
Abstract
Background:
It has been advocated to apply individualized strategies to evaluate thyroid nodules due to the growing awareness that the pathogenesis of thyroid cancer is not uniform. Molecular markers in fine needle biopsies (FNBs) may be helpful for the diagnosis and management decisions. Unlike the detection of BRAF mutations, the clinical utility of rat sarcoma viral oncogene homolog (RAS) mutations has not been fully elucidated. This study aimed at presenting a real-world performance of RAS mutations in identifying thyroid malignancies, at investigating the nature of thyroid tumors carrying RAS mutations, and at providing an additional reference for interpreting how to utilize the presence of RAS mutations in the decision-making process of thyroid nodule management.
Methods:
Between February 2015 and December 2017, 1400 sequential thyroid biopsies were performed at Boston Medical Center. Of these, 546 FNBs were evaluated for RAS mutations by using a ThyroSeq next-generation sequencing panel. Nodules carrying RAS mutations were prospectively followed, and medical records were collected.
Results:
ThyroSeq successfully provided molecular information in 504 nodules; 173 with molecular alteration(s); and 80 positive for mutations in the Kirsten-, Neuroblastoma-, or Harvey-RAS genes. RAS gene mutations constituted up to 46.2% of the total molecular alterations found in the study. Fifty-six of the 80 RAS-positive nodules underwent surgery, 33 (58.9%) were confirmed to be benign, 7 (12.5%) were noninvasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP), and 16 (28.6%) were thyroid carcinomas. The positive predictive value, negative predictive value, and accuracy of RAS mutations for identifying malignancies among cytologically indeterminate nodules were 25.5%, 89.7%, and 54.0% when NIFTP was not counted as cancer. A combination of RAS and other mutations increased the risk of malignancy. Twelve histopathologically proved RAS-only-positive malignant nodules all showed low-risk features and favorable prognosis. RAS isoforms added little assistance for predicting a malignancy and the response to therapy in our series.
Conclusions:
RAS mutations represent the most frequently detected genetic alterations in our series. RAS mutations, when occurring alone, are not helpful markers to identify malignancy among Bethesda III/IV cytologies, but may predict favorable behavior, and hence should be considered to guide initial management.
Introduction
Recently published guidelines of the American Thyroid Association (ATA) (1) on the management of thyroid nodules and differentiated thyroid cancer (DTC) have provided comprehensive recommended strategies for clinicians, and yet several dilemmas remain, including: (i) the currently suggested approaches cannot correctly identify or exclude all malignancies among thyroid nodules; (ii) although fine needle aspiration (FNA) cytology undeniably has proven to be very useful, the large proportion of nodules with cytologically indeterminate results are diagnostically challenging; and (iii) as indeterminate nodules harbor a higher risk of malignancy than cytologically benign lesions, resection and histologic examination are required for diagnosis. But surgical intervention may represent overtreatment for the patients with nodules displaying low-risk features for whom active surveillance might be considered; and finally, (iv) although decision making based on the aggregate of preoperative diagnostic data including history, physical examination, ultrasound (US) characteristics, and FNA cytology has been helpful, it has not been universally sufficient and more objective information is needed to provide accurate risk assessment (2).
An important impact on our understanding of the boundaries between benign nodules and DTC occurred with the recommendation in 2016 for re-classification of noninvasive encapsulated follicular variant papillary thyroid cancer (FVPTC) as non-invasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP), that is, a benign or indolent lesion. NIFTP tumors often present as indeterminate nodules and because they deserve much less aggressive treatment and require surgical pathology for diagnosis (3,4), they ideally should be recognized preoperatively to avoid surgery and overtreatment.
Introduction of molecular testing strategies has the potential to preoperatively resolve questions in diagnosis and management by differentiating malignant from benign nodules and providing more accurate preoperative risk stratification. To date, among the known DNA-based molecular markers, mutations in the B-type Raf kinase (BRAF) and rat sarcoma viral oncogene homolog (RAS) genes are of particular importance, particularly because BRAFV600E mutation is the most prevalent genetic alteration in papillary thyroid cancer (PTC), and it can be associated with an unfavorable prognosis of PTC (5 –8).
Compared with the significance of the presence of the BRAFV600E mutation in thyroid cancer, the clinical utility of RAS mutations has not yet been sufficiently clarified. This may be attributed to the presence of RAS mutations in benign nodules, NIFTP, and thyroid malignancies (9). However, RAS mutations are the most common mutation in indeterminate FNA specimens (10), and so understanding their significance seems key to this issue. Management and risk assessment of indeterminate nodules could be facilitated if further evidence demonstrated the value of detecting RAS mutations in predicting an indolent nature for these tumors.
We addressed this question by assessing a large cohort of fine needle biopsy (FNB) specimens in which molecular markers were examined by using a next-generation sequencing (NGS) technique. Prospective follow-up data were collected, (i) to study the real-world significance of the presence of RAS mutations in identifying thyroid malignancies, (ii) to investigate the nature of thyroid tumors carrying RAS mutations, and (iii) to provide an additional reference for interpreting how to apply the presence of RAS mutations to the decision-making process for the management of thyroid nodules.
Subjects and Methods
During the period between February 2015 and December 2017, patients seeking care of thyroid nodules more than 1 cm in diameter were evaluated at the Section of Endocrinology, Diabetes and Nutrition, Boston Medical Center (Boston, MA), according to the ATA clinical practice guidelines (1,11). Experienced endocrinologists collected the medical history and performed US, storing the images on the radiology picture archiving and communication system (PACS). All sequential thyroid nodules that were eligible to be biopsied underwent US-guided (Toshiba Xario™ 200 with 5–14 MHz 58 mm Linear Array Ultrasound Transducer or 4.2–10.2 MHz micro convex probe; Toshiba America Medical System, Tustin, CA) FNB by endocrinologists.
Following a well-established protocol, 4–6 separate passes with a 1.5-inch, 25-gauge needle from the same nodule were performed by using aspiration or capillary techniques. The content of the first pass was reserved according to the manufacturer's instructions and shipped to the laboratory at CBL Path (Rye Brook, NY), where mutational analysis was conducted later, if necessary, by using the ThyroSeq NGS panel (12). The remainder of the FNB samples were submitted for direct cytology smears on slides and placed into collection fluid (20 mL of carbowax, a dispersing agent, dissolved in 80 mL of 60% ethanol). Samples were immediately transferred to the BMC Cytopathology Department. Slides were reviewed by academic, board-certified cytopathologists using low- and high-power microscopic views and categorized by the Bethesda system for reporting thyroid cytopathology (13). For all consecutive FNB samples with a diagnosis of Bethesda-III, IV, or V category, as well as occasional samples requested by a physician with a diagnosis of Bethesda-I, II, and VI categories but having suspicious clinical features, RAS mutations were searched as part of ThyroSeq NGS.
At the Boston Medical Center, for cytologically malignant nodules, as well as cytologically indeterminate nodules harboring mutations or gene fusions that predict a risk of malignancy, surgeries were recommended, unless there were contraindications such as severe cardiovascular or respiratory diseases. For those nodules with a benign cytology or indeterminate cytology but no malignancy-related molecular alterations, periodical follow-up was recommended, unless compression symptoms existed or patients were too worried or anxious about having a nodule. After the surgery, histopathology interpretation was reported by experienced pathologists. The surgical pathology was used as the gold standard for determining whether the target nodule was malignant or benign.
On study completion, we collected all associated medical records, US images and reports, cytology and histology reports, and molecular analysis results. The target nodule was carefully identified by correlating the site and size according to the pre-biopsied US images saved on the PACS, to ensure that cytology, molecular analysis, radiology, and pathology reports belonged to the same specific nodule. For molecular maker-positive nodules, their pre-biopsied US images were reviewed by the same experienced endocrinologist. On the basis of the recently published American College of Radiology (ACR) Thyroid Imaging Reporting and Data System (TI-RADS) lexicon, nodules were scored according to their US features, including composition, echogenicity, shape, margin, and echogenic foci; then classified into five categories with TI-RADS levels from 1 to 5 (14).
For confirmed malignancy by histopathology, we documented the cancer type and specific PTC variant. Tumor size, multifocality, extrathyroidal extension, lymphovascular invasion, lymph node, and distant metastatic diseases were recorded as well. Cancer staging was defined according to the 7th and 8th American Joint Committee Cancer TNM system, respectively (1,15). Initial risk stratification was defined according to the latest ATA guidelines (1,16). The postoperative outcome was assessed based on results of biochemical and/or radiological examinations. For those nodules that did not undergo surgery but were being followed for >6 months, we reviewed all available sonographic reports during follow-up. Thyroid nodule growth was defined as a >20% change in the largest two nodule dimensions.
For the purposes of comparing clinical and ultrasonic features between thyroid nodules positive for Neuroblastoma RAS (NRAS), Harvey RAS (HRAS), and Kirsten RAS (KRAS) mutations and those positive for other molecular alterations, based on previous publications (17,18), we divided these molecular alterations into six subgroups: RAS-only mutation; RAS-like (RL) alterations included: (H-, K-, N-) RAS mutation, BRAFK601E and PAX8/PPPARG fusions; BRAFV600E -like (BVL) alterations included: BRAFV600E and RET/PTC fusions; low-risk alterations included: TSHR mutation, PTEN mutation and EIF1AX point mutation, and NIS overexpression; combined high-risk alterations included: TERT promoter mutations with BVL or RL alterations; other alterations included: THADA fusions, NTRK fusions, RET point mutations, TP53 mutations, TERT promoter mutations, and EIF1AX splice mutations.
All data were recorded in an Excel file. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), prevalence, and accuracy of RAS mutations for identifying thyroid malignancy were calculated. Statistical analysis was conducted by using SPSS software (SPSS version 20.0; IBM, USA). Unpaired t-test/Mann–Whitney U-test and one-way analysis of variance test/Kruskal–Wallis test were applied to compare parametric variables between two groups and among multiple groups, respectively. For the comparison between frequencies, Chi-squared test, Yates 2 × 2 Chi-squared test (when there was <10 number in data), or Fisher's test (when there was <4 number in data) were used. A two-sided p level of 0.05 or less was considered statistically significant.
Results
During the study period, that is, between February 2015 and December 2017, a total of 1400 FNB on thyroid nodules were performed at our center. Of these, 580 nodules were enrolled for the ThyroSeq NGS evaluation (V.2 and V.3 panels were applied to 546 and 34 nodules, respectively). Since 34 nodules were biopsied and evaluated twice with the ThyroSeq panel, we only took their first biopsies into consideration. Thus, the final population for the present analysis consisted of 546 nodules from 513 patients. These nodules included 87 cases (18.3%) that were cytologically regarded to be insufficient for diagnosis (Bethesda I), 37 cases (6.8%) that were categorized as benign (Bethesda II), and 21 (3.8%) as malignant (Bethesda VI). Indeterminate results (Bethesda System III–IV–V) were identified in 401 (73.4%) of the 546 FNBs. Bethesda III (atypia or follicular lesion of undetermined significance) cytology was present in 322 cases (59.0%), Bethesda IV (follicular neoplasm or suspicious for follicular neoplasm) in 50 cases (9.2%), and Bethesda V (suspicious for malignancy) in 29 cases (5.3%). ThyroSeq NGS evaluation successfully provided molecular information in 504 nodules, while the material obtained from the remaining 42 nodules did not yield valid results due to insufficient material.
Among 504 nodules with available ThyroSeq results, 173 (31.7%) were identified as having 1 or more molecular alterations. These consisted of 9 (10.3% of 87) nodules with Bethesda I cytology, 6 (16.2% of 37) with Bethesda II, 104 (32.3% of 322) with Bethesda III, 18 (36.0% of 50) with Bethesda IV, 19 (65.5% of 29) with Bethesda V, and 17 (81.0% of 21) nodules with Bethesda VI cytology. Of these 173 nodules with molecular alteration(s), 80 nodules were positive for mutations in the K-, N-, or H-RAS genes. Mutated RAS constituted 46.2% of the total molecular alterations found in this study, which indicates that the RAS genes were the most commonly affected genes in our thyroid nodule cohort. RAS mutations were positive in 8 (6.5% of 124) nodules with Bethesda I or II cytology, 68 (17.0% of 401) with indeterminate cytology (58 with Bethesda III or IV and 10 with Bethesda V cytology), and 4 (19.0% of 21) with malignant cytology.
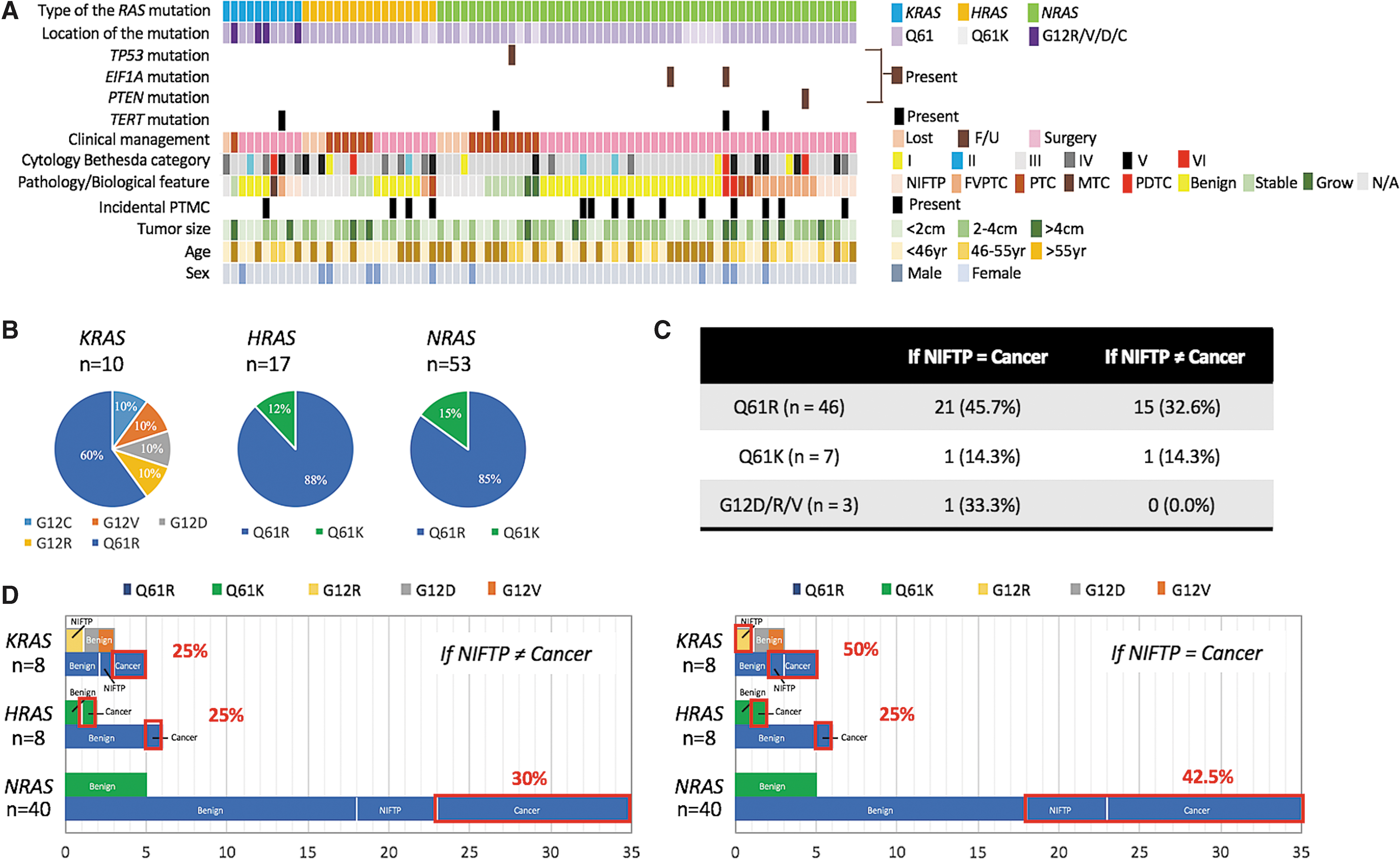
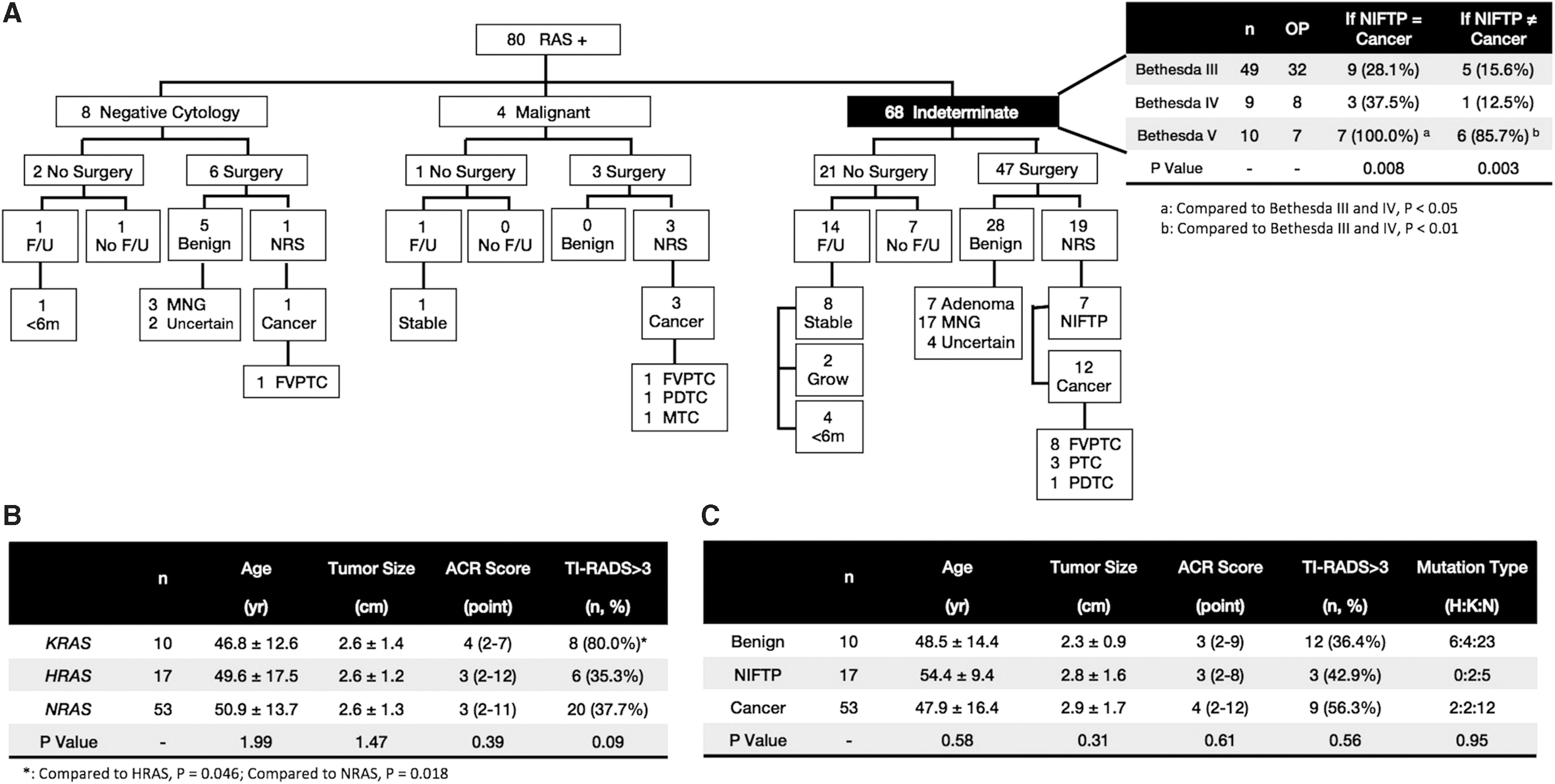
The landscape of mutated RAS genes in our cohort of thyroid nodules is presented in Figure 1. Of the 80 nodule specimens with RAS point mutations, 53 (66.3%) occurred in NRAS codon 61, 17 (21.2%) in HRAS codon 61, and 6 (7.5%) in codon 61, and 4 (5.0%) in codon 12 of KRAS, respectively. Tumor size, patient age at biopsy, sex distribution, ACR scores, and percentage of TI-RADS >3 did not show significant differences (Fig. 2) among the nodules harboring K-, N-, and H-RAS gene mutations. Two types of point mutations in codon 61, Q61R and Q61K, were identified in H- and N-RAS, with the Q61R mutation being more frequently present. For KRAS, only Q61R was seen in codon 61, while four types of point mutations in codon 12, that is, G12C, G12D, G12R, and G12V, were identified. In seven nodules, in addition to an RAS mutation, co-existing mutations included TERT promoter, TP53, PTEN, and EIF1AX mutations (Table 1).
RAS mutations detected in this study. (
Clinical characteristics and outcomes of 80 nodules carrying RAS mutations. (
Clinical Characteristics of the Patients with a Mutated RAS Combining Other Mutations
F, female; F/U, follow-up; FVPTC, follicular variant papillary thyroid cancer; M, male; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer; RAI, radioiodine; Tg, thyroglobulin; TSH, thyrotropin.
Fifty-six of the 80 RAS-positive nodules underwent surgery (Figs. 2 and 3). Total thyroidectomy was performed for 38 nodules and lobectomy was done for the remaining 18 nodules. Before 2017, all (n = 28) operations for nodules of this type were total thyroidectomies except for two cases. Since 2017, lobectomies were performed in 16 of 28 cases. Based on postsurgical histopathology, 33 (58.9%) of the 56 nodules were confirmed to be benign, 7 (12.5%) were diagnosed as NIFTP, and only 16 (28.6%) were diagnosed as thyroid cancer. The 16 confirmed malignancies included 10 FVPTC, 3 classic PTC, 2 poorly differentiated thyroid cancer (PDTC), and 1 medullary thyroid cancer (MTC). Incidental microcarcinomas were found by microscopic examination in 14 (25.0%) RAS-positive cases after surgical resection. K-, N-, and H-RAS mutations were associated with a comparable risk for thyroid cancer (25.0%, 25.0%, and 29.7%, respectively, p = 1.00) (Fig. 1D). When an RAS mutation occurred alone, only 22.4% of the nodules were malignant. However, 4 of the 5 operated nodules with an RAS mutation occurring concomitantly with another mutation were malignant (Table 1), thus suggesting that a combination of an RAS mutation with other mutations increases the risk of thyroid cancer.
Performance of RAS mutations for identifying malignant nodule. (
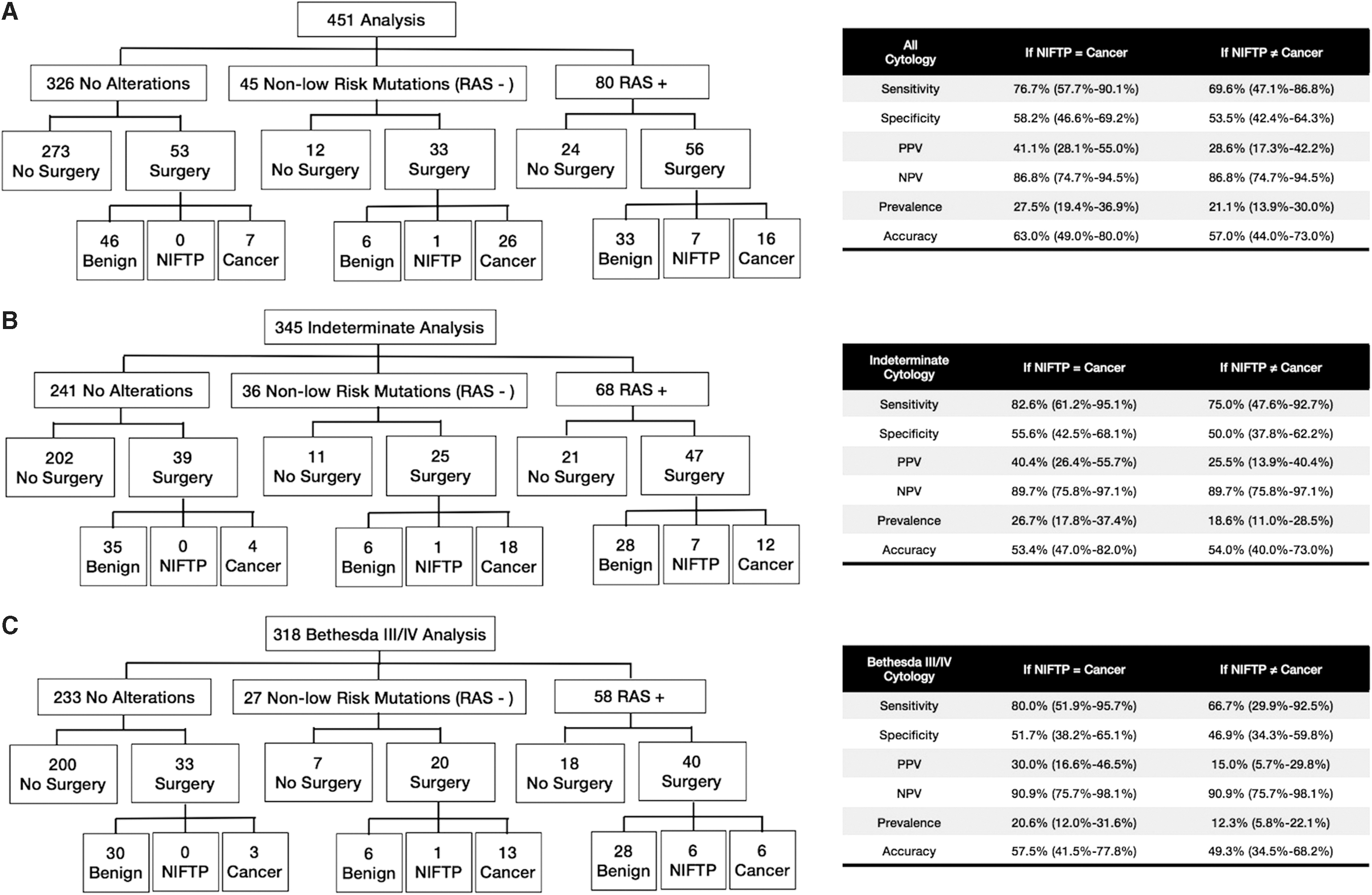
As demonstrated in Figure 2C, age, tumor size, and RAS mutation type were not significantly different among RAS-positive benign nodules, NIFTPs, and malignant nodules, neither were ACR scores and proportions of TIRADS level >3. This suggests that US features have limited value when performing preoperative characterization of RAS-positive nodules. Among the 68 indeterminate nodules (Bethesda III–IV–V) with RAS mutations, 47 underwent surgery to obtain a final pathology. Surgical pathology results showed that 40.4% (n = 19) were malignant if considering NIFTP as cancer, and 25.5% (n = 12) if NIFTP is being excluded from the cancer category. RAS mutation positive nodules in the Bethesda V category had a much higher risk to be malignant than those in the Bethesda III and IV categories, which suggests that the predictive value of mutated RAS alone for malignancy is less sensitive than the Bethesda classification.
We then calculated the sensitivity, specificity, PPV, NPV, and accuracy of RAS mutations for identifying malignant nodules. The results are listed in Figure 3, under the consideration of NIFTP being and not being cancer, respectively. When nodules in all Bethesda categories were included in the calculation (Fig. 3A), the sensitivity of a RAS mutation for predicting malignancy was around 70%, while the specificity fell below 60%, independent of whether NIFTP was counted as cancer or not. The PPV was unsatisfactorily low (28.6%–41.1%), and the NPV was 86.8%. When calculation was performed by using data of nodules with indeterminate cytology (Fig. 3B) or with Bethesda III and IV cytology (Fig. 3C), the sensitivity and NPV were not remarkably elevated, whereas the specificity and PPV further decreased.
In the pathologically proven nodules that were cytologically Bethesda III and IV, the prevalence of RAS mutations in malignant nodules [if NIFTP ≠ cancer, 26.1% (6/23); if NIFTP = cancer, 40.0% (12/30)] was comparable to that in benign cases (28/81, 34.6%). The prevalence of malignancy in RAS-positive nodules was 15.0% (if NIFTP ≠ cancer, 6/40) or 30.0% (if NIFTP = cancer, 12/40), suggesting that a positive RAS mutation test on a Bethesda categories III and IV nodule would indicate a higher risk of the thyroid nodule to be malignant or an NIFTP (12/40 vs. 3/33, i.e., 30% vs. 9.1%, p = 0.015).
Among the 21 RAS-positive indeterminate nodules that did not undergo surgery, 14 accepted periodical monitoring by US at the Boston Medical Center after the biopsy. Follow-up length exceeding 6 months (6–18 months) was achieved in 10 nodules by the end of this study. Among them, 8 nodules were stable but 2 (20.0%) increased in size on US. During the study period, 88 indeterminate nodules without any molecular alteration were followed for >6 months (6–29 months), and 7 (7.9%) increased in size. Due to inadequate sample size, we could not deduce whether indeterminate thyroid nodules harboring RAS mutations have a greater potential to grow in size than those that did not carry a mutation.
We further compared the clinicopathologic characteristics of the RAS-only-positive thyroid nodules with those harboring RL alterations, BVL alterations, low-risk alterations, combined high-risk alterations, or other genetic alterations (Table 2). The RAS-only-positive and RL-positive groups presented with similar features, although the latter group included eight additional nodules with a BRAFK601E or PAX8/PPPARG fusions. Nodules having BVL alterations were found in younger patients and were smaller in size; however, the differences did not reach statistical significance. All surgically removed BVL-positive nodules were confirmed as thyroid cancer; whereas in RAS-only-positive cases, malignancy occurred in ∼20%. Thyroid nodules having low-risk genetic alterations demonstrated comparable clinical characteristics as RAS-only-positive nodules, but they were entirely benign in surgically proved cases. Compared with the RAS-only-positive nodules, patients with a combination of high-risk alterations were less frequent in females, more prevalent in older patients, and malignant in all surgically treated cases (Table 2). In terms of nodules harboring other genetic alterations including THADA fusions, NTRK fusions, RET point mutations, TP53 mutations, TERT promoter mutations, and EIF1AX splice mutations, they had a significantly higher risk of cancer than RAS-only-positive nodules.
Comparison Among RAS-Only Mutation, RAS-Like Alterations, BRAFV600 E -Like Alterations, Low-Risk Alterations, Combined High-Risk Alterations, and Other Alteration Groups
RL alterations include: (H-, K-, N-) RAS mutation, BRAFK601E and PAX8/PPPARG fusions; BVL alterations include: BRAFV600E and RET/PTC fusions; Low-risk alterations include: TSHR mutation, PTEN mutation, and EIF1AX point mutation, NIS overexpression; Combined high-risk alterations include: TERT promoter mutations with BVL or RL alterations; other alterations include: THADA fusions, NTRK fusions, RET point mutations, TP53 mutations, TERT promoter mutations, and EIF1AX splice mutations.
Compared with the RAS-only mutation group, p < 0.05.
Compared with the RAS-only mutation group, p < 0.01.
Seven patients were not included in any group: 1 NRAS (p.Q61R) + TP53 (p.T170M); 1 NRAS (p.Q61R) + PTEN (p.232fs); 1 NRAS (p.Q61R) + EIF1AX (p.A113_splice); 3 calcitonin over expression; and 1 MET mutation.
ACR, American College of Radiology; AJCC, American Joint Committee Cancer; ATA, American Thyroid Association; BVL, BRAFV600E -like; DTC, differentiated thyroid cancer; F/U, follow-up; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; RL, RAS-like; TI-RADS, Thyroid Imaging Reporting and Data System.
Of the 12 histopathologically proved RAS-only-positive malignant nodules, 58.5% (n = 7) were FVPTC. There was no evidence of lymphovascular invasion, extrathyroidal extension, local lymph node metastases, or distant metastases in any of these seven FVPTC cases. Their initial ATA risk stratifications were all low risk, and furthermore there were no recurrences during the postoperative follow-up, independent of the extent of thyroid surgeries. Three of 12 RAS-only-positive thyroid cancer nodules were pathologically identified as classical type of PTC, and all demonstrated low-risk characteristics. One nodule with a KRAS Q61R mutation was found to be MTC. Although minimal extrathyroidal extension was seen, the patient had an excellent response to therapy with very low serum calcitonin and unremarkable neck US during the 26-month follow-up. Notably, one nodule harboring an NRAS Q61R mutation was confirmed as PDTC coexisting with multi-focal angioinvasion, resulting in an initial high ATA risk assessment. However, after total thyroidectomy and radioiodine ablation, this patient showed excellent response to therapy (thyroglobulin and thyroglobulin antibodies unmeasurable, negative neck US) at 14 months after initial treatment. In comparison to malignancies found in the RAS-only-positive group, thyroid cancers with BRAF-like mutations, combined high-risk mutations, or other non-low risk genetic alterations showed trends of being different in averaged largest dimension at study entry, and they were more likely to be in higher risk groups and to have a less favorable prognosis (Table 2). This tendency was most obvious in the group of nodules with combined high-risk mutations. These data suggest a more indolent phenotype among RAS-only-positive thyroid cancers.
Discussion
The human RAS gene family consists of three RAS genes, that is, KRAS, NRAS, and HRAS. Mutations in the RAS genes render RAS proteins, which function as GDP-GTP-regulated binary on
Mutations in RAS genes also occur in thyroid tumors and are the most frequent genetic alteration identified in nodules with an indeterminate FNA cytology. Indeed, RAS mutations are second in frequency only to BRAFV600E mutation as the most common to occur in thyroid malignancies (17,22 –24). Consequently, the determination of RAS mutations is incorporated in preoperative diagnostic molecular panels (25). However, unlike the prognostic significance of the BRAFV600E mutation, the utility of detecting RAS mutations in the management of thyroid nodules remains uncertain. In the present real-world study, we detected RAS mutations in more than 500 FNB samples of primarily cytologically indeterminate nodules, and prospectively collected long-term follow-up clinical data on the patients with these thyroid nodules. The data collected permit evaluation of the diagnostic performances of RAS mutations determination and its impact on management strategy and prediction of prognosis.
The data suggest that although the presence of RAS mutations is the most frequent genetic event in thyroid nodules, they provide poor value for prediction of thyroid cancer. Rather, on the basis of surgical pathology, most RAS mutations presented in benign nodules and NIFTPs, with thyroid cancer present in only 25.5% of cytologically indeterminate nodules harboring an RAS mutation. The relatively low PPV value in this study differs from that observed in four earlier studies and one meta-analysis. In two of these reports, RAS-positive, indeterminate nodules were histopathologically confirmed to be malignant in 52 of 63 (82.5%) and 66 of 87 (76%) of nodules (10,26). In another small series of subjects, 8 out of 10 (80.0%) RAS-positive nodules with abnormal or malignant cytology were surgically proven to be malignant (27). And a 93.3% PPV for malignancy was seen by An et al. with preoperative RAS mutation testing on BRAF-negative FNA specimens (28). Finally, a recent systematic review and meta-analysis indicated that the weighted averages for PPV and NPV of RAS mutations in indeterminate thyroid nodules were 78.0% and 64.0%, respectively (29).
That our study did not validate the “rule-in” capability of RAS mutations shown in the studies mentioned earlier relates to our exclusion for the first time from analysis and estimation of predictive value of FNB diagnosis of NIFTP. Two of the latter cited studies were completed before the application of the recently proposed terminology of “NIFTP” (4,30), and notably all RAS-positive thyroid cancers in both studies were FVPTC. As indicated by Paulson et al., more than half of the RAS-mutant tumors considered “carcinomas” were ultimately reclassified as NIFTP (31). Thus, it would be expected that neoplasms harboring RAS mutations would present a lower PPV for malignancy as in this study.
Another explanation for the disparity in PPV with earlier reports is the possible interference of co-existing genetic alterations on the risk of malignancy among RAS-positive thyroid nodules (32). In previous studies, the authors did not report whether RAS mutations had concomitant molecular changes, such as TERT promoter, P53 and EIF1AX gene mutations. The presence of mutations in these genes significantly increases the risk of malignancy in RAS-positive neoplasms, an observation that has been previously suggested (33 –35) and was confirmed in the study presented here. It is likely that the combination of RAS mutations and other genetic events was more common in the previous studies, leading to a higher PPV in comparison to this study.
Lastly, based on our results, the risk of cancer in an RAS-positive, cytologically indeterminate nodule is closely connected to its Bethesda category of FNA cytopathology. A Bethesda V cytological diagnosis coupled with an RAS mutation is associated with a much higher likelihood of a malignancy. In the study by Medici et al., at least half of the 10 RAS-positive thyroid nodules were cytologically diagnosed as Bethesda V or VI (27), mitigating the predictive value of RAS mutations reported for indeterminate nodules in their study.
The low predictive value of RAS mutations for malignancy revealed in this study led us to reconsider our past experience involving diagnoses of RAS-positive thyroid nodules, and in particular, cytologically indeterminate nodules. To many clinicians, the presence of RAS mutations indicates a high risk of malignancy sufficient to result in a surgical referral. We believe that other factors should be taken into account, including biological behavior of the nodules, worrisome US features, Bethesda V or VI cytological diagnosis, concurrent molecular alterations, or other clinical indications requiring a surgery.
We further investigated the clinical utility of RAS mutations as a prognostic tool to guide the extent of surgery for thyroid neoplasms. The potential management algorithm guided by RAS mutations in preoperative FNA specimens has been clarified by recent studies as well as our own data.
First, in cytologically benign thyroid nodules, RAS mutations play a minor role rather than driving carcinogenesis. In one long-term follow-up (mean 8.3 years) study, all cytological benign thyroid nodules carrying RAS mutations displayed exceptional stability without radiographic growth or adverse clinical consequences (27). Hence, these nodules can be conservatively followed and, according to findings by Medici et al. (27) and Durante et al. (36), the interval of repeat evaluation may be safely extended to 3 years.
Second, in cytologically indeterminate and malignant thyroid nodules, when RAS mutations occur alone, they may suggest a generally indolent phenotype inherent to the tumors. Previous studies have shown that low-risk FV-PTC contributed to the majority of nodules of this kind (10,37). After the introduction of the new nomenclature NIFTP, it became apparent that many RAS-positive nodules thought to be “carcinomas” were actually NIFTPs (31). We found a higher percentage of benign tumors in the present RAS-positive case series, and confirmed NIFTPs and low-risk DTC accounted for virtually all tumors requiring surgical management. Moreover, in contrast to other thyroid carcinomas with high-risk genetic alterations, recurrence and cancer-specific death were not seen in RAS-positive-only thyroid malignancies during the follow-up, confirming their relatively indolent nature. In the current ATA guidelines, lobectomy is considered sufficient therapy and recommended as an initial procedure for NIFTPs and low-risk DTC; active surveillance can also be one of the options for small low-risk DTC (1,30,38). As a result, the finding of solely RAS mutations in cytologically indeterminate nodules may indicate only lobectomy, or even only active surveillance if tumors are small.
Third, we should consider separately the uncommon RAS-positive thyroid carcinomas with poor behavior insofar as their more complex molecular profile will be associated with unfavorable outcomes. Coexistence of RAS mutations with additional oncogenic events, for instance, TERT promoter mutations, EIF1AX truncations, and P53 mutations, is likely responsible for this more aggressive phenotype (22,39 –43).
Consequently, a poorer prognosis will be seen in those patients with nodules displaying RAS mutations happening along with additional oncogenic alterations and management by a total thyroidectomy would be appropriate. With tumors lacking coexistent mutations, this modified RAS-guided approach, in fact, may have changed initial surgical decision making in up to 53% of patients in our series (Supplementary Fig. S1). For these patients, a less aggressive procedure appears to be sufficient, reducing the risks of surgical complications, and retaining more intrinsic thyroid function. Further well-designed prospective studies are needed to verify an RAS-based approach to management.
We also examined the influence of different RAS isoforms on thyroid cancer risk. Unlike pancreas, colon, and lung cancers, in which KRAS mutations are the predominant isoform and confer aggressive characteristics, thyroid neoplasms often may have an unique distribution of mutated RAS isoforms. Indeed, a few studies have demonstrated that NRAS mutations are the most frequently detected in thyroid nodules, followed by HRAS mutations and then KRAS mutations, despite the pathology being benign, NIFTP, or malignant (19,26,27,30,44). KRAS mutations may present a lower risk of malignancy (26,27).
Although our results are in accordance with previous reports regarding the distribution of RAS isoforms, we did not identify significant differences in terms of cancer proportion with different RAS isoforms. On another note, while two patients with thyroid cancer containing KRAS mutations were both classified as ATA intermediate risk initially, RAS isoforms added minimal assistance for predicting response to therapy in our series, which may be due to the small sample sizes. Further investigations may ascertain whether determination of RAS isoforms could enhance the precision of risk stratification and decision making.
Strengths of this study include that the amount of nodules harboring RAS mutations were greater than that in most previous studies of this kind, and that 70% of RAS-positive nodules had postsurgical histopathology with follow-up in 67% of nodules that were not resected. Employing the ThyroSeq NGS panel, we could determine the different phenotypes of nodules with an isolated RAS mutation versus those with the combination of RAS mutations and other genetic events. This information provides insight into expected clinical outcomes associated with wide variation of tumor behaviors in RAS-positive thyroid nodules.
Limitations of this study include that it was conducted in a single center with patients who may not be representative of the general US population. Second, the results of molecular markers were not blinded to pathologists. Third, we were unable to gain extra information on the prevalence and clinical significance of RAS mutations in benign nodules as we did not examine RAS mutations in the majority of cytologically benign nodules. Fourth, because a 100% of RAS-positive nodules did not undergo surgery, the precision calculation of predictive values for the presence of RAS mutations may have been influenced.
In conclusion, RAS mutations, when occurring alone, are not sufficient markers to identify malignancy in indeterminate thyroid nodules, but they may predict favorable behaviors, and hence should be considered in initial management decision making. Indeterminate thyroid nodules with an isolated RAS mutation deserve more conservative strategies, as opposed to routine (total/near total) thyroidectomy, to avoid irreversible injuries from unnecessarily aggressive interventions. The combination of RAS mutations and other genetic events may indicate higher risk of malignancy and poorer outcomes. In RAS-positive nodules, applying a panel to test additional molecular markers can be informative, especially when nodules exhibit clinical signs of aggressiveness.
Footnotes
Acknowledgments
The authors sincerely appreciate the support of Dr. Leonard Wartofsky for his valuable comments and help during the revision of this article.
Ethics
This prospective study was conducted in compliance with a protocol that was approved by the Boston University Institutional Review Board. Informed consent was given by all patients before performing the procedure.
Authors' Contributions
S.L. designed the study. H.G., G.T., and F.G. reviewed clinical records, collected data, and did data input. S.C. confirmed pathology information. D.M., G.D., L.B., and S.L. managed and followed up patients. H.G. performed statistical analysis; prepared the article, tables, and figures. S.R., G.D., and S.L. revised the article. All authors read and approved the article.
Author Disclosure Statement
The authors report no conflicts of interest in this work.
Funding Information
No funding was received.
Supplementary Material
Supplementary Figure S1