower prevalence of MDD in East Asian countries (including South Korea) compared with Western countries, the incidence reported in this study might represent the real-world situation in South Korea (30).
In this study, we found an increased risk of depression before thyroidectomy in all patients. Our findings regarding cancer status are consistent with previous findings from prospective and cross-sectional studies (31,32). In their large-scale nationwide cohort study, Lu et al. found that the relative rate for depression started to increase ∼10 months before any type of cancer diagnosis (32). In their multicenter cross-sectional study, Hartung et al. investigated patients with many types of cancer and found that patients with thyroid cancer had an increased risk of depression compared with normal controls (31). Therefore, a cancer diagnosis could have affected the increased risk of MDD found in our study even before the thyroid surgery. Further study will be needed to clarify whether a diagnosis of cancer or noncancer affects the increased risk of MDD seen before thyroid surgery in different ways.
This study also reveals that the incidence of MDD increased and reached a peak during the first two months after thyroidectomy among all subjects. We are the first to report that subjects who receive a total thyroidectomy might have an increased risk of MDD for up to 270 days longer than subjects who receive a partial thyroidectomy. Because our findings might have been influenced by self-knowledge of the cancer diagnosis or the cancer diagnosis itself, we conducted two separate subanalyses by cancer status to investigate the effects of total and partial thyroidectomy on the risk of MDD (33).
In cancer patients, the risk of MDD peaked during the first two months after thyroidectomy. Consistent with our results, a nationwide matched cohort study in Sweden revealed that the relative risk for depression peaked during the first week after a cancer diagnosis (32). Also, a nationwide cohort study from England found that the suicide risk was highest in the first 6 months after a cancer diagnosis, although those researchers did not investigate the association between depression and a cancer diagnosis (34). Similar to our results, Choi et al. found that patients with thyroid cancer who underwent thyroidectomy had an increased risk of depressive disorder for up to 1 year after the operation compared with normal controls (35). Compared with cancer patients, subjects without cancer showed a different chronological pattern for the risk of depression. Even though no previous studies have investigated the association between depression and thyroid surgery, two studies have assessed QoL before and after thyroid surgery in patients with benign thyroid goiters or nontoxic nodular goiters (11,12). Contrary to our results, those two prospective studies showed improved or restored QoL after thyroidectomy (11,12). However, those studies assessed only a short period of time (up to six months after surgery). Our results imply that subjects with thyroidectomy should be monitored for a relatively long period, more than a year and a half.
The surgery itself might affect the increased risk of depression found in this study. However, because we compared the effect of partial and total thyroidectomy on depression, we tentatively conclude that total thyroidectomy influenced the risk of MDD in a more prolonged manner than partial thyroidectomy. The increased risk of MDD in the first year and a half might be caused by the fact that patients had to adjust to surgery and postoperative therapies, including radioactive iodine ablation therapy and TSH-suppressive therapies (8,9,35). Although we could not evaluate postoperative therapeutic factors, we assume that patients who received a total thyroidectomy had a higher chance of experiencing postoperative therapies and complications than those with partial thyroidectomy. Furthermore, patients with total thyroidectomy might have a higher risk of thyroid dysfunction than those who received a partial thyroidectomy. One recent investigation demonstrated an association between diminished QoL and total thyroidectomy using psychological questionnaires and functional brain imaging (7). The findings of that study suggested that thyroid hormone withdrawal after total thyroidectomy affects multiple brain areas and is associated with diminished QoL (7). Similarly, several population-based cohort studies have shown that hypothyroidism is associated with an increased risk of MDD (36 –41). However, because we did not evaluate any detailed information about thyroid function, further studies will be needed to clarify the relationship between thyroid dysfunction and the incidence of MDD in subjects who undergo partial or total thyroidectomy.
In the analyses stratified by sex and age (older and younger than 50), we found that the increased risk of MDD among subjects who underwent a total thyroidectomy compared with those who received a partial thyroidectomy applied only to male subjects aged 50 years or older. To our knowledge, no previous studies compared the risk of depression between total thyroidectomy and partial thyroidectomy depending on age group or sex. However, one previous report offered findings similar to ours: subjects with cancer aged 50 years or older were associated with a higher risk of suicide than younger cancer patients (34). Although male subjects aged 50 years or older might be vulnerable to the risk of depression due to low testosterone levels (42 –44), further studies will be needed to clarify the association between the type of surgery and risk of depression on the one hand and male hormone levels and other associated factors on the other.
This study has several strengths. First, it included the entire Korean population and used claims data for all patients who underwent partial or total thyroidectomy during the study period. Thus, our study results represent a large real-world population in South Korea. Second, we conducted SCCS analyses, which control for patient-specific measured and unmeasured confounding factors that do not vary over time. In addition, we adjusted all our analyses for time-varying confounders such as age and season. Third, we evaluated subjects with thyroidectomy during relatively long pre- and postexposure periods. This could provide new information about MDD incidence in subjects with partial or total thyroidectomy. Fourth, in the subanalyses performed using Cox proportional hazard models, we were able to investigate the risk of MDD due to partial or total thyroidectomy while controlling for possible confounding factors, including thyroid cancer status, hypertension, diabetes, cerebrovascular disease, and ischemic heart disease. Also, we could reveal differences between different sex and age groups.
This study also has several limitations. First, information might have been inaccurately coded, and records might have been incomplete. A validation study comparing diagnoses from the health insurance database with the actual diagnoses recorded in patient medical records in Korea revealed that the overall positive predictive value was ∼70% (16). Thus, the diagnostic accuracy in this study might be limited. However, there is no reason to suspect a differential rate of misclassification in the unexposed, pre-exposure, and exposure periods, so this limitation is unlikely to introduce bias into our study. Second, our database did not provide important sociodemographic risk factors for depression, including socioeconomic status, marital status, education level, and personal income. However, because we used an SCCS analysis, individual baseline risk factors do not influence our study results or conclusions. Third, due to the nature of the SCCS analysis, we could not directly compare the effects of partial versus total thyroidectomy on MDD. However, using Cox proportional hazard models, we evaluated the HR of total thyroidectomy compared with partial thyroidectomy on the incidence of MDD. Fourth, due to the lack of any sociodemographic data except age and sex in the Cox proportional hazard models, we could not find any effect of those missing factors on the risk of an MDD diagnosis. Fifth, due to lack of information about thyroid hormone status and postoperative therapy, we could not directly determine the mechanism for the increased risk of depression, especially in subjects with a total thyroidectomy. Future studies should consider information about related medical and postoperative conditions.
In conclusion, the risk of MDD appears to be the highest during the first two months after a partial or total thyroidectomy in all subjects and subjects with cancer. This study emphasizes the importance of considering regular psychiatric assessments for at least one or two years in patients who undergo partial or total thyroidectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Original Technology Research Program for Brain Science through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (Grant No. NRF-2016M3C7A1947307; PI H.J.J.) and by the Bio & Medical Technology Development Program of the NRF funded by the Korean Government, MSIP (Grant No. NRF-2017M3A9F1027323; PI H.J.J.). The Korean Ministry of Science and ICT and the NRF of Korea had no role in study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit this article for publication.