
Abstract
Background:
Subclinical thyroid disease occurs in approximately 5–8% of all pregnancies and is associated with a higher risk of adverse outcomes such as miscarriage, preterm birth, and suboptimal child neurodevelopment. It is generally assumed that subclinical thyroid disease that persists from early to late pregnancy is associated with a higher risk of adverse outcomes than transient disease. However, it is unknown as to what percentage of women with subclinical disease during early pregnancy have persistent disease in the third trimester.
Methods:
This study comprised 42,492 mothers for whom early and late pregnancy thyrotropin (TSH), free thyroxine (fT4), triiodothyronine (T3), or TPOAbs were available and who did not receive thyroid treatment before or during pregnancy. We adjusted for potential confounders, including maternal age, parity, anthropometrics, and β-hCG concentrations.
Results:
Subclinical hypothyroidism and hypothyroxinemia persisted in 24.8% and 17.7% of cases. Overt hyperthyroidism persisted in 8.4% of cases while subclinical hyperthyroidism persisted in 20.9% of cases. Low T3 persisted in 43.4% of cases while elevated T3 persisted in 15.7% of cases. TPOAb positivity persisted in 84.0% of cases. In women with subclinical hypothyroidism, a TSH below ∼5 mU/L at the time of diagnosis was associated with an up to 50% lower risk of persistency. The fT4 concentration at diagnosis predicted hyperthyroidism persistency and TPOAb positivity predicted persistency of all disease entities.
Conclusions:
Early pregnancy thyroid disease only persists until the third trimester in 8.4–24.8% of cases when left untreated. The main predictor for persistency is TPOAb positivity, with TPOAb-positive women having a lower risk that subclinical hypothyroidism or hypothyroxinemia persists, but a higher risk that (subclinical) hyperthyroidism persists.
Introduction
Overt maternal thyroid disease occurs in roughly 0.5% of all pregnancies and is a well-known risk factor for various adverse pregnancy and child outcomes such as pre-eclampsia, premature delivery and suboptimal child neurocognitive development (1). Subclinical thyroid disease is mostly a biochemical diagnosis of thyroid dysfunction that occurs in approximately 5–8% of all pregnancies. Recent studies show that subclinical thyroid disease, such as subclinical hypothyroidism and isolated hypothyroxinemia, is associated with a higher risk of adverse outcomes similar to those reported for overt hypothyroidism (1 –4). The majority of studies in this field focus on the first half of pregnancy. During this period, thyroid hormone regulates metabolic adaptations related to pregnancy, and fetal thyroid hormone availability depends on the placental transfer of maternal thyroid hormone. However, data on intra-individual changes in thyroid function throughout pregnancy are lacking due to this focus on early pregnancy. Moreover, we lack knowledge on the natural course of subclinical thyroid dysfunction between the first and third trimester as well as reliable thyroid function reference ranges during the third trimester.
Additional knowledge on the natural course of gestational thyroid dysfunction is crucial for improving the clinical interpretation of thyroid function tests during pregnancy. It is currently unknown as to what percentage of women with thyroid dysfunction during early pregnancy have persistent dysfunction in the third trimester. This is important because women with transient thyroid dysfunction could differ in the risk of adverse clinical outcomes and response to thyroid hormone therapy than women with persistent disease. Identification of women with persistent disease and quantification of its risk factors can improve future studies on the consequences of persistent and transient dysfunction, as well as the relevance of third trimester thyroid (dys)function and the risk of adverse pregnancy and child outcomes.
Therefore, the aim of this study was to investigate the changes in thyroid function and TPOAbs from the first to the third trimester, and to investigate how many women with thyroid dysfunction during early pregnancy have persistent dysfunction through the third trimester. Further, we aimed at identifying determinants of the change in thyroid function and TPOAbs between the first and third trimester and at establishing thyroid function reference ranges for both time points.
Materials and Methods
Patient enrollment
This study was performed in the International Peace Maternity and Child Health Hospital (IPMCH), a large community hospital providing secondary and tertiary care in Shanghai, China. All women presenting underwent first trimester screening as part of a standard work-up in the hospital between January 2013 and December 2016. A total of 52,027 women were enrolled, all of whom had either thyrotropin (TSH), free thyroxine (fT4), triiodothyronine (T3), or TPOAb concentrations available measured at first presentation (weeks 8–14) or during the late pregnancy follow-up visit (weeks 30–35). Women who underwent in vitro fertilization, who had a twin pregnancy, fetal loss, or a history of thyroid disease or thyroid medication use at the beginning of pregnancy were excluded. In addition, some women were treated with thyroid (interfering) medication based on their thyroid function test in early pregnancy at the discretion of the attending physician; these women were excluded for analyses on persistency. We performed sensitivity analyses to assess differences between treated and untreated women for each disease entity to identify and quantify potential bias. The project was approved by the Ethics Committee of IPMCH (No. GKLW2012-49).
Data collection
During the hospital visit, all data were prospectively collected by nurses, residents, and gynecologists with use of the electronic patient files. Fasting blood samples were drawn from the median cubital vein, and the serum was separated by centrifugation within 6 hours. TSH, fT4, T3, and TPOAb concentrations were measured by using the Architect i2000 immunoassay (Abbott, Chicago, IL) according to the manufacturer's protocol during the full length of data collection. TPOAbs ≥6 IU/mL were considered as positive. Measurements for T3 were only performed in a subset of 9975 women who presented during 2015. β-hCG was measured in serum by using a solid-phase two-site chemiluminescent immunometric assay on an Immulite 2000 XPi system (Siemens Healthcare Diagnostics, Deerfield, IL) from January 2015 to December 2016 and was available in a subset of 29,453 women. We did not collect data on thyroid interfering medications other than thyroid hormone supplements or antithyroid drugs. Data on maternal age, parity, education level, and last menstrual period (LMP) were collected via interviews at first clinical presentation during which height and weight also were measured to calculate body mass index (BMI). Less than 0.1% of all women smoked or consumed alcohol.
Statistical analyses
After the previously mentioned exclusions, and additional exclusion of TPOAb positive women, reference ranges for TSH, fT4, and T3 were calculated as the 2.5th and 97.5th percentile. According to these percentile cut-offs, we defined overt hypothyroidism as a high (>97.5th population percentile) TSH with a low (<2.5th population percentile) fT4, subclinical hypothyroidism as a high TSH with a normal (2.5th to 97.5th population percentile) fT4, hypothyroxinemia as a low fT4 with a normal TSH, overt hyperthyroidism as a low TSH with a high fT4, and subclinical hyperthyroidism as a low TSH with a normal fT4. We used linear regression models to study the association of TSH, fT4, T3, or TPOAb concentrations in early pregnancy with those in the third trimester, and to study the association of potential determinants of the change in TSH, fT4, T3, and TPOAb concentrations between the first and third trimester. Model assumptions were checked with residual plots, outlier exclusions and by utilizing three to five restricted cubic splines to assess nonlinearity. For variables with missing data, multiple imputation according to the Markov chain Monte Carlo method was used by creating five imputed datasets for analyses. The imputation model included maternal BMI (missing in 1.5%) and LMP (missing in 3.1%). Further, we added covariates without missing data to the model as prediction variables only (maternal age, gestational age, education, marital status, parity, TSH, fT4, total T3, and TPOAb concentrations). No significant differences in descriptive characteristics were found between the original and imputed datasets. All statistical analyses were performed by using R statistical software v3.03 (package rms, visreg) or Statistical Package of Social Sciences v20.0 for Windows (SPSS v22.0; IBM Corp., Armonk, NY).
Results
After exclusions, the final study population comprised 46,186 pregnant women, of whom 42,492 women had at least one repeated measurement available (Fig. 1). The study population had a median (95% range) age of 30 years, BMI of 20.8 (17.1–26.7) kg/m2, and 24,245 women were pregnant of a male fetus (52.5%; Table 1). Sensitivity analyses on treated individuals showed that 0.3–13.6% of all women with thyroid disease during early pregnancy (for subclinical hyperthyroidism and subclinical hypothyroidism, respectively) were treated (Supplementary Table S1). For women with subclinical hypothyroidism in early pregnancy, those who received treatment had a higher median TSH (4.16 vs. 4.75 mU/L) and were more often TPOAb positive (23.4% vs. 53.4%; Supplementary Table S1).
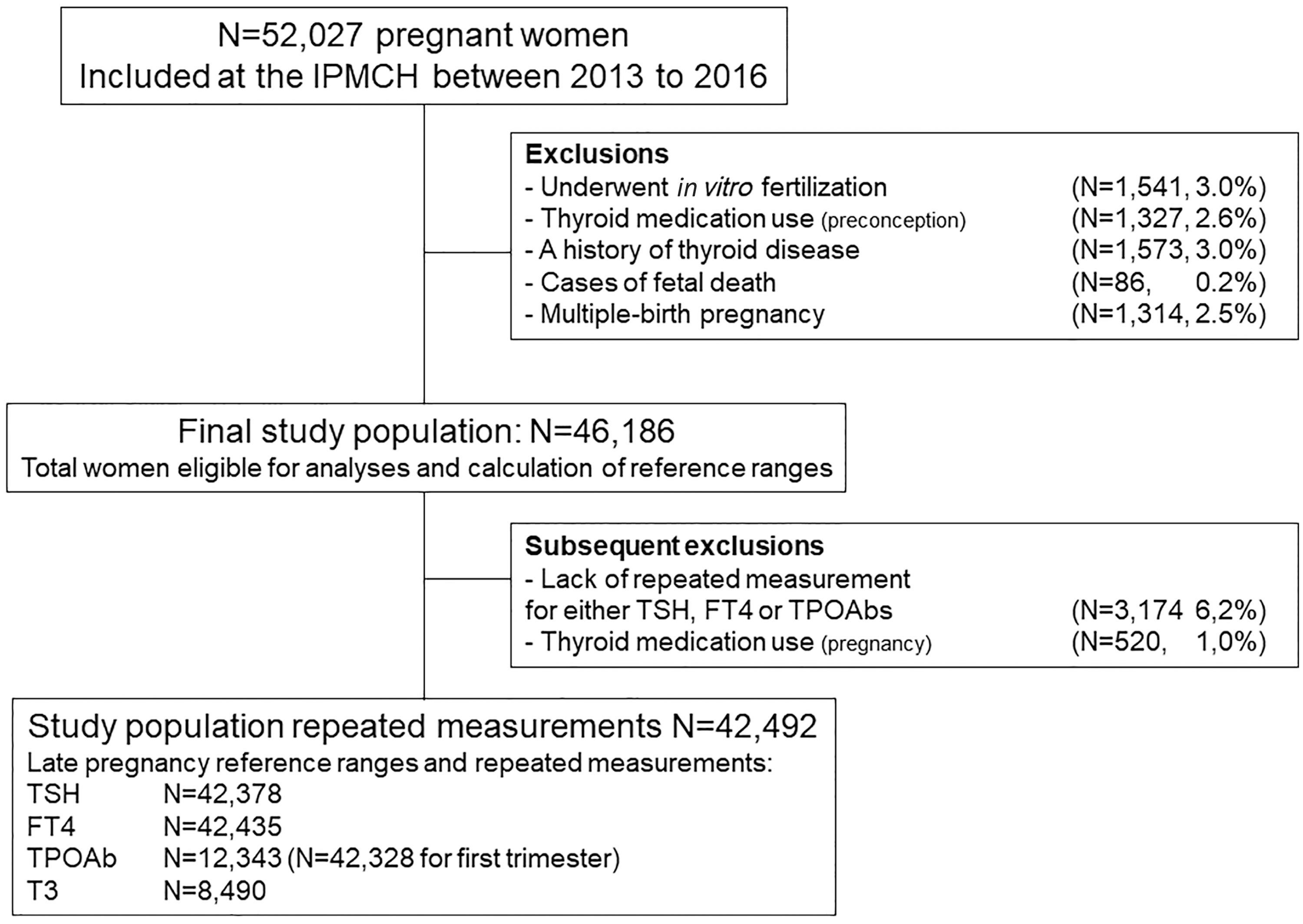
Flowchart illustrating study population selection and data availability.
Population Characteristics
BMI, body mass index; fT4, free thyroxine; LGA, large for gestational age; SGA, small for gestational age; T3, triiodothyronine; TSH, thyrotropin.
Reference ranges and natural course
The reference range for TSH in early pregnancy was 0.03–3.60 mU/L, and in the third trimester it was 0.39–3.69 mU/L (Table 2). The reference range for fT4 in early pregnancy was 11.7–19.8 pmol/L, and in the third trimester it was 9.1–14.4 pmol/L (Table 2). The reference range for T3 in early pregnancy was 1.6–3.1 nmol/L, and in the third trimester it was 1.4–2.8 nmol/L (Table 2).
Population-Based Reference Ranges for Thyrotropin, Free Thyroxine, and Triiodothyronine
Table shows the reference ranges for TSH, fT4, and T3 during early pregnancy and during the third trimester calculated as the 2.5th and 97.5th percentiles after exclusion of women who underwent in vitro fertilization, who had a twin pregnancy, had a history of thyroid disease, and used thyroid interfering medication (before pregnancy excluded for early pregnancy, additional exclusion of women who started during pregnancy for late pregnancy) and TPOAb-positive women.
Out of the 107 women with overt hypothyroidism, as defined by population-based reference ranges (instead of a TSH upper limit of 4.00 mU/L used in China at the time of data collection), 43 women were treated (Supplementary Table S1). Out of the 64 remaining non-treated women with overt hypothyroidism, 2 (3.1%) were hypothyroid and 13 (21.0%) were subclinically hypothyroid in late pregnancy. Out of all women with subclinical hypothyroidism during early pregnancy, subclinical hypothyroidism persisted into the third trimester in 24.8% of cases (Table 3). Isolated hypothyroxinemia during early pregnancy persisted into the third trimester in 17.7% of cases. Overt hyperthyroidism in early pregnancy persisted into the third trimester for 8.4% of cases, while subclinical hyperthyroidism in early pregnancy persisted into the third trimester for 20.9% of cases. A low T3 during early pregnancy persisted into the third trimester in 43.4% of cases while an elevated T3 in early pregnancy persisted into the third trimester in 15.7% of cases. In contrast, TPOAb positivity during early pregnancy persisted into the third trimester for 84.0% of cases. The thyroid function changes between early and late pregnancy for women who had a nonpersisting abnormal thyroid function test are shown in Supplementary Table S2.
Persistency of Thyroid Disease Entities from Early to Late Pregnancy
Table shows the number of women with (subclinical) thyroid disease during early pregnancy, and the number (percentage) of those women who still had (subclinical) thyroid disease during late pregnancy after exclusion of women who underwent in vitro fertilization, had a twin pregnancy, had a history of thyroid disease, or used thyroid interfering medication.
The median (95% range) change between the first and third trimester was for TSH +25.6% (+0.3 mU/L [−1.36 to +1.78]), for fT4 − 22.9% (−3.3 pmol/L [−7.6 to -0.3]), for T3 − 9.1% (−0.20 nmol/L [−0.9 to +0.4]), and for TPOAbs −67.4% (−39 IU/L [−1.7 to −514]; in TPOAb-positive women only, data not shown). We subsequently plotted the association of first trimester thyroid function with third trimester thyroid function against a 1:1 association (Fig. 2, black dotted line). We identified a pattern that was at least partly reflective of regression to the mean, with an increase for low concentrations and a decrease for higher concentrations on second measurement, for TSH, fT4, and T3. For women with a TSH <2.5 mU/L in early pregnancy, the TSH on average increased between the first and third trimester; for women with a TSH >2.5 mU/L in early pregnancy, the TSH decreased between the first and third trimester (Fig. 2). Both fT4 and T3 decreased between the first and third trimester; however, this difference was much larger for those with an fT4 or T3 below the median than those above the median in early pregnancy (Fig. 2).
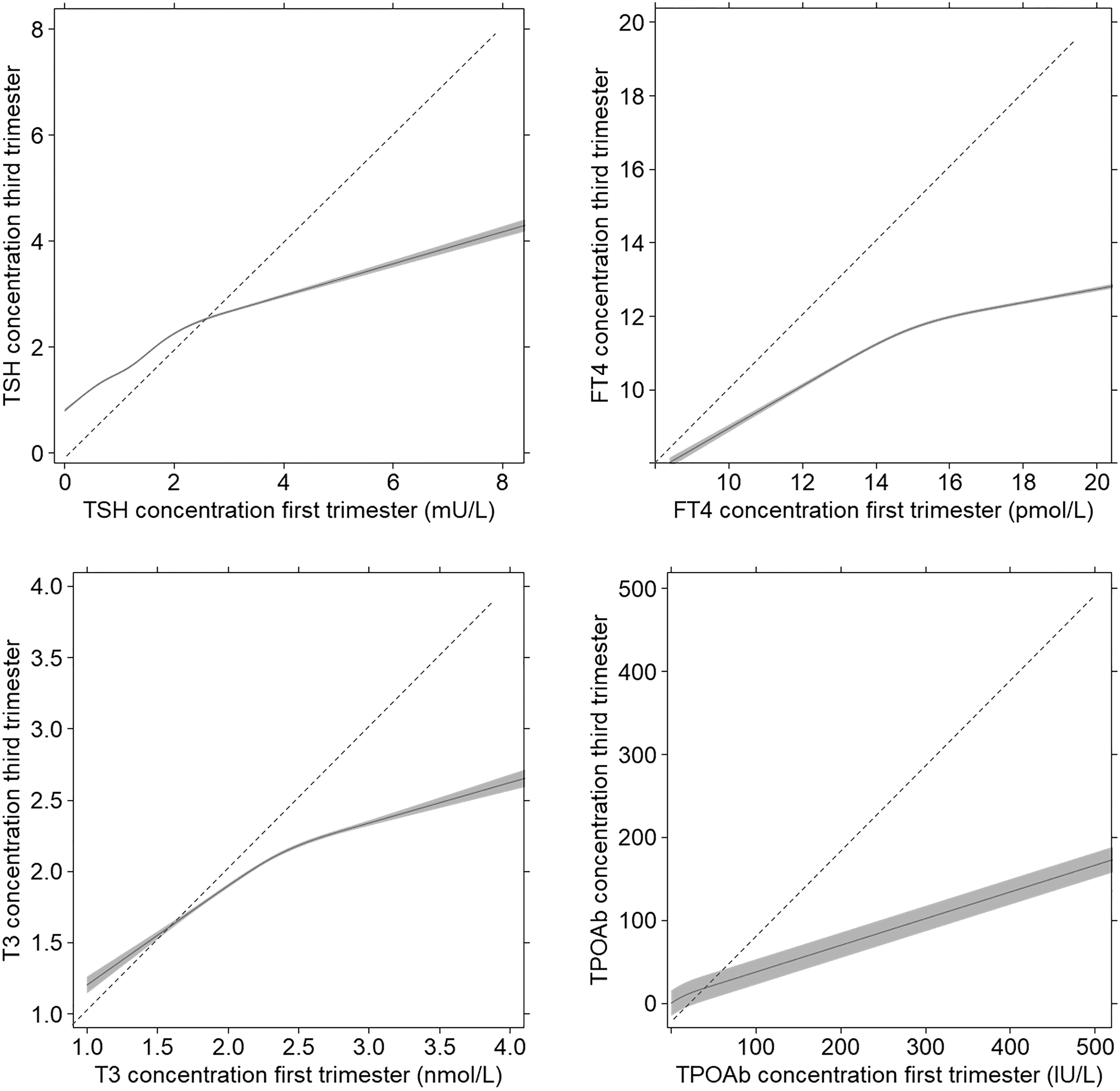
The association of first trimester with third trimester thyroid function measurements. Figure shows the association of early pregnancy TSH, fT4, T3, or TPOAb concentrations (9–14 weeks) with the corresponding concentrations measured during late pregnancy (32–36 weeks) as the predicted mean (black line) and 95% confidence interval (gray area). The dotted black line indicates a hypothetical 1:1 association. fT4, free thyroxine; T3, triiodothyronine; TSH, thyrotropin.
Determinants of persistency and thyroid function changes
We subsequently investigated whether the TSH, fT4, and TPOAb status or other thyroid function-related measurements at the time of diagnosis of thyroid disease during early pregnancy would be predictive of persistency of disease during later pregnancy. In women with subclinical hypothyroidism, a TSH below roughly 5 mU/L at the time of diagnosis was associated with an up to 50% lower risk of persistency while TPOAb positivity at the time of diagnosis was associated with a 77% lower risk of persistency (Fig. 3).
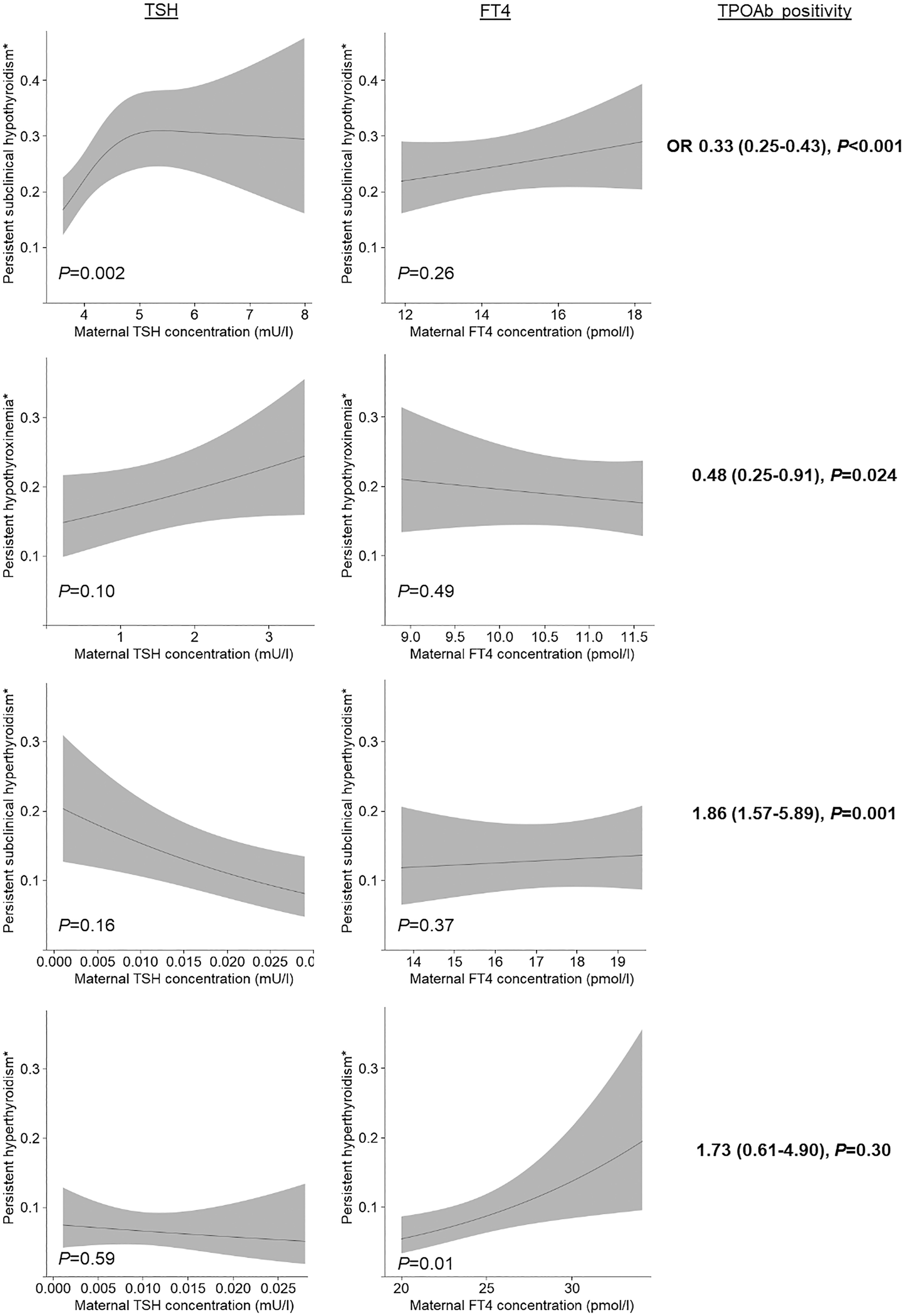
The association of TSH, fT4, and TPOAb positivity at the time of diagnosis with persistent gestational thyroid disease. Figures show the association of early pregnancy TSH or fT4 with the risk of persistent (subclinical) thyroid disease as predicted mean (black line) with 95% confidence interval (gray area); the right column shows the risk of persistent disease for TPOAb-positive women as an odds ratio and 95% confidence interval.
In women with isolated hypothyroxinemia, neither the TSH nor fT4 concentration at the time of diagnosis was associated with a higher risk of persistency, but TPOAb positivity at the time of diagnosis was associated with a 52% lower risk of persistency (Fig. 3). In women with subclinical hyperthyroidism, neither TSH nor fT4 was associated with persistency but TPOAb positivity was associated with an 86% higher risk of persistency (Fig. 3). For women with overt hyperthyroidism, a higher fT4 was associated with an up to twofold higher risk of persistency, while there was no association for TSH and there was insufficient statistical power to show an association for TPOAb positivity (Fig. 3). There was no association of thyroxine (T4), T3, or early pregnancy hCG concentrations with persistency (data not shown).
Characteristics and thyroid function changes
Subsequently, we analyzed which participant characteristics were determinants of the change in thyroid function between the first and third trimester. For TSH, a higher TPOAb concentration, and to a lesser extent also a higher BMI, was associated with a smaller increase in TSH between the first and third trimester (Fig. 4 and Supplementary Table S3). A higher hCG concentration during early pregnancy was associated with a higher increase in TSH between the first and third trimester (Fig. 4). For fT4, higher hCG concentrations during early pregnancy, a higher BMI, and higher age were associated with a larger decrease in fT4 between the first and third trimester (Fig. 4). For T3, a higher BMI was associated with a larger increase in T3 between the first and third trimester, while a higher maternal age was associated with a slightly larger decrease in T3 between the first and third trimester (Fig. 4). The effect estimates for other potential determinants such as fetal sex, maternal education level, marital status, and parity were considerably lower (Supplementary Tables S3, S4, S5). For TPOAbs, the only determinant of the change between the first and third trimester was early pregnancy TPOAb concentrations (Supplementary Table S6).
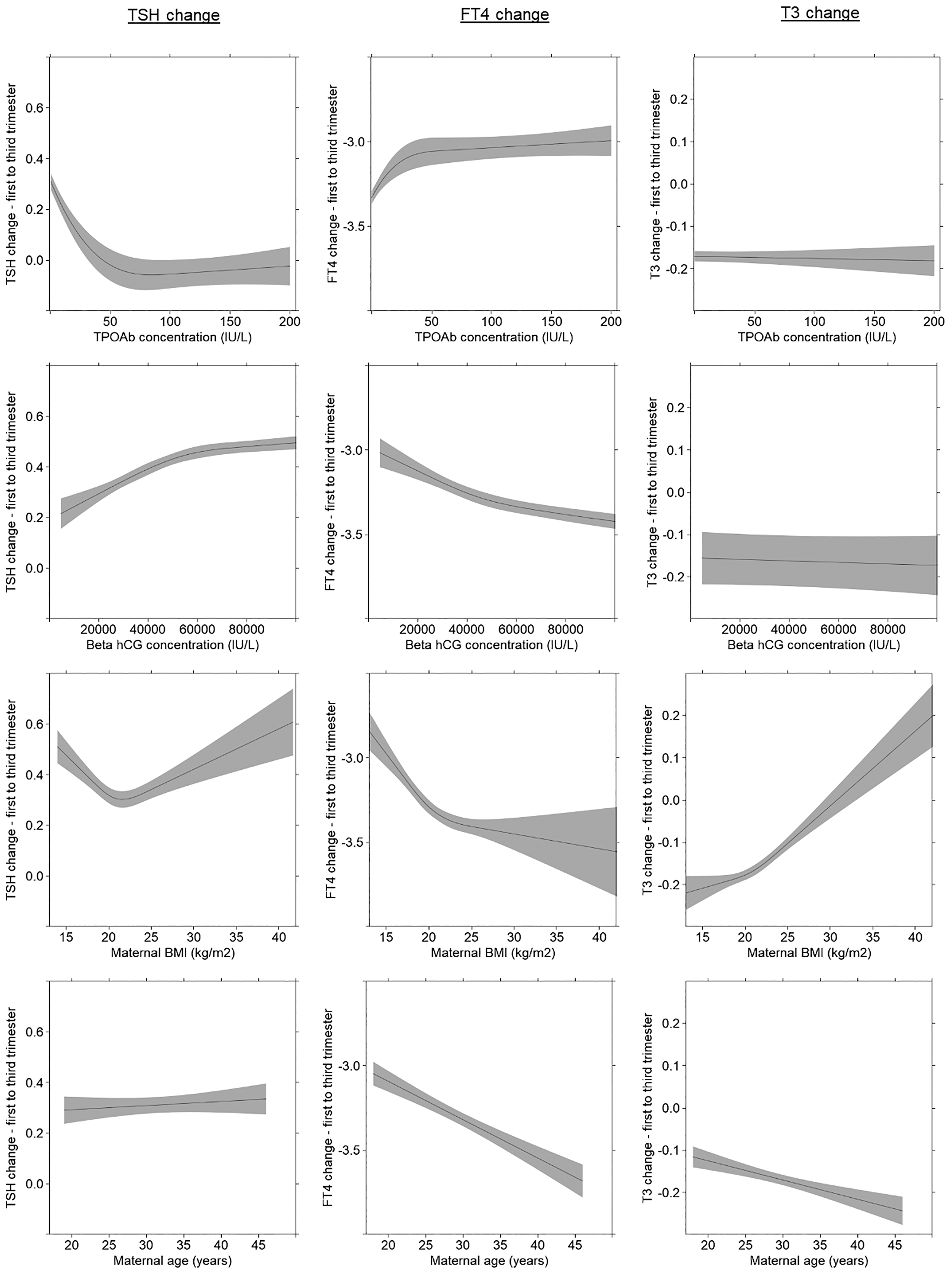
Determinants of the gestational change in thyroid function. Figures shows the association of TPOAbs, beta hCG, maternal BMI, and maternal age with the change in TSH, fT4, and T3 between early and late pregnancy as predicted mean (black line) with 95% confidence interval (gray area). BMI, body mass index.
Discussion
In this study, we present reference ranges for TSH, fT4, and T3 during the first and third trimester from a large Chinese hospital-based cohort and we quantify the inter-individual changes for these thyroid function measurements as well as TPOAb concentrations. The main finding of this study is that thyroid dysfunction during early pregnancy persists through the third trimester in only 8.4–24.8% of cases. Further, we show that a TSH concentration below 5 mU/L at diagnosis of subclinical hypothyroidism is associated with a lower risk of persistency, and that a higher fT4 concentration at diagnosis of hyperthyroidism is associated with a higher risk of persistency. Also, TPOAb positivity was associated with a lower risk of persistency of subclinical hypothyroidism and isolated hypothyroxinemia but a higher risk of persistency of (subclinical) hyperthyroidism.
To our knowledge, this study is the first to quantify what proportion of women have persisting thyroid dysfunction between early pregnancy and the third trimester. Our results show that only 8.4–24.8% of all women have persisting thyroid dysfunction. This suggests that the majority of gestational thyroid dysfunction entities diagnosed during early pregnancy represent a transient form of thyroid dysfunction. Most likely, the transient nature of thyroid dysfunction during early pregnancy is caused by the increased demand for thyroid hormone during early pregnancy (4). This increased demand is caused by the consumption of thyroid hormone by the fetus, the increase in thyroid hormone binding globulin, and the inactivation of thyroid hormone by type 3 deiodinase. Further, the thyroid gland is stimulated by the pregnancy-specific hormone hCG. We hypothesize that the transient nature of thyroid dysfunction as seen in the majority of women in this study could be caused by the inability of the thyroid gland to meet this increased thyroid demand. Alternatively, the low percentage of thyroid dysfunction persistency could merely reflect inter-individual variations in the physiological processes mentioned earlier.
The transient nature of both subclinical and overt hyperthyroidism (excluding toxic nodules or Graves' hyperthyroidism) is well recognized. Practically all studies to date have shown that these dysfunction entities are not associated with a higher risk of adverse pregnancy outcomes (5 –10). Therefore, current international guidelines recommend only close follow-up of women with (subclinical) hyperthyroidism during early gestation after exclusion of other causes such as Graves' hyperthyroidism. In this study, we show that TPOAb positivity is associated with an 86% higher risk of persistent subclinical hyperthyroidism. In line with these analyses, TPOAb positivity was associated with a 73% higher risk of persistent overt hyperthyroidism but this analysis did not reach statistical significance due to the relatively low number of women with overt hyperthyroidism. The higher risk of persistent (subclinical) hyperthyroidism in TPOAb-positive women is most likely due the common co-occurrence and shared genetic susceptibility of TPOAbs and TSH receptor stimulating antibodies (11 –13), which may be partly undiscovered (14). Unfortunately, TSH receptor (stimulating) antibodies were not routinely measured for this study. More studies are needed to investigate not only the role of TSH receptor antibodies but also that of thyroid nodules (15) in transient and persistent (subclinical) hyperthyroidism during pregnancy.
Previous studies show that TPOAbs decrease considerably during the course of pregnancy (16). In our study, TPOAb concentrations in TPOAb-positive women decreased on average by 67.4% (absolute change −39 IU/L [95% range: −1.7 to −514]), and due to this decrease, 16% of women were no longer considered TPOAb positive during the third trimester. It has been hypothesized that TPOAb positivity is a risk factor for postpartum thyroiditis because the reversal of maternal immune tolerance causes a flare-up in thyroid autoimmunity (17). As such, more data are needed to investigate whether the change in TPOAb concentrations is a more specific risk factor for the development of postpartum thyroiditis than TPOAb positivity alone.
Our results show that a higher β-hCG is associated with a larger increase in TSH and a larger decrease in fT4 between early and late pregnancy. These results fit with the biology that women with higher β-hCG concentrations in early pregnancy have a higher fT4 and lower TSH (4,18 –20). The lack of an association of hCG with the change in T3 as shown in this study may indicate that hCG stimulation does not affect T3 concentrations, however, we only had a limited overlap of hCG and T3 data (N = 497); therefore, further studies are needed to clarify this question. Our results also show that a higher TPOAb concentration is associated with a smaller increase in TSH and a smaller decrease in fT4 between early and late pregnancy, and this most likely also explains the finding that TPOAb-positive women are less likely to have persistent subclinical hypothyroidism. This most likely reflects an impaired thyroidal response to hCG stimulation caused by thyroid autoimmunity (19). Further, our results showing that especially BMI is an important determinant of the change in T3 could be because a higher BMI is associated with higher thyroxine binding globulin (TBG) concentrations, and TBG concentrations increase considerably throughout pregnancy (18,21). Therefore, a higher absolute TBG and/or an increase in TBG could account for the higher increase in TSH and T3, and the higher decrease in fT4 between the first and third trimester.
In this study, we were able to analyze prospectively collected data from a large population from an iodine-sufficient area (22) with detailed phenotyping and repeated thyroid function and TPOAb measurements. These data were collected in a hospital setting and therefore these are well generalizable to other hospital settings, especially in China. However, as compared with a population-based setting, a hospital-based setting comes with the limitation that some women are treated at the discretion of the attending physician. Although we excluded all women who received thyroid treatment, this could lead to an underestimation of the percentage of persistency. This was the most relevant for the group of subclinical hypothyroidism, in which 13.6% of women were treated. However, as compared with untreated women, treated women had only a slightly higher median TSH (4.16 vs. 4.75 mU/L) and we show that TSH concentrations only partially predict persistency of thyroid dysfunction. Further, participants excluded because of treatment were more likely TPOAb positive (23.4% vs. 53.4%) and TPOAb positivity was associated with a lower risk of persistency, which may counterbalance any potential underestimation. Another limitation of our study is that for TPOAbs and T3 repeated measurements were only available in a subset of the population (N = 12,343 for TPOAbs; N = 8490 for T3) and therefore should be interpreted with caution.
In conclusion, we show that early gestational thyroid dysfunction when left untreated only persists until the third trimester in 8.4–24.8% of cases. More specifically, we found that subclinical hypothyroidism persists in 24.8%, hypothyroxinemia persists in 17.7%, overt hyperthyroidism persists in 8.4%, and subclinical hyperthyroidism persists in 20.9%. The main predictor for persistency is the presence of TPOAb, with TPOAb-positive women having a lower risk of persistency of subclinical hypothyroidism or isolated hypothyroxinemia but a higher risk of persistency for (subclinical) hyperthyroidism. Further, a TSH below 5 mU/L was associated with a lower risk of persistency of subclinical hypothyroidism. In addition, we also report first and third trimester reference ranges for TSH, fT4, and T3 and identified that hCG, BMI, and age are the predominant determinants of the change in thyroid function between the first and third trimester. These data provide new insights into thyroid physiology during pregnancy and may aid clinicians in their clinical risk assessment of women with gestational thyroid dysfunction. Future studies are needed to investigate the effects of persistent gestational thyroid dysfunction on the risk of adverse outcomes.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions and efforts of all pregnant women who participated in this study and the doctors and nurses involved in data collection and patient care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (81471516, 81501274), the National Key Research and Development Program of China (2016YFC1000203), and the Foundation of Shanghai Municipal Commission of Health and Family Planning (15GWZK0701) and the Innovative Research Team of High-level Local Universities in Shanghai.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6