
Abstract
Background:
Exposure to moderate-to-high doses of ionizing radiation is the only established environmental risk factor for thyroid cancer and brain and central nervous system tumors. Considering the high lifetime prevalence and frequency of exposure to dental X-rays, the most common source of diagnostic radiation exposure in the general population, even a small associated increase in cancer risk would be of considerable public health importance. With the objective to inform clinical practice and guidelines, we synthesized the current epidemiological evidence on the association between dental X-rays and the risk of thyroid cancer, meningioma, and other cancers of the head and neck region.
Methods:
The Medline, Embase, and Web of Science databases were searched to identify eligible studies. Summary odds ratio/relative risk estimates and confidence intervals were extracted, and pooled risk ratios (RRs) for each cancer were calculated using random effects meta-analysis.
Results:
The literature search identified 5537 publications; of these, 26 studies including 10,868 cancer patients were included in the synthesis. The random effects meta-analyses, based on seven studies of thyroid cancer (six case/control, one cohort) and eight studies of meningioma (all case/control), showed that multiple (or repeated) exposures to dental X-rays were significantly associated with an increased risk of thyroid cancer (pooled RR = 1.87 [95% confidence interval, CI 1.11–3.15]) and meningioma (pooled RR = 1.53 [CI 1.26–1.85]). There was no association with glioma, and there were too few studies of other cancers of the head and neck region to conduct a meaningful meta-analysis.
Conclusions:
Based on a meta-analysis of retrospective case/control studies, these findings provide some support to the hypothesis that multiple (or repeated) exposures to dental X-rays may be associated with an increased risk of thyroid cancer and meningioma. These studies did not include individual organ doses and ages at exposure, and are subject to recall bias and other limitations. Furthermore, the thyroid exposure has decreased dramatically over time from the use of thyroid shields and improved technology/equipment. Prospective studies, based on dental X-ray records and patient follow-up, are needed to test the hypothesis further and clarify the possible cancer risk associated with dental radiography, as although the risk at the individual level, particularly with improved technology/equipment, is likely to be very low, the proportion of the population exposed is high. Considering that about one-third of the general population in developed countries is routinely exposed to one or more dental X-rays per year, these findings manifest the need to reduce diagnostic radiation exposure as much as possible.
Introduction
Dental X-rays constitute a common source of exposure to ionizing radiation, a known human carcinogen, in the general population. Although the dose of radiation associated with dental radiography is low, there is considered to be no threshold below which exposure to ionizing radiation is completely without risk (1), and patients are likely to be exposed to dental X-rays on multiple occasions over many years. Given this high lifetime prevalence and frequency of exposure, even a small associated increase in cancer risk would be of considerable public health importance.
Among the organs of the head and neck region, the thyroid gland is highly susceptible to radiation carcinogenesis, and exposure to high-dose ionizing radiation, particularly in childhood and adolescence, is the only established environmental cause of thyroid cancer—the anatomic position and the relatively high radiosensitivity of the thyroid gland make it an organ of great concern in dental radiography (2 –4). Evidence for the association between exposure to moderate-to-high doses of ionizing radiation and thyroid cancer has come from studies of children who had received X-ray treatment (mostly during the first half of the 1900s) for benign conditions such as enlarged tonsils or thymus gland, hemangioma, ringworm of the scalp (tinea capitis), skin disorders, and painful arthrosis and spondylosis of the cervical spine. Similar evidence has come from radiotherapy of children with cancer, where the treatment field included the thyroid.
Important additional evidence has come from the studies of survivors of the Hiroshima and Nagasaki atomic bombings of 1945 and the Chernobyl nuclear power plant accident in 1986 (2,3,5,6). An increased risk of thyroid cancer has also been observed in health professionals occupationally exposed to low-dose ionizing radiation, including dentists/dental assistants, diagnostic X-ray workers, and radiologic technologists, suggesting that multiple (or repeated) low-dose exposures in adults may also be important (7 –12). A number of studies have suggested an association between exposure to dental X-rays and the risk of thyroid cancer (13 –15), but no meta-analysis of this association has yet been conducted to summarize the pooled effect of the exposure.
In analogy with thyroid cancer, exposure to ionizing radiation is the only established environmental risk factor for brain and central nervous system (CNS) tumors. Studies of ionizing radiation include cohorts of children who received cranial radiation for treatment of tinea capitis, atomic bomb survivors, and patients with radiation exposures (diagnostic or therapeutic) in medical or occupational settings. The strongest evidence for radiation exposure and development of meningioma has come from cohorts of patients who received therapeutic radiation treatment to the head and neck region for neoplastic conditions (16,17), whereas studies of meningioma risk in atomic bomb survivors who received moderate-to-high doses of radiation (based on their distance from the hypocenter of explosion) (18,19) and dental patients who received diagnostic low-dose radiation from dental X-rays (20 –25) are less consistent.
In a recent meta-analysis including seven case/control studies, there was overall no association between exposure (ever vs. never) to dental X-rays and risk of meningioma (26). However, there was a significant increase in risk (based on two studies) with bitewing X-rays (odds ratio [OR] = 1.73 [95% confidence interval, CI 1.28–2.34]) (26). The meta-analysis examined only the effect of “ever versus never” exposures to different types of dental X-rays—the association between multiple (or repeated) dental X-ray exposures and meningioma was not investigated.
The incidence of both thyroid cancer and meningioma has increased in many countries during the past three decades (27 –32). In a recent study of cancer in adolescents in the United States, thyroid cancer was reported to have had the second largest annual increase in incidence (after non-Hodgkin's lymphoma) during the period 1975–2012 (33). Much of this increase is probably due to increased case ascertainment, particularly for thyroid cancer, but other contributing factors should be considered. Also, little is known about the impact of, or magnitude of risk associated with, dental X-rays, which have been the fastest growing source of human exposure to low-dose ionizing radiation during the past three decades (34).
To inform clinical practice and patient safety guidelines, we synthesized the published epidemiological evidence on the association between exposure to dental X-rays and the risk of thyroid cancer, meningioma, and other cancers of the head and neck region (including glioma, vestibular schwannoma, and cancers of the salivary glands, oral cavity, and larynx).
Methods
Search strategy and selection criteria
This report is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (35). The protocol was registered at the University of Sussex (
We carried out a systematic literature search of observational epidemiological studies, without language restriction, from inception up to 10 December 2018 using the electronic databases Embase (Ovid), Medline (Ovid), and Web of Science. Search terms included “dental x-ray(s),” “tooth radiography,” “teeth radiography,” “dental radiography,” “bitewing radiography,” “diagnostic x-ray(s),” “diagnostic radiography,” “ionizing radiation” AND “head,” “brain,” “neck,” “mouth,” “thyroid,” “meningioma,” “glioma,” “parotid,” “salivary gland” AND “neoplasm,” “cancer,” “carcinoma” as free text terms. The full-search strategy used for Medline in Ovid is given in Appendix Table A1. The references of all relevant full-text articles and reviews were searched manually to identify additional articles. Published case/control or cohort studies that reported the association between dental X-rays and a head or neck cancer as an OR or relative risk, or that reported sufficient information for the calculation of the OR of a head or neck cancer associated with dental X-ray exposure, were included in the synthesis.
We excluded editorials, commentaries, letters, and articles that did not contain sufficient information to calculate a risk estimate and CI. For articles that reported on the association between dental X-rays and a head or neck cancer but where insufficient information was provided to calculate the risk estimate, we first contacted the author(s) to ask if they could provide the relevant data; if this was not successful the study was included in the discussion of the results. For studies published in more than one report, the most comprehensive with the largest sample size was included in the synthesis. Two investigators independently screened the titles and abstracts of the articles retrieved from the literature search, and the full-texts of the potentially eligible articles were obtained for further assessment and final inclusion (Fig. 1).
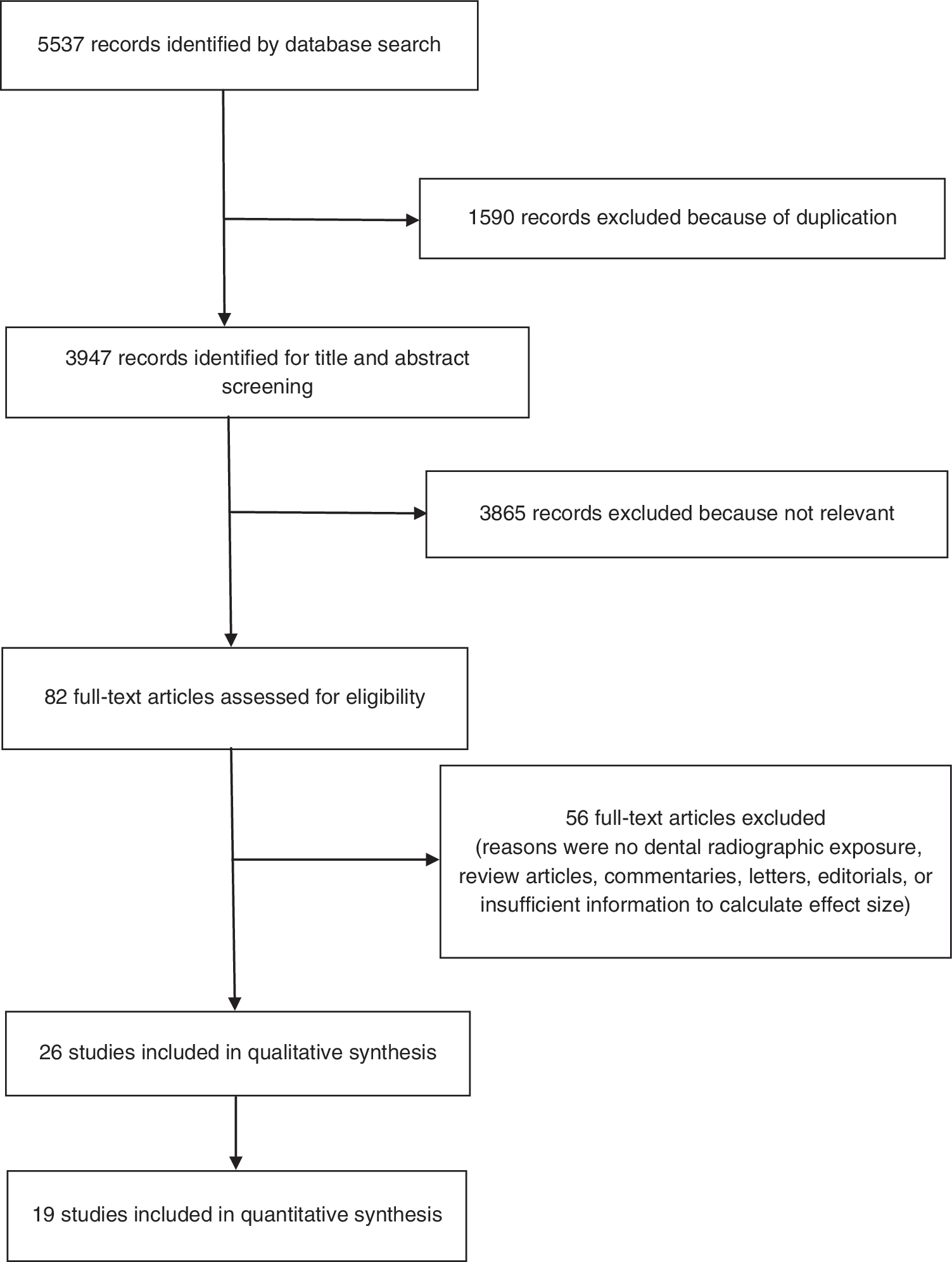
PRISMA flow diagram for study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Data extraction and analysis
Two investigators independently assessed the methodological quality of the included studies using the Newcastle/Ottawa Scale (36), which assigns scores to various aspects of case/control and cohort studies relating to selection of subjects and comparability of cases and controls and the exposed and nonexposed cohort, ascertainment of exposure and outcomes, and follow-up and nonresponse rates. Differences in scoring were resolved by discussion. Scores were summed across items to generate an overall quality score that ranged from 0 to 9. Studies were then classified as having a low (≥7), moderate (4 –6), or high (≤3) risk of bias. Of the 19 studies included in the meta-analyses, 6 scored ≥7 (good quality) and 13 scored between 4 and 6 (fair quality). Details of the scoring are given in Appendix Table A2.
The relevant data from individual studies were extracted using a preconceived and standardized data extraction form. Information extracted included the following: first author's name, year of publication, country, study design (case/control or cohort), details of cases and controls or noncases (number of subjects, year of diagnosis, age, and sex), type of dental X-ray exposure, and variables used for control of confounding (Table 1). Relevant results, including OR, relative risk, and their corresponding CI and p-values, and the number of cases and noncases exposed and not exposed to dental X-rays, were extracted. The principal summary measure extracted was the OR or relative risk of cancer among those exposed to dental X-rays compared with those not exposed, and where available, the OR or relative risk of exposures to multiple (or repeated) dental X-rays. Information on different types of dental X-rays was also extracted. Where necessary and when sufficient data were available, we estimated the ORs and CI. For studies where only the risk estimate and p-value were reported, we estimated the CI based on the p-value using the method outlined by Altman and Bland (37). Where the risk estimate for those never exposed to dental X-rays was not available, the lowest exposure category was used as the reference category.
Characteristics of Studies Included in the Systematic Review and Meta-Analyses
Mean value.
The effective sample size for dental X-ray exposure.
RR from Cox proportional hazards regression.
CI estimated.
Data for all cases (glioma, meningioma, and vestibular schwannoma, information on gender was not available for each tumor type).
Date of death due to brain cancer.
Estimated from article (43% women).
CC, case/control; CI, 95% confidence interval; CT, computed tomography; OR, odds ratio; RR, risk ratio.
The risk estimates and their corresponding CI were pooled and meta-analyses were conducted separately for studies of thyroid cancer, meningioma, and glioma. Two meta-analyses were conducted for each of these cancer outcomes, the first examining associations between any (i.e., ever vs. never) exposure to dental X-rays and cancer, and the second examining the association between multiple (or repeated), or yearly, exposures to dental X-rays and cancer. Where a risk estimate for cancer associated with exposure to more than one type of dental X-ray was presented in the article (i.e., full-mouth, bitewing, Panorex), the estimate for full-mouth X-ray was used in the meta-analysis. The standard errors (SE) used in the meta-analyses were calculated from the stated risk estimates and lower and upper limits of the CI.
Heterogeneity between studies was assessed with I2 and Cochran's Q statistics. As the included studies covered diverse populations, had a number of different ways of classifying dental X-ray exposure, and included subjects exposed to dental X-rays at different ages and different historical time points (and hence very different resultant total radiation exposure), random effects models were fitted throughout. Where the heterogeneity was below 50%, we also examined the effect of fitting a fixed effects model. We did not test for funnel plot asymmetry due to the small number of studies in each cancer outcome (<10), which would make it difficult to distinguish real asymmetry from chance (38). For each meta-analysis, we performed a sensitivity analysis to evaluate robustness and stability by sequentially omitting one study at a time and rerunning the meta-analysis. All analyses were carried out in R 3.5.0 using the metafor package (39).
Results
The systematic literature search identified 5537 records. After exclusion of duplicates, titles and abstracts of 3947 records were screened, and full-text was obtained for 82 articles. Of these, 26 were selected for inclusion in the synthesis (Fig. 1). The characteristics of these 26 studies are given in Table 1. The meta-analysis included seven studies of thyroid cancer (six case/control, one cohort), eight of meningioma (all case/control), and eight of glioma (all case/control). There were too few studies of other head or neck cancers to include in the meta-analyses: three studies examined the association with salivary gland tumors, two studies each examined the association between dental X-rays and vestibular schwannoma, and one study examined oral cancer, laryngeal cancer, and non-Hodgkin's lymphoma. The majority (n = 15) of the studies were conducted in the United States, five in Sweden, and one each in Australia, Canada, Italy, Germany, Kuwait, and Taiwan.
The association between ever exposure or multiple (or repeated) exposures to dental X-rays and thyroid cancer is shown in Figure 2. The seven studies on thyroid cancer included 78,546 individuals and 1572 cases of thyroid cancer. The random effects meta-analysis showed that exposure (ever vs. never) to dental X-rays was significantly associated with an increased risk of thyroid cancer, with a pooled risk ratio (RR) of 1.48 [CI 1.04–2.11] (I 2 = 59.5% p = 0.019). In the sensitivity analysis, where the meta-analysis was rerun repeatedly omitting one study at a time, the pooled RR varied between 1.32 [CI 0.91–1.91] on excluding the study by Memon et al. (13), and 1.72 [CI 1.24–2.39] after excluding the study by Zhang et al. (40), which also reduced the heterogeneity by the greatest amount to I 2 = 28.4% (p = 0.27).
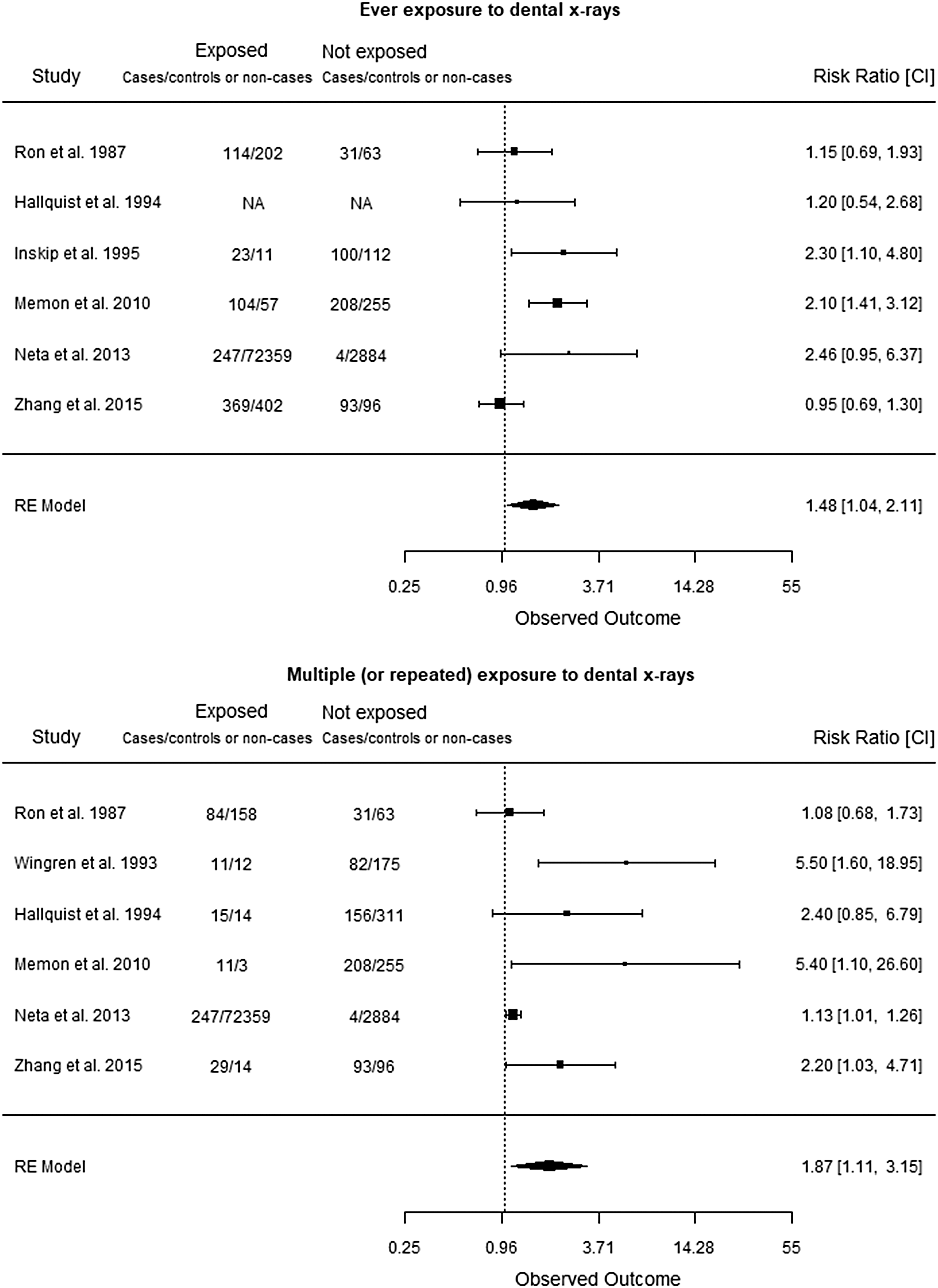
Random effects meta-analysis of the association between exposure to dental X-rays and the risk of thyroid cancer. RRs for each study are presented as squares, with the position of the square corresponding to the risk estimate and the CI shown by horizontal lines. CIs for each study shown in the forest plot are obtained by back transformation using the calculated standard error used in the analysis and do not always conform exactly to the stated CIs in the article. The area of the square is inversely proportional to the variance in the RR. The diamond represents the pooled RR and corresponding CI. Heterogeneity: I 2 = 59.5%, p = 0.019. CI, 95% confidence interval; RR, risk ratio.
There was also a significant association between multiple (or repeated) exposures to dental X-rays and the risk of thyroid cancer, with a pooled RR of 1.87 [CI 1.11–3.15] (I 2 = 72.8%, p = 0.013). The study by Neta et al. (15) reported ORs for total and papillary thyroid cancer, and Zhang et al. (40) reported ORs for total, papillary, and well-differentiated thyroid cancer. A significant association was also observed when all these ORs for all the thyroid cancer subtypes were included in the meta-analysis (pooled RR = 1.57 [CI 1.17–2.11]. In the sensitivity analysis, the pooled RR varied between 1.49 [CI 0.99–2.23], after excluding the study by Wingren et al. (41), and 2.28 [CI 1.21–4.29], after excluding the study by Neta et al. (15), which also reduced the heterogeneity by the greatest amount to I 2 = 58.3% (p = 0.04).
The association between ever exposure or multiple (or repeated) exposures to dental X-rays and meningioma is shown in Figure 3. The eight studies on meningioma included 25,440 individuals and 6166 cases of meningioma. There was no apparent association between ever being exposed to dental X-rays and meningioma (pooled RR = 1.12 [CI 0.93–1.36]), I 2 = 58.5% (p = 0.005). In the sensitivity analysis, the pooled RR varied between 1.00 [CI 0.87–1.16], on excluding the study by Lin et al. (42) (which also reduced the heterogeneity to 0%), and 1.17 [CI 0.97–1.41], after excluding the study by Preston-Martin et al. (22). However, there was a significant association between multiple (or repeated) exposures to dental X-rays and the risk of meningioma, with a pooled RR of 1.53 [CI 1.26–1.85] (I 2 = 15.1%, p = 0.355). A significantly increased risk of similar magnitude was observed when this association was examined using a fixed effects model (pooled RR = 1.55 [CI 1.34–1.80]). In the sensitivity analysis, the pooled RR varied between 1.44 [CI 1.08–1.93], on excluding the study by Lin et al. (42), and 1.64 [CI 1.40–1.93], after excluding the study by Claus et al. (43), which also reduced the heterogeneity to 0%.
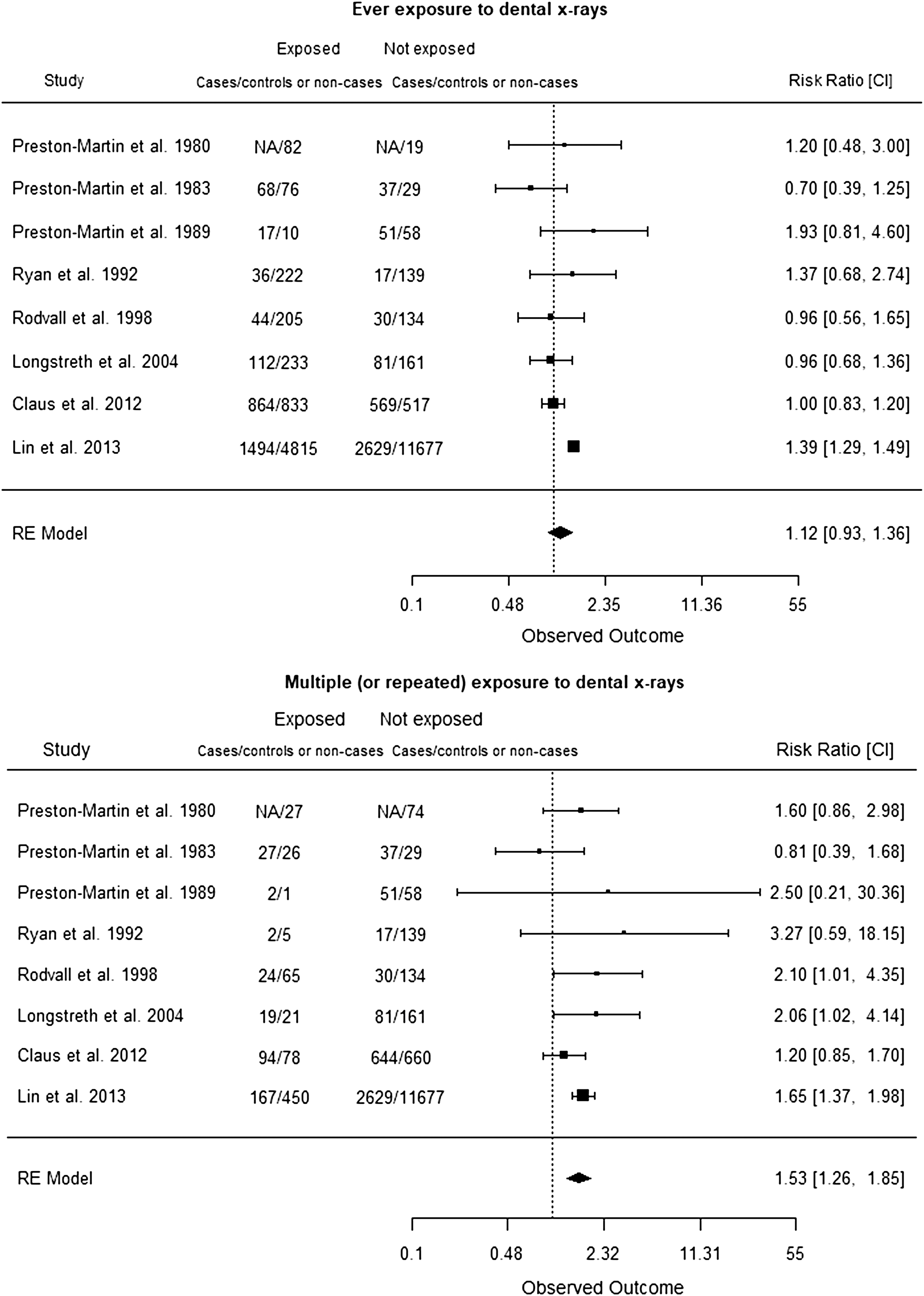
Random effects meta-analysis of the association between exposure to dental X-rays and the risk of meningioma. RRs for each study are presented as squares, with the position of the square corresponding to the risk estimate and the CI shown by horizontal lines. CIs for each study shown in the forest plot are obtained by back transformation using the calculated standard error used in the analysis and do not always conform exactly to the stated CIs in the article. The area of the square is inversely proportional to the variance in the RR. The diamond represents the pooled RR and corresponding CI. Heterogeneity: I 2 = 72.8%, p = 0.013.
The association between ever exposure or multiple (or repeated) exposures to dental X-rays and glioma is shown in Figure 4. The eight studies on glioma included 5354 individuals and 1860 cases of glioma. The random effects meta-analysis found no association between ever being exposed to dental X-rays and glioma, with a pooled RR of 0.98 [CI 0.66–1.46] (I 2 = 75.1%, p = 0.002). In the sensitivity analysis, the pooled RR varied between 0.87 [CI 0.63–1.21], after excluding the study by Neuberger et al. (44), and 1.07 [CI 0.64–1.80], on excluding the study by Ruder et al. (45), while the heterogeneity was reduced to I 2 = 54.2% (p = 0.011) after excluding the study by Ryan et al. (24). There was also no association between multiple (or repeated) exposures to dental X-rays and glioma, with a pooled RR of 0.97 [CI 0.64–1.49] (I 2 = 20.0%, p = 0.171). In the sensitivity analysis, the pooled RR varied between 0.86 [CI 0.60–1.24], after excluding the study by Ryan et al. (24), which also reduced the heterogeneity to I 2 = 0.002% (p = 0.321), and 1.24 [CI 0.66–2.33], after excluding the study by Davis et al. (46).
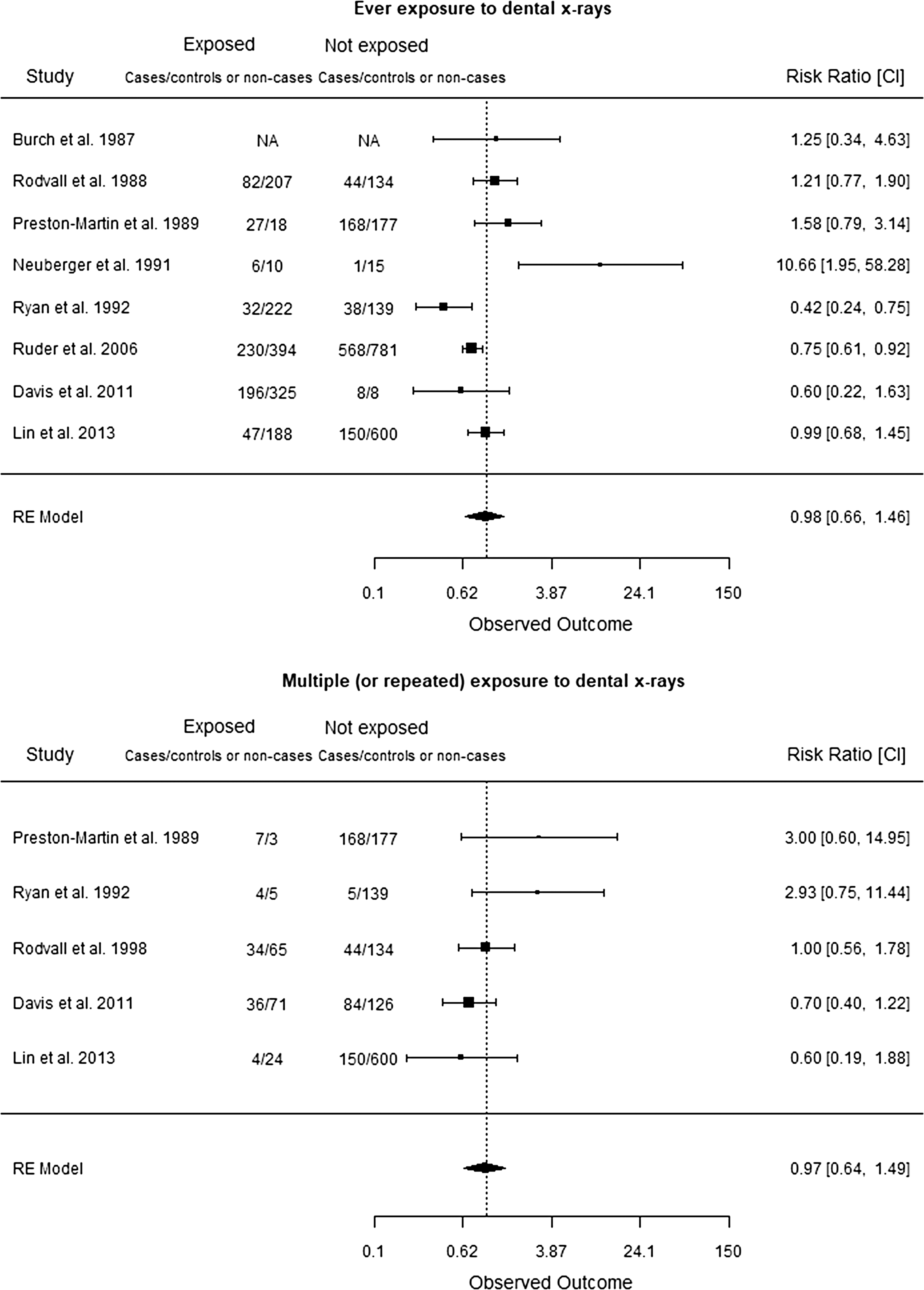
Random effect meta-analysis of the association between exposure to dental X-rays and the risk of glioma. RRs for each study are presented as squares, with the position of the square corresponding to the risk estimate and the CI shown by horizontal lines. CIs for each study shown in the forest plot are obtained by back transformation using the calculated standard error used in the analysis and do not always conform exactly to the stated CIs in the article. The area of the square is inversely proportional to the variance in the RR. The diamond represents the pooled RR and corresponding CI. Heterogeneity: I 2 = 58.5%, p = 0.005.
The two studies that examined associations between dental X-rays and vestibular schwannoma had inconsistent findings. Han et al. (47) found a positive association between ever being exposed and multiple (or repeated) exposures to dental X-rays and vestibular schwannoma, whereas Rodvall et al. (25) did not find an association. As for the other organs in the head and neck region, there was no association between dental X-rays and cancers of the salivary glands, oral cavity, or larynx (Table 1). In one study, there was some indication of increased risk of salivary gland cancer with multiple (4+) full-mouth series dental X-rays (48); whereas in another study, there was increased risk of laryngeal cancer in heavy smokers who had had multiple (5+) dental X-rays (49).
Discussion
In this most comprehensive and up-to-date synthesis of published epidemiological evidence, including 113,007 individuals and 10,969 cases of cancer of the head and neck region, multiple (or repeated) exposures to dental X-rays were significantly associated with an increased risk of thyroid cancer (pooled RR = 1.87 [CI 1.11–3.15] and meningioma (pooled RR = 1.53 [CI 1.26–1.85]).
For the general population, medical diagnostic X-rays of the head and neck region, particularly dental X-rays, are an important source of low-dose ionizing radiation. The anatomic position and relatively high radiosensitivity of the thyroid gland and meninges make these organs a concern in dental radiography. It has been hypothesized that low-dose ionizing radiation used in dental radiography may induce DNA damage that can result in cancer (50). It is generally accepted that the likelihood of developing cancer increases linearly with radiation dose, and that there is no real threshold level of radiation exposure below which carcinogenesis does not occur (51). This is also consistent with the results of recent studies that have found associations between other diagnostic X-ray procedures and the risk of thyroid cancer (40,52), and with a pooled analysis of cohort studies of subjects exposed to low-dose radiation in childhood, which found a linear association between radiation dose and subsequent thyroid cancer risk (53).
Considering the steady increase in the incidence of thyroid cancer and meningioma in many countries during the past three decades, exposure to ionizing radiation (particularly in childhood and adolescence) being the only established environmental cause of thyroid cancer, strong and consistent evidence linking increased risk of meningioma with exposure to ionizing radiation, and the relatively high lifetime prevalence and frequency of multiple (or repeated) exposures to dental X-rays in the general population, even a small increase in risk due to low-dose ionizing radiation is of great public health importance.
Clinical guidelines and the International Commission on Radiological Protection recommend that X-rays should only be prescribed if the clinical benefit to the patient warrants the risk associated with radiation exposure (54). A recent study that examined 1.3 million treatment claims by National Health Service (NHS) dentists in Scotland reported that there are significant increases in the prescription of X-rays when dentists receive fee-for-service rather than salary payments and when patients are made exempt from payment for dental treatment (55).
Exposure to moderate-to-high dose ionizing radiation is the only established environmental risk factor for tumors of the brain and CNS. However, it is not clear whether this association differs according to the type of brain and CNS tumor, age at exposure, or dose and frequency of exposure to ionizing radiation. In our synthesis, multiple (or repeated) exposures to dental X-rays were associated with a significantly increased risk of meningioma, and there was no association with glioma. This finding is consistent with earlier studies of increased risk of meningioma in patients exposed to diagnostic (including computerized tomography scans) or therapeutic radiation (52,56,57), and with a recent systematic review of epidemiological studies of ionizing radiation and the risk of brain and CNS tumors that found that ionizing radiation was more strongly associated with risk of meningioma compared with glioma (58). It is noteworthy that meningiomas are usually slow growing tumors and the vast majority (>90%) are histologically benign.
A limitation of this synthesis is that it is based on a relatively small number of published epidemiological studies (thyroid cancer: six case/control, one cohort; meningioma: eight case/control studies). There was relatively high heterogeneity in some of the meta-analyses, notably for multiple (or repeated) dental X-ray exposures and risk of thyroid cancer, which may reflect factors such as variation in the age at exposure and in the total radiation dose received. However, in the sensitivity analysis, there was no material change in the pooled risk estimates when any particular study(s) was excluded. Although case/control design is probably the most suitable (and feasible) to test this hypothesis, the study design can be subject to a number of potential biases, including issues of case and control ascertainment, selection bias, and recall and information bias between cases and controls. There is also the possibility of confounding due to the absence of information on potential confounding factors. The large majority of thyroid cancer studies, in the meta-analysis, adjusted for the potential confounding factors, including radiation exposures other than dental X-rays (13,15,40,41,59) (Table 1).
In addition, meta-analyses can be subject to publication bias—the propensity to publish “positive” findings. It is therefore not possible to estimate the impact of this potential bias. In all but one study (42) (which used medical insurance claims records) included in this synthesis, self-reported information on past exposure(s) to dental X-rays was collected via questionnaires and/or interviews.
It is noteworthy that unlike general/family practice or hospital records, which are available for most populations in developed countries and usually follow the patient when they move residence or register with another doctor, comprehensive long-term dental X-ray records are usually not maintained at most dental clinics and usually do not follow the patient. Considering the unavailability of comprehensive historical dental X-ray records (i.e., age at exposure(s), type of X-ray, number of X-rays), it has not been possible to conduct studies based on dental X-ray records. In an unrelated dental X-ray validation study, which compared information from patient interviews (self-report) and dental records, recall was found to be unbiased since the measures of agreement between self-report and dental record data were similar for cases and controls. The authors concluded that interview data alone may be used for case/control comparisons of dental X-ray exposure(s), and would, because of unbiased misclassification, tend to underestimate the relative risks (21,60). As in most interview-based case/control studies, a general recall bias must be considered. However, this is unlikely to wholly account for the significant dose/response pattern and the consistently increased risk associated with dental X-ray exposure on stratifying the analysis by various potential confounders (such as age, sex, education, nationality, or number of live births) found by Memon et al. (13).
There are two main types of dental X-rays: intraoral (the X-ray film is inside the mouth) and extraoral (the X-ray film is outside the mouth). Intraoral X-rays, which are the most common type of dental X-ray, include bitewing, periapical, and occlusal X-rays; extraoral X-rays include panoramic X-rays, tomograms, cephalometric projections, dental computed tomography (CT), cone-beam CT, and digital imaging. It is noteworthy that the effective radiation dose to the patient varies considerably within and between these procedures depending on how many images are taken, exposure settings on X-ray machines, and the particular type and age of machine used. It has been estimated that the radiation dose may vary between 1 and 20 μSv for intraoral radiography, 4–30 μSv for panoramic radiography, and from less than 100 to 700 μSv for dental CT (61). It is generally considered that the doses received by patients historically from dental radiography were considerably higher (62), and that average patient doses have continued to decrease in intraoral radiography due to increasing use of digital imaging (63). It is anticipated that with newer generation digital imaging systems, which utilize very short exposure times, patient doses will gradually also decrease in panoramic radiography (63).
In a recent study, Chang et al. (64) summarized and compared estimates of absorbed radiation dose by the thyroid in patients who underwent diagnostic radiographic examinations during the years 1930–2010. It was estimated that the thyroid doses from dental radiography decreased markedly throughout the decades, from an average of 390 mGy for a full-mouth series in the 1930s to an average of 0.31 mGy at present. However, the authors noted that the present-day modern dental radiography (without the use of thyroid shield) results in thyroid doses of a few hundredths of mGy to a few tenths of mGy, depending on the type of dental X-ray; and that dose to the thyroid from dental radiography has been relatively constant since the 1980s. It can be inferred that since the 1930s there has been a gradual decline in radiation dose to the thyroid, which was followed by a stabilization of the dose from the 1980s onward. On the contrary, the number of dental radiographic examinations increased significantly since the 1980s. For example, in the United States, the estimated number of dental radiographic examinations (i.e., bitewing exposures) increased from 101 million in 1980–81 to 500 million in 2006 (65).
Considering the different types of dental X-rays and X-ray machines (with varying radiation doses) and periodic frequency of exposures, it has been difficult to determine or estimate lifetime radiation dose received by the patients. For patient safety in clinical practice, it is the age at exposure, frequency, lifetime prevalence, and thyroid shielding that are most important. Recent studies suggest that thyroid shields can reduce the radiation dose by 50% from panoramic X-rays (66) and by 70–75% from upper anterior dental X-rays (67). Other studies have reported a statistically significant reduction in radiation dose from cone-beam CT with thyroid shielding (68,69). Current U.K., European, and U.S. guidelines stress the need for thyroid shielding during dental radiography (70 –72).
For the general population, dental X-rays are the most common (and the fastest growing) source of medical low-dose ionizing radiation exposure. The Health Protection Agency has estimated that 20.5 million dental radiographs are taken per year in general dental practice in the United Kingdom, suggesting that as much as one-third of the general population may be routinely exposed to one or more dental X-rays per year (73). Although they are an important part of clinical assessment of patients, ionizing radiation is a known human carcinogen and there is no threshold below which the radiation exposure is completely without risk. In this context, the linear nonthreshold hypothesis (when applied at the population level) suggests that the likelihood of developing cancer increases linearly with radiation dose, and there is as such no threshold below which carcinogenesis does not occur (51). A recent review of the epidemiological evidence on radiation expose and cancer risk supported the continued use of the linear no-threshold model for the purpose of radiation protection, although the authors acknowledged that the possible risk associated with very low doses of radiation is small and uncertain (1). In a pooled analysis of nine cohort studies of childhood low-dose radiation exposures (including children who received therapeutic radiation for cancer/benign diseases and survivors of the atomic bombing in Japan), the authors concluded that their analyses reaffirmed the linearity of the dose/response relationship between low-dose radiation exposure and thyroid cancer (53). Studies of U.S. radiologic technologists have shown that cumulative radiation exposure from routine medical X-ray examinations is associated independently with increased chromosomal damage and number of chromosome translocations, which are established radiation biomarkers and a possible intermediary, suggesting the possibility of elevated long-term cancer risk (74,75).
In conclusion, this synthesis of published epidemiological evidence provides some support to the hypothesis that multiple (or repeated) exposures to low-dose ionizing radiation through dental X-rays may be associated with an increased risk of developing thyroid cancer and meningioma.
The public health and clinical implications of these findings are particularly relevant in light of (i) the reports of an increasing incidence of thyroid cancer and meningioma in many countries during the past three decades, (ii) the relatively high lifetime prevalence and frequency of exposure to dental X-rays in the general population, (iii) the increasing number of children and adolescents undergoing orthodontic treatment, (iv) the concern that like chest (or other upper body) X-rays, dental X-rays should only be prescribed when the patient has a specific clinical need, (v) the lack of evidence for clinical benefit of prescribing dental X-rays as a necessary part of evaluation for new patients, for routine checkup, or for periodic screening for dental caries/decay in children, and (vi) discussions in the literature questioning the adequacy of dentists'/orthodontists' full appreciation (or lack of knowledge) of issues associated with the routine prescription of dental radiography and radiation protection for patients (76 –78). Recommendations by the American Dental Association, American Thyroid Association, and the European Commission stress the need to shield the thyroid gland during dental X-ray examination (66,79 –81).
The notion that low-dose radiation exposure through dental radiography, which is the most common medical radiation exposure in the general population, is completely without risk needs to be investigated further, as although the individual risk, particularly with modern equipment, is likely to be very low, the proportion of the population exposed is high. Prospective studies, based on dental X-ray records and patient follow-up, are needed to test the hypothesis further and clarify the plausible cancer risk associated with dental radiography.
Contributors
A.M. conceived and designed the study. I.R., P.P., and J.S. did the literature search and quality assessment of included studies. I.R. and J.S. selected the studies and extracted the relevant information. I.R., J.S., and A.M. synthesized the data. A.M. and I.R. wrote the article. All authors approved the final version of the article for publication. A.M. guided and supervised the overall work.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Newcastle/Ottawa Quality Assessment of Included Studies
| Case/control studies | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study | Is case definition adequate? | Representativeness of the cases | Selection of controls | Definition of controls | Comparability of cases and controls | Ascertainment of exposure | Same ascertainment method for cases and controls | Nonresponse rate same for both groups |
| Burch et al. (85) | * | * | ** | * | ||||
| Claus et al. (43) | * | * | * | ** | * | |||
| Davis et al. (46) | * | * | * | ** | * | |||
| Hallquist et al. (82) | * | * | * | ** | * | * | ||
| Inskip et al. (14) | * | * | * | ** | * | |||
| Lin et al. (42) | * | * | * | ** | * | * | * | |
| Longstreth et al. (84) | * | * | * | ** | * | |||
| Memon et al. (13) | * | * | ** | * | * | |||
| Neuberger et al. (44) | * | ** | * | |||||
| Preston-Martin et al. (23) | * | * | * | ** | * | |||
| Preston-Martin et al. (22) | * | * | ** | * | ||||
| Preston-Martin et al. (83) | * | * | ** | * | ||||
| Rodvall et al. (25) | * | * | * | ** | * | * | ||
| Ron et al. (59) | * | * | * | * | ** | * | ||
| Ruder et al. (45) | * | * | * | * | ** | * | ||
| Ryan et al. (24) | * | * | * | ** | * | |||
| Wingren et al. (41) | * | * | ** | * | ||||
| Zhang et al. (40) | * | * | * | * | ** | * | * | |
| Cohort studies | ||||||||
| Study | Representativeness of exposed cohort | Selection of nonexposed cohort | Ascertainment of exposures | Demonstration that outcome of interest not present at start of study | Comparability of cohorts | Assessment of outcome | Was follow-up long enough? | Adequacy of follow-up of cohorts |
| Neta et al. (15) | * | * | ** | * | * | |||
The Newcastle/Ottawa Scale evaluates case/control and cohort studies across three parameters (selection, comparability, and outcome). Eight specific items are assessed, for each of which a study can score either 0 or 1 point, with the exception of comparability, which can score up to 2 points. An asterisk in the table indicates that the article scored a point for the specified item.