
Abstract
Background:
The cribriform-morular variant (CMV) is a rare subtype of papillary thyroid carcinoma (PTC), and is often associated with familial adenomatous polyposis (FAP). This variant is generally indolent, but some aggressive cases have been reported.
Patient Findings:
We present the case of a 24-year-old woman who underwent total thyroidectomy with prophylactic central lymph node dissection and modified radical neck dissection for CMV-PTC. No distant metastases were identified preoperatively. However, multiple large lung metastases were detected three and half years after surgery. She also had FAP with a germline APC gene mutation.
Summary:
She was started on lenvatinib because of the metastatic disease. One month after the initiation of lenvatinib (24 mg), her lung metastases reduced significantly. She has continued lenvatinib for 24 months (present dose, 10 mg). The lung metastases have not progressed during this period. Only a few small polyps were newly detected on endoscopy after lenvatinib administration. This number was considerably higher before therapy, when an average of 21–75 polyps were resected at each endoscopy session.
Conclusions:
This is the first report of the use of lenvatinib for the treatment of distant metastases from CMV-PTC. In addition to the efficacy in treating metastatic lesions of this rare variant of PTC, lenvatinib shows promise in the management of associated FAP. This treatment strategy may be useful in the management of recurrent CMV-PTC and in those with FAP who refuse colectomy.
Introduction
Cribriform-morular variant (CMV) is a rare subtype of papillary thyroid carcinoma (PTC). CMV patients often have APC gene mutations, which are associated with familial adenomatous polyposis (FAP). However, CMV may also occur sporadically with no relationship with FAP (1 –3). Morphologically, these tumors are encapsulated or circumscribed with a cribriform pattern without colloid, and demonstrate morules with peculiar nuclear clearing on hematoxylin–eosin (H–E) staining. They also show typical immunohistochemical profiles, with nuclear and cytoplasmic localization of beta-catenin, and negativity or only focal staining for thyroglobulin (3,4). Furthermore, strong positivity for estrogen receptor (ER) and progesterone receptor (PR) in CMV-PTC has been reported (3,4); however, their expression levels are not specific for CMV-PTC (5). CMV generally has an indolent character, although a few aggressive cases with distant metastases and dire prognoses have been reported (6 –8). CMV is a very rare histological subtype, accounting for up to only 0.40% of all PTCs; most patients are young females (4,9 –14). Previous studies showed that CMV only occasionally metastasizes to regional lymph nodes, although recurrences within the remnant thyroid have been observed after hemithyroidectomy in FAP-associated CMV (4,10).
Lenvatinib is a selective inhibitor of receptor tyrosine kinases related with tumor cell proliferation and angiogenesis, including FLT-1, VEGFR-1 and -2, RET, FGFR1, PDGFR-beta, and c-KIT (15). A randomized phase III trial showed its efficacy in progressive metastatic radioactive iodine (RAI)-refractory differentiated thyroid carcinoma. However, some significant adverse events were reported, which include hypertension, proteinuria, diarrhea, dysphonia, and, if used for other malignancies, hypothyroidism (16).
In this study, we report the case of a patient with aggressive FAP-associated CMV-PTC with multiple and large lung recurrences soon after total thyroidectomy. The pathological findings of this case have been published previously (17), but the subsequent clinical course is of particular interest. The patient was successfully treated with lenvatinib, which showed remarkable efficacy not only in controlling the lung metastases but also in the associated colon polyposis.
Case presentation
A 24-year-old female patient visited our hospital with complaints of a mass in the right neck. On examination, the right lobe of the thyroid revealed a fairly hard and mobile palpable mass. Ultrasound examination showed a solid nodule in the right lobe measuring 87 × 41 × 53 mm, with no pathological lymph nodes. The nodule was cytologically diagnosed to be CMV-PTC owing to the presence of tall columnar cells with a cribriform arrangement. Her thyroid function was normal. The thyroglobulin level was 85.0 ng/mL, and she tested negative for antithyroglobulin antibodies. No lung metastases were detected on the preoperative computed tomography (CT) scan. On enquiring about her family history, the patient mentioned that her mother died of colon carcinoma at the age of 41 years.
After preoperative assessment, she underwent total thyroidectomy with prophylactic central node dissection and right modified radical neck dissection. The tumor was pathologically diagnosed as CMV-PTC because of the typical morphological characteristics on H–E staining (Fig. 1a), and nuclear and cytoplasmic localization of beta-catenin (Fig. 1b). Carcinoma cells were also positive for ER (Fig. 1c) and PR; however, this is not a specific characteristic of CMV-PTC (5). The Ki-67 labeling index (LI) was high in the hot spots, at 50% (Fig. 1d). The carcinoma cells tested negative for thyroglobulin. Moreover, carcinoma cells were negative for chromogranin and synaptophysin. No lymph node metastases were detected pathologically. Although no adjuvant RAI was administered after surgery, her thyroglobulin levels were found to be undetectable, and she underwent postoperative follow-up under thyroid stimulating hormone suppression.
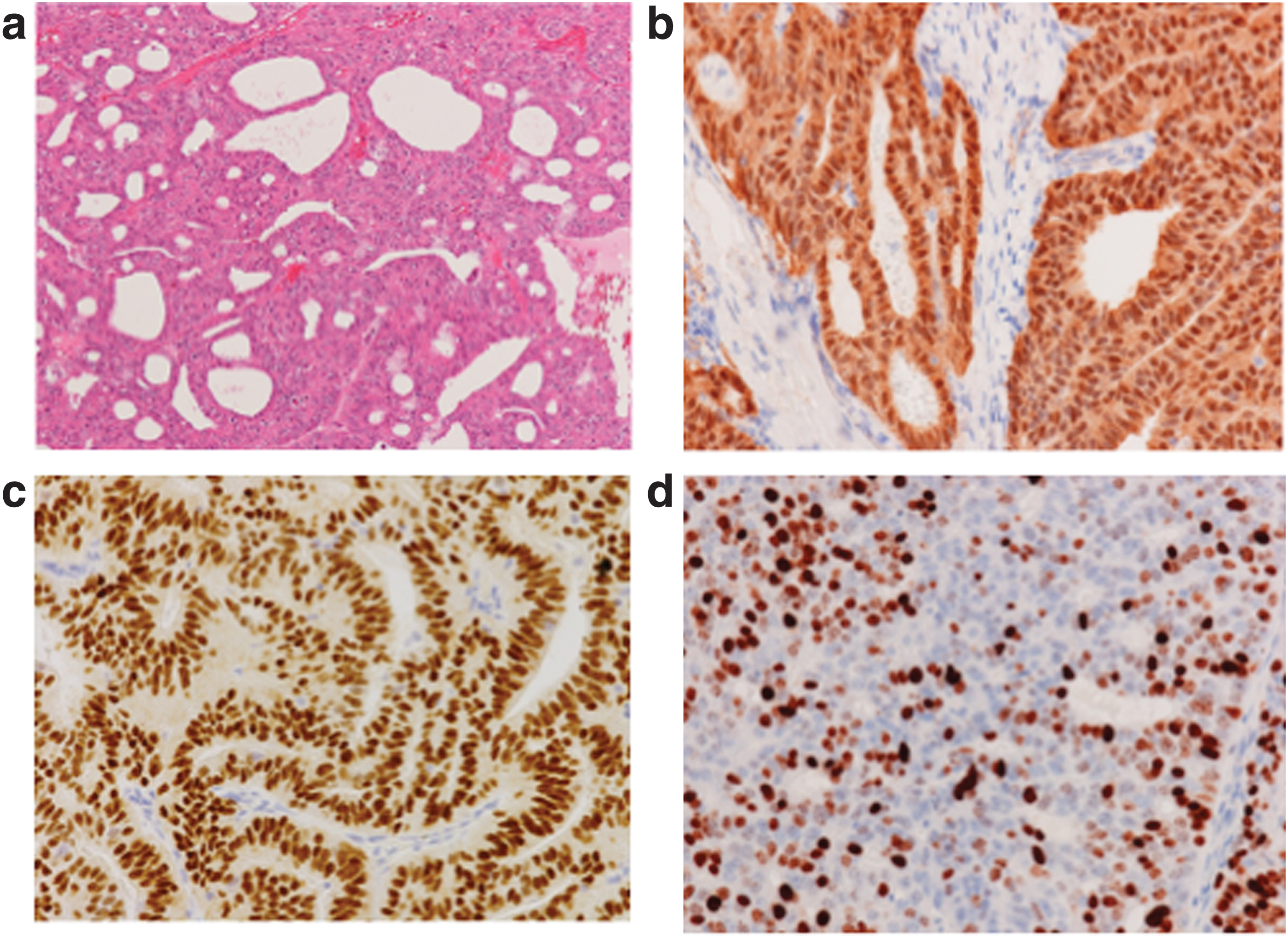
H–E staining and immunohistochemical staining of primary lesion. (
Forty-two months after surgery, a follow-up CT scan revealed multiple bilateral lung lesions (maximal diameter was 41 mm on the right side, and the sum of the two largest lesions for RECIST measurement was 71 mm) (Fig. 2a). Serum thyroglobulin at 24 months after surgery was found to be detectable, yet low, at 1.1 ng/mL. The level gradually became elevated to 5.47 ng/mL at the time of detection of the suspected lung metastases. Although the thyroglobulin level was low for the volume of the lung lesions, the associated thyroglobulin doubling-time (Tg-DT) was short. It amounted to 0.59 years from the time that the thyroglobulin became detectable to the time that the lung lesions were detected. Her lung lesions were diagnosed as metastatic CMV-PTC based on the histopathological findings on H–E staining of the surgical biopsy specimen (Fig. 3), and on the immunostaining profiles of beta-catenin, ER, and PR. Ki-67 LI was 70% in the hot spots; the carcinoma cells also tested negative for thyroglobulin, as previously reported (17). Then, at 45 months after surgery, she underwent RAI treatment at a dose of 100 mCi after levothyroxine withdrawal. However, the lung lesions demonstrated no uptake. The positron-emission tomography (PET)-CT scan showed no metastases other than those in the lung. Magnetic resonance imaging of the brain revealed no metastases.
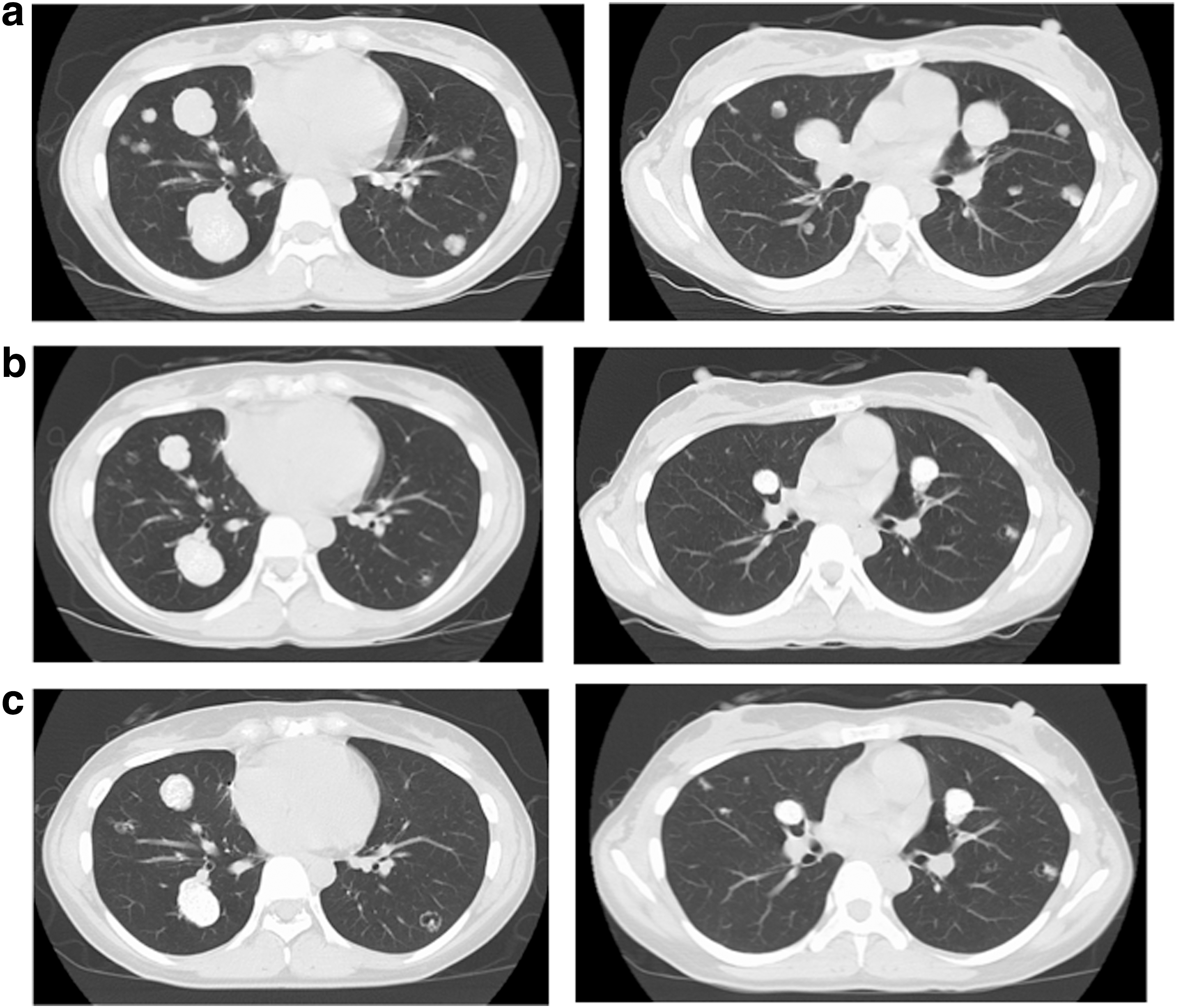
Computed tomography findings showing lung metastases (
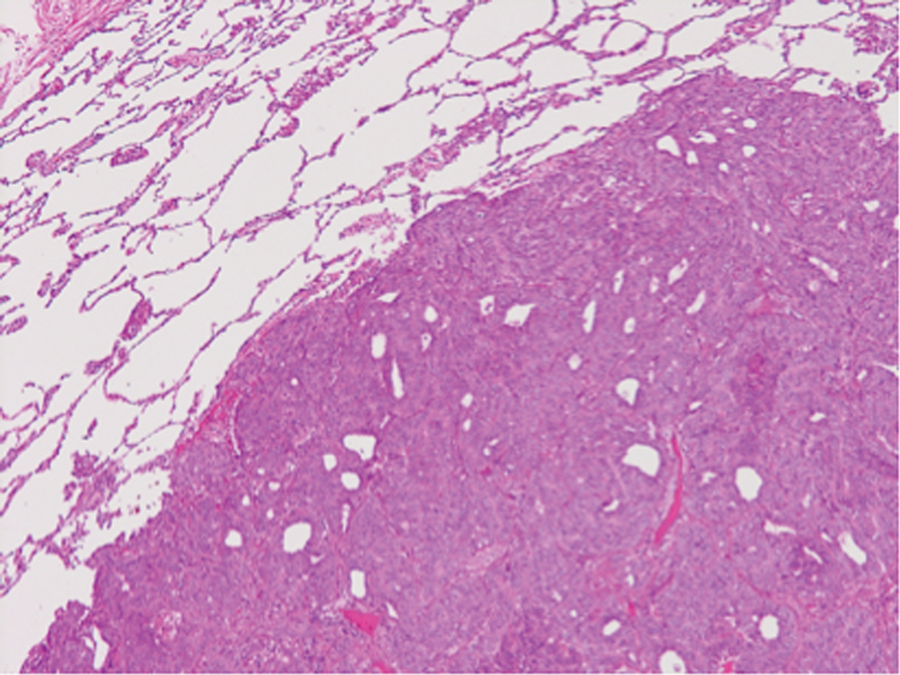
H–E staining of biopsy specimen of the lung metastasis.
Subsequently, at 46 months after surgery, lenvatinib (24 mg) was initiated for the treatment of the lung metastases. The doses of lenvatinib and the changes in the thyroglobulin levels are summarized in Figure 4. Four weeks after its initiation, lenvatinib had to be withheld for 1 week due to proteinuria (grade 3), and was restarted at a dose of 20 mg. Further dose reductions were necessary at 8 and 10 weeks of therapy for the same reason, bringing the daily dose down to 10 mg. At each instance, lenvatinib was withheld for 1 week before being restarted. Further dose reductions were not necessary, but the drug had to be withheld for short periods (not exceeding 1 week) for various reasons including diarrhea, constipation, nausea, anorexia, and infection of the airways. She did not develop hypertension during the course of therapy. At 19 months after initiating treatment, a slight elevation was noted in her thyroglobulin levels; a PET-CT scan performed to rule out metastases to other organs revealed no significant metastases, except in the lung.
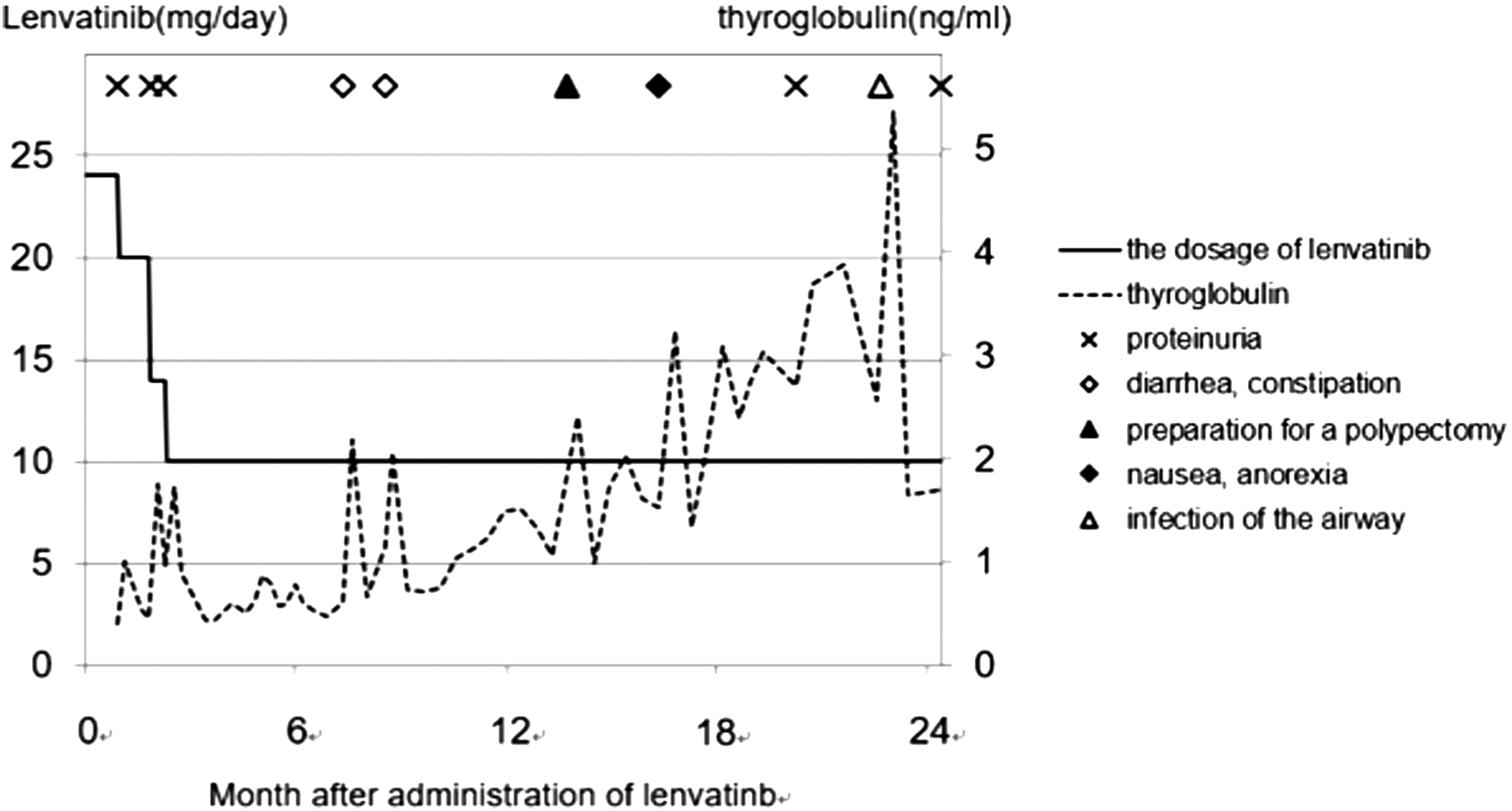
Change in doses of lenvatinib and thyroglobulin levels. The periods and reasons for withholding lenvatinib are also shown.
The CT scans at 1 and 24 months (most recent evaluation) after the initiation of lenvatinib showed considerable reduction in the lung metastases (Figs. 2b, c). Figure 5 shows the change in the sum of the diameters of the two largest metastases, for the evaluation based on RECIST measurements (version 1.1) (18). Metastatic lesions of the lung were judged to have achieved partial response six months after the initiation of lenvatinib, and the partial response was maintained throughout thereafter.

Change in the sum diameters of the two largest metastases. At six months after the initiation of lenvatinib, they were judged to be partial response based on RECIST. PR, partial response.
Since she had the CMV histology of PTC, and her mother died of colon carcinoma, she was also started on treatment for FAP by periodical endoscopic polypectomies. She was found to have the APC gene mutation (stop codon at codon 325) and was enrolled in a clinical study entitled “Intervention trial for colorectal cancer prevention by endoscopic polypectomy in patients with FAP” (UMIN000009365). She had multiple small polyps not exceeding six mm in size (Fig. 6). The first polypectomy was performed 20 months after thyroid surgery, and 21 polyps were dissected. She subsequently underwent colon endoscopy with polypectomy five more times. At each endoscopy session, all visible polyps were dissected; this indicated that most polyps dissected at each session had newly developed after the previous session. Endoscopic polypectomy was performed three more times before her lenvatinib administration. At 27 and 35 months after thyroid surgery, 45 and 75 polyps measuring up to 6 mm, respectively, were dissected. During 35–43 months after surgery, she was enrolled in a randomized clinical study entitled “Japan familial adenomatous polyposis prevention study: Randomized controlled trial by low-dose aspirin and/or mesalazine” (UMIN000018736). It became known after the trial period that she had received aspirin while in the study. The number of polyps not exceeding 6 mm had decreased to 33 at 43 months after thyroid surgery. She discontinued aspirin at this point as the clinical study had ended. In the two endoscopy sessions after administration of lenvatinib, the number and maximal size of dissected polyps drastically reduced. Only 2 polyps measuring up to 3 mm and 1 polyp measuring 4 mm were discovered and removed at each session at 52 and 60 months, respectively, after thyroid surgery (and 6 and 14 months after lenvatinib initiation, respectively). All these findings are summarized in Figure 7.

Colonic polyps of this patient as seen during endoscopy (arrows).
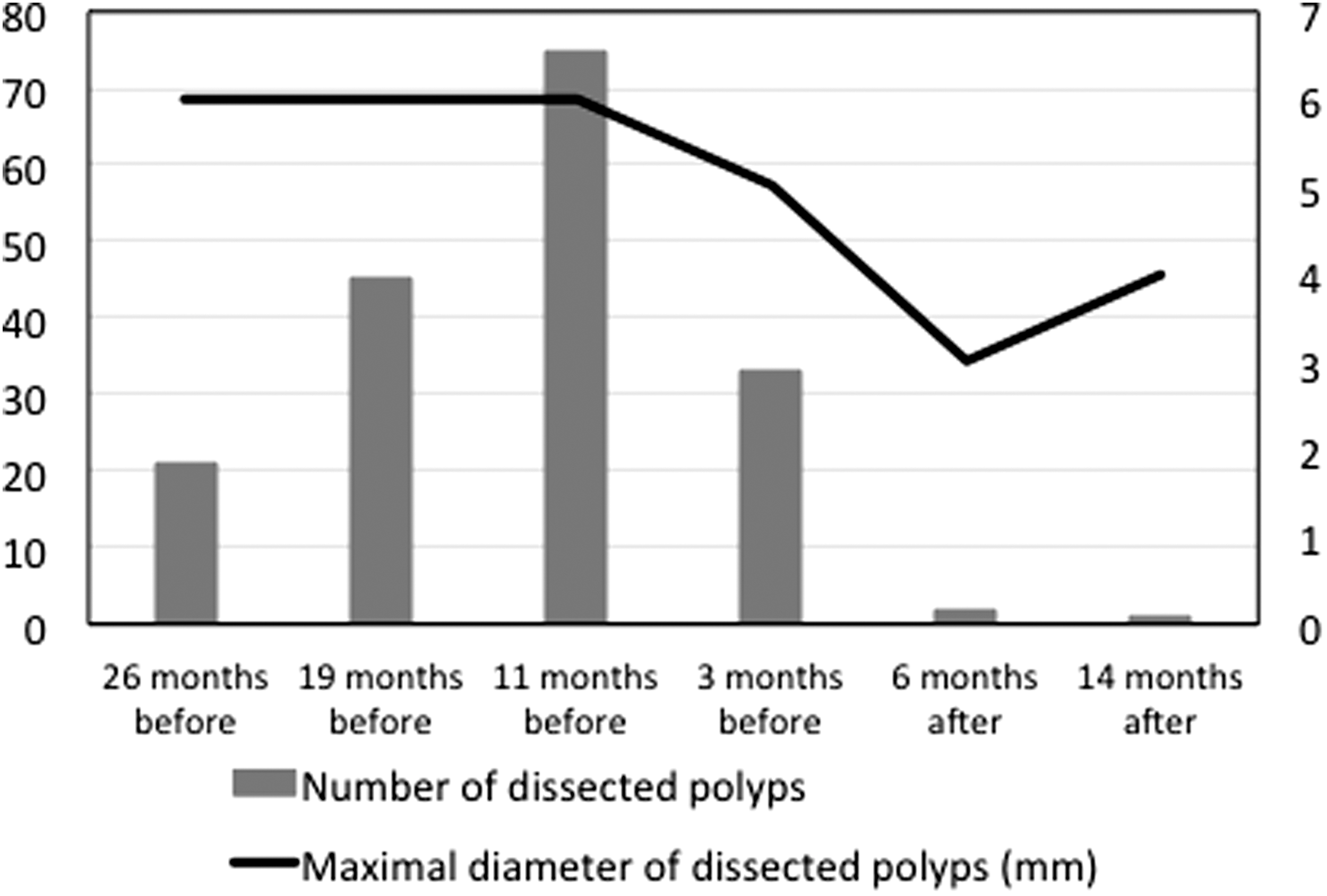
Number and maximal sizes of polyps dissected before and after the initiation of lenvatinib. Administration of aspirin was commenced and completed in 11 and 3 months, respectively, for the patient before lenvatinib administration.
Discussion
We present an aggressive case of FAP-associated CMV-PTC with multiple lung metastases, which occurred shortly after total thyroidectomy. This is the first reported use of lenvatinib for the treatment of distant recurrences from CMV-PTC, a rare histological subtype. This case provides some important lessons for clinicians. A notable lesson is that CMV-PTC does not express thyroglobulin or, at best, expresses it very weakly (2). Therefore, elevations of serum thyroglobulin at the time of recurrence in CMV-PTC are much lower than that of conventional PTC. Considering that CMV-PTC generally has an indolent character, early diagnoses of CMV recurrences are difficult. In this case, despite the large tumor burden in the lung, the thyroglobulin levels at the time of detection of metastases were still low, at 5.47 ng/mL. However, Tg-DT between the time of detection of thyroglobulin and detection of recurrence was very short, at 0.59 years. Miyauchi et al. demonstrated that the 10-year cause-specific survival rate was very low, at 50%, in thyroglobulin antibody-negative PTC patients with Tg-DT shorter than 1 year (19). This suggests that when untreated, the lung recurrence in our case would probably have progressed rapidly, and may have become life threatening. Therefore, during the postoperative follow-up of CMV-PTC, significant attention needs to be paid to the Tg-DT when thyroglobulin becomes detectable; this will aid early detection of recurrences.
Another notable point is the high Ki-67 LI. We previously demonstrated that Ki-67 LI has strong prognostic implications in PTC (20). In our experience, Ki-67 LI in CMV-PTC is generally high, at 10–20%, despite its indolent character (21). However, in this case, Ki-67 LI was extraordinarily high, at 50% in the primary lesion, and 70% in the metastatic lesions. This was an important feature, which indicated an aggressive behavior and predicted early recurrence in this case. We could not find any other pathological markers predicting poor prognosis in this case. We investigated the expression of chromogranin and synaptophysin because in a case of aggressive CMV-PTC with neuroendocrine differentiation, the patient died with lung and brain metastasis 17 months after thyroidectomy (6). However, in this case, the expression for these markers was negative.
This patient has been successfully treated with lenvatinib for her lung metastases. After one month of treatment with lenvatinib, the metastatic lesions shrunk significantly; this is a typical effect of lenvatinib therapy (22). No disease progression has been noted during the periods of follow-up. Sugino et al. analyzed the clinical factors related to the efficacy of lenvatinib, and reported that the presence of tumor-related symptoms, including dyspnea due to lung metastases or pleural effusions, bleeding from metastatic lesions, dysphagia due to esophageal, or pharyngeal metastasis, and pain or paralysis due to bone metastases were independent predictors of poor progression-free and overall survival in patients administrated lenvatinib for RAI-refractory metastases from differentiated carcinoma (23). Since this patient did not demonstrate tumor-related symptoms during initiation of lenvatinib, despite the huge metastatic tumor volumes, she is more likely to achieve long-term survival. Furthermore, the success of treatment could also be attributed to the fact that she could continue lenvatinib without withholding it for long intervals. Consequently, her lung metastases are stable, and continued shrinking.
Her thyroglobulin levels, however, fluctuated frequently and even gradually increased during lenvatinib treatment. Therefore, we performed a PET-CT scan at 19 months after initiating treatment; however, it revealed no metastasis to other organs and her lung lesions were stable. The reasons for these thyroglobulin elevations remain unknown and continuous active surveillance is, therefore, indicated. However, at least at present, changes in the metastatic lesions on imaging should be considered more reliable than thyroglobulin levels in evaluating disease status.
The features of CMV-PTC are known to have distinctive clinical, pathological, and molecular profiles compared with the conventional PTC (24). Although some aggressive cases have been reported, in general, CMV-PTC is a biologically and clinically indolent tumor. Uchino et al. investigated 129 patients with FAP and reported that 24 patients (18.6%) (17 females and 7 males) had solid thyroid nodules (25). In the 17 female patients with solid nodules, CMV-PTC was found in 8 of 9 patients aged 35 years or younger, but in none of the 8 patients older than 35 years. This shows that CMV-PTC possibly regresses with age. However, since distant metastases in CMV-PTC are extremely rare, whether lung metastases will regress with age in this case remains unknown.
Sorafenib is another accepted line of therapy in lenvatinib-failure cases in Japan. However, CMV-PTC strongly expresses ER and PR, which was also observed in this case. Therefore, selective ER modulators such as tamoxifen may be effective in treating this variant of PTC, although there is no evidence in the literature.
The standard treatment for FAP is subtotal colectomy. However, endoscopic management is an acceptable alternative in patients refusing colectomy (26). This patient was enrolled in a clinical trial for colorectal cancer prevention by endoscopic polypectomy. Although the sizes of her colon polyps were generally small, they were multiple, and reappeared in large numbers after each polypectomy session before the initiation of lenvatinib. As reported previously, the number of polyps decreased to some extent during aspirin therapy (27). However, this patient discontinued aspirin at 43 months after thyroid surgery, and 3 months before the initiation of lenvatinib, indicating that aspirin did not influence the status of the polyps at the time of lenvatinib initiation. After the initiation of lenvatinib, the number of newly appearing polyps significantly decreased, and their size became smaller. This suggested that lenvatinib is effective not only for lung metastases, but also for the control of colon polyps, although the exact mechanism is yet to be elucidated. This treatment strategy could, therefore, be an alternative for FAP-associated CMV-PTC having aggressive distant metastases, because active surveillance of FAP by colonoscopy is less invasive than surgery. This may also be an alternative for patients who refuse colectomy. A previous case report demonstrated the efficacy of imatinib mesylate, another tyrosine kinase inhibitor, in managing FAP in a patient with chronic myelogenous leukemia (28). Imatinib mesylate is a c-KIT signal transduction inhibitor (29). Lenvatinib also inhibits signal networks mediated by c-KIT (15), indicating that this may be related to the efficacy of lenvatinib for colon polyps, although the mechanisms remain unknown.
This report describes the remarkable benefits of lenvatinib therapy in the simultaneous treatment of distant metastases from CMV-PTC and FAP. This treatment strategy could be an acceptable alternative for the urgent management of rapidly progressing recurrences of FAP-associated CMV-PTC, and for FAP patients who refuse colectomy.
Statement of ethics
The patient and her family provided written informed consent for publishing these data in the report.
Footnotes
Author Disclosure Statement
No competing financial interests exist.