
Abstract
Background:
Elevated levels of antithyroperoxidase antibodies (TPOAbs) have been associated with progression of subclinical thyroid dysfunction, extrathyroidal diseases, and decrease in functional status. However, TPOAb as determinant of future thyroid dysfunction and other clinical outcomes has not been studied well for adults aged 85 years and over. This study aimed to assess associations of TPOAb levels with thyroid function, survival, physical function, disability in activities of daily living (ADL), cognitive function, and depressive symptoms in the oldest old.
Methods:
Data from a population-based cohort study (Leiden 85-plus Study) of residents of Leiden, the Netherlands, aged 85 and older were used. Baseline serum TPOAb levels were available for 488 participants (82% of the total cohort). We considered levels ≥35 IU/mL as elevated. Thyroid function (thyrotropin [TSH] and free thyroxine) was assessed at age 85 (baseline), 87, and 88 years. Survival, physical function, disability in ADL, cognitive function, and depressive symptoms were assessed from age 85 through 90 years.
Results:
At baseline, 64 of the 85-year old participants (13.1%) had elevated TPOAb levels. They were more often female, had higher TSH levels, and a higher prevalence of overt or subclinical hypothyroidism than participants with normal TPOAb levels. Over time, elevated TPOAb levels were independently associated with a lower mortality risk (hazard ratio 0.72, [95% confidence interval 0.53–0.99]), but were not associated with changes in thyroid function, nor with physical function, disability in ADL, cognitive function, or depressive symptoms.
Conclusions:
In community-dwelling oldest old, elevated TPOAb levels are cross-sectionally associated with higher TSH levels. Over time, elevated TPOAb levels are associated with a survival benefit but are not associated with changes in thyroid function, functional status, or depressive symptoms in old age. The added clinical value of TPOAb tests in oldest old persons with thyroid dysfunction is limited.
Introduction
In recent decades, the interest in autoimmune antibodies as predictive biomarkers has risen (1,2). Since the discovery of antithyroperoxidase antibodies (TPOAbs), its usefulness as a determinant of health status in thyroid dysfunction has been investigated, but results have been ambiguous. Guidelines are starting to cautiously recommend assessing TPOAb status to assess risk of thyroid disease progression, choose follow-up modalities, and weigh treatment options (3).
The relationship between elevated TPOAbs and the progression of subclinical hypothyroidism to overt hypothyroidism is well established (4 –7), but estimates of progression range between 4.3% and 80% for TPOAb-positive patients (4,5). In addition, elevated TPOAb levels have been found in the presence of several other debilitating extrathyroidal diseases (8 –11). It is currently unclear whether elevated TPOAbs are causally interfering with extrathyroidal disease processes, or whether they are merely a marker of a common pathway associated with autoimmune diseases. However, the co-occurrence of elevated TPOAbs with comorbidities may suggest associations between thyroid antibody status and clinical outcomes that could be of interest to clinicians and patients. There are ample data to suggest that thyroid (dys-)function is associated with age (12). Accordingly, potential effects of elevated TPOAb levels may be profoundly different in oldest old persons. Although associations have been found in younger age groups, prediction of thyroid dysfunction progression using TPOAbs has not been studied well for adults aged 85 years and over, nor have associations with other clinical outcomes.
Therefore, in this study, we aimed to investigate the associations of TPOAb levels with thyroid function, survival, physical function, disability in activities of daily living (ADL), cognitive function, and depressive symptoms in a community-dwelling prospective cohort of oldest old persons.
Materials and Methods
Study population
This study was performed using data from the Leiden 85-plus Study, a population-based cohort study of 85-year-old residents of Leiden, the Netherlands. Eligible participants were all inhabitants of Leiden who reached the age of 85 years between September 1997 and September 1999. Participants were visited in residential settings annually for interviews with trained research nurses, performing of functional tests, and the collection of nonfasting venous blood samples during a five-year follow-up period. Full details of the study protocol and procedures are described elsewhere (13). The Medical Ethical Committee of the Leiden University Medical Center approved the study. Informed consent was obtained from all participants. For severely cognitively impaired participants, informed consent was obtained by proxy.
Laboratory measurements of thyroid function
To reduce diurnal variation, nonfasting venous blood samples were drawn at each annual visit (85–90 years) between 8 and 11 a.m. Biobank samples were stored at −80°C.
TPOAb levels were measured once (age 86 years) and were assessed from biobank samples in a single batch by a solid-phase enzyme-labeled chemiluminescent sequential immunometric assay, using an Immulite 2000 XPi Immunoassay System (Siemens AG, Berlin, Germany; WHO 1st IRP 66/387 standard compliant). The lower and upper limits of detection were 5 and 1000 IU/mL, respectively (within-run coefficient of variation 5.5%, total 6.9%). TPOAb levels below the detection limit of 5 IU/mL were set at 5 IU/mL for the aim of the present analyses.
TPOAb levels ≥35 IU/mL were considered elevated in compliance with local laboratory reference ranges. Serum TPOAb levels were available for 488 participants (of a total 599 participants in the total cohort) at the age of 86 years, that is, 1 year after start of the study. Earlier research demonstrated little to no change in TPOAb levels over time, even when underlying thyroid disease was treated (14). Therefore, TPOAb levels at age 86 years were assumed to be constant over time and representative for the levels at age 85 years. A more detailed description of the included participants is included as a flowchart (Supplementary Fig. S1).
Plasma levels of thyrotropin (TSH) and free thyroxine (fT4) were measured 3 times for a 4-year period (85, 87, and 88) and were analyzed in batches using a fully automated Elecsys 2010 system (Hitachi, Tokyo, Japan). Reference ranges used for TSH were 0.3 to 4.8 mIU/L and 13.0 pmol/L (1.00 ng/dL) to 23.0 pmol/L (1.79 ng/dL) for fT4 in accordance with manufacturer specifications and local laboratory cutoffs. TSH and fT4 measurements were available at age 85 (baseline), 87, and 88 years. Participants were grouped into 5 clinical strata of thyroid function based on TSH and fT4 levels: overt hypothyroidism (TSH >4.8 and fT4 < 13), subclinical hypothyroidism (TSH >4.8 and 13 ≤ fT4 ≤ 23), euthyroidism (0.3 ≤ TSH ≤4.8), subclinical hyperthyroidism (TSH <0.3 and 13 ≤ fT4 ≤ 23), and overt hyperthyroidism (TSH <0.3 and fT4 > 23) at age 85, 87, and 88 years.
Mortality
Mortality information was available for a 10-year follow-up period and obtained from records of Statistics Netherlands (Centraal Bureau voor de Statistiek, The Hague) up to September 2008 (available for all participants).
Functional parameters
Outcomes of physical function, disability in ADL, cognitive function, or depressive symptoms were available for a 5-year follow-up period (age 85 to 90 years) unless otherwise specified.
Physical function
Hand grip strength measurements in kilograms using a Jamar hand dynamometer (Sammons Preston, Inc., IL) were used as a proxy for overall muscle strength (15). Hand grip strength measurements were performed at age 85 and 89 years. At ages 86 through 90 years, gait speed was measured over a dual 3 m walk with a turn halfway and expressed in meters per second (16).
Activities of daily living
Disability in ADL was assessed using the self-reported Groningen Activity Restriction Scale (GARS) (17). This questionnaire consisted of 18 items of daily functioning and independent living such as “getting in and out of bed” and “ability to fully dress yourself.” Each item could be awarded a maximum of four points, with one point indicating “able to do so independently” and four points indicating “requiring assistance.” A higher summed score indicates more disability in ADL.
Cognitive function
Mini Mental State Examination (MMSE) questionnaires (18) were taken for assessing overall cognitive functioning as well as Stroop-card examinations (concentration) (19) and Letter Digit Coding Tests (LDCTs, cognitive processing speed) (20). The MMSE questionnaire contains 19 items adding up to a total score of 30. Higher scores indicate better cognitive functioning. For the Stroop-card examination, the time in seconds it took to complete the third card with 40 words of colors printed in a different color was used. The Stroop test demonstrates the interference effect in the reaction time for a color-word task. Shorter times indicate better concentration. For the LDCT, participants completed digits corresponding to a random set of preprinted letters according to a key. The number of correct substitutions in 60 seconds was used for analysis.
Depressive symptoms
A presence of depressive symptoms was evaluated with the Geriatric Depression Scale (GDS-15) (21) consisting of 15 individual items in all subjects with a MMSE score ≥18 points. Higher scores indicate the presence of more depressive symptoms.
Demographics and medication
Information on highest completed level of education and independent living status was gathered during the interview. Use of any or a combination of thyroid influencing medication (levothyroxine, antithyroid medication, amiodarone, lithium, glucocorticosteroids, and/or interferon) was ascertained annually through registries of pharmacy records.
Statistical analyses
Continuous variables were described as mean with standard deviation or as median with interquartile range, where appropriate, and categorical variables were presented as frequency with percentage of the total. Participants were stratified into a normal (negative) TPOAb group (<35 IU/L) or elevated (positive) TPOAb group (≥35 IU/L) at baseline. Between-group comparisons of baseline characteristics were performed with Mann–Whitney U tests for continuous variables or χ2 tests for categorical data.
Association of TPOAbs with all-cause 10-year cumulative survival was estimated with the Kaplan–Meier method in all participants for which a TPOAb measurement was available, with follow-up starting at age 86 years. Survival analysis was performed using multivariable Cox proportional hazards regression model, adjusted for sex and fT4 levels, and excluding participants with thyroid influencing medication.
Associations of elevated TPOAb levels with TSH and fT4 levels over time were assessed with repeated measurements linear mixed effect models with an unstructured covariance structure, adjusted for sex, and reported as an estimated mean difference over time for both TSH and fT4. Slope divergence was assessed through the inclusion of a TPOAb × time-interaction covariate.
Incident thyroid dysfunction was defined as newly developed thyroid dysfunction between age 85 and 88 years in euthyroid participants at age 85 years. Changes in TSH and fT4 over 3 years' time (ΔTSH and ΔfT4) were calculated by subtracting the baseline thyroid function levels from levels at age 88 years and modeling these changes in linear mixed effect models adjusting for sex and using an unstructured covariance structure. Thyroid dysfunction at age 85 years was cross-tabulated, and χ2 tested, with thyroid dysfunction at age 87 and 88 years for all clinical thyroid strata, provided the participant was still alive at age 88 years, to determine whether TPOAb levels are associated with change from one clinical thyroid stratum to another.
Longitudinal associations between TPOAbs and physical function, disability in ADL, cognitive function, and depressive symptoms were assessed with repeated measurements linear mixed models with an unstructured covariance structure, adjusted for sex, and reported as estimated mean change and difference in both TPOAb groups in function over five years of follow-up.
For all analyses, SPSS Statistics Software version 22.0 for Windows (IBM, Armond, NY) was used. A p-value <0.05 was considered statistically significant.
Sensitivity analysis
All analyses were repeated excluding all participants (n = 26) using any form of thyroid influencing medication at baseline (levothyroxine, antithyroid medication, amiodarone, lithium, glucocorticosteroids, or interferon).
Results
Study population characteristics at baseline
Table 1 shows the baseline characteristics for all study participants in whom TPOAb was measured. In total, 64 (13.1%) of 488 study participants aged 85 years had elevated TPOAb levels. Participants in the elevated TPOAb group more often were female compared with the normal TPOAb group (81.3% vs. 65.8%, p = 0.008).
Study Population Characteristics at 85 Years of Age
The Stroop test demonstrates the interference effect in the reaction time for a color-word task. Data are presented as counts (%) for demographics and clinical thyroid function strata, as median (IQR) for thyroid function parameters and functional status with exception of LDTC and grip strength, which are mean (SD).
Use of any or a combination of levothyroxine, antithyroid medication, amiodarone, lithium, glucocorticosteroids, or interferons.
fT4, free thyroxine; GARS, Groningen Activity Restriction Scale; GDS, geriatric depression scale; IQR, interquartile range; LDCT, Letter Digit Coding Test; MMSE, Mini Mental State Examination; SD, standard deviation; subs/m, correct substitutions per minute; TPOAbs, thyroperoxidase antibodies; TSH, thyrotropin.
At baseline, elevated TPOAb was associated with an increased percentage of overt hypothyroidism (14.5% vs. 6.4%, p = 0.012) and subclinical hypothyroidism (16.1% vs. 3.1%, p < 0.001) compared with normal levels of TPOAbs. Median TSH levels were higher in participants with elevated TPOAbs (2.5 mIU/L vs. 1.8 mIU/L, p < 0.001). Level of education and independent living status were comparable between the groups. No clinically meaningful differences were observed for assessments of depressive symptoms and physical or cognitive functioning.
TPOAbs and survival
A Kaplan–Meier curve shows a small 10-year cumulative survival benefit in participants with elevated TPOAb levels compared with normal TPOAb levels (p = 0.032, Log-Rank test, Fig. 1). In a multivariable Cox-regression model, adjusted for sex and fT4, and excluding participants with thyroid influencing medication, elevated TPOAb levels were associated with improved survival (hazard ratio 0.72, [95% confidence interval, CI, 0.53–0.99], p = 0.044).
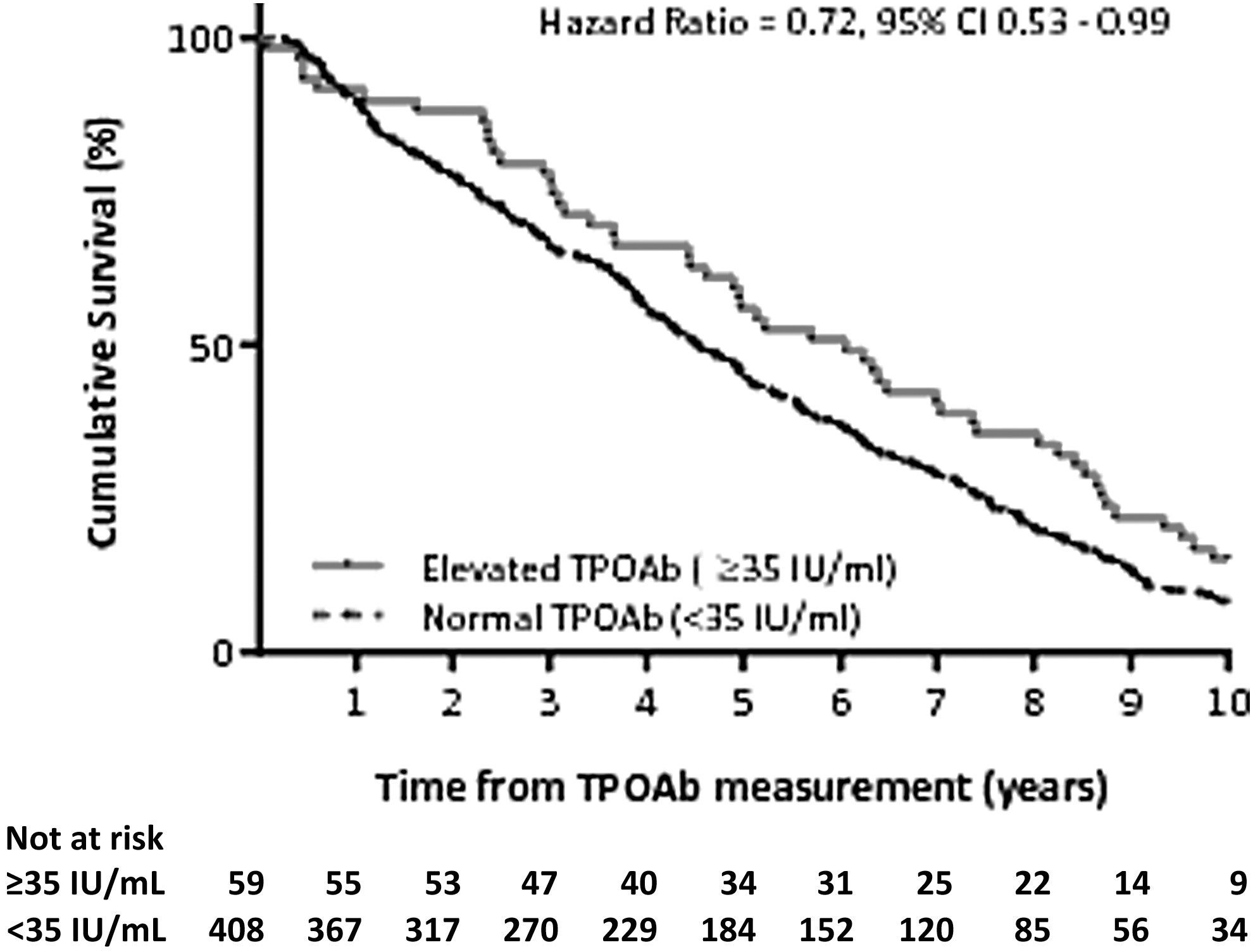
Association of baseline TPOAbs with all-cause 10-year cumulative survival from 86 years of age. Survival was estimated with the Kaplan–Meier method in all participants for which a TPOAb measurement was available, with follow-up starting at age 86 years. Hazard ratio was assessed using multivariable Cox proportional hazards regression models adjusted for sex and excluding participants with thyroid influencing medication. TPOAbs, thyroperoxidase antibodies.
TPOAbs and changes in thyroid function
Median fT4 levels were comparable at ages 85, 87, and 88 years between participants with elevated or normal TPOAb levels (estimated mean difference between participants with elevated TPOAbs and normal TPOAbs −0.15 mIU/L, [95% CI −0.96 to 0.66], p = 0.715) (Fig. 2). Participants with elevated TPOAb levels had higher median TSH levels at baseline than participants with normal TPOAb levels (age 85 years, respectively, 2.46 mIU/L vs. 1.78 mIU/L, p < 0.001) and this difference remained over time in linear mixed regression models (estimated mean difference 1.45 mIU/L, [95% CI 0.862.04], p < 0.001). Differences in TSH levels between the groups, however, did not increase or decrease with time (estimated mean difference −0.08 mIU/L, [95% CI −0.65 to 0.48], p-value for time interaction = 0.645).
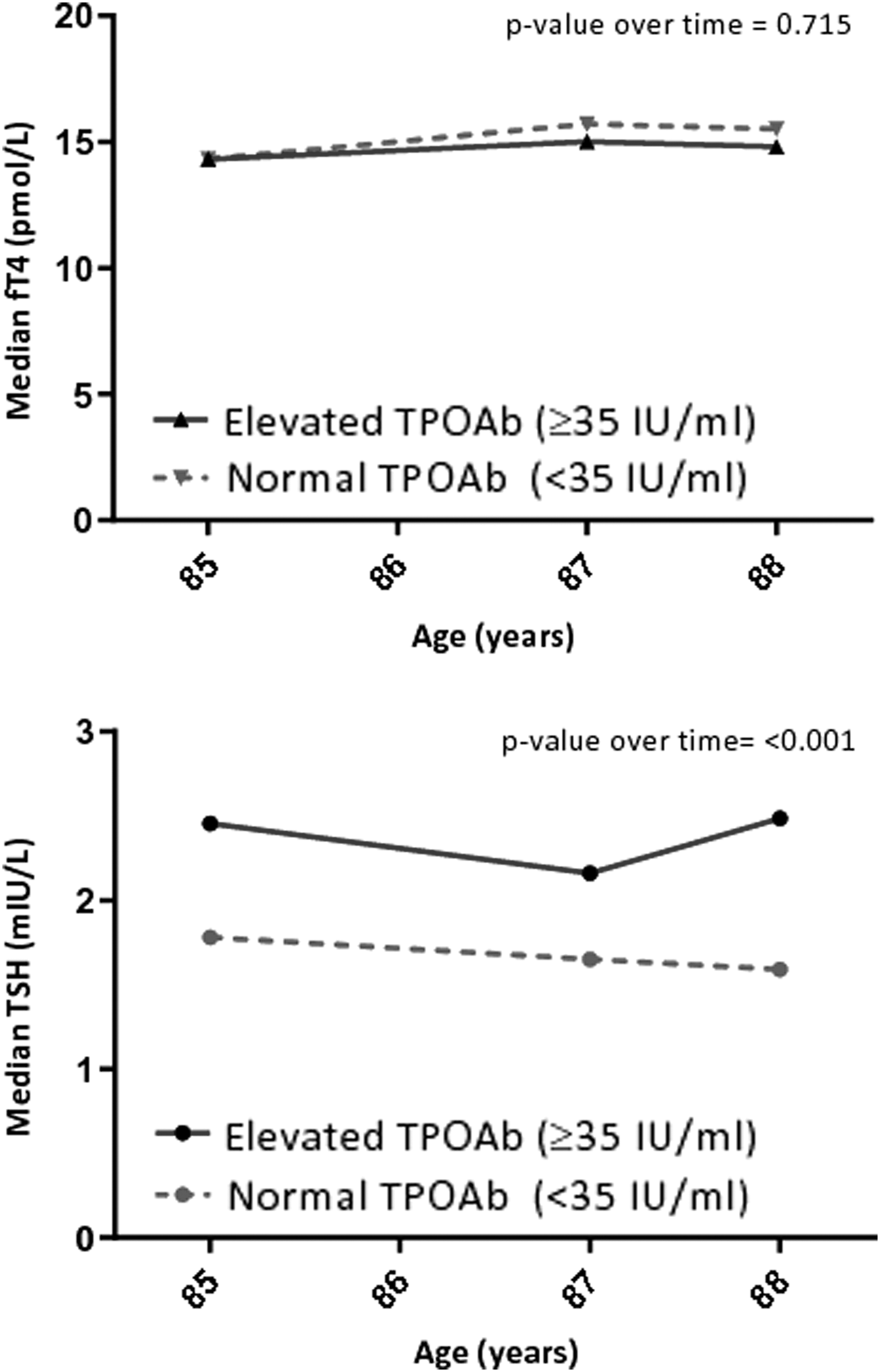
Association of baseline TPOAbs with TSH and fT4 during three-year follow-up. Associations over time were estimated using repeated measures linear mixed models, correcting for sex. fT4, free thyroxine; TSH, thyrotropin.
TPOAbs and incident thyroid disease
Incident cases of thyroid disease during follow-up in all euthyroid participants at baseline, who were still alive at age 88 years, are presented in Table 2. Of the surviving participants who were euthyroid at baseline, 97.1% remained euthyroid after 3 years of follow-up regardless of TPOAb status. Incidence of thyroid disease in the entire cohort was low with six new cases in the elevated TPOAb group versus one new case in the elevated TPOAb group. Participants with elevated TPOAb levels showed a very slight annual increase in TSH levels compared with participants with normal TPOAb levels (0.1 mIU/L vs. −0.1 mIU/L, p = 0.013). Participants with thyroid dysfunction at baseline either remained in their respective clinical thyroid stratum or regressed to a more euthyroid state (i.e., overt hypothyroidism regressed to subclinical hypothyroidism) after three years of follow-up in equal proportions in the normal and elevated TPOAb groups (data not shown).
Association of Thyroperoxidase Antibodies in Euthyroid Participants at Baseline with Thyroid Function During Three-Year Follow-Up
Data are presented as counts (%) and median (IQR). Incident thyroid dysfunction was assessed by reclassifying all euthyroid participants at baseline per TSH and fT4 status after three years and assessed using χ2 tests. Δ TSH and fT4 were calculated as mean change in thyroid function after three years using linear mixed effect models adjusting for sex.
TPOAbs and functioning
Table 3 shows associations between TPOAbs and functional status over a five-year follow-up period. No clear differences were observed in physical functioning (grip strength or gait speed), activity restriction scores (GARS), cognitive function (MMSE, LDCT, and Stroop card examination) and depressive symptoms scores (GDS) over time.
Longitudinal Associations of Thyroperoxidase Antibody Levels and Physical Function, Disability in Activities of Daily Living, Cognitive Function, and Depressive Symptoms for Five Years of Follow-Up
The Stroop test demonstrates the interference effect in the reaction time for a color-word task. Data are presented as estimated mean change in physical or cognitive function calculated for five years of follow-up per TPOAb group. The difference is estimated using repeated measures linear mixed models with normal TPOAb levels as reference group, adjusted for sex and baseline scores, with corresponding CIs. Higher scores in grip strength, gait speed, MMSE scores and LDCT scores, and lower scores in GARS scores, Stroop examination scores, and GDS scores indicate better function.
CI, confidence interval.
Sensitivity analysis
Excluding all participants (n = 26) using any form of thyroid influencing medication at baseline did not change the results considerably (data not shown).
Discussion
The main findings of this observational prospective cohort study in oldest old community dwelling participants were first that elevated TPOAb levels were associated with higher TSH both at baseline and during follow-up. Second, elevated TPOAbs were associated with a decreased 10-year mortality risk. Third, elevated TPOAbs were not associated with an increased risk of incident thyroid disease. Fourth, elevated TPOAbs were not associated with changes in physical function, disability in ADL, cognitive function, or depressive symptoms.
The baseline associations between elevated TPOAb levels and female sex, elevated TSH levels, and prevalent overt and subclinical hypothyroidism described in this study are in line with earlier studies. Elevated TPOAb levels can be found in up to 10% of euthyroid older persons (22) and are more frequently found in Hashimoto's thyroiditis (90%), Graves' disease (80%), and nonautoimmune thyroid disease (23). Such conditions are more prevalent in female patients, can give rise to elevated TSH levels, and may lead to subclinical and overt thyroid disease through a myriad of disease mechanisms.
In this study, elevated TPOAb levels were associated with a 10-year cumulative survival benefit. Moreover, this association was independent of sex or fT4 levels, suggesting that any effects on survival are probably not mediated through an increased or decreased thyroid function. Earlier research investigating associations between TPOAbs and survival yielded contradicting results, with some suggesting that mild thyroid dysfunction may be associated with favorable health status and longevity in old age (24 –26 years), while subsequent large-scale individual participant data meta-analysis failed to demonstrate similar effects (27). The increased overall all-cause survival associated with elevated TPOAbs is an interesting epidemiological finding, particularly in light of earlier identified prolonged survival in participants aged ≥85 years with thyroid dysfunction; however, etiologic research is needed to further explain any potential beneficial effects from a physiologic standpoint (25).
Thyroid dysfunction usually progresses from euthyroid and subclinical thyroid disease to overt thyroid pathology (28). Although number of incidences were low, in this study, no differences in disease progression were found when participants were stratified by TPOAb levels, comparable with results of recent studies in older age groups (29,30). Although the TPOAb-positive participants demonstrated increased survival time, and both groups demonstrated a decline in functional status not uncommon of this age group, associations between TPOAbs and physical function, disability in ADL, cognitive function, or the presence of depressive symptoms during follow-up were not identified. Earlier research has provided ambiguous findings for most of the aforementioned associations. However, when examined more carefully, in general these earlier results are in line with the findings of this study. For instance, it has been suggested that the presence of elevated TPOAbs is related with an increased risk of depressive symptoms and depression, regardless of thyroid status (31 –34). However, these studies were performed in small, younger, or highly selected populations such as pregnant or perimenopausal women. When investigated in large scale or slightly older populations, such associations were no longer clearly demonstrable (35,36), and in older patients these associations were clearly absent (37). Any potential extrathyroidal effects of TPOAbs that contribute to functional decline may be subtle and clinically of little importance in old age. Our study corroborates the opinion that the relevance of TPOAb measurement for the prediction of progression of thyroid disease is possibly lower in the older age group than in middle or younger age groups (38,39).
The findings of our study suggest a limited role for adding TPOAb measurements to the standard thyroid function tests (TSH and fT4) in the oldest old, which have been well established for estimating and monitoring the severity, pathophysiology, and progression of thyroid (dys-)function (40), even in the oldest old. However, future research with repeated TPOAbs, thyroid function, and physical and cognitive function measurements over a longer period of time and in cohorts of older persons is needed for proper causal inferences and to establish whether elevated TPOAbs causally influence clinical outcomes.
Strengths and weaknesses
The prospective follow-up design of the study with a full 5-year follow-up of clinical data and 10-year follow-up for mortality data is a strong point of the study. The unselected, population-based, and sizable sample is an accurate representation of the older community-dwelling population in the Leiden district and the Netherlands as a whole (Supplementary Fig. S1). The highly standardized study protocol with validated assessments and a repeated measurements design ensured high precision and reliability of the collected data. Moreover, iodine intake is considered sufficient in the Netherlands (41).
TPOAb levels were assessed only once after 15 years of frozen storage at −80°C. It is currently unknown how and to what extent TPOAb stability is affected during prolonged freezing periods. In an earlier study, no statistically significant changes were found in TPOAb samples stored at +4°C for 6 days or in samples exposed to 50 freezing and thawing cycles (42). Hence, we assume little to no changes in TPOAb levels during storage. Even if degradation has occurred, we expect the degradation to be similar across the groups. Unfortunately, TPOAb measurements were only available at age 86 years, while other thyroid function measures were available from age 85 years onward. We cannot exclude the possibility that TPOAb levels at age 85 years or from age 87 years onward were different or changed over time. However, the demonstrated persistence of having elevated or normal TPOAb levels over time, even when underlying thyroid disease is being treated (14), reinforces our premise that TPOAb levels remained constant at all visits in all but a negligible number of participants.
Until now, earlier research for TPOAbs in older age groups has mainly focused on estimating TPOAb prevalence and incidence estimates (4 –6). To the authors' knowledge, this is one of the first studies to cross-sectionally and longitudinally assess associations between TPOAbs and clinically relevant health outcomes in an unselected cohort of community-dwelling oldest old.
In conclusion, our study confirms the cross-sectional associations of elevated TPOAb levels with high TSH levels and a higher prevalence of subclinical and overt hypothyroidism in the oldest old. Over time, elevated TPOAb levels predict a survival benefit for a 10-year follow-up but are not associated with thyroid dysfunction progression, a decline in presence of depressive symptoms, or a decline in physical or cognitive functioning.
Footnotes
Author Disclosure Statement
Dr. Du Puy had full access to the study data and article and takes responsibility for the integrity of the work as a whole. The corresponding author attests that all listed authors meet authorship criteria according to the ICMJE recommendations and that no other persons meeting the criteria have been omitted. The sponsor had no role in the design and conduct of the study, in the collection, analysis, and interpretation of the data, nor in the preparation, review, or approval of the article. The authors declare that they have no competing financial interests.
Funding Information
The Leiden 85-plus Study was partly funded by an unrestricted grant from the Dutch Ministry of Health, Welfare and Sports (1997–2001).
Supplementary Material
Supplementary Figure S1